Advanced Diagnosis of SLAP Tears: Clinical Presentation, Examination & Imaging in an Athlete
Key Takeaway
Diagnosing athletic SLAP tears requires a detailed history of overhead shoulder pain. Clinical exam focuses on superior glenoid tenderness and positive tests (O'Brien's, Speed's, Kim's). While X-rays exclude bony issues, MRI or MR arthrography confirms Type II/IV labral tears with biceps anchor involvement, crucial for precise diagnosis.
Patient Presentation & History
We present the case of a 32-year-old male, a professional racquet sport athlete, who presented with a 9-month history of persistent right shoulder pain. His primary complaint was deep, aching pain, localized to the anterior and superior aspects of the glenohumeral joint, significantly exacerbated by overhead activities, especially during the serving motion and follow-through. He reported mechanical symptoms including occasional clicking and a subjective sensation of "dead arm" after strenuous activity, but denied frank instability or recurrent dislocations.
The inciting event occurred approximately 9 months prior when he experienced an acute episode of sharp pain in his dominant shoulder following a forceful serve. He initially attributed this to muscle strain and sought conservative management, including rest, non-steroidal anti-inflammatory drugs (NSAIDs), and a course of physical therapy focusing on rotator cuff strengthening and scapular stabilization. Despite adherence to the prescribed regimen for several months, his symptoms failed to resolve, progressively worsening to the point of impacting his athletic performance and daily activities. He reported a functional deficit characterized by decreased power and accuracy in overhead movements.
Past medical history was unremarkable, with no significant comorbidities. He denied any previous shoulder injuries or surgeries. Social history was pertinent for his occupation requiring high-demand overhead arm movements. He was a non-smoker and consumed alcohol occasionally.
Clinical Examination
Initial examination revealed a well-muscled, athletic individual in no acute distress.
Inspection
- Static: Symmetrical bilateral shoulder girdles. No obvious muscle atrophy, fasciculations, or deformities. Scapular resting position appeared normal. No skin changes, scars, or ecchymosis.
- Dynamic: Observation of active range of motion revealed mild dyskinesia of the right scapula, particularly during abduction and flexion, suggesting potential scapulothoracic muscle imbalance. No winging was noted.
Palpation
- Tenderness was elicited over the anterior aspect of the glenohumeral joint line, specifically at the bicipital groove and the superior glenoid rim.
- The acromioclavicular (AC) joint was non-tender.
- No significant tenderness over the greater tuberosity, subacromial space, or trapezius origin.
- Palpation of the rotator cuff insertions revealed no focal tenderness.
Range of Motion
-
Active Range of Motion (AROM):
- Forward Flexion: 160° (L: 180°) with pain in the terminal arc.
- Abduction: 155° (L: 180°) with pain in the terminal arc.
- External Rotation (at 0° abduction): 50° (L: 60°) with mild pain.
- Internal Rotation (at 0° abduction): T10 (L: T7).
- Internal Rotation (behind back): Reached L1 (L: T12).
- Passive Range of Motion (PROM): Full and pain-free through all planes, suggesting no adhesive capsulitis or significant capsular restriction. Pain was reproduced only at the extremes of motion, specifically with combined abduction and external rotation.
-
Resisted Isometrics:
- Significant pain with resisted elbow flexion (biceps engagement).
- Mild pain with resisted supination.
- No significant weakness or pain with resisted external rotation (infraspinatus/teres minor), internal rotation (subscapularis), or abduction (supraspinatus).
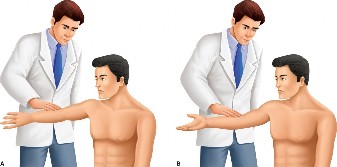
- Pain reproduced with O'Brien's active compression test (thumb down position), relieved with thumb up.
- Positive Speed's test (pain in bicipital groove with resisted shoulder flexion against an extended elbow and supinated forearm).
- Yergason's test was positive (pain with resisted forearm supination and elbow flexion with the elbow flexed to 90 degrees and the arm adducted).
- Anterior Slide test produced pain and a click at the superior aspect of the glenohumeral joint.
- Compression-Rotation test elicited a painful click when the arm was abducted to 90°, elbow flexed to 90°, and an axial load applied through the humerus while rotating the humerus internally and externally.
- Kim's Biceps Load II test was performed, reproducing the patient's typical pain.
Neurological & Vascular Assessment
- Neurological: Intact motor and sensory function in the C5-T1 dermatomes and myotomes. No muscle weakness attributed to specific nerve palsies. Deep tendon reflexes (biceps, triceps, brachioradialis) were 2+ bilaterally and symmetrical. No signs of axillary nerve neuropraxia or suprascapular nerve impingement.
- Vascular: Radial and ulnar pulses were 2+ and symmetrical. Capillary refill was brisk in all digits. No signs of vascular compromise.
Overall, the clinical picture strongly suggested a superior labral pathology involving the biceps anchor, with no overt signs of rotator cuff tear, significant glenohumeral instability, or AC joint pathology. The positive specific tests for SLAP lesions, coupled with bicipital groove tenderness and pain with resisted biceps contraction, pointed towards a Type II or IV SLAP tear with associated biceps involvement.
Imaging & Diagnostics
X-ray Findings
Initial radiographs of the right shoulder included anterior-posterior (AP), Y-scapular, and axillary views.
* These demonstrated concentric glenohumeral joint spaces with no evidence of significant degenerative changes, subluxation, or dislocation.
* No acute fractures of the humerus, scapula, or clavicle were identified.
* The acromion morphology was Type I (flat), with no evidence of significant acromial spurring that would predispose to rotator cuff impingement.
* No calcific tendinopathy was noted.
* The findings were largely unremarkable for acute bony pathology but served to exclude other causes of shoulder pain.
MRI & MR Arthrogram Indications
Given the persistent symptoms despite conservative management and the clinical suspicion of a labral tear, magnetic resonance imaging (MRI) of the right shoulder without contrast was initially performed.
* The MRI demonstrated some signal abnormality within the superior labrum but was inconclusive regarding the extent of the tear and its involvement with the biceps anchor. While it suggested a possible labral delamination, the exact configuration and stability of the superior labrum-biceps complex were not clearly defined. Mild tendinosis of the long head of the biceps tendon was noted within the bicipital groove.
* Due to the equivocal findings on non-arthrographic MRI, an MR arthrogram was indicated and performed to enhance diagnostic accuracy. The MR arthrogram involved intra-articular injection of gadolinium-based contrast medium, which distended the joint capsule and allowed for better visualization of the labral-biceps complex.
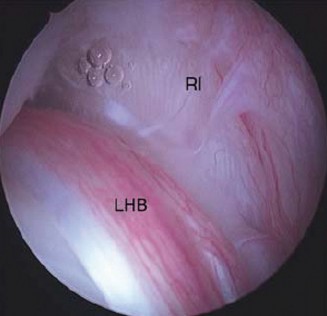
* The MR arthrogram clearly demonstrated a detachment of the superior labrum from the glenoid rim, extending anteriorly and posteriorly to the biceps anchor. The biceps tendon appeared to originate directly from the detached labral tissue, indicating instability of the biceps anchor. There was T2 hyperintensity and extravasation of contrast into the superior labral-biceps complex, consistent with a tear. The tear extended along the anterior-superior and posterior-superior aspects of the labrum, definitively identifying it as a Snyder Type II SLAP lesion, with evidence of degenerative changes at the tear site. The rotator cuff tendons appeared intact with no evidence of full-thickness tears. The glenohumeral ligaments were intact, and no significant capsular laxity was observed.
* Below is a representative image that illustrates the typical findings on an MR arthrogram consistent with a SLAP tear, demonstrating contrast extravasation into the superior labral-biceps complex.
Templating
Templating, primarily used for arthroplasty, is not directly applicable to SLAP tear diagnosis or repair. However, the comprehensive assessment of the glenoid version and inclination, if performed, would be crucial in complex instability cases or for ruling out dysplasia, which was not indicated here. In the context of arthroscopic repair, pre-operative templating involves planning portal placement and anchor trajectories based on anatomical landmarks to optimize repair construct and minimize neurovascular risk.
Differential Diagnosis
The presentation of persistent shoulder pain, particularly with overhead activities and mechanical symptoms, necessitates a broad differential diagnosis. Distinguishing SLAP tears from other common shoulder pathologies is critical for appropriate management.
| Condition | Key History Points | Key Exam Findings | Key Imaging Findings (MRI/MR Arthrography) |
|---|---|---|---|
| SLAP Tear (e.g., Type II) | - Overhead athlete, acute injury (FOOSH) or chronic repetitive microtrauma. | - Deep, aching pain, localized to superior/anterior shoulder. | - MR Arthrography is gold standard: Contrast between superior labrum and glenoid, extending into biceps anchor. Biceps anchor detachment. |
| - Clicking, popping, grinding, "dead arm" sensation. | - Pain with resisted biceps contraction (Speed's, Yergason's). | - Non-arthrographic MRI may show T2 hyperintensity at superior labrum, but often equivocal. | |
| - Pain with overhead activities. | - Positive O'Brien's, Compression-Rotation, Anterior Slide, Biceps Load II tests. | - Exclude other pathologies. | |
| Rotator Cuff Tendinopathy/Tear | - Overhead activities, repetitive lifting, or acute injury. | - Pain with overhead motion, reaching, sleeping on affected side. | - Tendinopathy: Increased signal intensity within tendon, thickening. |
| - Weakness, especially with abduction and external rotation. | - Painful arc (60-120° abduction). | - Partial-thickness tear: Focal high signal intensity within tendon, articular or bursal side involvement, but not through entire tendon thickness. | |
| - Night pain. | - Positive impingement signs (Hawkins-Kennedy, Neer). | - Full-thickness tear: Fluid signal extending through entire tendon thickness, retraction, muscle atrophy (chronic). | |
| - No mechanical clicking usually, unless associated with bursitis or bicipital pathology. | - Weakness and pain with resisted external rotation (infraspinatus/teres minor), abduction (supraspinatus), or internal rotation (subscapularis). | ||
| Biceps Tendinopathy/Subluxation | - Repetitive overhead activities, lifting. | - Anterior shoulder pain, particularly over bicipital groove. | - Tendinopathy: Increased signal within tendon, thickening or thinning, fluid in tendon sheath. |
| - Snapping sensation (subluxation). | - Positive Speed's, Yergason's tests (often more localized pain than SLAP). | - Subluxation/dislocation: Tendon displacement from bicipital groove, often with rupture of transverse humeral ligament. | |
| - Can coexist with SLAP tears or rotator cuff pathology. | - Palpation of bicipital groove elicits tenderness. | - Tear: Discontinuity of tendon fibers, retraction. | |
| Glenohumeral Instability | - History of dislocations or subluxations (traumatic or atraumatic). | - Apprehension with specific arm positions (e.g., abduction/external rotation). | - Bankart lesion (anterior inferior labral tear), Hill-Sachs lesion (posterior superior humeral head impaction fracture). |
| - "Dead arm" sensation often more pronounced with overt instability events. | - Positive apprehension and relocation tests. | - HAGL lesion (humeral avulsion of glenohumeral ligaments). | |
| - Young patients, often athletes. | - General ligamentous laxity may be present (Beighton score). | - Capsular laxity, glenoid bone loss. |
Surgical Decision Making & Classification
Given the patient's persistent, debilitating pain, failure of a prolonged course of conservative management, and objective evidence of a Type II SLAP lesion on MR arthrography correlating with clinical findings, surgical intervention was indicated. The patient's high-demand athletic requirements further supported an operative approach to restore function and allow return to sport.
Classification: Snyder Classification of SLAP Lesions
The Snyder classification system is widely used to categorize superior labrum tears:
*
Type I:
Degeneration and fraying of the superior labrum, but the biceps anchor remains firmly attached to the superior glenoid. This is typically managed non-operatively with debridement if symptoms persist.
*
Type II:
Detachment of the superior labrum and the biceps anchor from the superior glenoid. This is the most common type and was identified in our patient. It is further subdivided:
* IIA: Predominantly anterior detachment.
* IIB: Predominantly posterior detachment.
* IIC: Combined anterior and posterior detachment.
* Our patient exhibited an IIC pattern. Type II tears generally warrant arthroscopic repair.
*
Type III:
A bucket-handle tear of the superior labrum that displaces into the joint, but the biceps anchor remains intact. This is treated with arthroscopic debridement of the unstable labral flap.
*
Type IV:
A bucket-handle tear of the superior labrum that extends into the biceps tendon, creating a split within the tendon. This type also typically requires arthroscopic repair of both the labrum and the biceps tendon, or a biceps tenodesis/tenotomy depending on tendon quality and patient age/activity.
Additional, less common classifications (Types V-VII) exist, incorporating other pathologies:
*
Type V:
Type II SLAP tear with an associated anterior-inferior Bankart lesion.
*
Type VI:
Type II SLAP tear with an unstable superior labral flap (similar to a Type III but with biceps involvement).
*
Type VII:
Type II SLAP tear that extends anteriorly under the middle glenohumeral ligament (MGHL) into the anterior capsule.
For our patient, a Type IIC SLAP lesion, arthroscopic labral repair with re-establishment of the biceps anchor stability was the treatment of choice. This approach aims to restore the anatomic attachment of the superior labrum and biceps, crucial for maintaining normal glenohumeral kinematics and preventing secondary instability or pain generator. In younger, active individuals, repair is generally preferred over debridement or tenodesis/tenotomy to preserve biomechanical function, though the latter may be considered for older patients or those with significant biceps pathology.
Surgical Technique / Intervention
The patient underwent right shoulder arthroscopy and superior labral repair.
Patient Positioning
The patient was positioned in the lateral decubitus position . This allows for excellent visualization of the glenohumeral joint and ample working space for instrumentation. The right arm was suspended using a traction tower at approximately 70-80 degrees of abduction and 15-20 degrees of forward flexion, with 10-15 pounds of traction applied. Adequate padding was ensured at all pressure points. A posterior bump was utilized to maintain the shoulder in a slightly anteriorly rotated position.
Approach & Portals
Standard arthroscopic portals were utilized:
1.
Posterior Viewing Portal:
This was established approximately 1 cm medial and 1 cm inferior to the posterolateral corner of the acromion. A spinal needle was used to locate the glenohumeral joint, followed by an incision and blunt dissection to avoid neurovascular structures (axillary nerve). The arthroscope was then introduced through this portal for diagnostic arthroscopy.
2.
Anterior-Superior Working Portal (Neviaser Portal):
A spinal needle was inserted anteriorly, just lateral to the coracoid process, aiming for the superior glenoid neck. This portal provides an excellent trajectory for superior labral repair, allowing for anchor placement and suture management.
3.
Anterior-Inferior Working Portal:
This portal was established adjacent to the Neviaser portal, more inferiorly, to assist with instrument maneuvering and suture retrieval, particularly for the more anterior extent of the labral tear.
Diagnostic Arthroscopy
A thorough diagnostic arthroscopy confirmed the Type IIC SLAP lesion.
* Visualization from the posterior portal clearly showed the superior labrum detached from the superior glenoid rim, extending anteriorly and posteriorly around the biceps anchor.
* The biceps tendon origin was unstable, lifting off with probing, confirming its involvement.
* The articular cartilage was pristine, with no significant chondral lesions.
* The rotator cuff tendons (supraspinatus, infraspinatus, subscapularis) were inspected and found to be intact.
* The anterior and posterior labrum were stable.
* The glenohumeral ligaments were intact.
Labral Preparation and Reduction
- Debridement: Using a motorized shaver through the anterior-superior portal, the frayed and degenerative edges of the superior labrum were debrided back to stable tissue. The superior glenoid neck was decorticated with a burr to create a bleeding bed, promoting biological healing of the repaired labrum to the bone. Care was taken to preserve the healthy labral tissue and avoid excessive removal.
- Mobilization: The detached labrum and biceps anchor were carefully mobilized using a blunt probe to ensure full reduction back to the glenoid rim without tension. This confirmed the ability to achieve an anatomical repair.
Fixation Construct
The repair was performed using bioabsorbable suture anchors.
1.
Anchor Placement:
Typically, 2 to 3 suture anchors are required for a Type II SLAP repair. For a Type IIC lesion, anchors are strategically placed to secure both the anterior and posterior extensions of the tear, as well as the biceps anchor.
* The first anchor was placed at the posterior-superior glenoid, immediately adjacent to the articular cartilage, at approximately the 11 o'clock position (for a right shoulder). A drill guide was used through the anterior-superior portal to drill a pilot hole. A 2.9 mm bioabsorbable suture anchor, preloaded with two sutures, was then inserted and deployed.
* The second anchor was placed at the anterior-superior glenoid, typically at the 1 o'clock position (for a right shoulder), in a similar fashion.
2.
Suture Management and Repair:
* For each anchor, a suture passer (e.g., BirdBeak, Scorpion) was used through the anterior-inferior or anterior-superior portal to retrieve the sutures.
* For the posterior anchor, one suture limb was passed through the posterior aspect of the superior labrum, approximately 5-7 mm from the glenoid rim, and the other through the biceps anchor.
* For the anterior anchor, sutures were passed through the anterior aspect of the superior labrum and the biceps anchor, ensuring comprehensive coverage.
* Each suture was retrieved through the anterior-superior portal and tied using arthroscopic knot-tying techniques (e.g., Cinch, Revo, or a series of half-hitches with alternating posts). The knots were carefully seated to ensure anatomical reduction and tensioning of the labrum and biceps anchor without over-tightening or strangulating the tissue. The stability of the repair was checked with a probe.
Closure
Following satisfactory repair, the glenohumeral joint was thoroughly irrigated. The portals were closed with a single subcutaneous suture and sterile dressings were applied. A sling with an abduction pillow was applied to immobilize the shoulder in a protected position.
Post-Operative Protocol & Rehabilitation
Post-operative rehabilitation following SLAP repair is critical for successful outcomes and requires a structured, phased approach to balance protection of the repair with progressive return to function. This protocol applies specifically to a Type II repair and is typically individualized based on surgeon preference, intraoperative findings, and patient factors.
Phase I: Maximum Protection (Weeks 0-6)
- Goals: Protect repair, minimize pain and inflammation, prevent stiffness, begin early motion.
-
Immobilization:
- Sling with abduction pillow worn continuously (except for hygiene and exercises) for 4-6 weeks.
-
Motion:
- Passive range of motion (PROM) initiated early (within the first week) by a qualified therapist.
- Strict precautions: No active shoulder flexion, abduction, or external rotation. No resisted biceps activity. Avoid combined abduction and external rotation, especially during the first 6 weeks.
-
PROM to tolerance:
- Forward flexion: 0-90 degrees.
- External rotation (in scaption/abduction pillow): 0-30 degrees.
- Internal rotation: Restricted.
- Elbow, wrist, and hand AROM exercises initiated immediately.
-
Strengthening:
- None for the shoulder. Isometric bicep contraction is contraindicated.
- Modalities: Ice, NSAIDs for pain and swelling.
- Weight Bearing: Non-weight bearing on the affected arm.
Phase II: Moderate Protection / Early Strengthening (Weeks 7-12)
- Goals: Gradually increase ROM, initiate gentle active motion and rotator cuff strengthening, improve neuromuscular control.
- Immobilization: Sling discontinued, usually at 6 weeks, as tolerated.
-
Motion:
- Gradual progression to full passive ROM.
- Initiate active-assisted range of motion (AAROM) then AROM, respecting pain and surgeon's guidelines.
- Precautions: Continue to avoid resisted biceps activity. Avoid positions of apprehension.
- Progressive AROM for forward flexion, abduction, external, and internal rotation.
-
Strengthening:
- Begin gentle isometric exercises for rotator cuff and scapular stabilizers.
- Light elastic band exercises for internal and external rotation (at side, elbow 90 degrees), scapular retraction.
- Core stability exercises.
- Avoid direct biceps strengthening.
- Functional Activities: Begin light, non-weight-bearing activities of daily living.
Phase III: Minimum Protection / Advanced Strengthening (Weeks 13-20)
- Goals: Restore full pain-free ROM, progressively increase strength and endurance, improve proprioception.
-
Motion:
- Achieve full, pain-free AROM.
- Stretching to address any residual capsular tightness.
-
Strengthening:
- Progressive resistive exercises for rotator cuff and scapular musculature.
- Initiate biceps strengthening with light resistance, gradually increasing load.
- Eccentric strengthening of shoulder musculature.
- Plyometric exercises for power athletes (e.g., medicine ball throws).
- Proprioceptive training (e.g., rhythmic stabilization, balance exercises).
- Functional Activities: Gradual return to more demanding activities, including work-related tasks, but no overhead sports.
Phase IV: Return to Activity (Weeks 21-24+)
- Goals: Return to sport-specific activities, optimize power, endurance, and sport-specific movements.
-
Strengthening:
- Continued advanced strengthening, focusing on power and endurance.
- Sport-specific conditioning and interval throwing programs (for overhead athletes).
-
Return to Sport:
- Requires full pain-free ROM, excellent strength (compared to contralateral side), and no apprehension.
- Gradual progression through sport-specific drills, starting with low intensity and gradually increasing.
- Return to competitive play is typically not before 6 months, and often 9-12 months for overhead athletes.
- Functional testing (e.g., Upper Extremity Functional Index, Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score) should guide decision-making.
Throughout all phases, ongoing assessment by the surgeon and therapist is crucial to ensure appropriate progression and address any setbacks.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- High Index of Suspicion: Persistent, deep shoulder pain, particularly in overhead athletes or following a traumatic event (e.g., FOOSH), warrants suspicion for a SLAP tear, even with negative initial imaging.
- Clinical Examination is Key: While MRI is important, a thorough clinical examination, including specific provocative tests (O'Brien's, Speed's, Yergason's, Compression-Rotation, Biceps Load II), correlating findings with symptom reproduction is paramount. Understand the limitations and specificities of each test. No single test is diagnostic.
- MR Arthrography Superior: For definitive diagnosis of SLAP lesions, especially Type II, MR arthrography significantly improves sensitivity and specificity compared to conventional MRI. It's crucial for pre-operative planning.
- Snyder Classification Guides Treatment: Understand the Snyder classification (Types I-IV) and their respective management strategies (debridement vs. repair vs. tenodesis/tenotomy). Type II is the most common and typically requires repair in active individuals.
-
Arthroscopic Nuances:
- Portals: Proper portal placement (posterior for viewing, anterior-superior and anterior-inferior for working) is essential for adequate visualization and instrument trajectory for superior labral repair.
- Glenoid Preparation: Thorough debridement of frayed labral tissue and decortication of the superior glenoid rim are critical for promoting biological healing.
- Anchor Placement: Anchors should be placed immediately adjacent to the articular cartilage, not too far medially, to ensure anatomical reduction of the labrum. Use appropriate anchor size and type (bioabsorbable).
- Suture Management: Carefully pass sutures through the labrum and biceps anchor, ensuring proper tissue bite and appropriate tensioning. Avoid strangulation or excessive tension.
- Concomitant Pathology: Always perform a complete diagnostic arthroscopy to identify and address any co-existing pathologies (e.g., rotator cuff fraying, subtle instability, biceps pulley lesions, AC joint arthritis).
- Rehabilitation Protocol Adherence: A strict and progressive post-operative rehabilitation protocol, emphasizing early protected motion followed by gradual strengthening and return to activity, is fundamental for successful outcomes and preventing re-injury or stiffness. Biceps restriction in the early phase is non-negotiable for Type II repairs.
- Biceps Tenodesis/Tenotomy Option: For older patients (e.g., >40-50 years old), or those with significant degenerative changes of the biceps tendon, a biceps tenodesis or tenotomy may offer more predictable pain relief and faster recovery compared to SLAP repair, especially for Type II lesions where the biceps anchor is involved. This avoids potential complications of failed SLAP repair or persistent biceps pain.
Pitfalls
- Misdiagnosis: Confusing SLAP tears with other shoulder pathologies (e.g., isolated biceps tendinopathy, impingement, AC joint arthritis) due to overlapping symptoms can lead to inappropriate treatment.
- Over-reliance on Non-Arthrographic MRI: A negative or equivocal non-arthrographic MRI for a clinically suspicious SLAP tear should not deter further investigation with an MR arthrogram.
- Inadequate Glenoid Preparation: Failure to adequately debride the superior glenoid neck and labral edges can result in fibrous non-union or failed healing of the repair.
- Poor Anchor Placement: Placing anchors too far medially on the glenoid neck can lead to insufficient reduction of the labrum, leaving a gap, or placing them too laterally can cause them to pull out. Drilling too steeply into the glenoid can breach the posterior cortex.
- Over-tensioning or Under-tensioning: Over-tensioning the repair can lead to excessive stiffness, while under-tensioning can result in residual laxity and failed healing. Achieving appropriate tension requires experience.
- Ignoring Biceps Pathology: If the biceps tendon itself is degenerated or significantly torn, simply repairing the labrum may not resolve biceps-related pain. Consider tenodesis or tenotomy.
- Aggressive Rehabilitation: Advancing rehabilitation too quickly, especially in the early phases (weeks 0-12), can jeopardize the integrity of the labral repair and lead to re-detachment. Particularly, early active biceps contraction or active overhead motion must be avoided.
- Incomplete Evaluation of Concomitant Pathology: Missing associated lesions (e.g., rotator cuff tear, subscapularis tear, articular cartilage damage) can lead to persistent symptoms despite a successful SLAP repair. Always perform a comprehensive diagnostic arthroscopy.
- Patient Selection: Not all Type II SLAP tears require repair. Consider non-operative management for sedentary individuals or those with low functional demands and minimal symptoms, or consider tenodesis/tenotomy in older patients.
You Might Also Like