Comprehensive Management of Spinal Infections: Nonoperative Protocols and Surgical Principles
Key Takeaway
The management of spinal infections requires a multidisciplinary approach, balancing targeted antimicrobial therapy with mechanical stabilization. While nonoperative treatment—comprising culture-specific intravenous antibiotics and orthotic immobilization—remains the primary modality, surgical intervention is mandated for progressive neurological deficits, epidural abscesses, or structural instability. Accurate diagnosis via MRI and image-guided biopsy is critical to optimizing clinical outcomes and preventing catastrophic complications such as paralysis or severe kyphotic deformity.
PRINCIPLES OF NONOPERATIVE TREATMENT
The traditional treatment of spinal infection has historically relied upon prolonged bed rest and rigid immobilization. While these principles remain the foundational mainstay of conservative care, modern orthotic advancements have largely replaced the cumbersome body cast with removable, custom-molded thoracolumbosacral orthoses (TLSO) or body jackets in compliant patients.
The cornerstone of nonoperative management is targeted, culture-specific antimicrobial therapy. Empirical treatment should be avoided until a definitive microbiological diagnosis is established via blood cultures or image-guided biopsy, except in cases of fulminant sepsis or rapid neurological decline.
Pharmacokinetics and Antibiotic Penetration
Selecting the appropriate antibiotic requires an understanding of the unique avascular microenvironment of the intervertebral disc and the surrounding necrotic bone. Specific antibiotics that demonstrate excellent serum bactericidal activity may fail to achieve minimum inhibitory concentrations (MIC) within the spinal axis.
Clinical Pearl: Eismont et al. demonstrated that 1 hour post-injection, cephalothin was undetectable in the intervertebral disc, penetrating to less than 4% of serum values. Conversely, clindamycin and tobramycin achieved greater than 50% of serum levels within the same timeframe.
Furthermore, Gibson et al. confirmed these pharmacokinetic limitations in pediatric populations undergoing anterior spinal surgery, noting that neither flucloxacillin nor cephradine was identifiable in the discs despite therapeutic serum concentrations in adjacent tissues.
Duration of Therapy and Monitoring
The optimal duration of antibiotic therapy remains highly variable and patient-specific. Intravenous (IV) antibiotics are typically administered for a minimum of 6 weeks. Transition to oral suppressive therapy is dictated by clinical response and the normalization of acute-phase reactants, primarily the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP).
Collert established the paradigm that antimicrobial therapy must continue until the ESR returns to baseline. Failure of the ESR to normalize, or the persistence of mechanical back pain and radiculopathy, should immediately prompt a reevaluation. This may necessitate a repeat percutaneous biopsy or an open biopsy to obtain fresh cultures and debride sequestered, necrotic material.
While home IV antibiotic therapy has revolutionized outpatient management, it carries a significant risk of late pathological fracture of the infected, mechanically compromised vertebrae. If ambulatory therapy is selected, rigorous patient education and close radiographic monitoring are mandatory.
PROGNOSIS AND BIOMECHANICAL COMPLICATIONS
Even in cases where an absolute microbiological diagnosis remains elusive, the natural history of most spinal infections involves symptomatic and radiographic resolution within 9 to 24 months of onset. However, the prognosis is heavily contingent upon the host's immune status and the structural integrity of the spinal column.
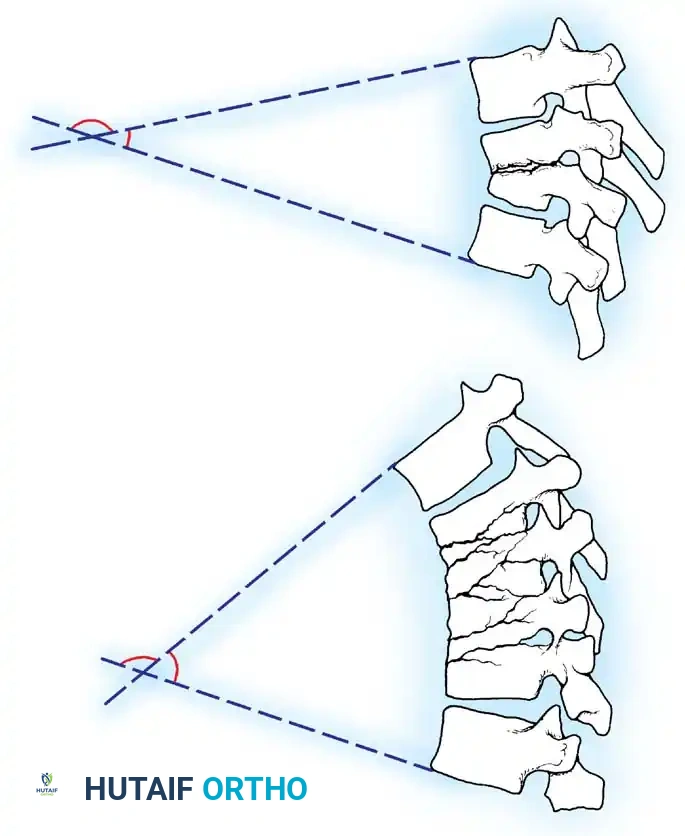
Recurrence of infection is a persistent threat, particularly during periods of transient immunosuppression. The most devastating delayed complications include progressive kyphosis, paralysis, and myelopathy.
These catastrophic risks peak during the "soft bone" phase—the period when the active infection is microbiologically controlled, but the osteomyelitic bone remains structurally deficient. During this vulnerable window, the healing process has not yet advanced to the point of solid neo-osteogenesis or spontaneous arthrodesis around the infected tissue, making the spine highly susceptible to axial collapse and angular deformity.
SPECIFIC INFECTIONS AND PATHOGENESIS
Pyogenic Vertebral Osteomyelitis
The vertebral column is involved in 0.15% to 3.9% of all osteomyelitis cases. Epidemiological data from Digby and Kersley indicate an incidence of 1 in 250,000 individuals annually. The demographic distribution skews heavily toward adult males (55% to 75% incidence), with a peak age of onset between 45 and 65 years.
Staphylococcus aureus remains the most ubiquitous pathogen. However, specific patient populations exhibit unique microbiological profiles; for instance, intravenous drug abusers (IVDU) have a markedly higher propensity for Pseudomonas aeruginosa infections. Eismont et al. noted that S. aureus infections carry the highest risk of progressing to epidural extension and subsequent paralysis.
Pediatric Discitis
Pediatric discitis presents a unique clinical entity, characterized by a triad of fever, elevated ESR, and delayed disc space narrowing on plain radiographs (typically visible 4 to 6 weeks post-onset). The average age of onset is 6 to 7 years.
Clinical Presentation:
* Refusal to walk or crying during ambulation.
* Loss of normal lumbar lordosis; the child holds the spine rigidly erect.
* Hamstring tightness and vague abdominal pain (often leading to misdiagnosis in older children).
* Neurological deficits are exceedingly rare but highly ominous.
Diagnostic Imaging:
Plain radiographs are notoriously insensitive in the acute phase. Magnetic Resonance Imaging (MRI) with gadolinium contrast is the gold standard, offering the highest sensitivity and specificity. Alternatively, a combination of Technetium-99m bone scanning and Gallium-67 scanning can provide early indications of inflammatory processes.
Treatment Controversies:
The management of pediatric discitis is highly debated:
* Conservative Isolation: Spiegel et al. and Boston et al. historically recommended bed rest and immobilization without antibiotics, arguing a self-limiting or viral etiology in very young children (<6 years).
* Antimicrobial Protocol: Wenger et al. advocated for blood cultures followed by immediate IV antibiotics until the child is pain-free and ambulatory, followed by 3 weeks of oral therapy.
Spontaneous interbody fusion occurs in approximately 25% of pediatric patients. Aggressive surgical debridement is rarely indicated unless the patient presents with caseating granulomatous disease (e.g., Tuberculosis) or an epidural abscess causing neurological compromise.
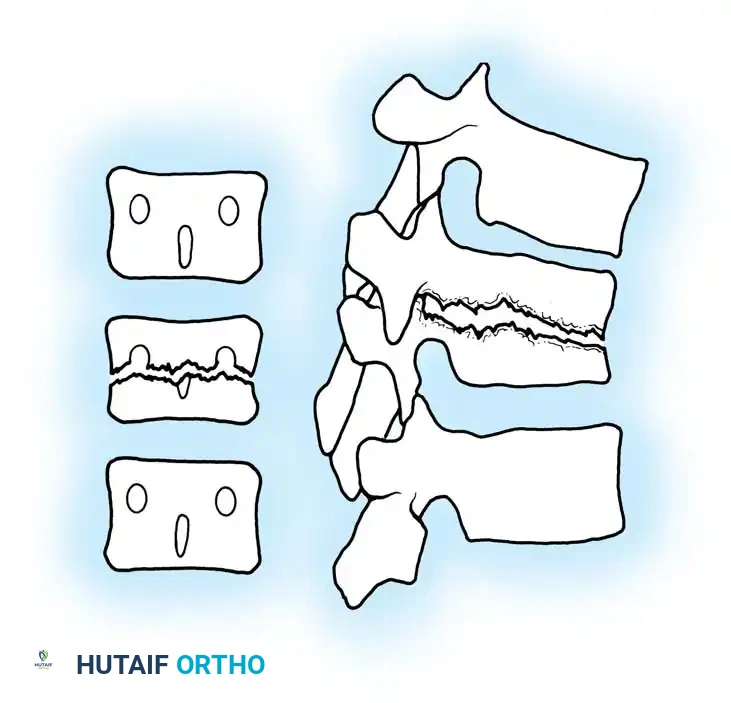
Adult Disc Space Infection
Unlike the pediatric spine, the adult intervertebral disc is entirely avascular. Consequently, primary hematogenous disc space infection is virtually impossible without preceding vertebral endplate osteomyelitis. True isolated disc space infections in adults are almost exclusively iatrogenic, resulting from direct penetrating trauma such as surgical discectomy or discography.
The incidence of postoperative discitis ranges from 1% to 2.8% following open disc surgery, and 0.5% to 1% following discography. S. aureus is the predominant organism.
Diagnosis is frequently delayed due to the confounding presence of expected postoperative back pain. However, the persistence of severe, unrelenting muscle spasm, inability to mobilize, and an ESR that fails to normalize 4 to 6 weeks postoperatively are highly indicative of infection. MRI is the modality of choice for rapid identification. Treatment consists of rigid orthotic immobilization and prolonged culture-specific antibiotics until the ESR normalizes and spontaneous intervertebral fusion occurs (typically 8 to 24 months).
EPIDURAL SPACE INFECTIONS AND ABSCESSES
Spinal epidural abscesses (SEA) are rare but potentially lethal, with an incidence of 0.2 to 1.2 cases per 10,000 hospital admissions. The morbidity and mortality rates are exceptionally high, particularly in immunosuppressed cohorts.
Pathoanatomy and Clinical Progression
An epidural abscess typically spans three to five vertebral segments. The longitudinal and circumferential extension is dictated by the intricate anatomy of the spinal canal. Hogan's cryomicrotome studies demonstrated that the epidural fat and venous plexus are discontinuous, which somewhat compartmentalizes the infection.
Abscesses arising from direct extension of vertebral osteomyelitis are almost universally located in the ventral (anterior) epidural space, directly compressing the thecal sac.
The clinical presentation is far more acute than isolated osteomyelitis:
1. Rapid onset of neurological symptoms (progressing over days, not weeks).
2. Acute, high-grade febrile illness.
3. Meningeal irritation (positive straight leg raise, nuchal rigidity).
Surgical Warning: The classic progression of SEA is sequential: generalized spinal ache $\rightarrow$ radicular pain $\rightarrow$ motor weakness $\rightarrow$ irreversible paralysis. This entire cascade can occur within 7 to 10 days.
Management Strategies: Medical vs. Surgical
The etiology of neurological impairment in SEA is debated, with theories split between direct mechanical compression (Feldenzer et al.) and secondary septic thrombophlebitis causing vascular ischemia.
Nonoperative Management:
Savage et al. demonstrated that medical management (IV antibiotics and close observation) is a viable alternative only for highly selected patients who present solely with axial back pain or whose neurological deficits have been completely stable for >72 hours. Any hint of neurological deterioration mandates emergent surgical decompression.
Surgical Decompression:
Heusner established that early decompression—performed before the onset of profound paralysis or within 36 hours of initial motor weakness—yields a >50% chance of complete neurological recovery.
SURGICAL INTERVENTION: INDICATIONS AND APPROACHES
When nonoperative management fails, or when specific high-risk criteria are met, surgical intervention becomes the definitive standard of care. The goals of surgery are threefold: radical debridement of infected tissue, decompression of neural elements, and restoration of biomechanical stability.
Indications for Surgery
- Progressive neurological deficit (e.g., evolving myelopathy, cauda equina syndrome).
- Spinal instability or progressive kyphotic deformity.
- Failure of medical management (persistent bacteremia, rising ESR/CRP despite appropriate IV antibiotics).
- Large epidural abscesses causing critical central canal stenosis.
- Intractable pain secondary to structural collapse.
- Need for open biopsy when percutaneous methods yield negative cultures.
Surgical Approaches and Techniques
The selection of the surgical approach is dictated entirely by the anatomical location of the pathology.
Surgical Pitfall: Laminectomy is strictly contraindicated in patients with ventral (anterior) osteomyelitis and secondary epidural abscess. Removing the posterior tension band in the presence of an anterior column defect will inevitably result in catastrophic iatrogenic destabilization, rapid kyphotic collapse, and worsening neurological injury.
1. Posterior Approach (Laminectomy and Instrumentation)
- Indications: Isolated dorsal (posterior) epidural abscesses, isolated facet joint pyarthrosis, or subdural/spinal cord abscesses.
- Technique: The patient is positioned prone on a Jackson table. A standard midline incision is made. Bilateral subperiosteal dissection exposes the posterior elements. A wide laminectomy is performed over the affected levels to evacuate the purulent collection. The epidural space is copiously irrigated with pulsatile lavage. If the posterior elements are structurally compromised, pedicle screw instrumentation is placed to bridge the defect, followed by posterolateral bone grafting.
2. Anterior Approach (Corpectomy and Strut Grafting)
- Indications: Ventral epidural abscesses, extensive vertebral body osteomyelitis, and anterior column collapse.
- Technique (Thoracolumbar):
- Positioning: Lateral decubitus position.
- Approach: A retroperitoneal or transthoracic approach is utilized depending on the level. The segmental vessels are ligated to mobilize the great vessels (aorta/vena cava) away from the infected spine.
- Debridement: A radical corpectomy is performed. All necrotic bone, infected disc material, and epidural purulence are meticulously excised back to bleeding, healthy cancellous bone. The posterior longitudinal ligament (PLL) is often resected to ensure complete decompression of the ventral thecal sac.
- Reconstruction: The anterior column defect is reconstructed using a structural autograft (e.g., tricortical iliac crest, fibula) or a titanium mesh cage packed with autologous bone.
- Stabilization: Anterior plating or supplemental posterior pedicle screw fixation is applied to provide rigid biomechanical stability, which is essential for infection eradication and successful arthrodesis.
Postoperative Protocols
Postoperative care requires seamless integration between orthopedic surgery and infectious disease specialists.
* Antimicrobial Therapy: IV antibiotics are continued for a minimum of 6 weeks postoperatively, tailored to intraoperative deep tissue cultures.
* Immobilization: Depending on the rigidity of the internal fixation, patients may be mobilized in a custom TLSO brace for 3 to 6 months to protect the structural graft until radiographic union is achieved.
* Surveillance: Serial inflammatory markers (ESR, CRP) are drawn weekly. Follow-up radiographs are obtained at 6 weeks, 3 months, and 6 months to monitor for graft subsidence, hardware failure, or progressive deformity. MRI is reserved for cases of suspected clinical recurrence or new neurological symptoms.
You Might Also Like


