Operative Management of Lower Extremity Fractures: A Comprehensive Surgical Guide
Key Takeaway
The operative management of lower extremity fractures requires a profound understanding of injury biomechanics, precise anatomical reduction, and stable internal fixation. This guide explores critical classifications, including Lauge-Hansen and Danis-Weber for ankle trauma, alongside advanced surgical approaches for tibial pilon, plateau, and femoral fractures. Mastery of these principles ensures optimal restoration of articular congruity, mechanical alignment, and early functional rehabilitation in complex orthopedic trauma.
PRINCIPLES OF LOWER EXTREMITY TRAUMA
The operative management of lower extremity fractures demands a rigorous synthesis of biomechanical principles, meticulous soft-tissue handling, and precise osteosynthesis. The primary objectives are the restoration of the mechanical axis, absolute stability of articular surfaces, and relative stability of diaphyseal segments to promote early, pain-free mobilization. This masterclass delineates the evidence-based surgical strategies for fractures spanning the ankle, tibia, knee, and femur, tailored for the postgraduate orthopedic surgeon.
ANKLE FRACTURES AND FRACTURE-DISLOCATIONS
Ankle fractures represent a complex disruption of the mortise, requiring an intimate understanding of rotational biomechanics. The stability of the talus within the mortise is paramount; even a 1-mm lateral shift of the talus reduces tibiotalar contact area by 42%, leading to rapid post-traumatic arthrosis.
Biomechanics and Classification
The evaluation of ankle fractures relies heavily on two foundational classification systems: Lauge-Hansen and Danis-Weber.
The Lauge-Hansen Classification
This system predicts the sequence of ligamentous and osseous failure based on foot position at the time of injury (Supination vs. Pronation) and the direction of the deforming force (External Rotation, Adduction, or Abduction).
* Supination-External Rotation (SER): The most common pattern. The sequence progresses from the anterior inferior tibiofibular ligament (AITFL) to a short oblique fibular fracture, followed by the posterior inferior tibiofibular ligament (PITFL) or posterior malleolus, and finally the medial malleolus or deltoid ligament.
* Pronation-External Rotation (PER): Begins medially (deltoid or medial malleolus), progresses to the AITFL, results in a high fibular fracture (Maisonneuve variant), and concludes with posterior mortise disruption.
Clinical Pearl: For fractures resulting from an external rotation mechanism, closed reduction is achieved by reversing the vector of injury—utilizing a pronation, inversion, or internal rotation manipulation.
The Danis-Weber Classification
Based purely on the anatomical level of the fibular fracture relative to the syndesmosis:
* Type A: Infrasyndesmotic (typically Supination-Adduction).
* Type B: Transsyndesmotic (typically SER).
* Type C: Suprasyndesmotic (typically PER), highly associated with syndesmotic disruption.
Surgical Warning: Some authors caution against relying solely on the Lauge-Hansen classification to dictate operative intervention. Treatment must be predicated on a clinical and radiographic determination of stability. O’Leary and Ward described a deceptive abduction–external rotation mechanism resulting in a medial malleolar fracture and simultaneous avulsion of the deltoid ligament, emphasizing the difficulty in determining the full extent of injury after high-velocity impacts.
Surgical Approaches and Fixation Techniques
Lateral Malleolus
* Positioning: Supine with a bump under the ipsilateral hip to internally rotate the leg, bringing the fibula anteriorly.
* Approach: A direct lateral or posterolateral incision. The posterolateral approach is preferred if a posterior malleolar fracture requires simultaneous fixation.
* Fixation: For Weber B fractures, a lag screw placed perpendicular to the fracture plane followed by a lateral neutralization plate is the gold standard. In osteoporotic bone, locking plates or antiglide plating (placed posterolaterally) provide superior biomechanical stability.
Medial Malleolus
* Approach: Anteromedial or direct medial incision, taking care to protect the great saphenous vein and saphenous nerve.
* Fixation: The joint must be inspected for osteochondral debris. Fixation is typically achieved with two partially threaded 4.0-mm cancellous screws to provide interfragmentary compression. For vertical shear fractures (Supination-Adduction), an anti-glide plate is biomechanically superior to screw fixation alone.
Syndesmotic Injury and Deltoid Ligament Tears
Whitelaw et al. strongly recommend the intraoperative evaluation of ankle joint stability using the anterior drawer and external rotation stress tests (Cotton test) after bony stabilization of the malleoli.
* If the syndesmosis is unstable, reduction is achieved with a large pointed reduction forceps.
* Fixation utilizes one or two 3.5-mm or 4.5-mm cortical screws placed parallel to the joint line, 2 to 3 cm proximal to the plafond, engaging three or four cortices. Alternatively, dynamic suture-button constructs have shown excellent outcomes with reduced hardware-related complications.
TIBIAL PILON FRACTURES
Tibial pilon fractures involve the weight-bearing articular surface of the distal tibia, typically resulting from high-energy axial loading combined with rotational forces. The management of the soft tissue envelope dictates the surgical timing and approach.
Staged Management Protocol
High-energy pilon fractures are notorious for devastating soft-tissue complications, including wound dehiscence and deep infection. The modern standard of care is a Two-Stage Delayed Open Reduction and Internal Fixation.
- Stage 1 (Damage Control): Immediate application of a spanning joint-bridging external fixator (Delta frame). The fibula may be plated acutely if the soft tissues laterally are pristine, which helps restore limb length and alignment.
- Stage 2 (Definitive Fixation): Delayed 10 to 21 days until the "wrinkle sign" appears, indicating the resolution of soft-tissue edema.
Operative Approaches
- Anterolateral Approach: Utilized for valgus deformity patterns and Chaput fragment fractures. The incision is placed between the tibia and fibula, utilizing the internervous plane between the superficial and deep peroneal nerves.
- Anteromedial Approach: Indicated for varus patterns. Care must be taken to avoid placing the incision directly over the tibial crest to prevent wound breakdown.
- Posterolateral Approach: Ideal for posterior shearing fractures (Volkmann fragment). The patient is positioned prone. The incision is made between the Achilles tendon and the peroneal tendons, mobilizing the flexor hallucis longus (FHL) medially to expose the posterior tibia.
Surgical Pitfall: Never compromise the soft tissue bridge between incisions. If both medial and lateral approaches are required, a minimum skin bridge of 7 cm must be maintained to prevent catastrophic skin necrosis.
TIBIAL SHAFT FRACTURES
The subcutaneous nature of the tibial diaphysis makes it highly susceptible to open fractures and nonunions.
Intramedullary Nailing
Reamed, statically locked intramedullary (IM) nailing is the gold standard for displaced diaphyseal tibial fractures.
* Positioning: Supine on a radiolucent table with the knee flexed over a triangle, or utilizing a fracture table.
* Entry Point: A medial parapatellar or transpatellar tendon approach. The exact entry point is critical: it must be slightly medial to the lateral tibial spine and immediately extra-articular on the anterior cortex.
* Biomechanics: Reaming increases the endosteal contact area, allowing for the insertion of a larger, stiffer nail, which enhances biomechanical stability and provides an autogenous bone graft effect at the fracture site.
Plate and Screw Fixation
While IM nailing is preferred for the diaphysis, plate fixation (Minimally Invasive Plate Osteosynthesis - MIPO) is indicated for:
* Metaphyseal fractures too proximal or distal for stable IM nail fixation.
* Fractures with intra-articular extension.
* Open physes in pediatric patients.
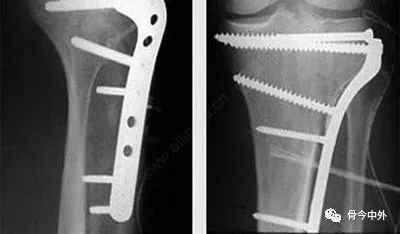
TIBIAL PLATEAU FRACTURES
Tibial plateau fractures disrupt the articular congruity of the knee and are frequently associated with meniscal and ligamentous pathology.
Classification
- Schatzker Classification:
- I: Lateral split.
- II: Lateral split-depression.
- III: Pure lateral depression.
- IV: Medial plateau (high energy, associated with knee dislocation).
- V: Bicondylar.
- VI: Plateau fracture with diaphyseal dissociation.
- Hohl and Moore Classification: Focuses on fracture-dislocations and the risk of neurovascular compromise.
Surgical Treatment
The goal is anatomical restoration of the articular surface, restoration of the mechanical axis, and stable fixation to allow early range of motion.
- Fracture of the Lateral Condyle (Schatzker I-III):
- Addressed via an anterolateral submeniscal approach.
- Depressed articular segments are elevated from below using a cortical window and bone tamps.
- The resulting metaphyseal void must be filled with autograft, allograft, or bone substitutes to prevent subsidence.
- Fixation is achieved with a lateral pre-contoured locking buttress plate.
- Arthroscopically Assisted Reduction: Increasingly utilized for Schatzker I-III fractures to directly visualize articular reduction and address concomitant meniscal tears (present in up to 50% of Schatzker II fractures) without extensive arthrotomy.
- Comminuted Proximal Fractures (Schatzker V-VI): Require dual plating (medial and lateral) or a combination of lateral locking plates and medial external fixation to prevent varus collapse.
FRACTURES OF THE DISTAL FEMUR
Distal femoral fractures (supracondylar and intercondylar) present significant challenges due to the deforming forces of the gastrocnemius (causing apex posterior angulation) and the quadriceps (causing shortening).
Operative Techniques
- Plate and Screw Fixation: The advent of anatomically pre-contoured lateral locking plates has revolutionized the treatment of distal femur fractures. These plates act as fixed-angle devices, providing superior hold in osteoporotic bone. They are typically inserted via a subvastus or lateral parapatellar approach.
- Dynamic Condylar Screw (DCS): Historically used for supracondylar fractures, the DCS provides excellent compression across the intercondylar notch but requires significant bone stock and is less effective in highly comminuted or osteoporotic fractures compared to locking plates.
- Retrograde Intramedullary Nailing: An excellent option for extra-articular supracondylar fractures (AO Type 33-A) and simple intra-articular splits (AO Type 33-C1).
- Approach: Inserted through the intercondylar notch via a medial parapatellar arthrotomy.
- Advantage: Minimizes soft tissue stripping laterally and is biomechanically advantageous for load-sharing.
FRACTURES OF THE FEMORAL SHAFT
Femoral shaft fractures are high-energy injuries that carry a risk of significant hemorrhage and systemic complications, including Acute Respiratory Distress Syndrome (ARDS). Early stabilization (within 24 hours) is critical for systemic resuscitation.
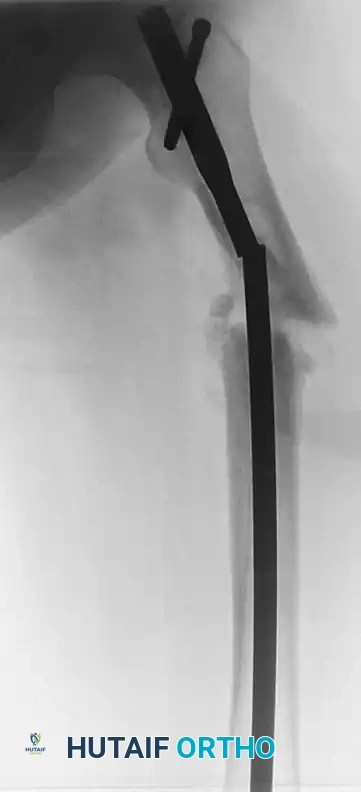
Intramedullary Fixation
IM nailing is the absolute standard of care for femoral shaft fractures.
- Antegrade Femoral Nailing:
- Entry Point: Piriformis fossa (collinear with the long axis of the femur) or the Greater Trochanter (requires a specifically designed trochanteric entry nail to avoid varus malalignment).
- Positioning: Lateral decubitus or supine on a fracture table.
- Retrograde Nailing of the Femur:
- Indicated in polytrauma patients, ipsilateral tibial shaft fractures (floating knee), ipsilateral femoral neck fractures, or morbidly obese patients where antegrade positioning is difficult.
- Complications: Knee pain is the most frequently cited complication of retrograde nailing, necessitating meticulous countersinking of the nail beneath the articular cartilage of the intercondylar notch.
Clinical Pearl: In cases of a femoral shaft fracture with a concomitant femoral neck fracture (occurring in 2-6% of cases), the femoral neck fracture takes absolute priority. It must be anatomically reduced and stabilized first (typically with cancellous screws or a sliding hip screw) before addressing the shaft, often utilizing a retrograde nail or a single reconstruction-style antegrade nail.
External Fixation
External fixation of the femur is generally reserved for damage control orthopedics in the hemodynamically unstable polytrauma patient (in extremis). Once the patient's physiology is optimized, the external fixator is converted to an intramedullary nail, ideally within 14 days to minimize the risk of pin-tract infections seeding the medullary canal.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of lower extremity fracture surgery is inextricably linked to postoperative rehabilitation.
* Early Mobilization: Continuous Passive Motion (CPM) and early active range of motion are instituted immediately for intra-articular fractures (pilon, plateau, distal femur) to nourish the articular cartilage and prevent arthrofibrosis.
* Weight-Bearing: Diaphyseal fractures treated with IM nails can often be weight-bearing as tolerated immediately. Conversely, intra-articular fractures treated with plate osteosynthesis require strict non-weight-bearing or touch-down weight-bearing for 8 to 12 weeks until radiographic evidence of bridging callus is observed.
* DVT Prophylaxis: Chemical thromboprophylaxis (e.g., Low Molecular Weight Heparin) is mandatory for all lower extremity fractures requiring operative intervention, continued until the patient is fully ambulatory.
You Might Also Like