Operative Management of Peripheral Nerve Injuries of the Shoulder Girdle
Key Takeaway
Peripheral nerve injuries around the shoulder, including the axillary, suprascapular, and musculocutaneous nerves, require meticulous clinical evaluation. Diagnosis often hinges on differentiating specific muscle weakness, such as isolating biceps function from the brachioradialis. Surgical management ranges from nerve decompression, such as releasing the transverse scapular ligament, to complex nerve grafting or tendon transfers, depending on the injury mechanism and patient age.
INTRODUCTION TO SHOULDER GIRDLE NEUROPATHIES
Peripheral nerve injuries around the shoulder girdle present a complex diagnostic and therapeutic challenge for the orthopedic surgeon. The intricate neurovascular anatomy of the brachial plexus and its terminal branches—specifically the axillary, suprascapular, and musculocutaneous nerves—renders them susceptible to a variety of traumatic, traction, and compressive insults. Accurate clinical examination, augmented by electrodiagnostic studies and advanced imaging, is paramount.
This comprehensive guide details the surgical anatomy, pathomechanics, clinical evaluation, and operative management of these critical nerve injuries, providing evidence-based protocols for residents, fellows, and practicing consultants.
THE AXILLARY NERVE
The axillary nerve is a terminal branch of the posterior cord of the brachial plexus, carrying fibers primarily from the C5 and C6 nerve roots. It provides critical motor innervation to the deltoid and teres minor muscles, and sensory innervation to the lateral shoulder (the "regimental badge" area) via the superior lateral cutaneous nerve of the arm.
Surgical Anatomy and Biomechanics
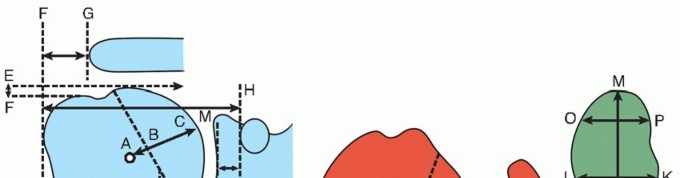
After branching from the posterior cord anterior to the subscapularis muscle, the axillary nerve courses inferiorly and posteriorly to exit the axilla through the quadrilateral space.
The boundaries of the quadrilateral space are strictly defined as:
* Superiorly: Teres minor (and the inferior capsule of the glenohumeral joint).
* Inferiorly: Teres major.
* Medially: Long head of the triceps brachii.
* Laterally: Surgical neck of the humerus.
Within this space, the axillary nerve is accompanied by the posterior humeral circumflex artery. The nerve then divides into anterior and posterior branches. The anterior branch winds around the surgical neck of the humerus to supply the anterior and middle deltoid, while the posterior branch supplies the teres minor and posterior deltoid before terminating as a cutaneous sensory branch.
Mechanisms of Injury
The axillary nerve is highly vulnerable to traction and direct trauma. It is most commonly injured during:
1. Anterior Dislocation of the Shoulder: The nerve is tethered at the quadrilateral space and is stretched across the dislocating humeral head.
2. Fractures of the Proximal Humerus: Particularly surgical neck fractures.
3. Iatrogenic Injury: During open or arthroscopic shoulder surgery, such as inferior capsular shifts or subdeltoid approaches.
Quadrilateral Space Syndrome (QSS)
Quadrilateral Space Syndrome is a rare neurovascular compression syndrome caused by the entrapment of the axillary nerve and the posterior humeral circumflex artery within the quadrilateral space. It typically affects young, overhead athletes (e.g., pitchers, volleyball players).
Clinical Pearl: Diagnosing QSS
In Quadrilateral Space Syndrome, there is usually no profound loss of sensation or catastrophic loss of strength, making clinical diagnosis elusive. Furthermore, Electromyography (EMG) is frequently normal. Diagnosis relies heavily on dynamic imaging.
A subclavicular arteriogram or dynamic MR angiography is often indicated. The study is considered positive if occlusion of the posterior humeral circumflex artery occurs with less than 60 degrees of shoulder abduction and external rotation. Diagnostic local anesthetic blocks, accomplished easily by inserting needles along the posterior border of the deltoid into the quadrilateral space, can also confirm the diagnosis if symptoms are temporarily relieved.
Treatment and Outcomes After Axillary Nerve Injury
Management depends entirely on the mechanism of injury and the temporal progression of recovery.
Conservative Management:
If the injury is a closed traction neuropraxia or axonotmesis (e.g., following a simple anterior dislocation), expectant management is the gold standard. Signs of return of function may not be observed for 3 to 12 months. However, the prognosis is generally excellent, with most patients (approximately 90%) progressing to full functional recovery.
Surgical Exploration and Nerve Repair:
If there is no clinical or EMG evidence of recovery by 3 to 6 months, or if the injury is an open, penetrating wound, surgical exploration is indicated. Options include neurolysis, direct end-to-end neurorrhaphy, or sural nerve cable grafting depending on the gap length.
Tendon and Muscle Transfers for Deltoid Paralysis:
In cases of irreversible axillary nerve palsy where nerve reconstruction has failed or presents too late, salvage procedures are required to restore shoulder abduction and forward elevation. Tendon and muscle transfers for paralysis of the deltoid typically involve transferring the origin of the pedicled latissimus dorsi or the pectoralis major to the proximal humerus or acromion.
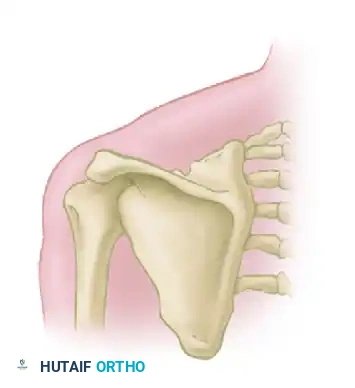
THE SUPRASCAPULAR NERVE
The suprascapular nerve (C5, C6) branches from the upper trunk of the brachial plexus. It is a mixed motor and sensory nerve, providing critical motor supply to the supraspinatus and infraspinatus muscles, and sensory branches to the glenohumeral and acromioclavicular joints.
Pathomechanics of Entrapment
The nerve is most vulnerable at two distinct anatomic choke points:
1. The Suprascapular Notch: Covered by the transverse scapular ligament. Entrapment here causes weakness in both the supraspinatus (abduction) and infraspinatus (external rotation).
2. The Spinoglenoid Notch: Covered by the spinoglenoid ligament. Entrapment here (often due to paralabral cysts associated with SLAP tears) causes isolated infraspinatus weakness.
Surgical Approach: Division of the Transverse Scapular Ligament
When conservative management for suprascapular nerve entrapment at the suprascapular notch fails, surgical decompression via division of the transverse scapular ligament is indicated. This can be performed arthroscopically or via a classic open posterior approach.
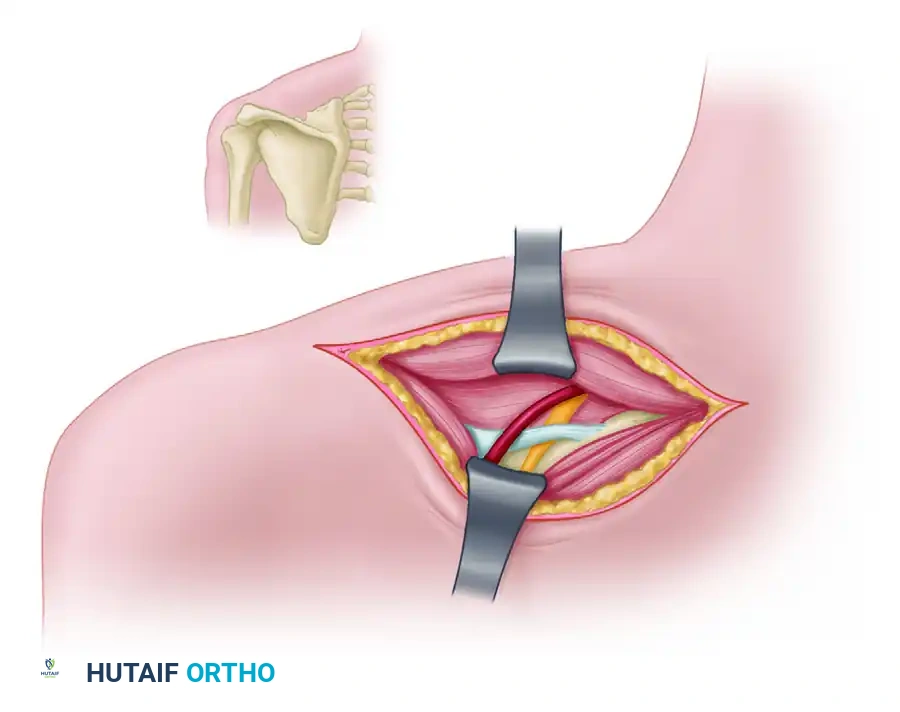
Step-by-Step Open Posterior Approach:
1. Positioning: The patient is placed in the lateral decubitus or prone position with the operative arm draped free to allow manipulation.
2. Incision: A linear incision is made parallel to and approximately 2 cm superior to the spine of the scapula, extending over the supraspinatus fossa.
3. Superficial Dissection: The trapezius muscle fibers are identified. They can be split in line with their fibers or detached from the scapular spine and retracted superiorly to expose the underlying supraspinatus muscle.
4. Deep Exposure: The supraspinatus muscle is carefully mobilized and retracted posteriorly and inferiorly. This exposes the floor of the supraspinatus fossa.
5. Identifying the Notch: Blunt dissection proceeds laterally along the superior border of the scapula until the suprascapular notch is palpated.
Surgical Warning: The "Army over Navy" Rule
Meticulous dissection is required at the notch. The suprascapular artery passes above (superior to) the transverse scapular ligament, while the suprascapular nerve passes beneath (inferior to) the ligament through the notch. Iatrogenic injury to the artery can cause severe bleeding that obscures the surgical field.
- Ligament Release: A blunt right-angle probe or a Freer elevator is passed beneath the transverse scapular ligament to protect the underlying nerve. The ligament is then sharply divided using a scalpel or Kerrison rongeur.
- Neurolysis: Once the ligament is divided, the nerve is inspected. Epineurotomy is rarely required unless severe intrinsic scarring is present. The nerve should be completely free from tethering.
- Closure: The supraspinatus is allowed to fall back into place. The trapezius is meticulously repaired to the scapular spine using heavy non-absorbable sutures to prevent postoperative weakness.
THE MUSCULOCUTANEOUS NERVE
The musculocutaneous nerve is a major terminal branch of the lateral cord of the brachial plexus, carrying fibers from C5 and C6. It provides essential motor innervation to the anterior compartment of the arm (coracobrachialis, biceps brachii, and brachialis) and continues distally as the lateral antebrachial cutaneous nerve, supplying sensation to the lateral aspect of the forearm.
Surgical Anatomy
The nerve originates at the inferior border of the pectoralis minor. It classically pierces the coracobrachialis muscle approximately 3 to 8 cm distal to the coracoid process. It then descends obliquely between the biceps brachii and the brachialis, innervating both, before piercing the deep fascia lateral to the biceps tendon to become a purely sensory nerve.
Mechanisms of Injury
The musculocutaneous nerve is most commonly injured by:
* Penetrating Injuries: Lacerations, stab wounds, or gunshot wounds to the axilla or anterior arm.
* Traction Injuries: Occasionally caused by severe anterior dislocation of the shoulder.
* Fractures: Displaced fractures of the humeral neck.
* Iatrogenic: Retractor placement during the deltopectoral approach (e.g., Latarjet procedure or total shoulder arthroplasty), especially if retractors are placed medial to the conjoined tendon.
When this nerve is injured in the axilla, the injury is often in conjunction with injuries to other components of the brachial plexus. Isolated musculocutaneous nerve injuries are relatively rare.
Clinical Examination and Diagnostic Pitfalls
Complete division of the musculocutaneous nerve may be easily overlooked by the unwary clinician.
Clinical Pitfall: Masked Biceps Paralysis
Flexion of the elbow by the brachioradialis (innervated by the radial nerve) may be strong enough to completely mask biceps paralysis. A patient with a transected musculocutaneous nerve can often still flex their elbow against gravity.
To accurately examine the musculocutaneous nerve, the clinician must isolate the biceps. The only muscle supplied by the musculocutaneous nerve that can be examined accurately is the biceps; the brachialis and the coracobrachialis are deep and difficult to palpate independently.
Examination Technique:
1. Position the patient's forearm in full supination (this disadvantages the brachioradialis).
2. Ask the patient to flex the elbow against resistance.
3. It is essential to physically palpate the biceps muscle belly and its distal tendon during this maneuver to identify specific muscle contractions.
Sensory examination is of no great diagnostic value because complete anesthesia in the lateral forearm is rare due to overlapping sensory dermatomes from the radial and median nerves.
Treatment Strategies
The disability resulting from an isolated division of the musculocutaneous nerve is surprisingly minimal compared to that of any other major nerve in the body. Because elbow flexion can be powerfully compensated by the brachioradialis (radial nerve) and the pronator teres (median nerve), the functional deficit is often well-tolerated.
For this reason, especially in older, low-demand patients, surgical suture or nerve grafting occasionally is not even indicated.
However, in young, active patients, or manual laborers who require strong supination and sustained elbow flexion power, surgical intervention is recommended.
* Primary Repair: Indicated for sharp, clean lacerations if tension-free approximation is possible.
* Nerve Grafting: Required for delayed presentations or blast injuries with a zone of injury.
* Nerve Transfers: In cases of proximal root avulsions or delayed presentations (>12 months), transferring a redundant fascicle of the ulnar or median nerve (Oberlin transfer) to the biceps motor branch has shown excellent results in restoring elbow flexion.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Regardless of the specific nerve addressed, postoperative rehabilitation follows a phased, biologically respectful protocol.
Phase I: Protection (Weeks 0-3)
* Immobilization in a sling or orthosis to remove tension from the repair site.
* Passive range of motion (PROM) of adjacent joints (wrist, hands) to prevent stiffness.
* Strict avoidance of stretch on the repaired nerve (e.g., avoiding shoulder extension and external rotation for axillary/suprascapular repairs; avoiding elbow extension for musculocutaneous repairs).
Phase II: Early Motion (Weeks 3-6)
* Gradual introduction of PROM to the affected joint within safe zones.
* Initiation of active-assisted range of motion (AAROM) as tolerated.
* Neuromuscular electrical stimulation (NMES) may be utilized to maintain muscle bulk in the denervated target muscles while awaiting reinnervation.
Phase III: Strengthening (Weeks 6-12+)
* Progression to active range of motion (AROM).
* Isotonic and isometric strengthening begins once clinical or EMG evidence of motor return is documented.
* Because nerve regeneration occurs at approximately 1 mm per day (or 1 inch per month), patients must be counseled that maximal functional recovery may take 12 to 18 months. Regular clinical follow-up and serial EMG studies at 3, 6, and 12 months are critical to monitor progress and determine if secondary salvage procedures (like tendon transfers) are required.
You Might Also Like