Comprehensive Spinal Anatomy and Surgical Approaches: An Advanced Operative Guide
Key Takeaway
A comprehensive mastery of spinal anatomy is the foundation of safe and effective spine surgery. This guide details the osteology, arthrology, and neurology of the vertebral column, alongside step-by-step surgical approaches. Designed for orthopedic residents and consultants, it explores biomechanics, patient positioning, and precise anatomical dissection techniques required for anterior and posterior spinal exposures, ensuring optimal postoperative outcomes and minimized iatrogenic complications.
Introduction to Spinal Osteology and Alignment
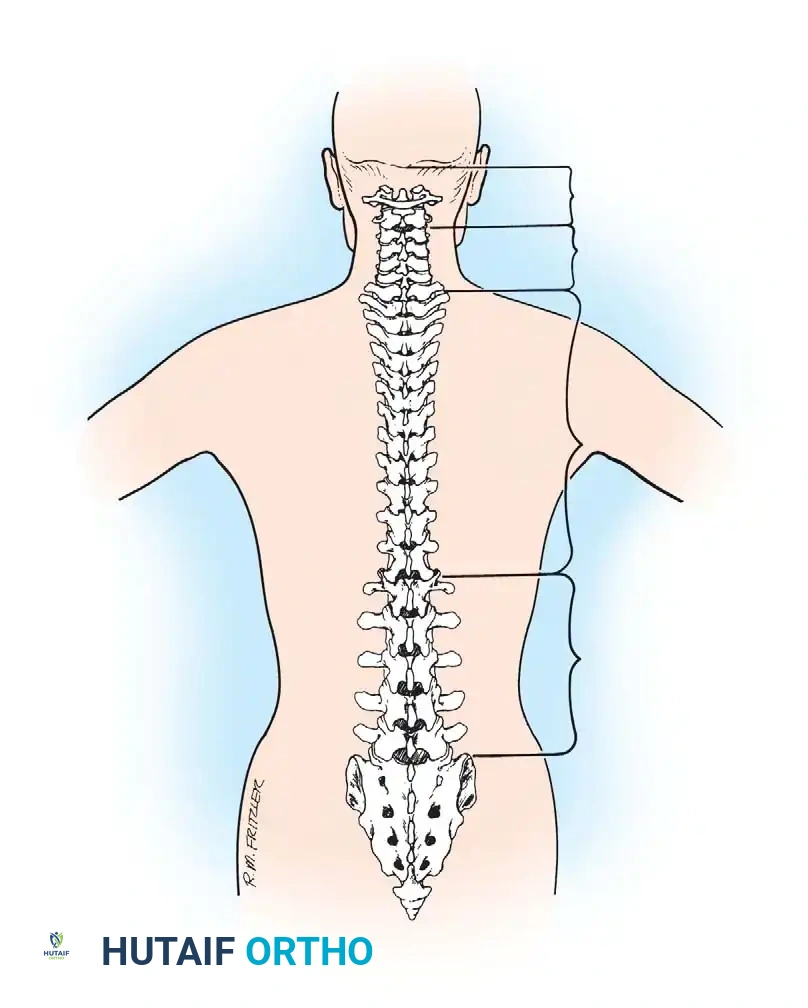
The vertebral column is a highly complex, biomechanically optimized structure designed to protect the neural elements, support the structural weight of the trunk, and facilitate a wide range of truncal motion. A profound understanding of spinal anatomy is the absolute prerequisite for executing safe and effective surgical approaches.
The vertebral column comprises 33 vertebrae divided into five distinct anatomical sections: seven cervical, 12 thoracic, five lumbar, five sacral, and four coccygeal segments. Because the sacral and coccygeal vertebrae are fused in the adult skeleton, the spine typically allows for 24 mobile segments. Congenital anomalies, such as transitional vertebrae (lumbarization of S1 or sacralization of L5) and variations in segmentation, are common and must be identified on preoperative imaging to prevent wrong-level surgery.
Sagittal alignment is a critical component of spinal biomechanics. The cervical and lumbar segments develop secondary lordotic curves as an infant acquires an erect posture and begins to walk. Conversely, the thoracic and sacral segments maintain the primary kyphotic postures present in utero. These kyphotic segments serve as rigid attachment points for the rib cage and pelvic girdle, respectively.
In general, the cross-sectional area of each mobile vertebral body increases progressively from cranial to caudal to accommodate increasing axial loads. The length of the vertebral column averages 72 cm in men and 62 to 65 cm in women. The central vertebral canal extends throughout the length of the column, providing a rigid, protective conduit for the spinal cord, conus medullaris, and cauda equina.
Anatomy of the Typical Vertebra
A typical vertebra comprises an anterior load-bearing body and a posterior neural arch that together enclose the vertebral canal.
- The Neural Arch: Composed of two stout pedicles laterally and two laminae posteriorly, which unite in the midline to form the spinous process.
- Processes: Projecting from the arch are the transverse processes (laterally) and the superior and inferior articular processes.
- Articulations: The articular processes articulate with adjacent vertebrae to form synovial facet joints. The relative spatial orientation of these articular processes dictates the degree of flexion, extension, lateral bending, or rotation possible at each specific segment.
- Muscular Attachments: The spinous and transverse processes serve as critical lever arms for the numerous paraspinal muscles and ligaments attached to them, facilitating dynamic stability.
Clinical Pearl: The pedicle is the anatomical bridge between the anterior and posterior columns. Its morphology changes significantly throughout the spine. Lumbar pedicles are wider and more sagittally oriented, making them ideal for transpedicular screw fixation, whereas mid-thoracic pedicles are narrower and angled more medially.
Anatomy of the Spinal Joints
The individual vertebrae are dynamically linked by a three-joint complex at each level: two posterior zygapophyseal (facet) joints and one anterior interbody joint.
Zygapophyseal (Facet) Joints
The joints between the neural arches are the zygapophyseal or facet joints. They exist between the inferior articular process of the cranial vertebra and the superior articular process of the caudal vertebra. These are true diarthrodial synovial joints. Their surfaces are covered by hyaline articular cartilage, bridged by a synovial membrane, and enclosed within a fibrous joint capsule.
Surgical Warning: The facet joints are innervated by the medial branches of the posterior primary rami. When performing posterior spinal exposures, excessive lateral dissection or aggressive retraction can denervate and devascularize the multifidus muscle and violate the capsule of the adjacent, non-operative facet joint, leading to adjacent segment disease (ASD).
Intervertebral Discs
The interbody joints contain specialized fibrocartilaginous structures called intervertebral discs. These are found throughout the vertebral column, with the notable exception of the atlantoaxial (C1-C2) articulation. Discs are engineered to accommodate multidirectional movement, sustain immense weight-bearing forces, and act as shock absorbers. They form a secondary cartilaginous joint (symphysis) at each level.
Each disc consists of three distinct components:
1. Vertebral End Plates: These are 1 mm-thick sheets of cartilage (a blend of fibrocartilage and hyaline cartilage) that cap the superior and inferior aspects of the vertebral bodies. With advancing age, the ratio of fibrocartilage to hyaline cartilage increases.
2. Nucleus Pulposus: A semifluid, gel-like mass of mucoid material located centrally. It is highly hydrated, consisting of 70% to 90% water. Its dry weight is predominantly proteoglycan (65%, primarily aggrecan) and Type II collagen (15% to 20%), which provides compressive resistance.
3. Anulus Fibrosus: A dense peripheral ring sandwiching the nucleus. It consists of 12 to 15 concentric lamellae. The collagen fibers in successive lamellae alternate their orientation (approximately 30 degrees to the horizontal), creating a highly engineered structure capable of withstanding multidirectional tensile and torsional strains. The anulus is 60% to 70% water, with Type I collagen constituting 50% to 60% of its dry weight.
The anulus and nucleus merge in a transitional zone without strict demarcation. Notably, intervertebral discs are the largest avascular structures in the human body. They rely entirely on passive diffusion from a specialized capillary network within the vertebral end plates for cellular nutrition and waste removal.
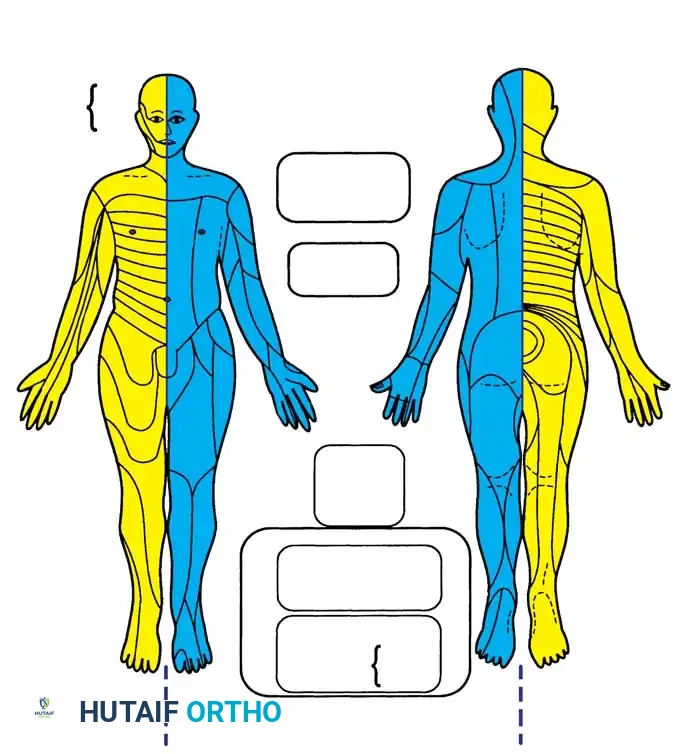
Neurologic Anatomy and Topographical Mapping
The spinal cord typically terminates at the L1-L2 intervertebral disc space as the conus medullaris, continuing distally as the cauda equina. Understanding the precise topographical mapping of dermatomes and myotomes is essential for localizing spinal pathology during clinical examination and avoiding iatrogenic injury during surgery.
Operative Surgical Approaches
Mastery of surgical approaches requires a deep understanding of internervous and intermuscular planes. The following sections detail the most critical anterior and posterior approaches utilized in modern operative orthopaedics.
Anterior Approach to the Cervical Spine (C3 to C7)
The anterior approach to the subaxial cervical spine, popularized by Smith and Robinson, is the workhorse exposure for anterior cervical discectomy and fusion (ACDF), corpectomy, and disc arthroplasty.
Indications:
* Cervical spondylotic myelopathy or radiculopathy.
* Herniated nucleus pulposus.
* Anterior column trauma (fractures/dislocations).
* Infectious discitis or osteomyelitis.
Patient Positioning:
* The patient is placed supine on the operating table.
* A transverse roll is placed between the scapulae to allow the shoulders to fall posteriorly, naturally extending the neck and opening the anterior disc spaces.
* The head is stabilized, often with a foam donut or Mayfield tongs if rigid fixation is required.
* The shoulders may be taped down to facilitate intraoperative fluoroscopy of the lower cervical spine (C6-T1).
Step-by-Step Surgical Technique:
1. Incision: A transverse incision is made within a natural skin crease (Langer's lines) on either the left or right side of the neck, depending on surgeon preference and pathology. A left-sided approach theoretically decreases the risk of injury to the recurrent laryngeal nerve, which has a more constant and protected course on the left.
2. Superficial Dissection: The skin and subcutaneous tissues are divided. The platysma muscle is identified and divided in line with the skin incision. Subplatysmal flaps are elevated superiorly and inferiorly.
3. Fascial Incision: The superficial layer of the deep cervical fascia is incised along the anterior border of the sternocleidomastoid (SCM) muscle.
4. Deep Dissection: The dissection proceeds bluntly through the avascular plane between the carotid sheath (containing the carotid artery, internal jugular vein, and vagus nerve) laterally, and the visceral axis (trachea, esophagus, and thyroid gland) medially.
5. Omohyoid Management: The omohyoid muscle crosses the operative field obliquely. It can be retracted inferiorly or divided if necessary for extensive exposures.
6. Prevertebral Fascia: The prevertebral fascia is identified and incised longitudinally in the midline.
7. Longus Colli Elevation: The medial borders of the longus colli muscles are identified. They are elevated subperiosteally from medial to lateral using electrocautery. Self-retaining retractors are placed beneath the elevated muscle bellies to protect the sympathetic chain, which lies on the lateral aspect of the longus colli.
Pitfall: Placement of retractor blades too laterally over the longus colli muscle can compress or injure the cervical sympathetic chain, resulting in postoperative Horner's syndrome (ptosis, miosis, anhidrosis).
Postoperative Protocol:
Patients are typically mobilized on the day of surgery. A soft cervical collar may be used for comfort, though rigid orthoses are rarely required following modern instrumented ACDF. Swallowing precautions and soft diets are recommended for the first 48 hours to mitigate transient dysphagia.
Posterior Approach to the Lumbar Spine (L1 to L5)
The posterior midline approach is the most common exposure in spine surgery, utilized for decompressions, discectomies, and pedicle screw instrumentation.
Indications:
* Lumbar spinal stenosis.
* Posterior instrumented fusion for degenerative disc disease or spondylolisthesis.
* Posterior column trauma or tumor resection.
Patient Positioning:
* The patient is placed prone on a specialized radiolucent spine table (e.g., Jackson frame).
* It is imperative that the abdomen hangs completely free. Any abdominal compression increases intra-abdominal pressure, which translates to the epidural venous plexus (Batson's plexus), resulting in excessive intraoperative bleeding.
* The hips and knees are slightly flexed to relax the sciatic nerve and psoas muscles.
Step-by-Step Surgical Technique:
1. Incision: A longitudinal midline incision is made centered over the spinous processes of the target levels, confirmed by fluoroscopy.
2. Fascial Incision: The lumbodorsal fascia is incised strictly in the midline, directly over the tips of the spinous processes.
3. Subperiosteal Dissection: Using Cobb elevators and electrocautery, the paraspinal muscles (multifidus and longissimus) are stripped subperiosteally from the spinous processes and laminae. The dissection proceeds from medial to lateral.
4. Facet Exposure: The dissection is carried laterally to the facet joints. For decompression alone, the medial aspect of the facet is exposed. For pedicle screw placement or posterolateral fusion, the dissection is carried over the facet joint to expose the transverse processes.
5. Hemostasis: Self-retaining retractors (e.g., Weitlaner or specialized spine retractors) are deployed. Meticulous hemostasis is achieved using bipolar cautery and hemostatic agents.
Surgical Warning: When exposing the transverse processes for fusion, care must be taken not to dissect anterior to the intertransverse membrane, as the exiting nerve roots and segmental vessels lie immediately ventral to this structure.
Postoperative Protocol:
Early mobilization is encouraged to prevent deep vein thrombosis and pulmonary complications. Postoperative bracing (e.g., TLSO) is dependent on bone quality and the rigidity of the internal fixation. Physical therapy focuses on core stabilization and isometric strengthening.
Anterior Retroperitoneal Approach to the Lumbar Spine (L1 to L5)
The anterior approach to the lumbar spine provides direct access to the anterior column for interbody fusion (ALIF) and total disc replacement, avoiding the posterior musculature and spinal canal.
Indications:
* Anterior Lumbar Interbody Fusion (ALIF).
* Lumbar total disc arthroplasty.
* Anterior corpectomy for trauma, tumor, or infection.
* Correction of sagittal plane deformity (restoration of lordosis).
Patient Positioning:
* The patient is positioned supine on a radiolucent table.
* A bump may be placed under the lumbar spine to accentuate lordosis and open the anterior disc spaces.
* The arms are extended abducted to 90 degrees.
Step-by-Step Surgical Technique:
1. Incision: A paramedian vertical, transverse, or oblique incision is made on the left side of the abdomen. The left-sided approach is preferred because it is easier to mobilize the aorta than the more fragile, thin-walled inferior vena cava (IVC).
2. Rectus Sheath: The anterior rectus sheath is incised. The rectus abdominis muscle is mobilized and retracted medially.
3. Retroperitoneal Access: The posterior rectus sheath and transversalis fascia are carefully incised to enter the retroperitoneal space. The peritoneum is bluntly swept medially off the undersurface of the abdominal wall.
4. Psoas Identification: The dissection proceeds posteriorly along the inner table of the ilium until the psoas major muscle is identified. The ureter, which adheres to the undersurface of the peritoneum, is swept medially and protected.
5. Vascular Mobilization: The great vessels are identified. At the L4-L5 level, the aorta bifurcates into the common iliac arteries, and the IVC bifurcates into the common iliac veins.
6. Ligation of the Iliolumbar Vein: To safely mobilize the left common iliac vein medially and access the L4-L5 disc space, the ascending iliolumbar vein must be meticulously identified, ligated, and divided. Failure to do so can result in catastrophic avulsion of the vein from the common iliac vein.
7. Disc Exposure: Once the vessels are safely retracted using blunt, padded retractors, the anterior longitudinal ligament (ALL) and the target intervertebral disc are exposed.
Clinical Pearl: The L5-S1 disc space is typically accessed below the bifurcation of the great vessels, working between the diverging common iliac arteries and veins. The L4-L5 disc space is accessed by mobilizing the great vessels from left to right.
Postoperative Protocol:
Patients are monitored closely for signs of vascular compromise or retroperitoneal hematoma. Diet is advanced slowly as postoperative ileus is a common, albeit transient, complication of retroperitoneal dissection. Deep vein thrombosis prophylaxis is critical due to the intraoperative manipulation of the iliac veins.
Conclusion
The surgical management of spinal pathology demands an uncompromising knowledge of osteology, arthrology, and neurovascular topography. Whether executing an anterior cervical decompression or a complex retroperitoneal lumbar exposure, the principles remain constant: meticulous preoperative planning, precise patient positioning, strict adherence to anatomical planes, and profound respect for the neural and vascular elements. Mastery of these foundational concepts ensures the highest standard of patient safety and optimal surgical outcomes.
You Might Also Like
