Spinal and Pelvic Abscess Drainage: Advanced Surgical Techniques
Key Takeaway
Spinal and pelvic abscesses, often secondary to pyogenic or tuberculous spondylodiscitis, require precise anatomical drainage to prevent catastrophic neurological compromise and sepsis. This guide details evidence-based surgical approaches—including extraoral cervical drainage, thoracic costotransversectomy, and psoas abscess evacuation—emphasizing critical neurovascular anatomy, patient positioning, step-by-step dissection, and postoperative protocols for orthopedic surgeons and spine specialists.
INTRODUCTION TO SPINAL AND PELVIC ABSCESS DRAINAGE
The surgical management of spinal and pelvic abscesses demands a profound understanding of fascial planes, regional neurovascular anatomy, and the pathophysiology of spinal infections. Whether secondary to pyogenic spondylodiscitis or granulomatous infections such as tuberculosis (Pott’s disease), an abscess cavity around the spine and pelvis can rapidly lead to mechanical instability, sepsis, and catastrophic neurological deficits.
Because purulent or tuberculous detritus follows the path of least resistance along established anatomical fascial planes, surgical drainage must be tailored to the specific anatomical level. This comprehensive guide details the operative techniques, biomechanical considerations, and step-by-step surgical approaches for evacuating abscesses in the cervical, dorsal (thoracic), lumbar, and pelvic regions.
Surgical Warning: Laminectomy is strictly contraindicated for anterior spinal abscesses or spondylodiscitis. Removing posterior tension-band structures in the presence of anterior column destruction exacerbates kyphotic deformity and fails to adequately decompress the anteriorly situated neural elements.
CERVICAL SPINE ABSCESS DRAINAGE
Infections of the cervical spine frequently result in abscess formation within the retropharyngeal space, the posterior triangle of the neck, or the supraclavicular fossa. If left untreated, tuberculous detritus or pyogenic pus may gravitate downward beneath the prevertebral fascia, ultimately forming a life-threatening mediastinal abscess.
Drainage of a Retropharyngeal Abscess
Drainage of a retropharyngeal abscess through a direct intraoral incision in the posterior wall of the pharynx is warranted only in an acute emergency, specifically when the patient presents with cyanosis, severe stridor, and impending respiratory collapse.
Under all other circumstances, drainage must be performed through a formal extraoral approach to ensure adequate evacuation, allow for dependent drainage, and prevent aspiration of purulent material.
Clinical Pearl: The extraoral approach minimizes the risk of secondary polymicrobial infection from the oral flora and provides a safer, more controlled environment for thorough debridement of the prevertebral space.
🔪 Surgical Technique: Extraoral Approach
- Incision: Make a 7.5-cm longitudinal incision along the posterior border of the sternocleidomastoid (SCM) muscle, centered at the junction of its middle and upper thirds.
- Fascial Dissection: Incise the superficial layer of the deep cervical fascia.
- Nerve Protection: Meticulously identify and protect the spinal accessory nerve (CN XI), which pierces the SCM and runs obliquely across the posterior triangle. Iatrogenic injury here results in profound trapezius palsy and shoulder dysfunction.
- Muscle Retraction: Retract the SCM medially. In cases of severe scarring or massive abscess, the muscle may be divided transversely, though this is rarely necessary.
- Deep Dissection: Using blunt dissection, expose the levator scapulae and splenius capitis muscles. Displace the internal jugular vein anteriorly. Palpate the fluctuant abscess anterior to the transverse processes and vertebral bodies.
- Evacuation: Puncture the abscess wall carefully with a closed hemostat. Spread the jaws to enlarge the opening parallel to the neurovascular structures, and gently but thoroughly evacuate the purulent material.
- Closure: If the abscess is unusually large and systemic symptoms are severe, leave the wound open for delayed primary closure or pack it lightly. If the cavity is small and well-debrided, close the wound in anatomical layers over a closed-suction drain.
Alternative Anterior Approach (Smith-Robinson Type)
For abscesses spanning C2 to C7, the standard anterior cervical approach provides excellent exposure. A transverse incision is utilized for localized disease (two or three vertebrae), whereas a longitudinal incision along the medial border of the SCM is preferred for extensive, multi-level involvement.
Surgical Warning: A tracheostomy set must be immediately available in the operating room. Patients with massive retropharyngeal abscesses are at high risk for sudden airway loss due to laryngeal edema or spontaneous intraoperative rupture of the abscess into the pharynx.
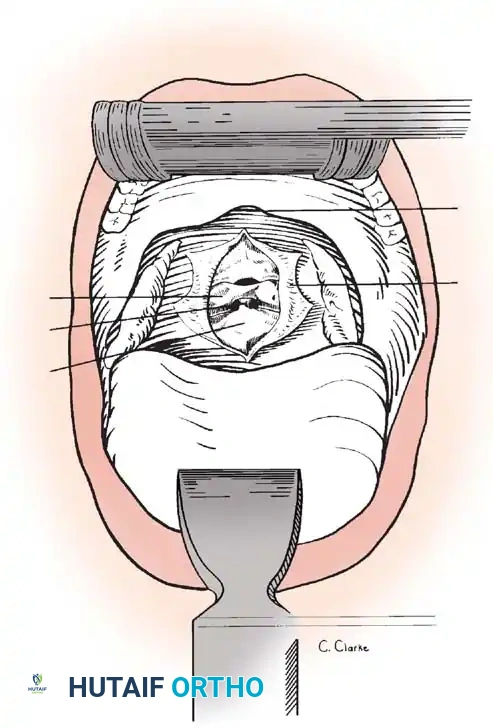
🔪 Surgical Technique: Anterior Cervical Drainage
- Positioning: Place the patient supine. Administer endotracheal anesthesia via a noncollapsible, wire-reinforced tube. Turn the head 10 to 20 degrees to the right (for a left-sided approach). Place a small roll beneath the neck to induce slight extension.
- Traction: Apply a head halter or Gardner-Wells tongs with several pounds of traction to stabilize the cervical spine.
- Incision & Superficial Dissection: Incise the skin and divide the platysma muscle longitudinally in the direction of its fibers. Open the cervical fascia along the anteromedial border of the SCM.
- Deep Plane Development: Develop the avascular plane between the SCM/carotid sheath laterally and the strap muscles (omohyoid, sternohyoid)/visceral axis (trachea, esophagus, thyroid) medially.
- Retraction: Palpate the carotid pulse and gently retract the sheath laterally. Identify the esophagus (facilitated by a preoperatively placed nasogastric tube).
- Esophageal Mobilization: Dissect the filmy connective tissue on the posterolateral aspect of the esophagus along the entire exposure. This prevents the esophagus from ballooning over the retractor blades, reducing the risk of iatrogenic perforation.
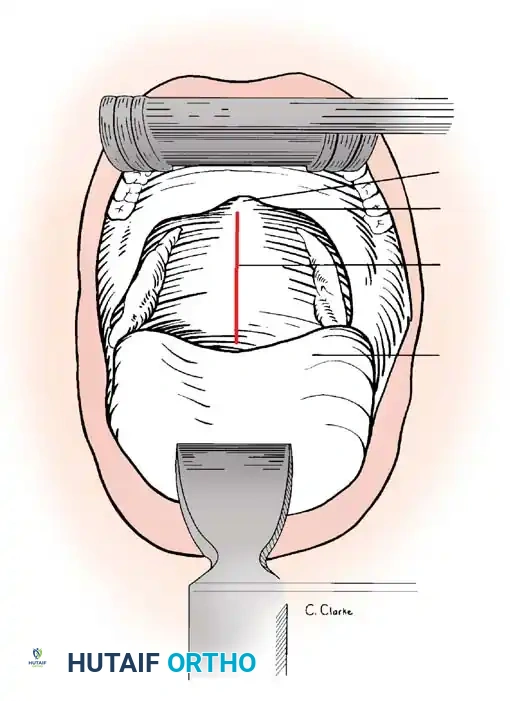
- Abscess Evacuation: Expose the bulging prevertebral fascia. Aspirate with a hypodermic needle to confirm purulence and obtain a lateral radiograph to verify the vertebral level. Incise the fascia and evacuate the cavity.
- Closure: Drain the wound standardly. Do not tightly close the deep cervical fascia, as postoperative hematoma or residual pus can cause airway compromise. Close the skin loosely.
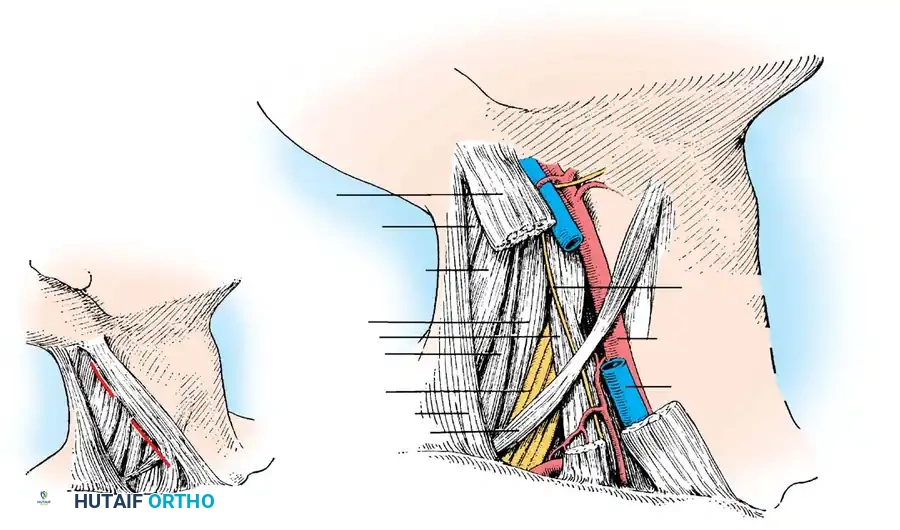
Drainage of an Abscess of the Posterior Triangle
- Incision: Incise the skin and superficial fascia obliquely for 6.3 cm along the posterior border of the SCM.
- Exposure: Retract the SCM medially, protecting the external jugular vein and the superficial cervical plexus nerves (e.g., great auricular nerve).
- Deep Dissection: Identify the scalene musculature. Crucial step: Locate and protect the phrenic nerve, which runs obliquely from lateral to medial across the anterior surface of the scalenus anterior muscle.
- Evacuation: Develop the cleavage line between the scalenus anterior and longus colli muscles via blunt dissection, directing the hemostat obliquely inward beneath the paravertebral fascia to enter the abscess. Evacuate and close over a drain.
DORSAL (THORACIC) SPINE ABSCESS DRAINAGE
Thoracic spinal infections frequently present with paravertebral abscesses that can compress the spinal cord, leading to Pott's paraplegia. Because the thoracic kyphosis naturally places the spinal cord anteriorly against the vertebral bodies, anterior decompression is mandatory.
Costotransversectomy
Originally described by Ménard in 1894, costotransversectomy remains the gold standard for evacuating dorsal spine abscesses. It allows direct access to the anterior column without violating the posterior tension band or manipulating the vulnerable thoracic spinal cord.
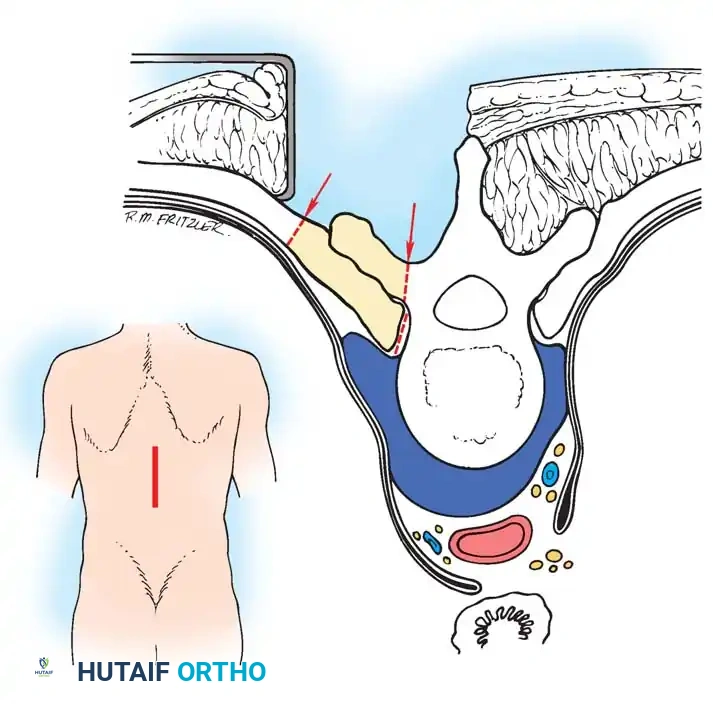
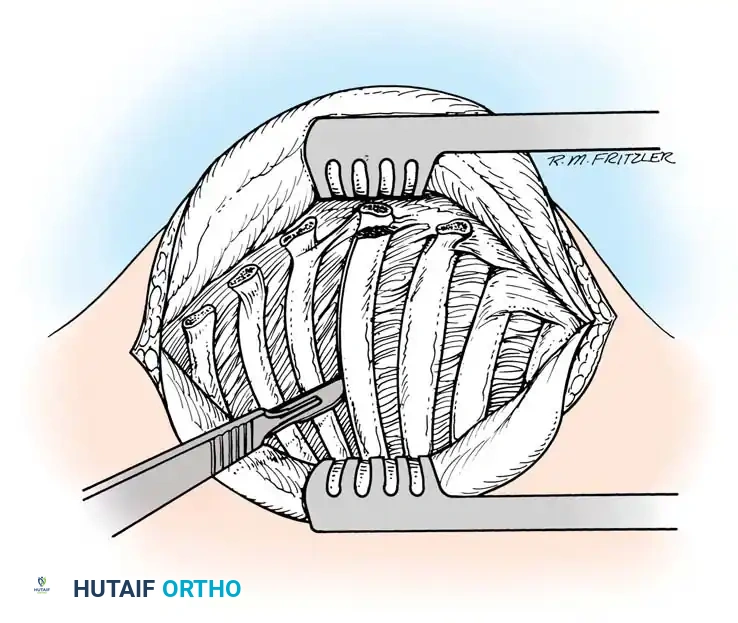
🔪 Surgical Technique: Standard Costotransversectomy
- Incision: Make a midline longitudinal incision spanning three spinous processes centered over the apex of the deformity or abscess.
- Soft Tissue Reflection: Reflect the periosteum and paraspinal muscles laterally from the spinous processes and laminae on the affected side.
- Bone Resection: Expose the middle transverse process fully and resect it at its base using a Leksell rongeur or high-speed burr.
- Rib Resection: Reflect the periosteum from the contiguous rib. Resect its medial end by dividing it approximately 5 cm from the tip of the transverse process. Bevel the remaining end of the rib to prevent soft tissue irritation.
- Pleural Protection: Exercise extreme caution to avoid puncturing the parietal pleura. If a pleural tear occurs, repair it immediately over a red rubber catheter while applying positive end-expiratory pressure (PEEP).
- Abscess Entry: Advance bluntly close to the vertebral body to enter the abscess. Enlarge the opening to permit thorough exploration and removal of necrotic bone, disc material, and caseous debris.
- Neurovascular Management: If multiple ribs are resected, doubly ligate and divide the intervening intercostal neurovascular bundles to prevent hemorrhage and neuralgia.
Anterolateral Decompression (Seddon's Approach)
For extensive disease with significant kyphosis, a wider anterolateral decompression is required.
- Incision: Begin a semicircular skin incision in the midline 10 cm proximal to the kyphotic apex, curve it laterally to 10 cm from the midline, and return to the midline 10 cm distal to the apex. (A straight midline incision suffices for pyogenic infections without kyphosis).
- Muscle Division: Elevate the skin flap. Divide the erector spinae muscles transversely opposite the apex of the deformity.
- Exposure: Using electrocautery, expose the medial 8.3 cm of at least three ribs, their corresponding transverse processes, and the lateral third of the laminae.
- Resection: Remove the transverse processes. Subperiosteally expose the ribs.
- Rib Transection: Transect the rib 6.8 cm lateral to the costotransverse joint. Use a curved gouge to free the medial end, pushing gently anteriorly and medially until striking the vertebral body. Rotate and extract the rib head.
- Evacuation: Pus will immediately extrude from the defect; evacuate it with high-volume suction. Explore the cavity digitally, dislodging sequestra. Apply local antibiotics (e.g., streptomycin powder for TB) and close without a drain to prevent sinus tract formation in tuberculous cases.
LUMBAR SPINE AND PELVIC DRAINAGE
Infections of the lumbar spine frequently track along the psoas muscle sheath, presenting as a psoas abscess. These are entirely extraperitoneal. Depending on the volume and gravitational tracking, they may point posteriorly, laterally at the iliac crest, or anteriorly in the groin.
Drainage of Paravertebral Abscess
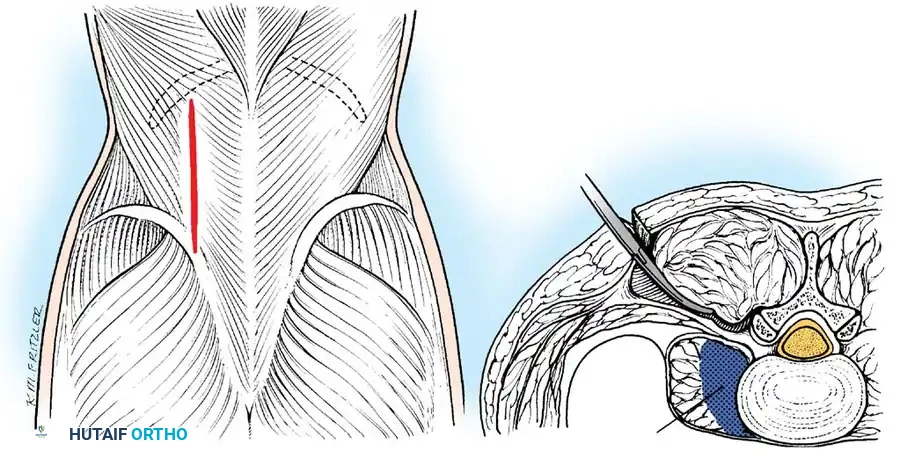
- Incision: Make a 7.5 to 10-cm longitudinal incision 5 to 7.5 cm lateral to the midline, parallel to the spinous processes.
- Fascial Dissection: Divide the lumbodorsal fascia. Pass a hemostat bluntly around the lateral and anterior borders of the erector spinae muscles toward the transverse processes.
- Entry: If the abscess is not immediately encountered, puncture the deep layer of the lumbodorsal fascia separating the quadratus lumborum from the erector spinae, forcing the hemostat along the anterior border of the transverse processes. Evacuate and close in layers.
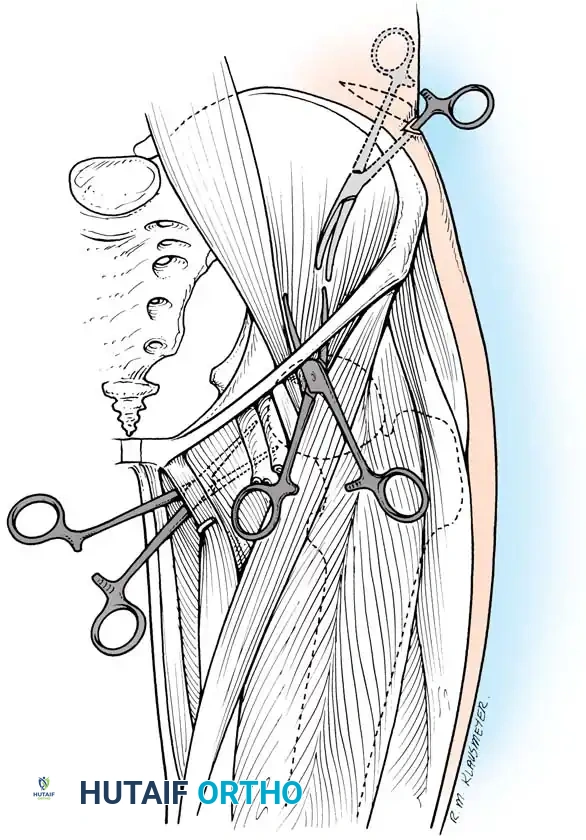
Drainage of Psoas Abscess
Psoas abscesses require tailored approaches based on their most prominent point of fluctuance.
1. Drainage through the Petit Triangle
The Petit triangle (lumbar triangle) is bounded by the latissimus dorsi (medially), external oblique (laterally), and the iliac crest (inferiorly). The floor is the internal oblique.
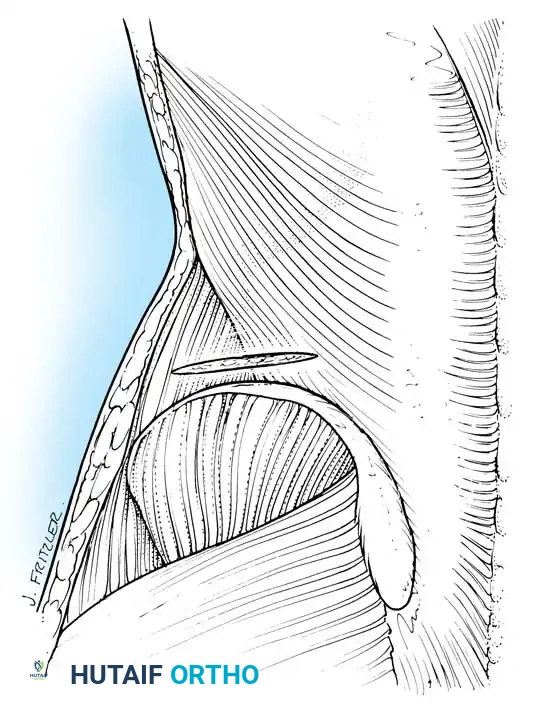
- Incision: Make a 7.5-cm incision 2.5 cm proximal to and parallel with the posterior crest of the ilium.
- Dissection: Expose the Petit triangle. Bluntly dissect through the internal oblique muscle fibers directly into the retroperitoneal abscess cavity. Evacuate and close.
- Postoperative Care: Because psoas spasm induces a severe hip flexion contracture, postoperative Buck traction is mandatory to gradually stretch the spastic muscle and restore full hip extension.
2. Drainage by Lateral Incision
- Incision: Make a 10-cm incision along the middle third of the iliac crest.
- Dissection: Free the attachments of the internal and external oblique muscles from the crest.
- Evacuation: Palpate the fluctuant extraperitoneal mass on the inner table of the iliac wing. Puncture with a hemostat, strictly avoiding perforation of the adjacent peritoneum.
3. Drainage by Anterior Incision
When the abscess burrows beneath the inguinal (Poupart) ligament, it presents in the proximal anterior thigh.
- Incision: Begin at the anterior superior iliac spine (ASIS) and extend 5 to 7.5 cm distally along the anterior thigh.
- Dissection: Identify the sartorius muscle. Retract it laterally and carry the dissection deep to its medial border toward the anterior inferior iliac spine (AIIS).
- Nerve Protection: The femoral nerve lies immediately medial to this dissection plane; it must be identified and protected.
- Evacuation: Insert a long hemostat along the medial surface of the iliac wing, passing under the inguinal ligament to puncture the abscess. Spread the blades to ensure complete evacuation.
4. Drainage by Ludloff Incision
For abscesses pointing subcutaneously in the medial adductor region (lesser trochanteric insertion of the psoas), a medial Ludloff approach is utilized. This involves an incision over the adductor longus, developing a plane between the adductor longus/brevis anteriorly and the adductor magnus posteriorly to reach the lesser trochanter.
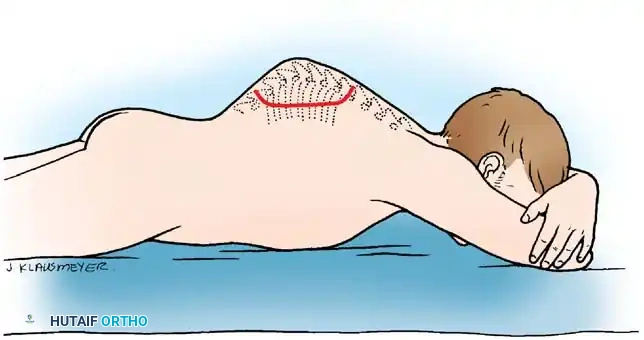
Coccygectomy for Drainage of a Pelvic Abscess
In severe lower lumbar and lumbosacral tuberculosis, massive soft-tissue abscesses may gravitate deep into the true pelvis, pooling anterior to the sacrum.
Clinical Pearl: Anterior thigh or iliac crest drainage alone is insufficient for deep presacral abscesses. Inadequate dependent drainage inevitably results in a chronically draining sinus tract, regardless of the efficacy of systemic antimicrobial therapy.
To achieve definitive dependent drainage, a coccygectomy is performed. The patient is placed in the prone or lateral decubitus position. A midline incision is made over the sacrococcygeal junction. The coccyx is subperiosteally dissected and excised, providing direct, dependent access to the presacral space. The abscess is evacuated, and a large-bore drain is placed to ensure continuous egress of fluid during the postoperative period.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Successful surgical drainage must be coupled with rigorous postoperative management:
- Microbiological Analysis: Intraoperative samples must be sent for aerobic, anaerobic, mycobacterial (AFB smears and cultures), and fungal testing. Histopathology is critical to confirm granulomatous disease.
- Antimicrobial Therapy: Empiric broad-spectrum intravenous antibiotics are initiated immediately post-drainage and tailored once sensitivities are available. Tuberculous abscesses require a prolonged course (9-12 months) of multi-drug therapy (Rifampin, Isoniazid, Pyrazinamide, Ethambutol).
- Spinal Stability: Patients must be evaluated for mechanical instability. Orthotic bracing (e.g., TLSO for thoracic/lumbar lesions, rigid cervical collar) is often required until bony fusion or stabilization occurs.
- Mobilization: Early mobilization is encouraged to prevent deep vein thrombosis and pulmonary complications, provided the spine is mechanically stable. Physical therapy focuses on resolving secondary contractures, particularly hip flexion contractures associated with psoas abscesses.
You Might Also Like


