Comprehensive Evaluation of Spinal Injury: A Clinical Guide
Key Takeaway
The evaluation of spinal injury requires a meticulous, systematic approach rooted in Advanced Trauma Life Support (ATLS) principles. A high index of suspicion must be maintained, particularly in polytrauma patients or those with distracting injuries. This comprehensive guide details the critical steps of historical assessment, rigorous physical and neurological examinations utilizing the ASIA impairment scale, and advanced radiographic clearance protocols essential for preventing secondary neurological deterioration and optimizing patient outcomes.
INTRODUCTION TO SPINAL INJURY EVALUATION
The evaluation of a patient with a suspected spinal injury is one of the most critical and high-stakes scenarios in orthopedic trauma. A missed spinal fracture or an unrecognized unstable ligamentous injury can lead to catastrophic, irreversible neurological deficits. The initial assessment must be strictly governed by Advanced Trauma Life Support (ATLS) protocols, prioritizing airway, breathing, and circulation while maintaining rigid in-line cervical immobilization.
The primary objective during the evaluation phase is to identify structural instability, document the exact baseline neurological status, and prevent secondary spinal cord injury caused by hypoxia, hypotension, or mechanical manipulation. This masterclass provides an exhaustive, evidence-based framework for the clinical and radiographic evaluation of spinal trauma, designed for orthopedic residents, fellows, and practicing consultants.
HISTORY AND MECHANISM OF INJURY
Obtaining a detailed history regarding the mechanism of injury is paramount, though frequently unobtainable directly from the patient at the initial presentation due to altered mental status, intubation, or concomitant severe trauma. In such cases, emergency medical services (EMS) personnel and witnesses are invaluable sources of information.
The most common etiologies of severe spinal trauma include motor vehicle collisions (MVCs), high-energy falls, diving accidents, and penetrating trauma (e.g., gunshot wounds).
Clinical Pearl: Spinal injury must be suspected in any patient presenting with a head injury, severe facial fractures, or scalp lacerations. The biomechanical forces required to fracture the cranium or facial skeleton are routinely transmitted to the cervical spine.
In any patient with recent trauma, complaints of neck pain or thoracolumbar pain must be considered indicative of a spinal fracture until definitively proven otherwise. Lee et al. identified several critical risk factors associated with occult spinal injuries. These include:
* Inability to accurately assess neck pain due to a secondary distracting injury (e.g., femur fracture, visceral trauma).
* Abnormal neurological findings on initial survey.
* A history of transient neurological symptoms (e.g., burning hands syndrome, transient quadriparesis) at the scene.
* Physical signs of direct spinal trauma, such as ecchymosis, abrasions, or seatbelt signs over the torso.
* An unreliable clinical examination (due to intoxication, traumatic brain injury, or language barriers).
* Significant head or maxillofacial trauma.
* An inconsolable pediatric patient.
If the cervical spine is not already rigidly immobilized in a patient exhibiting any of these risk factors, a rigid cervical collar must be applied immediately before the physical examination proceeds. While Lee et al.'s foundational study focused on young children, these rigorous recommendations are universally applicable to older children, adolescents, and adults.
SYSTEMATIC PHYSICAL EXAMINATION
A comprehensive general physical examination is conducted with the patient in the supine position, strictly adhering to spinal precautions. The patient’s mental status and Glasgow Coma Scale (GCS) score must be assessed and documented immediately, as this dictates the pathway for spinal clearance.
Cranial and Maxillofacial Assessment
The head must be meticulously examined for lacerations, contusions, and palpable step-offs indicative of skull fractures. The facial skeleton is palpated for instability. The external auditory canals must be inspected using an otoscope to rule out hemotympanum or the leakage of cerebrospinal fluid (CSF), which strongly suggests a basilar skull fracture and raises the index of suspicion for upper cervical spine trauma (occipitoatlantal or atlantoaxial dissociation).
Spinal Palpation and Inspection
The entire spine must be palpated from the inion to the sacrum. This requires a coordinated log-roll maneuver, utilizing a minimum of four trained personnel to maintain strict in-line stabilization of the neuroaxis.
During the log-roll, the spinous processes are palpated for tenderness, step-offs, or crepitus. A painful spinous process is a primary indicator of a spinal injury. Furthermore, palpable defects or widening in the interspinous ligaments strongly suggest disruption of the posterior ligamentous complex (PLC), a critical determinant of spinal stability.
Surgical Warning: Any complaint of pain or tenderness upon palpation of the cervical spine mandates continued rigid collar immobilization. If a patient arrives with a collar in place, active or passive neck motion must never be evaluated until the spine is radiographically and clinically cleared.
Neck motion should only be assessed after the patient reports zero pain or tenderness during the static examination. An assistant must hold the head steady in a neutral position while the torso, thoracic, lumbar, and sacral regions are exposed for inspection.
Hemodynamic Assessment: Neurogenic vs. Hypovolemic Shock
The patient's hemodynamic status provides vital clues regarding spinal cord integrity. Initial blood pressure may be profoundly decreased without a compensatory tachycardia. This phenomenon, known as neurogenic shock, results from the loss of sympathetic tone due to a cervical or high thoracic spinal cord injury.
* Neurogenic Shock: Hypotension accompanied by bradycardia and warm, flushed extremities.
* Hypovolemic Shock: Hypotension accompanied by tachycardia and cold, clammy extremities.
Bradycardia or episodes of asystole may be the only presenting signs of a severe injury to the axial region of the cervical spine due to unopposed vagal tone.
Prevention of Decubitus Ulcers
While the spine must be protected during the initial assessment, prolonged immobilization on a rigid spine board is highly detrimental. Once a spinal cord injury has been identified or ruled out, and appropriate precautions (such as a rigid collar or log-roll protocols) are established, the patient must be removed from the rigid extrication board as rapidly as possible to prevent the rapid development of decubitus ulcers, which can complicate future surgical approaches.
DETAILED NEUROLOGICAL EVALUATION
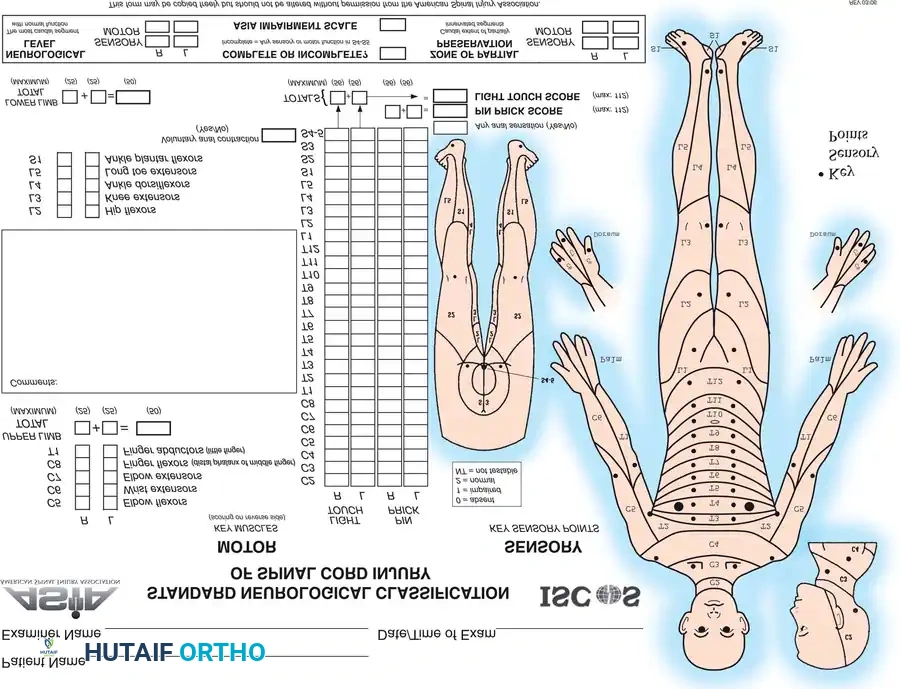
Bohlman, Stauffer, and Meyer have all extensively documented that an accurate, meticulous, and repeatable neurological evaluation is the cornerstone of spinal trauma management. The American Spinal Injury Association (ASIA) Impairment Scale is the universal gold standard for organizing and communicating this evaluation.
Mental Status and Cranial Nerves
The level of consciousness is determined using the Glasgow Coma Scale (GCS). Pupillary size and reactivity must be documented. An expanding epidural or subdural hematoma, or a depressed skull fracture, can cause progressive neurological deterioration that may mask or complicate the assessment of a spinal cord injury.
Table: Glasgow Coma Scale (GCS)
* Eyes Open: Spontaneous (4), To sound (3), To pain (2), Never (1).
* Best Verbal Response: Oriented (5), Confused (4), Inappropriate words (3), Incomprehensible sounds (2), None (1).
* Best Motor Response: Obeys commands (6), Localizes pain (5), Flexion withdrawal (4), Abnormal flexion/decorticate (3), Extension/decerebrate (2), None (1).
Sensory Examination
Sensory testing is performed bilaterally using light touch (assessing the dorsal columns) and pinprick with a sterile needle (assessing the spinothalamic tracts). Pinwheels are strictly avoided to prevent the transmission of bloodborne pathogens. Testing begins at the head and neck and progresses distally across specific dermatomes.
Key dermatomal landmarks include:
* C5: Lateral aspect of the antecubital fossa.
* C6: Dorsal surface of the proximal phalanx of the thumb.
* C7: Dorsal surface of the proximal phalanx of the middle finger.
* C8: Dorsal surface of the proximal phalanx of the little finger.
* T4: Nipple line.
* T7: Xiphoid process.
* T10: Umbilicus.
* T12/L1: Inguinal ligament region.
* S2, S3, S4: Perineum and perianal region.
The skin should be marked with a surgical pen where sensation transitions from absent to present.
Motor Examination
Motor strength is graded on a scale of 0 to 5 and examined sequentially, beginning with the upper extremities. It is critical to differentiate between a complete spinal cord injury, an incomplete spinal cord injury, and an isolated nerve root lesion. For instance, a unilateral dislocated facet in the cervical spine may produce an isolated C6 nerve root paralysis, whereas a central cord syndrome will present with bilateral weakness, typically worse in the upper extremities than the lower.
Key Muscle Groups for ASIA Motor Evaluation:
* C5: Elbow flexors (biceps, brachialis).
* C6: Wrist extensors (extensor carpi radialis longus/brevis).
* C7: Elbow extensors (triceps).
* C8: Finger flexors (flexor digitorum profundus to the middle finger).
* T1: Small finger abductors (abductor digiti minimi).
* L2: Hip flexors (iliopsoas).
* L3: Knee extensors (quadriceps).
* L4: Ankle dorsiflexors (tibialis anterior).
* L5: Long toe extensors (extensor hallucis longus).
* S1: Ankle plantarflexors (gastrocnemius, soleus).
Sacral Sparing and Complete vs. Incomplete Injury
The most critical distinction in the neurological exam is determining if the injury is complete or incomplete. This is defined entirely by the presence or absence of sacral sparing.
Motor and sensory evaluation of the rectum and perirectal area is mandatory. Evidence of sacral sensory sparing (perianal sensation to light touch or pinprick) or sacral motor sparing (voluntary contraction of the external anal sphincter or voluntary toe flexion) establishes the diagnosis of an incomplete spinal cord injury. If voluntary contraction of sacrally innervated muscles is present alongside sacral sensation, the prognosis for meaningful neurological recovery is significantly improved.
Conversely, if there is absolutely no motor or sensory function preserved in the S4-S5 sacral segments once spinal shock has resolved, the injury is classified as complete (ASIA A), and the prognosis for distal recovery is exceedingly poor.
Reflexes and Spinal Shock
Deep tendon reflexes and pathological reflexes must be assessed. Paralyzed patients in the acute phase are usually areflexic due to spinal shock. It is vital to note that a triple-flexion withdrawal response of the legs to a painful stimulus is a spinal reflex arc and does not indicate voluntary motor control.
Hyperreflexia, sustained clonus, and pathological reflexes (such as a positive Babinski sign in the lower extremities or a Hoffmann sign in the upper extremities) indicate upper motor neuron lesions and chronic spinal cord compression.
Spinal Shock Resolution:
Spinal shock is a state of transient physiological (rather than anatomical) reflex depression of cord function below the level of injury. It typically resolves within 24 to 48 hours but can persist longer. The end of spinal shock is heralded by the return of the bulbocavernosus reflex or the anal wink reflex.
- Bulbocavernosus Reflex: Elicited by squeezing the glans penis or applying traction to the Foley catheter while performing a digital rectal examination. A reflex contraction of the anal sphincter indicates an intact S2-S4 reflex arc and the termination of spinal shock.
- Anal Wink Reflex: A visible contraction of the anal sphincter in response to a pinprick stimulus applied to the perianal skin.
If the bulbocavernosus reflex returns and there is still no voluntary motor or sensory function below the level of injury, the diagnosis of a complete spinal cord injury is confirmed.
RADIOGRAPHIC AND IMAGING EVALUATION
Radiographic evaluation must be systematic and protocol-driven. The initial ATLS radiographic series for a polytrauma patient includes a lateral view of the cervical spine, an anteroposterior (AP) view of the chest, and an AP view of the pelvis.
Plain Radiography
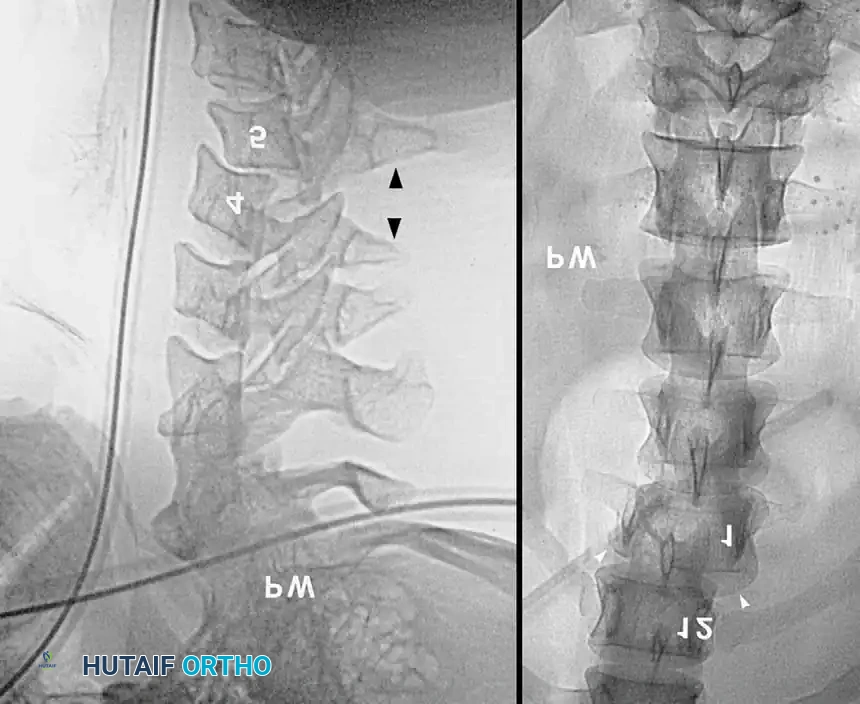
When utilizing plain films, the lateral cervical spine radiograph must visualize the entire cervical spine down to the superior endplate of T1. The most frequently missed cervical spine fractures on plain radiographs occur at the extremes of the cervical spine: the odontoid process (C2) and the cervicothoracic junction (C7-T1). If T1 cannot be visualized due to shoulder shadow, a Swimmer's view or, preferably, a CT scan is mandatory.

A standard non-trauma radiographic series of the injured neck includes AP, lateral, and bilateral oblique projections, taken with the patient strictly immobilized.
Prevertebral Soft Tissue Swelling:
Weir established classical criteria for evaluating the cervical spine, highlighting the prevertebral soft-tissue shadow. Historically, this shadow should not exceed 5 mm in width at the anteroinferior border of C3. A width exceeding 5 mm suggests hemorrhage and edema secondary to a fracture or ligamentous disruption.
However, modern evidence has challenged the reliability of this metric. Herr et al., in a study of 212 patients, demonstrated that prevertebral soft-tissue measurement at C3 is an insensitive marker for cervical spine fractures or dislocations and does not reliably correlate with the location or mechanism of injury. Furthermore, the loss of the normal cervical lordotic curve is often due to muscular spasm and is not, in isolation, definitive evidence of structural injury.
Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
Due to the limitations of plain radiography, high-resolution Computed Tomography (CT) with sagittal and coronal reconstructions has become the gold standard for the initial osseous evaluation of the spine in trauma centers. CT provides unparalleled detail of bony architecture, facet joint alignment, and the presence of retropulsed bone fragments within the spinal canal.
If a patient is unconscious, obtunded, or uncooperative, clinical clearance of the cervical spine is impossible. In these scenarios, a normal CT scan of the C-spine (C1-T1) is highly reliable for ruling out unstable osseous injuries. However, if the patient remains comatose or if there is a high suspicion of a purely ligamentous injury, spinal cord contusion, or epidural hematoma, Magnetic Resonance Imaging (MRI) is the definitive modality. MRI is exquisitely sensitive for evaluating the posterior ligamentous complex, intervertebral discs, and the spinal cord parenchyma itself.
CONCLUSION AND SURGICAL DECISION-MAKING
The evaluation of a spinal injury is a dynamic, continuous process that bridges the gap between the trauma bay and the operating theater. A rigorous adherence to ATLS principles, combined with a meticulous ASIA neurological examination and advanced cross-sectional imaging, ensures that unstable injuries are rapidly identified.
Once an injury is fully characterized, the orthopedic spine surgeon can formulate a definitive treatment plan. Whether the indication calls for closed reduction and halo-vest immobilization, or urgent open reduction, decompression, and rigid internal fixation, the success of the intervention is entirely predicated on the accuracy and thoroughness of the initial clinical evaluation.
You Might Also Like


