Kyphosis & Scheuermann Disease: Comprehensive Operative Management
Key Takeaway
Scheuermann disease is a structural kyphosis of the thoracic or thoracolumbar spine characterized by anterior wedging of at least three consecutive vertebrae. While non-operative management with bracing is effective in skeletally immature patients, severe deformities exceeding 75 degrees or those associated with intractable pain require surgical intervention. Modern operative management typically involves posterior-only spinal fusion utilizing Ponte osteotomies, pedicle screw instrumentation, and meticulous rod contouring to restore physiological sagittal balance.
INTRODUCTION TO SPINAL SAGITTAL ALIGNMENT
In the sagittal plane, the normal human spine exhibits four balanced, alternating curves that optimize biomechanical efficiency and load distribution. The cervical spine is lordotic; the thoracic spine is kyphotic (ranging from 20 to 50 degrees), with the curve typically extending from T2 or T3 down to T12; the lumbar region is lordotic (ranging from 31 to 79 degrees); and the sacral curve is kyphotic. Upon standing, the thoracic kyphosis and lumbar lordosis exist in a state of harmonious balance, minimizing the energy expenditure required to maintain an upright posture.
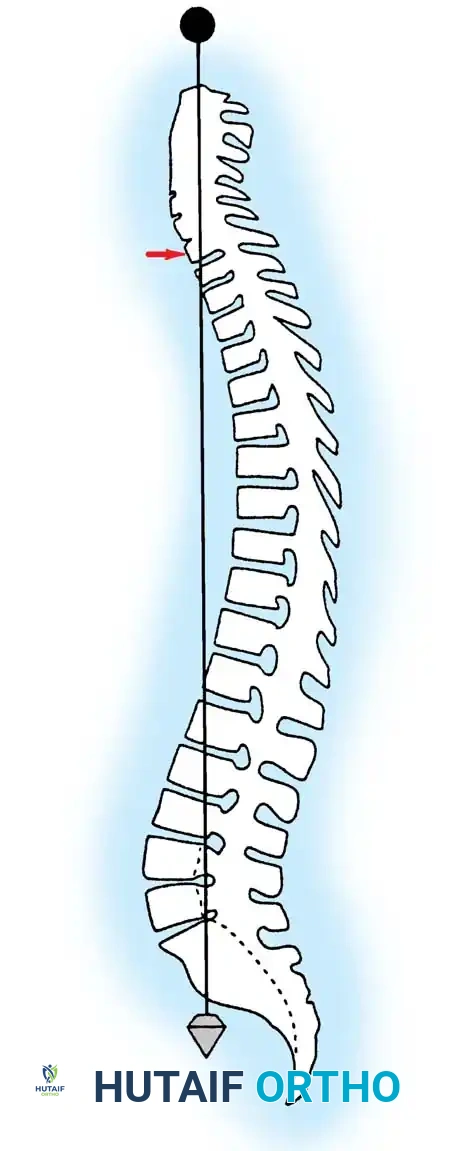
Normal sagittal balance is clinically defined by a plumb line dropped from the center of the C7 vertebral body, which should intersect the posterior superior corner of the S1 vertebra.
Positive sagittal balance occurs when the sagittal vertical axis (SVA) plumb line falls anterior to the sacrum, whereas negative sagittal balance occurs when the plumb line falls posterior to the sacrum. In the upright position, the spine is continuously subjected to gravitational forces. Several anatomical structures act in concert to maintain stability: the intervertebral disc complex (nucleus pulposus and anulus fibrosus), the ligamentous restraints (anterior longitudinal ligament, posterior longitudinal ligament, ligamentum flavum, apophyseal joint capsules, and interspinous ligaments), and the dynamic muscular envelope (long spinal erectors, short intrinsic rotatores/multifidi, and the abdominal musculature).
Kyphosis measuring 50 degrees or more in the thoracic spine is generally considered abnormal. Pathologic kyphotic deformity typically manifests when the anterior spinal column is unable to withstand compressive loads, leading to anterior column shortening. Conversely, disruption of the posterior column and an inability to resist tensile forces can lead to relative lengthening of the posterior elements, further exacerbating the kyphosis.
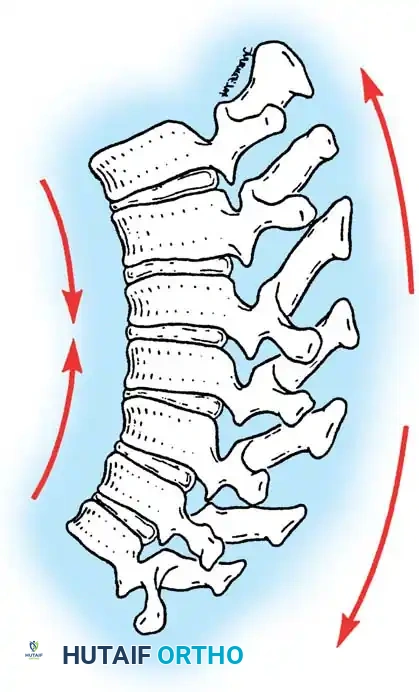
Clinical Pearl: The fundamental biomechanical principle of kyphotic deformity is the failure of the anterior column under compression combined with the failure of the posterior column under tension. Surgical correction must address both vectors: anterior column support and posterior column shortening.
SCHEUERMANN DISEASE: PATHOPHYSIOLOGY AND ETIOLOGY
Scheuermann disease is a rigid, structural kyphosis of the thoracic or thoracolumbar spine, occurring in 0.4% to 8.3% of the general population, with a slight male predominance. The age of onset typically coincides with the prepubertal growth spurt, between 10 and 12 years of age.
Etiological Theories
The precise etiology of Scheuermann disease remains multifactorial and highly debated.
* Osteonecrosis Theory: Scheuermann originally proposed that the kyphosis resulted from avascular necrosis of the ring apophysis of the vertebral body. However, Bick and Copel later demonstrated that the ring apophysis lies outside the true cartilaginous physis and does not contribute to longitudinal vertebral growth; thus, its disturbance cannot cause vertebral wedging.
* Disc Herniation Theory: In 1930, Schmorl suggested that vertebral wedging is caused by the herniation of nuclear disc material into the vertebral body (Schmorl nodes). He theorized that this extrusion diminishes intervertebral disc height, increasing anterior pressure and disturbing enchondral ossification. However, Schmorl nodes are ubiquitous and frequently occur in patients without Scheuermann disease.
* Vascular Groove Theory: Ferguson implicated the persistence of anterior vascular grooves in the vertebral bodies during adolescence, suggesting these defects create structural weaknesses leading to wedging.
* Ligamentous Bowstringing: Bradford and Moe investigated histological changes and found a thickened anterior longitudinal ligament (ALL) creating a bowstring effect across the apex of the kyphosis. Disc material was extruded under this ligament, compressing the bodies.
* Mechanical Factors: Mechanical overload is a highly probable contributor. Lambrinudi suggested that upright posture and ALL tightness contribute to the deformity. The condition is notably more common in adolescents engaged in heavy lifting or manual labor. Increased anterior pressure on the vertebral endplates causes uneven growth via the Hueter-Volkmann principle (a corollary to Wolff's law), where increased compression inhibits physeal growth.
* Biochemical Abnormalities: Aufdermaur, Spycher, Ippolito, and Ponseti identified abnormal collagen fibers and a decreased collagen-to-proteoglycan ratio in the endplate cartilage matrix, suggesting an underlying biochemical matrix defect.
CLASSIFICATION OF SCHEUERMANN DISEASE
Scheuermann disease is categorized into two distinct clinical entities based on the location and natural history of the deformity:
Typical Scheuermann Disease (Thoracic)
This is the classic and most common form, primarily involving the thoracic spine. It is defined by the Sorensen criteria: three or more consecutive vertebrae, each wedged 5 degrees or more, producing a rigid structural kyphosis.
Atypical Scheuermann Disease (Lumbar/Thoracolumbar)
Atypical Scheuermann disease is localized to the thoracolumbar junction or the lumbar spine. It is characterized by vertebral endplate irregularities, disc space narrowing, and anterior Schmorl nodes, but it does not strictly require the presence of three consecutively wedged vertebrae. This variant is frequently seen in male athletes and heavy laborers, suggesting a traumatic micro-injury etiology to the vertebral physes rather than a purely developmental anomaly.
CLINICAL EVALUATION
Patients typically present during the adolescent growth spurt. The primary complaints are postural deformity, mid-to-lower back pain, or both. Parents often mistakenly attribute the deformity to "poor posture," delaying formal diagnosis.
Pain is usually localized to the apex of the deformity or the compensatory hyperlordotic lumbar spine. It is exacerbated by physical activity and prolonged sitting, and typically subsides upon skeletal maturity. If lumbar pain is severe in a patient with thoracic kyphosis, the clinician must maintain a high index of suspicion for concurrent spondylolysis.
Physical Examination
Physical examination reveals a sharp, angular thoracic or thoracolumbar kyphosis accompanied by compensatory cervical and lumbar hyperlordosis.
Crucially, the kyphosis is rigid. During the Adams forward bending test, the deformity becomes more pronounced. When the patient is evaluated using the prone extension test, the structural kyphosis fails to correct, differentiating it from flexible postural kyphosis.

Rigid Scheuermann kyphosis failing to correct on prone extension.

Flexible postural kyphosis demonstrating correction.
Clinical presentation of severe thoracic kyphosis.
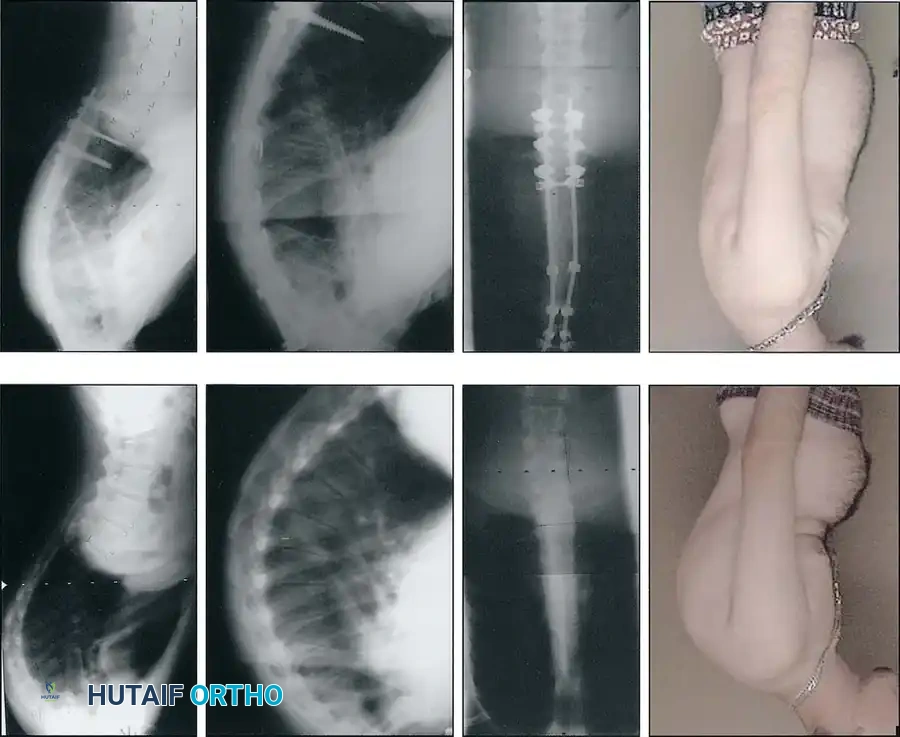
Clinical presentation demonstrating compensatory lumbar hyperlordosis.
Tightness of the hamstring and pectoral muscles is a nearly universal finding. Furthermore, minimal structural scoliosis (10 to 20 degrees) is present in up to 30% of patients. Neurological deficits are exceedingly rare but can occur secondary to severe apical angulation, thoracic disc herniation, or epidural cysts. Any signs of hyperreflexia, myelopathy, or lower extremity weakness mandate an immediate MRI.
RADIOGRAPHIC EVALUATION
Standard radiographic assessment requires full-length, standing posteroanterior (PA) and lateral spine radiographs on 36-inch cassettes.
The diagnostic criteria for typical Scheuermann disease include:
1. Thoracic kyphosis > 50 degrees.
2. Anterior wedging of > 5 degrees in at least three adjacent apical vertebrae.
3. Vertebral endplate irregularities and Schmorl nodes.

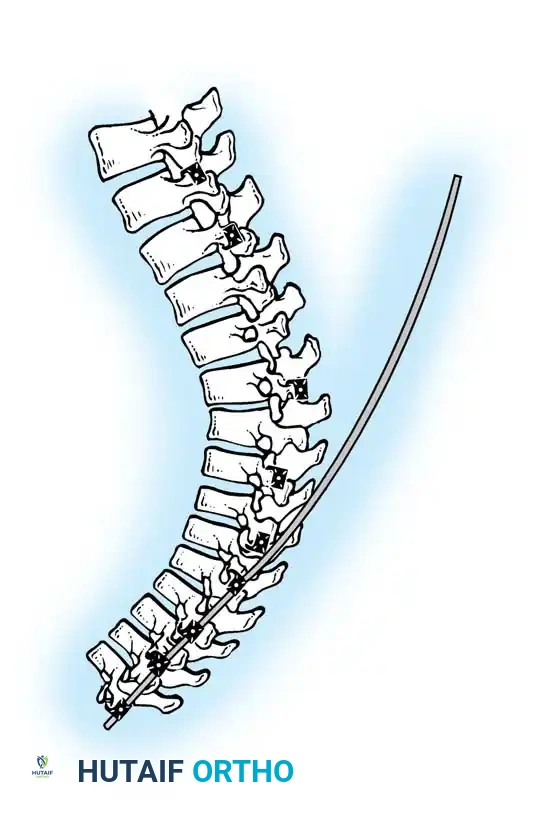
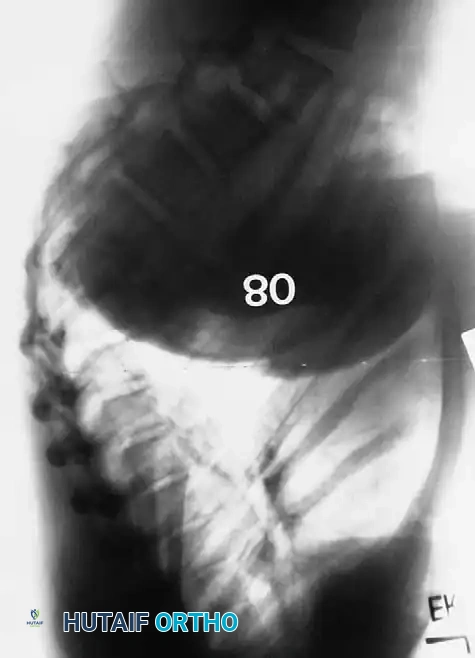
Lateral radiograph demonstrating classic Scheuermann kyphosis with severe anterior wedging and Schmorl nodes.
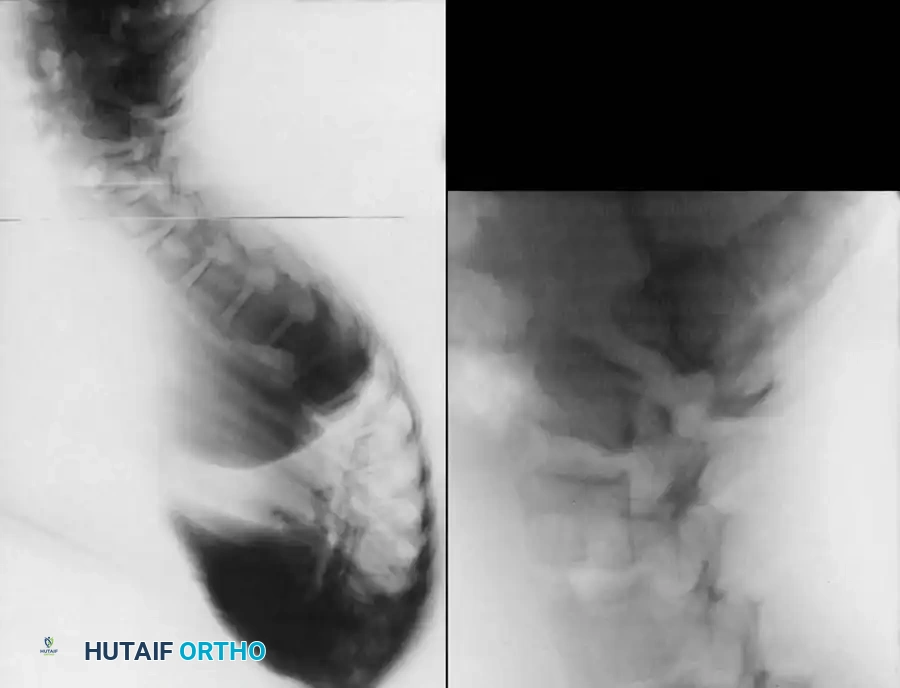
Preoperative lateral radiograph highlighting the rigid structural curve.
Detailed view of apical vertebral wedging and endplate destruction.
A lateral radiograph taken with the patient hyperextended over a bolster is critical to assess the flexibility of the curve and to aid in preoperative planning.
Two primary curve patterns exist in typical thoracic Scheuermann disease:
* Type I (Classic): Extends from T1/T2 to T12/L1, with the apex between T6 and T8.
* Type II (Thoracolumbar): Extends from T4/T5 to L2/L3, with the apex at the thoracolumbar junction. This pattern is generally more flexible but carries a higher risk of progression and chronic pain in adulthood.
NATURAL HISTORY
In the majority of cases, Scheuermann disease results in mild deformity and self-limiting symptoms. However, untreated curves can progress significantly during the adolescent growth spurt. Factors predicting progression include the magnitude of the curve at presentation, the number of wedged vertebrae, and the remaining years of skeletal growth (Risser sign).
Long-term studies (such as those by Murray, Weinstein, and Spratt) indicate that adults with untreated Scheuermann kyphosis (averaging 71 degrees) experience more intense back pain and loss of trunk extension compared to matched controls. However, this rarely leads to severe disability, and most patients adapt well without significant interference in their activities of daily living or occupational capacity. Restrictive pulmonary disease is generally only observed in curves exceeding 100 degrees.
OPERATIVE MANAGEMENT
While bracing (e.g., Milwaukee brace or custom TLSO) is the mainstay of treatment for skeletally immature patients with curves between 50 and 75 degrees, surgical intervention is indicated for specific, severe presentations.
Surgical Indications
- Curve Magnitude: Progressive kyphosis > 75 degrees.
- Pain: Intractable back pain unresponsive to conservative measures (physical therapy, NSAIDs, bracing).
- Cosmesis: Severe, unacceptable cosmetic deformity causing significant psychological distress.
- Neurological Deficit: Cord compression (rare).
- Curve Pattern: Thoracolumbar curves > 65 degrees, as they are highly prone to progression and chronic pain.
Preoperative Planning and Level Selection
Meticulous selection of the Upper Instrumented Vertebra (UIV) and Lower Instrumented Vertebra (LIV) is the most critical step in preventing postoperative complications, specifically Proximal Junctional Kyphosis (PJK) and Distal Junctional Kyphosis (DJK).
- UIV Selection: Must include the proximal end vertebra of the kyphosis, typically T2 or T3. Stopping at T4 or T5 in a high thoracic curve inevitably leads to PJK.
- LIV Selection: The LIV must extend past the distal end vertebra to include the first lordotic disc space. The sagittal plumb line from the UIV must fall posterior to the LIV. Failure to include the first lordotic disc is the primary cause of DJK and subsequent sagittal decompensation.
Surgical Warning: Never terminate a kyphosis construct at the apex of the lumbar lordosis or short of the stable sagittal vertebra. The LIV must be parallel to the sacrum on the standing lateral radiograph.
Surgical Approach: Posterior-Only vs. Anterior-Posterior
Historically, severe, rigid curves required an anterior release (via thoracotomy) followed by posterior instrumentation. However, with the advent of high-density pedicle screw constructs and posterior column osteotomies (Ponte osteotomies), the posterior-only approach has become the gold standard, offering equivalent correction with significantly reduced morbidity, blood loss, and pulmonary complications.
Step-by-Step Surgical Technique (Posterior Approach)
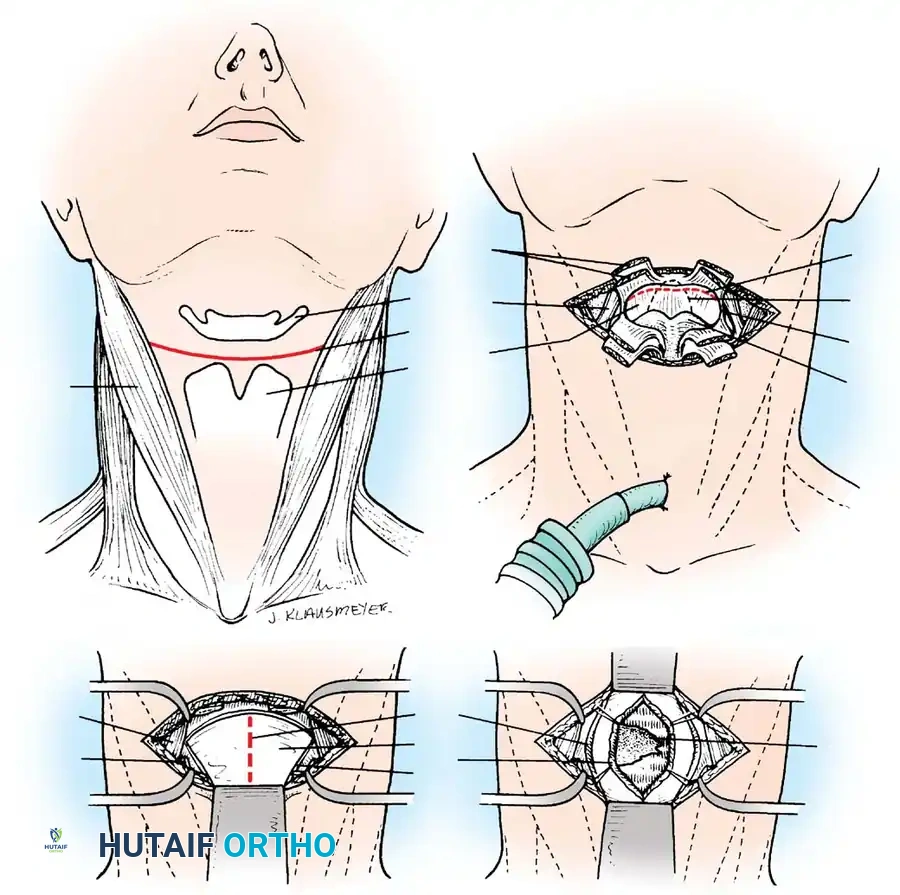
1. Positioning and Exposure
The patient is placed prone on a Jackson spinal table. Care is taken to pad all bony prominences. The abdomen must hang free to decrease intra-abdominal pressure, thereby reducing epidural venous bleeding. A standard midline posterior approach is utilized, exposing the spine subperiosteally from the UIV to the LIV, extending laterally to the tips of the transverse processes.
2. Facetectomies and Ponte Osteotomies
To mobilize the rigid deformity, wide, bilateral, multi-level Ponte osteotomies are performed at the apex of the curve.
* The inferior articular processes of the cranial vertebra and the superior articular processes of the caudal vertebra are resected.
* The ligamentum flavum is completely excised, exposing the dura.
* This posterior column shortening allows for 5 to 10 degrees of correction per level when the spine is extended.
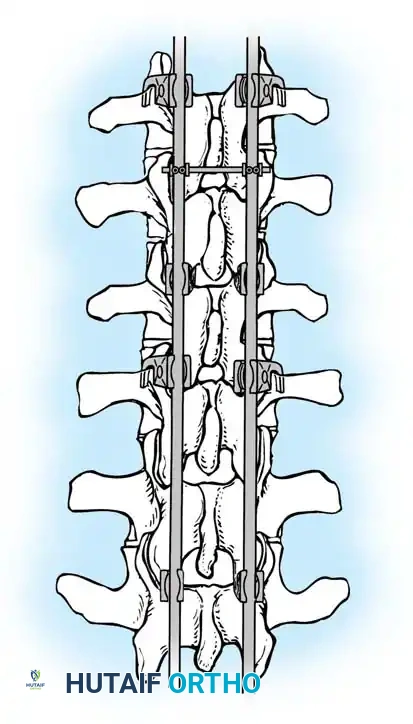
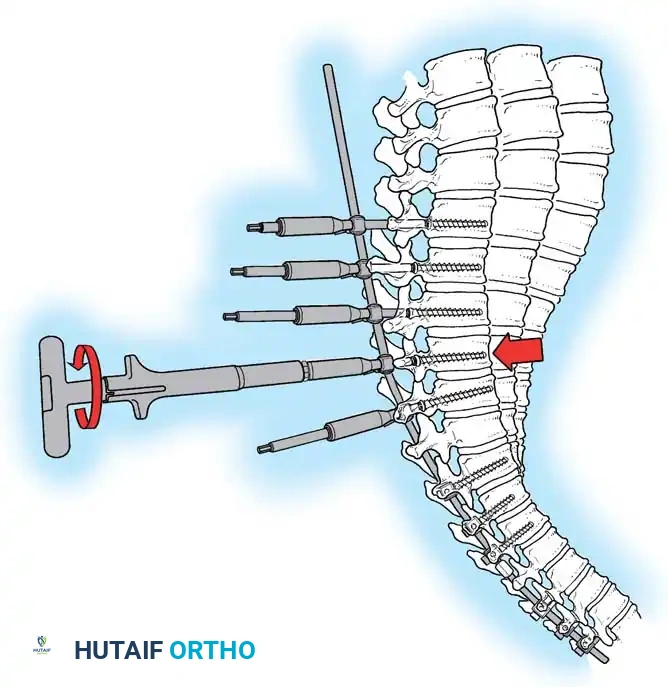
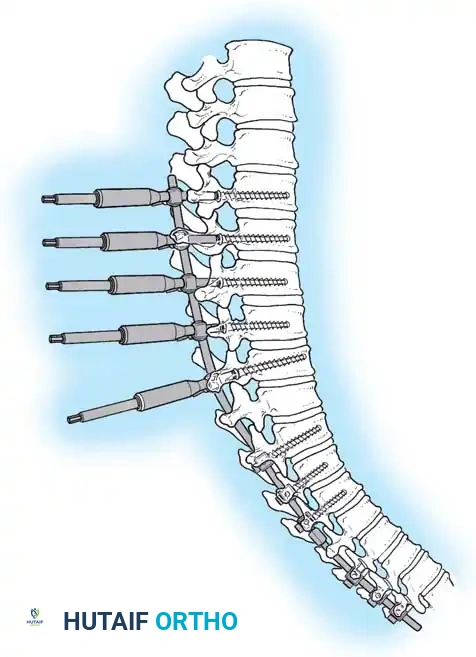
Diagram illustrating the placement of pedicle screws and the site of posterior column osteotomies.
3. Pedicle Screw Instrumentation
Free-hand or navigation-assisted pedicle screws are placed bilaterally. High implant density is crucial at the apex (to allow for powerful reduction forces) and at the cranial and caudal foundations (to prevent pullout).
4. Rod Contouring and Reduction
Two rigid rods (typically 5.5mm or 6.0mm Cobalt Chrome or Titanium) are meticulously contoured. The rods must be under-contoured relative to the patient's current deformity but over-contoured relative to the desired final physiological kyphosis (aiming for 40 degrees).
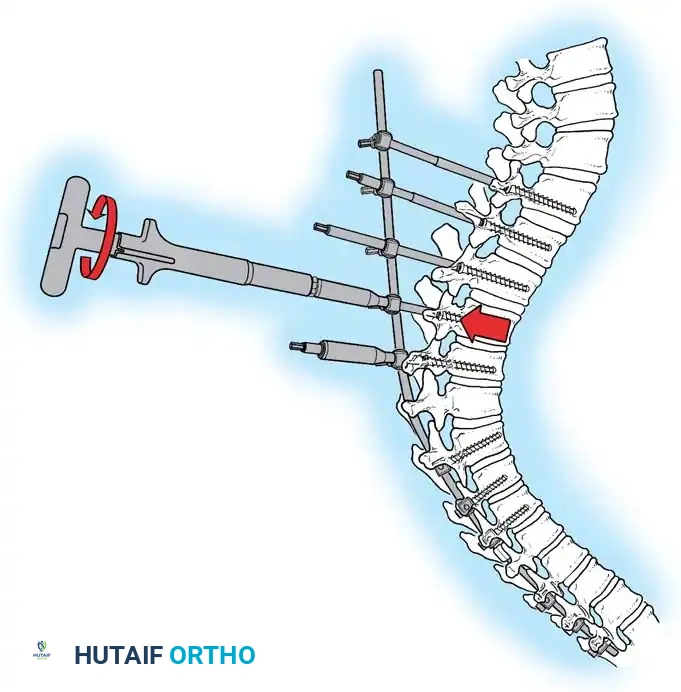
Insertion of the contoured rod into the pedicle screw construct.
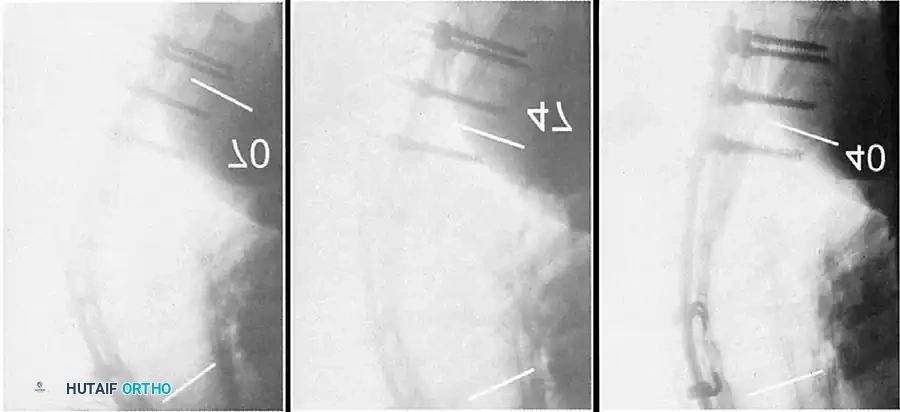
The reduction is achieved via a cantilever maneuver. The rods are seated in the distal foundation screws first. Using reduction tubes and set screws, the rod is sequentially drawn into the apical and proximal screws. This maneuver translates the spine to the rod, simultaneously correcting the kyphosis and restoring sagittal balance.

Cantilever reduction maneuver closing the posterior osteotomies and correcting the kyphotic deformity.
5. Apical Compression
Once the rods are seated, sequential compression is applied across the apical screws. This closes the Ponte osteotomies, shortens the posterior column, and acts as a fulcrum to lengthen the anterior column, effectively reversing the biomechanical pathology of Scheuermann disease.
6. Arthrodesis and Closure
Meticulous decortication of the posterior elements (laminae, transverse processes) is performed. Copious amounts of autograft (from the facetectomies) and allograft are packed into the lateral gutters to ensure a robust posterolateral fusion. The wound is closed in layers over subfascial drains.
Postoperative Radiographic Outcomes
Successful surgical intervention yields dramatic restoration of sagittal balance and correction of the deformity.
Postoperative AP radiograph demonstrating a well-aligned posterior pedicle screw construct.
Postoperative lateral radiograph showing excellent restoration of thoracic kyphosis and sagittal balance.

Postoperative AP radiograph of an extended construct.
Postoperative lateral radiograph demonstrating correction of a severe thoracolumbar curve.

Long-term follow-up lateral radiograph showing solid arthrodesis and maintenance of correction.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Rehabilitation
With modern rigid pedicle screw constructs, postoperative bracing is generally unnecessary. Patients are mobilized on postoperative day one with physical therapy. Bending, lifting, and twisting are restricted for the first 3 months. Return to non-contact sports is typically permitted at 6 months, with full unrestricted activity at 1 year pending radiographic evidence of solid fusion.
Complications
- Junctional Kyphosis (PJK/DJK): The most common complication, occurring in up to 20-30% of cases. It is mitigated by meticulous level selection, avoiding over-correction of the apex (do not correct > 50% of the original curve magnitude), and preserving the interspinous ligaments at the UIV and LIV.
- Neurological Deficit: The risk of spinal cord injury during correction is approximately 0.5%. Continuous intraoperative neuromonitoring (SSEPs and MEPs) is mandatory. If signals drop during the cantilever reduction, the correction must be immediately released, and mean arterial pressure (MAP) increased.
- Infection and Wound Dehiscence: Mitigated by meticulous closure, prophylactic antibiotics, and intrawound vancomycin powder.
- Implant Failure/Pseudarthrosis: Rare with modern high-density constructs and thorough decortication, but requires revision if symptomatic.
In conclusion, the operative management of Scheuermann kyphosis is a highly effective intervention for severe, progressive, or painful deformities. Mastery of sagittal plane biomechanics, precise preoperative planning, and rigorous execution of posterior column osteotomies are essential for achieving optimal, long-lasting clinical outcomes.
📚 Medical References
- Scheuermann kyphosis, J Bone Joint Surg 75A:236, 1993.
- Neithard FV: Scheuermann’s disease and spondylolysis, Orthop Trans 7:103, 1983.
- Ogilvie JW, Sherman J: Spondylolysis in Scheuermann’s disease, Spine 12:251, 1987.
- Ponseti IV, Friedman B: Changes in the scoliotic spine after fusion, J Bone Joint Surg 32A:751, 1950.
- Ponte A, Gebbia F, Eliseo F: Nonoperative treatment of adolescent hyperkyphosis, Orthop Trans 9:108, 1985.
- Ryan MD, Taylor TKF: Acute spinal cord compression in Scheuermann’s disease, J Bone Joint Surg 64B:409, 1982.
- Sachs BL, Bradford DS, Winter RB, et al: Scheuermann’s kyphosis: follow-up of Milwaukee-brace treatment, J Bone Joint Surg 69A:50, 1987.
- Scheuermann H: Kyphosis dorsalis juvenile, Ztschr Orthop Chir 41:305, 1921.
- Schmorl G: Die Pathogenese der juvenilen Kyphose, Fortschr Geb Roentgenstr Nuklearmed 41:359, 1930.
- Scoles PV, Latimer BM, Digiovanni BF: Vertebral alterations in Scheuermann’s kyphosis, Spine 16:509, 1991.
- Shuffl ebarger HL: Clinical issue: rod rotation in scoliosis surgery, Warsaw, Ind, 1994, DePuy Motech. Shuffl ebarger HL: The theory of the segmental approach to spinal instrumentation: a defi nitive method of planning spinal instrumentation for every spinal pathology, Warsaw, Ind, 1994, DePuy Motech. Shuffl ebarger HL, Harms J: Moss Miami three-dimensional spinal instrumentation: surgical technique, Warsaw, Ind, 1994, DePuy Motech. Shuffl ebarger HL, Harms J: Moss Miami three-dimensional spinal instrumentation: taking spinal instrumentation to a new dimension, Warsaw, 1994, DePuy Motech. Singh M, Nagrath AR, Maini PS: Changes in trabecular pattern of the upper end of the femur as an
You Might Also Like