Circulation of the Spinal Cord and Anterior Surgical Approaches: A Comprehensive Masterclass
Key Takeaway
A comprehensive understanding of spinal cord circulation is paramount for spine surgeons. The arterial supply relies on segmental vessels and the critical Artery of Adamkiewicz, while venous drainage occurs via the valveless Batson plexus. Mastering this vascular anatomy minimizes ischemic complications during anterior spinal approaches. This guide details the biomechanics, surgical indications, and step-by-step techniques for anterior spinal decompression and fusion.
INTRODUCTION TO SPINAL CORD VASCULARITY
A profound understanding of the circulation of the spinal cord is a fundamental prerequisite for any surgeon undertaking complex spinal pathology, particularly during anterior approaches. The vascular network of the spinal cord is highly variable, intricate, and unforgiving of iatrogenic compromise. Historically determined through gross anatomical dissection and latex arterial injections, the vascular architecture dictates surgical decision-making, from the level of segmental vessel ligation to the postoperative hemodynamic management of the patient.
This masterclass delineates the arterial supply, venous drainage, and the critical surgical principles required to preserve spinal cord perfusion. Furthermore, it expands upon the evolution, indications, and step-by-step execution of anterior spinal approaches, ensuring maximum safety and optimal biomechanical outcomes.
ARTERIAL SUPPLY OF THE SPINAL CORD
The arterial supply to the spinal cord is derived from a complex network of segmental arteries that feed into longitudinal channels. This system is designed to respond dynamically to metabolic demands but possesses distinct watershed areas that are highly vulnerable to ischemia.
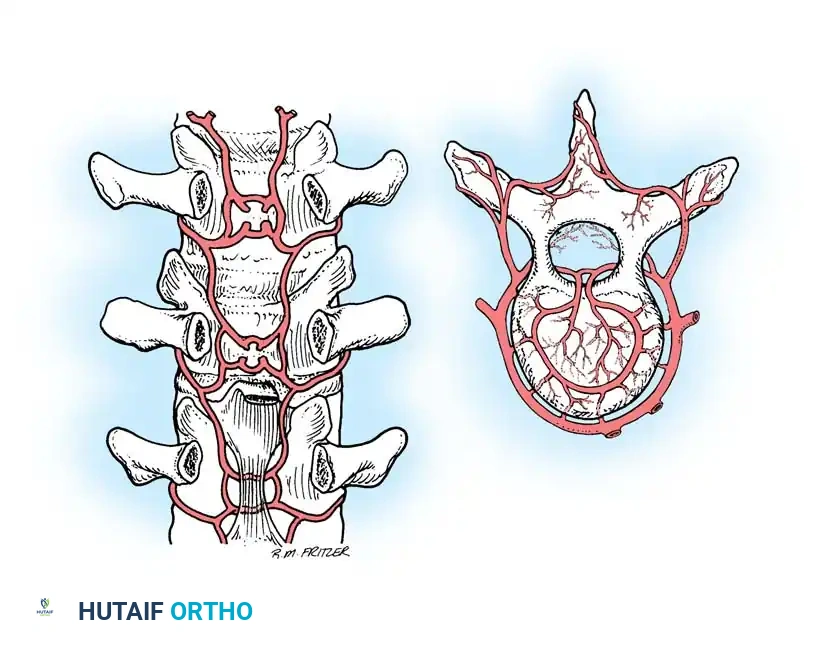
Segmental Arteries of the Spine
At every vertebral level, a pair of segmental arteries supplies both extraspinal and intraspinal structures. The origins of these vessels vary by anatomical region:
* Cervical Region: Segmental arteries arise primarily from the vertebral arteries, as well as the costocervical and thyrocervical trunks. In approximately 60% of individuals, an additional supplementary source arises from the ascending pharyngeal branch of the external carotid artery.
* Thoracic and Lumbar Regions: The segmental arteries arise directly from the posterior aspect of the descending aorta.
* Sacral Region: The lateral sacral arteries are the primary suppliers, with supplementary contributions from the fifth lumbar, iliolumbar, and middle sacral arteries. Sacral medullary feeders accompany the distal roots of the cauda equina, featuring reversible flow and adjustable volume based on metabolic demand.
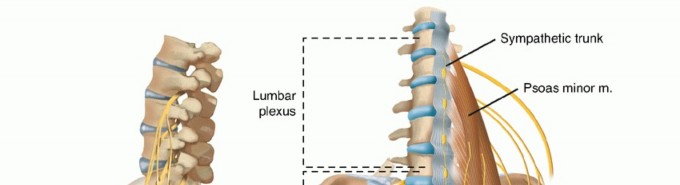
The "Distribution Point" and Anastomotic Networks
As the segmental arteries approach the spine, they divide into numerous branches at the intervertebral foramen, a critical anatomical junction termed the "distribution point."
Beyond the distribution point, a secondary anastomotic network lies within the spinal canal, embedded in the loose connective tissue of the extradural space. This rich anastomotic web is present at all levels but is most heavily concentrated in the cervical and lumbar regions. These channels offer vital alternative pathways for arterial flow, often preserving spinal cord circulation even after the unilateral ligation of segmental arteries during surgery.
The Artery of Adamkiewicz (Arteria Radicularis Magna)
The artery of Adamkiewicz is the largest and most critical medullary feeder to the lumbar cord.
* Location: It is predominantly located on the left side (in 80% of individuals) and typically enters the spinal canal between the T9 and T11 levels.
* Clinical Significance: While it is a massive feeder, the continuous integrity of the anterior longitudinal arterial channel is arguably more crucial than any single medullary feeder. Preservation of the artery of Adamkiewicz alone does not guarantee satisfactory circulation if the longitudinal anastomoses are compromised.
Surgical Warning: In principle, it is of immense practical value to protect and preserve each contributing segmental artery as far as surgically possible. Ischemic injury to the artery of Adamkiewicz can result in anterior spinal artery syndrome, characterized by bilateral loss of motor function and pain/temperature sensation, with preservation of proprioception and vibratory sense.
Variability and the Critical Vascular Zone
The variability of blood supply is a striking feature of spinal cord anatomy. However, there is absolute conformity to one principle: the cervical and lumbar cord enlargements possess a rich, redundant blood supply, whereas the thoracic cord is relatively watershed.
- The Critical Vascular Zone (T4–T9): The blood supply to the thoracic cord from approximately T4 to T9 is the poorest, and the spinal canal in this region is at its narrowest. Consequently, T4–T9 is considered the critical vascular zone of the spinal cord. Interference with circulation in this zone carries the highest risk of iatrogenic paraplegia.
Direction of Flow and Longitudinal Channels
The spinal cord is supplied by three primary longitudinal arterial channels (one anterior spinal artery and two posterior spinal arteries). This system functions on principles identical to the circle of Willis in the brain, permitting the reversal of flow and alterations in blood volume in response to metabolic demands.
This "inner arterial circle" is surrounded by at least two "outer arterial circles":
1. The extradural space network.
2. The extravertebral tissue plane network.
Through these outer circles, the spinal cord enjoys reserve sources of blood supply. However, the "outlet points" connecting these networks to the cord are strictly limited to the perforating sulcal arteries and the pial arteries. Recent clinical evidence from extensive anterior spinal surgeries suggests that the posterior spinal arteries, though historically underappreciated, play a massive role in collateral protection of the cord.
VENOUS DRAINAGE OF THE SPINAL CORD
The venous drainage of the spinal cord is highly variable and more difficult to define clearly than the arterial supply. It is divided into two primary sets of veins: the veins of the spinal cord itself, and the plexiform network known as Batson's plexus.
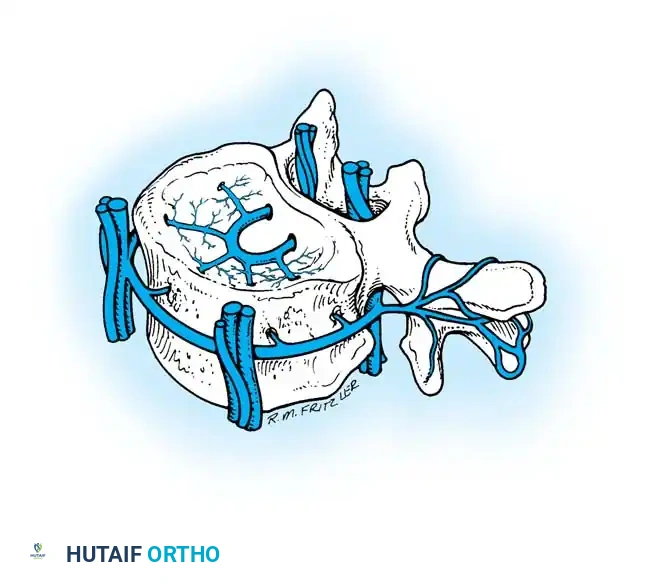
Batson's Venous Plexus
The veins of the spinal cord are a small component that ultimately drains into the Batson plexus. This is a massive, complex, and valveless venous channel extending from the base of the skull to the coccyx. It communicates directly with the superior and inferior vena cava systems and the azygos system.
The Batson plexus consists of three components:
1. Extradural Vertebral Venous Plexus: Located within the spinal canal.
2. Extravertebral Venous Plexus: Includes the segmental veins of the neck, intercostal veins, azygos communications in the thorax/pelvis, and lumbar veins.
3. Veins of the Bony Structures: Draining the vertebral bodies themselves.
Clinical Pearl: Because the Batson plexus is valveless and communicates directly with the venous systems of the head, chest, abdomen, and pelvis, it plays a critical role in the metastatic spread of neoplastic disease (e.g., prostate or breast cancer) and infectious diseases (e.g., discitis/osteomyelitis) directly to the vertebral column.
SURGICAL PRINCIPLES FOR PRESERVING CIRCULATION
During anterior spinal surgery, particularly in the thoracic and lumbar regions where segmental vessels must be mobilized or sacrificed for exposure, strict adherence to empirical vascular principles is mandatory to prevent cord ischemia.
The Four Commandments of Segmental Artery Ligation:
1. Ligate segmental spinal arteries only as absolutely necessary to gain surgical exposure.
2. Ligate segmental spinal arteries near the aorta (mid-vertebral body) rather than near the intervertebral foramina to preserve the anastomotic "distribution point."
3. Ligate segmental spinal arteries on one side only whenever possible, leaving the collateral circulation intact on the contralateral side.
4. Limit deep dissection in the vertebral foramina to a single level when possible, ensuring collateral circulation is disturbed as little as possible.
ANTERIOR APPROACHES TO THE SPINE
Historical Context and Evolution
Common use of the anterior approach for spinal surgery did not evolve until the 1950s. Pioneers such as Cloward, Southwick, Robinson, Bailey, and Badgley revolutionized cervical and lumbar approaches. The transthoracic approach developed more slowly, championed initially by Nachlas, Borden, Smith, and later perfected by Hodgson et al. in Hong Kong for the treatment of spinal tuberculosis. Today, advances in anesthesia, neuromonitoring, and intensive care have made these major surgical procedures highly safe and effective.
Indications for Anterior Approaches
Anterior approaches are primarily indicated for the direct decompression of neural elements (spinal cord, conus medullaris, cauda equina, or nerve roots) when anterior compression is documented by MRI or postmyelogram CT.
Pathological entities requiring anterior intervention include:
* Traumatic burst fractures with retropulsion.
* Neoplastic lesions (primary or metastatic) destroying the anterior column.
* Inflammatory or infectious lesions (e.g., osteomyelitis, tuberculosis).
* Degenerative conditions (e.g., cervical spondylotic myelopathy, OPLL).
* Congenital kyphotic deformities.
* Lumbar discogenic pain and instability requiring Anterior Lumbar Interbody Fusion (ALIF).
Multidisciplinary Team Approach
Anterior approaches to the spine carry a high risk of significant morbidity, including iatrogenic injury to major vascular (aorta, vena cava), visceral (esophagus, bowel, lung), or neurological structures. In many tertiary centers, a team approach is preferred, utilizing the combined skills of an orthopaedic spine surgeon, neurosurgeon, thoracic surgeon, or vascular/head-and-neck surgeon.
STEP-BY-STEP SURGICAL TECHNIQUES
Anterior Approach: Occiput to C3
The anterior approach to the upper cervical spine can be performed via a transoral or retropharyngeal route, depending on the pathology, the need for distal extension, and surgeon experience.
1. The Transoral Approach
Indications: Midline extradural lesions from the lower clivus to C2 (e.g., rheumatoid pannus, chordoma, basilar invagination).
Positioning: The patient is placed supine with the head secured in a Mayfield radiolucent headrest. The neck is slightly extended.
Surgical Steps:
* Preparation: Nasotracheal intubation is preferred. A Dingman mouth retractor is inserted to depress the tongue and elevate the soft palate.
* Incision: A midline vertical incision is made through the posterior pharyngeal wall, extending from the lower clivus to the C2-C3 disc space.
* Dissection: The longus colli and longus capitis muscles are elevated subperiosteally from medial to lateral.
* Decompression: A high-speed burr is used to resect the anterior arch of C1 and the odontoid process.
* Closure: Meticulous multilayer closure of the pharyngeal mucosa is critical to prevent cerebrospinal fluid (CSF) leaks and retropharyngeal abscesses.
2. The High Retropharyngeal Approach
Indications: Lesions requiring exposure from the clivus down to C3-C4, particularly when simultaneous anterior instrumentation is required (which is contraindicated in the contaminated transoral route).
Positioning: Supine, head turned slightly to the contralateral side.
Surgical Steps:
* Incision: A submandibular transverse incision is made approximately 2 cm below the mandible.
* Superficial Dissection: The platysma is divided. The mandibular branch of the facial nerve is protected by elevating the submandibular gland fascia. The facial artery and vein are ligated.
* Deep Dissection: The hypoglossal nerve (CN XII) and the superior laryngeal nerve are identified and mobilized. The carotid sheath is retracted laterally, and the pharynx/larynx is retracted medially.
* Exposure: The retropharyngeal space is entered, exposing the longus colli muscles, which are stripped laterally to reveal the anterior column from the clivus to C3.
Anterior Approach: Thoracic Spine (Transthoracic)
Indications: Thoracic disc herniations, burst fractures, or tumors from T4 to T11.
Positioning: Lateral decubitus position. The approach is typically from the left side to avoid the friable inferior vena cava and the liver, though right-sided approaches are used for upper thoracic lesions to avoid the aortic arch.
Surgical Steps:
* Incision: Made directly over the rib corresponding to the level of pathology (usually one or two levels above the target vertebra).
* Exposure: The rib is resected subperiosteally and saved for bone grafting. The parietal pleura is incised, and the lung is deflated (using a double-lumen endotracheal tube) and retracted.
* Vascular Management: The segmental vessels are identified in the valleys of the vertebral bodies. Following the "Four Commandments," they are ligated at the mid-vertebral body level to mobilize the aorta and expose the spine.
Anterior Approach: Lumbar Spine (Retroperitoneal)
Indications: ALIF, lumbar corpectomy for tumor or trauma (L2-L5).
Positioning: Supine or lateral decubitus, depending on the exact level and required instrumentation.
Surgical Steps:
* Incision: A transverse or oblique paramedian incision.
* Dissection: The rectus sheath is incised, and the retroperitoneal space is bluntly developed by sweeping the peritoneum medially.
* Vascular Mobilization: The psoas muscle is identified. The great vessels (aorta, IVC, and iliac bifurcations) are meticulously mobilized. The ascending lumbar vein and iliolumbar vein must often be ligated to allow safe medial retraction of the left common iliac vein, exposing the L4-L5 and L5-S1 disc spaces.
POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
Meticulous postoperative care is as critical as the surgical execution. Patients undergoing major anterior spinal reconstruction require intensive care unit (ICU) monitoring.
- Hemodynamic Parameters: Mean Arterial Pressure (MAP) must be strictly maintained above 85-90 mmHg for the first 72 hours postoperatively to ensure adequate perfusion to the spinal cord, particularly if the critical vascular zone (T4-T9) was manipulated.
- Neurological Monitoring: Hourly neurological checks are mandatory. Any acute deterioration warrants immediate evaluation for epidural hematoma or graft dislodgement via emergent MRI.
- Visceral and Pulmonary Care: For transthoracic approaches, chest tubes are managed until output is minimal. For retroperitoneal approaches, patients are monitored for paralytic ileus, and oral intake is advanced slowly.
- Mobilization: Early mobilization is encouraged within the constraints of the applied orthosis (e.g., TLSO or cervical collar) to prevent deep vein thrombosis and pulmonary complications.
By mastering the intricate vascular anatomy of the spinal cord and adhering to strict, evidence-based surgical principles, the modern orthopaedic spine surgeon can safely navigate anterior approaches, achieving optimal neural decompression and biomechanical stability while minimizing the catastrophic risk of ischemic paraplegia.
===FINAL_CHECK===
You Might Also Like