Advanced Avascular Necrosis (AVN) of the Femoral Head: A Detailed Orthopedic Case Study

Key Takeaway
Advanced avascular necrosis (AVN) of the femoral head, often Ficat-Arlet Stage IV, presents with intractable hip pain, antalgic gait, and severely restricted range of motion, especially internal rotation. Diagnosis involves plain radiographs showing subchondral collapse and joint space narrowing, confirmed by MRI revealing classic double-line signs, extensive edema, and cartilage loss. Patient history frequently includes chronic corticosteroid use.
Patient Presentation & History
A 45-year-old male presents with a chief complaint of severe, intractable right hip pain, progressively worsening over the past 18 months, significantly impacting his activities of daily living and ambulation. He reports constant deep aching pain localized to the groin, buttock, and lateral hip, exacerbated by weight-bearing, standing, and internal rotation, with nocturnal pain disrupting sleep. He rates his pain as 8/10 on a visual analogue scale. The patient ambulates with a significant antalgic gait, requiring a single crutch for ambulation over short distances.
His medical history is significant for systemic lupus erythematosus (SLE), diagnosed 10 years prior, for which he has been on chronic high-dose corticosteroid therapy (prednisone 10-20mg daily for 8 years, with multiple courses of higher doses for flare-ups). He also reports a history of moderate alcohol consumption (averaging 4-5 units per day) for approximately 15 years, which he has curtailed in the past year. There is no history of prior hip trauma or dislocation.
Approximately 3 years prior, he presented with insidious onset right hip pain and was diagnosed with Ficat-Arlet Stage II avascular necrosis (AVN) of the right femoral head. At that time, he underwent a right hip core decompression with bone marrow aspirate concentrate (BMAC) injection. While this initially provided temporary relief for about 6 months, his symptoms gradually recurred and progressed despite adherence to activity modification and physiotherapy. He reports no prior hip surgery on the left side, which remains asymptomatic. There are no other significant comorbidities relevant to orthopedic surgery apart from SLE.
Clinical Examination
General Inspection
The patient exhibits a noticeable antalgic gait, favoring the right lower extremity, with a shortened stance phase on the affected side. He uses a single crutch for ambulation. Inspection of the right hip reveals no obvious swelling, erythema, or skin changes. There is no limb length discrepancy apparent in a standing position, but a mild Trendelenburg sign is noted on the right side during single-leg stance. Muscle atrophy of the right gluteal and thigh musculature is evident when compared to the contralateral side.
Palpation
Palpation reveals tenderness over the anterior hip capsule, particularly in the region of the anterior superior iliac spine (ASIS) and greater trochanter. There is no palpable warmth or swelling. Distal pulses (femoral, popliteal, dorsalis pedis, posterior tibial) are bilaterally strong and symmetric. No palpable masses.
Range of Motion (ROM)
Active and passive range of motion of the right hip is significantly restricted and painful:
*
Flexion:
Limited to 70 degrees (contralateral 110 degrees) with pain at end-range.
*
Extension:
Limited to 0 degrees (contralateral 10 degrees hyperextension).
*
Abduction:
Limited to 15 degrees (contralateral 40 degrees) with pain.
*
Adduction:
Limited to 10 degrees (contralateral 20 degrees).
*
Internal Rotation:
Severely restricted to 0-5 degrees with excruciating pain (contralateral 30 degrees). This is a hallmark finding in advanced femoral head pathology.
*
External Rotation:
Limited to 20 degrees (contralateral 45 degrees).
A flexion-adduction-internal rotation (FADDIR) test elicits significant groin pain, indicative of femoroacetabular impingement secondary to femoral head collapse and osteophyte formation. The Straight Leg Raise (SLR) test is negative bilaterally.
Neurological & Vascular Assessment
Neurological examination of the right lower extremity reveals intact motor strength (5/5 in all major muscle groups: hip flexors, extensors, abductors, adductors; knee flexors, extensors; ankle dorsiflexors, plantarflexors) and sensation to light touch and pinprick in all dermatomes (L2-S1). Deep tendon reflexes (patellar and Achilles) are 2+ and symmetrical bilaterally. Vascular assessment confirms strong palpable pedal pulses bilaterally with normal capillary refill time (<2 seconds) in all toes, indicating no evidence of acute neurovascular compromise.
Imaging & Diagnostics
Initial Radiographs (Weight-Bearing AP Pelvis, Frog-Leg Lateral, True Lateral of Right Hip)
Initial plain radiographs confirm advanced avascular necrosis of the right femoral head.
*
AP Pelvis:
Demonstrates significant flattening and collapse of the superior aspect of the right femoral head. There is a subchondral lucency ("crescent sign") indicative of subchondral fracture, consistent with Ficat-Arlet Stage IV AVN. Sclerosis and cystic changes are evident within the femoral head. There is secondary osteoarthritic change in the acetabulum, with joint space narrowing and acetabular osteophytes, particularly superiorly.
*
Frog-Leg Lateral and True Lateral Views:
Further delineate the extent of femoral head collapse and involvement of the anterior and superior weight-bearing surfaces. The loss of sphericity of the femoral head is pronounced.
Advanced Imaging (MRI and CT)
Given the progression of symptoms and advanced changes on plain radiographs, further advanced imaging was obtained.
-
Magnetic Resonance Imaging (MRI) of the Right Hip:
- T1-weighted sequences: Showed low signal intensity in the femoral head, surrounded by a "double-line sign" on T2-weighted images, highly characteristic of AVN. The necrotic segment involved a significant portion of the superior and anterior weight-bearing femoral head (estimated >30% volume).
- T2-weighted and STIR sequences: Confirmed extensive edema within the femoral head and surrounding bone marrow, indicating active disease. Articular cartilage loss was evident superiorly, corresponding to the area of subchondral collapse. No significant soft tissue pathology, such as labral tears or abductor tendon pathology, was identified as a primary driver of symptoms, though secondary adaptive changes were noted. The MRI was critical in confirming the extent of necrosis, articular collapse, and evaluating the integrity of the surrounding cartilage and subchondral bone, confirming Ficat-Arlet Stage IV disease with secondary osteoarthritis.
-
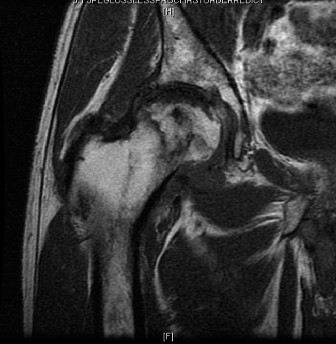
Figure 1: Pre-operative MRI of the right hip demonstrating extensive avascular necrosis of the femoral head (Ficat-Arlet Stage IV) with characteristic double-line sign, significant subchondral collapse, and early secondary degenerative changes in the acetabulum.
-
Computed Tomography (CT) Scan of the Right Hip:
- CT provided detailed assessment of the bone morphology, quantifying the extent of femoral head collapse, subchondral bone loss, and integrity of the acetabulum. It confirmed the presence of large cysts and sclerotic changes within the femoral head, with significant flattening. The CT scan was crucial for pre-operative templating, allowing for precise measurement of femoral canal dimensions, acetabular bone stock, and identification of any potential difficulties for implant placement or bone grafting requirements. The acetabular roof showed evidence of remodeling and minimal superior migration of the femoral head, indicating advanced degenerative changes.
Pre-operative Templating
Detailed digital templating was performed using specialized software on AP pelvis and lateral hip radiographs, augmented by CT data.
*
Femoral Component:
Multiple stem types and sizes (cemented vs. cementless, standard vs. custom) were templated to address potential proximal femoral bone loss or distortion. Given the patient's age and activity level, a cementless, modern tapered or conical stem was initially preferred. Measurements confirmed a relatively normal femoral canal, allowing for a standard stem length.
*
Acetabular Component:
Various acetabular cup sizes, designs (hemispherical, highly porous), and augments (wedges, cages) were templated. The goal was to achieve adequate press-fit and primary stability despite potential acetabular bone loss. The CT data highlighted the need for potential superior rim reaming and the possibility of bone grafting or specific cup positioning to achieve optimal coverage and stability.
Differential Diagnosis
A comprehensive differential diagnosis for hip pain in a 45-year-old male with chronic corticosteroid use and alcohol history presenting with advanced hip pathology is essential.
| Diagnosis | Key Features | Diagnostic Workup | Distinction from AVN |
|---|---|---|---|
| Avascular Necrosis (AVN) of the Femoral Head (Current Case) |
- Insidious onset, progressive groin pain
- History of corticosteroid use, alcohol abuse - Restricted, painful ROM (especially internal rotation) - Antalgic gait - Radiographs: crescent sign, flattening, sclerosis, joint space narrowing (late) - MRI: "double-line sign" (diagnostic), edema, necrotic segment. |
-
Plain Radiographs (AP, lateral):
Essential for initial staging.
- MRI (T1/T2/STIR): Gold standard for early diagnosis and staging. - CT Scan: Useful for detailed bone morphology and pre-operative planning. |
Primary diagnosis based on pathognomonic MRI findings and characteristic radiographic progression. The patient's history and prior imaging confirmed AVN progression. Other differentials are typically considered before AVN is confirmed or if the presentation is atypical. Secondary OA in this context is a consequence of AVN. |
| Primary Osteoarthritis (OA) of the Hip |
- Gradual onset, chronic groin/buttock pain
- Worse with activity, relieved by rest (initially) - Restricted ROM (loss of internal rotation early) - Stiffness, crepitus - No specific systemic risk factors (unless post-traumatic, developmental) - Radiographs: joint space narrowing, osteophytes, subchondral sclerosis, subchondral cysts (not crescent sign). |
-
Plain Radiographs (AP, lateral):
Primary diagnostic tool.
- MRI: To rule out other intra-articular pathology or assess cartilage if radiographs are equivocal. |
Unlike AVN, primary OA typically involves diffuse cartilage loss and bony remodeling without a distinct necrotic segment or "crescent sign" in its early stages. The onset is often more insidious and directly related to age/wear-and-tear. In advanced AVN, secondary OA changes can mimic primary OA, but the etiology is distinct. |
| Transient Osteoporosis of the Hip (TOH) |
- Acute/subacute onset of hip pain, typically in middle-aged men or third-trimester pregnant women.
- No history of trauma. - Painful weight-bearing, restricted ROM. - Radiographs: often normal initially, then patchy osteopenia. - MRI: extensive bone marrow edema (diffuse low signal on T1, high on T2/STIR) but no necrotic segment or "double-line sign." Resolves spontaneously within 6-12 months. |
-
Plain Radiographs:
Often normal initially.
- MRI: Crucial for diagnosis, demonstrating diffuse marrow edema without necrosis. - Bone Scan: Increased uptake. |
TOH lacks the distinct necrotic focus and the "double-line sign" seen on MRI in AVN. It is a self-limiting condition with diffuse edema, whereas AVN progresses to collapse. The patient's chronic symptoms and radiographic changes rule out TOH. |
| Femoral Neck Stress Fracture |
- Acute or subacute onset of pain, often after increased activity or impact.
- Pain with weight-bearing and impact loading. - Tenderness to palpation in the groin/trochanteric region. - Radiographs: subtle lucency or sclerosis along the femoral neck (if displaced, obvious fracture line). - MRI: line of low signal on T1, surrounding edema. |
-
Plain Radiographs:
May be normal, especially in early non-displaced fractures.
- MRI: High sensitivity for detecting stress fractures and associated edema. |
While a stress fracture could present with pain and altered gait, it would typically have a more acute onset related to activity and a distinct fracture line on imaging rather than the diffuse avascular changes and collapse of the femoral head. No history of recent increased activity or trauma. |
| Greater Trochanteric Pain Syndrome (GTPS) / Bursitis |
- Lateral hip pain, tenderness over the greater trochanter.
- Pain worse with lying on affected side, walking, stair climbing. - Often associated with gluteus medius/minimus tendinopathy or tears. - Normal hip ROM or pain only at end-range abduction/external rotation. |
-
Clinical Examination:
Localized tenderness, specific pain provocation tests.
- Ultrasound/MRI: To assess for bursal inflammation or gluteal tendinopathy/tears. |
This diagnosis is typically characterized by lateral hip pain and localized tenderness over the greater trochanter, with often preserved internal rotation. While it can co-exist, the patient's dominant groin pain and severe restriction of internal rotation point away from isolated GTPS. |
Surgical Decision Making & Classification
The patient's clinical presentation, coupled with advanced imaging, clearly indicates progression to Ficat-Arlet Stage IV avascular necrosis of the right femoral head. This stage is characterized by flattening and collapse of the femoral head, subchondral fracture (crescent sign), and secondary degenerative changes in the acetabulum. The Steinberg classification also places this in Stage IV or V, indicating significant articular surface involvement.
Why Operative vs. Non-Operative?
Given the Ficat-Arlet Stage IV classification, the prognosis for non-operative management is exceptionally poor.
*
Non-operative management:
In Ficat-Arlet Stages I and II, non-operative measures such as activity modification, bisphosphonates, anti-coagulants, lipid-lowering agents, and protected weight-bearing can be considered, often in conjunction with core decompression. However, once articular collapse has occurred (Stage III onwards), these measures are largely ineffective in preventing further collapse or alleviating symptoms. The patient has already failed core decompression with BMAC, underscoring the aggressive nature of his disease and the futility of further non-operative interventions. The persistent, severe pain and functional impairment warrant definitive surgical intervention.
Surgical Options for Advanced AVN (Ficat-Arlet Stage IV)
For Ficat-Arlet Stage IV AVN, the primary goal shifts from joint preservation to joint reconstruction or replacement. The patient's age (45 years old) and prior attempt at joint preservation complicate decision-making.
- Arthrodesis: While historically an option for young, active patients with end-stage hip disease, it results in significant functional limitations and is rarely performed today, especially with advances in arthroplasty. Not suitable for this patient given his desire for functional mobility.
- Femoral Head Osteotomy: Rotational osteotomies can shift the necrotic segment away from the weight-bearing zone. This is typically reserved for early-stage AVN (Ficat-Arlet Stage I/II) with relatively small lesions and intact articular cartilage. Given the extensive collapse and secondary acetabular changes, this is not an option.
- Hemiarthroplasty: Replacing only the femoral head. While simpler, it has high rates of acetabular erosion and pain in active patients. Generally reserved for elderly, low-demand patients with femoral neck fractures. Not appropriate for this relatively young, active patient.
- Resurfacing Arthroplasty: Involves capping the femoral head with a metal shell and placing a thin metal cup in the acetabulum. This preserves more femoral bone stock. However, it requires a healthy, well-contained femoral head with minimal collapse, which is not the case here. Concerns about metal-on-metal bearing surfaces in younger patients also exist.
- Total Hip Arthroplasty (THA): This is the gold standard for end-stage hip arthritis and is highly effective for pain relief and functional restoration in AVN with collapse. For a 45-year-old patient, concerns include implant longevity, wear, and the potential need for future revisions. However, with modern bearing surfaces and implant designs, outcomes in younger patients have significantly improved.
Surgical Decision
Considering the patient's age, activity level, significant femoral head collapse (Ficat-Arlet Stage IV), and failed previous joint-preserving surgery, a Total Hip Arthroplasty (THA) was deemed the most appropriate and effective surgical intervention. The goal was to provide durable pain relief and restore functional mobility. Given the possibility of secondary acetabular bone loss, careful templating and planning for potential augmentation or revision strategies were paramount. The choice of bearing surface and fixation would be critical for long-term outcomes in a younger, potentially active individual. A cementless fixation strategy with a large diameter ceramic-on-ceramic bearing was planned to optimize durability and minimize wear-related complications.
Surgical Technique / Intervention
The patient underwent an elective right total hip arthroplasty.
Pre-operative Preparation
- Antibiotic Prophylaxis: Intravenous cefazolin 2g administered 60 minutes prior to incision, with appropriate dosing for patient weight and renal function.
- Deep Venous Thrombosis (DVT) Prophylaxis: Mechanical compression devices (intermittent pneumatic compression) applied pre-operatively.
- Templating Review: Final review of templating to confirm implant sizes and potential intra-operative challenges.
- Blood Management: Type and cross-match blood was available, though not routinely transfused for primary THA.
Patient Positioning
The patient was positioned in the left lateral decubitus position on a standard fracture table, ensuring proper padding of all pressure points. The right lower extremity was draped free to allow for full range of motion intra-operatively. A beanbag was used for stability, and an axillary roll was placed to protect the brachial plexus.
Surgical Approach
A standard
posterior approach
(Kocher-Langenbeck) was utilized.
1.
Incision:
A curvilinear incision was made centered over the greater trochanter, extending proximally along the iliac crest and distally along the femur.
2.
Deep Dissection:
The fascia lata was incised, and the gluteus maximus fibers were split. The short external rotators (piriformis, obturators, gemelli, quadratus femoris) and conjoined tendon were identified and released from their femoral insertion with a small wafer of bone, preserving the neurovascular structures. The sciatic nerve was identified and protected.
3.
Capsulotomy:
A T-shaped capsulotomy was performed.
4.
Femoral Head Dislocation:
The hip was dislocated by internally rotating and adducting the limb, bringing the femoral head out of the acetabulum.
Femoral Osteotomy and Preparation
- Femoral Neck Osteotomy: A precise femoral neck osteotomy was performed with an oscillating saw, typically 1 cm proximal to the lesser trochanter, guided by pre-operative templating. The resected femoral head was removed for pathological examination.
-
Femoral Canal Preparation:
- The femoral canal was opened using a box osteotome.
- Progressive reaming of the femoral canal was performed using appropriately sized intramedullary reamers until cortical contact was achieved. This ensured proper fit and alignment for the femoral stem.
- Sequential broaching was performed with increasing sizes until solid stability and appropriate anteversion were achieved, confirming the final broach size corresponded to the templated stem.
- The trial femoral neck and head were assembled onto the broach.
Acetabular Preparation
- Acetabular Reaming: The acetabulum was prepared by excising the labrum and osteophytes, then reaming with sequential hemispherical reamers. Reaming commenced with a smaller reamer to establish the true acetabular floor and was progressively increased in size by 1-2 mm increments until healthy, bleeding subchondral bone was exposed, ensuring a press-fit of the chosen implant. Care was taken to preserve the anterior and posterior walls.
- Debridement: All remaining cartilage and sclerotic bone from the acetabular floor were meticulously debrided.
- Acetabular Component Insertion: A highly porous, cementless hemispherical acetabular component (e.g., plasma-sprayed titanium) was impacted into the prepared acetabulum, aiming for 40 degrees of abduction and 15-20 degrees of anteversion. Initial stability was assessed. Two-to-three supplementary screws were placed through the screw holes in the cup into the ilium and ischium, avoiding danger zones (superior gluteal nerve/vessels, sciatic nerve, obturator nerve/vessels).
- Liner Insertion: A ceramic liner was locked securely into the metal shell.
Final Trial Reduction and Leg Length Assessment
- Trial Assembly: The trial femoral stem with the appropriate neck length (offset) and ceramic head was assembled.
- Reduction: The hip was reduced.
- Stability Assessment: Dynamic assessment of hip stability in flexion, extension, internal and external rotation was performed.
- Leg Length & Offset: Careful assessment of leg length was performed using intra-operative landmarks (ischial tuberosity, medial malleoli), visual comparison, and the "shuck test." Offset was confirmed to optimize abductor mechanics. Adjustments to femoral neck length or head size were made as necessary to achieve optimal stability, leg length equality, and soft tissue tension.
Final Implant Insertion
- Femoral Stem Insertion: The trial components were removed. The definitive cementless femoral stem was impacted into the prepared femoral canal.
- Final Head Insertion: The ceramic femoral head was impacted onto the femoral stem taper.
-
Final Reduction:
The hip was reduced.
-

Figure 2: Post-operative AP radiograph of the right hip demonstrating a well-fixed cementless total hip arthroplasty with an appropriately sized ceramic-on-ceramic bearing, restoring hip biomechanics and leg length. The femoral stem is aligned centrally in the femoral canal, and the acetabular component shows excellent coverage and screw fixation.
-
Closure
- Capsular Repair: The released short external rotators and posterior capsule were meticulously repaired through drill holes in the greater trochanter and/or reattachment to the posterior capsule and gluteus maximus, which significantly reduces dislocation risk.
- Fascial Closure: The fascia lata was closed.
- Subcutaneous and Skin Closure: Layered closure of subcutaneous tissues and skin was performed. A sterile dressing was applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-3)
- Pain Management: Multimodal analgesia including regional blocks (e.g., fascia iliaca block), oral opioids, NSAIDs (if no contraindications), and acetaminophen.
- DVT Prophylaxis: Continued mechanical prophylaxis (SCDs) and pharmacological prophylaxis (e.g., low molecular weight heparin or oral anticoagulants) initiated according to hospital protocol and patient risk factors.
- Weight-Bearing: Immediate weight-bearing as tolerated (WBAT) with the aid of a walker or crutches.
-
Physiotherapy:
Early mobilization is crucial.
- Day 0: Ankle pumps, quad sets, gluteal sets.
- Day 1: Sitting on the edge of the bed, supervised transfers to chair, short ambulation with walker.
- Day 2-3: Progressive ambulation, stair training if appropriate.
-
Hip Precautions (Posterior Approach):
Strict adherence to posterior hip precautions to minimize dislocation risk:
- Avoid hip flexion >90 degrees.
- Avoid hip adduction past midline.
- Avoid hip internal rotation.
- Use an abduction pillow when lying in bed.
- No crossing legs.
Early Rehabilitation (Weeks 1-6)
- Home/Inpatient Rehab: Patients typically discharged home with outpatient physical therapy or to an inpatient rehabilitation facility based on functional status and support.
-
Therapeutic Exercises:
Focus on restoring strength and range of motion while respecting precautions.
- Strengthening: Hip abductor strengthening (side-lying abduction, standing abduction), quadriceps strengthening (straight leg raises), hamstring curls, gluteal strengthening (bridging).
- Range of Motion: Gentle hip flexion, abduction, and external rotation within safe limits. Avoid painful movements.
- Gait Training: Progression from walker to crutches, then to a single cane as strength and balance improve. Focus on normalizing gait pattern.
- Activities of Daily Living (ADLs): Training on proper techniques for dressing, bathing, and transfers with hip precautions. Adaptive equipment may be recommended.
- Wound Care: Incision monitoring for signs of infection. Suture/staple removal at 10-14 days.
Intermediate Rehabilitation (Weeks 6-12)
- Discontinuation of Precautions: Depending on surgeon preference and patient progress, hip precautions may be discontinued after 6-8 weeks, assuming strong capsular repair and no concerns for instability.
- Advanced Strengthening: Increased resistance and complexity of exercises. Introduction of closed-chain exercises, proprioceptive training.
- Balance Training: Single-leg stance, dynamic balance exercises.
- Return to Light Activities: Gradual return to recreational activities such as cycling (stationary), swimming.
- Gait Aid Progression: Transition from cane to no gait aid.
Long-Term Rehabilitation (Beyond 12 Weeks)
- Functional Progression: Focus on optimizing strength, endurance, and function for desired activities.
- Impact Activities: Avoid high-impact activities (e.g., running, jumping, contact sports) to minimize wear on the prosthetic components. Low-impact sports are generally encouraged.
- Regular Follow-ups: Clinical and radiographic follow-up at 3 months, 6 months, 1 year, and annually thereafter to monitor implant integration, alignment, and for signs of wear or loosening.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Early Diagnosis & Staging: In AVN, early diagnosis (Ficat-Arlet Stages I/II, Steinberg I/II) via MRI is paramount. This is the window for joint-preserving procedures like core decompression, vascularized fibular grafting, or osteotomies. Missing this window significantly limits options.
- Risk Factor Management: Aggressive management of underlying risk factors (e.g., corticosteroid withdrawal/dose reduction, alcohol cessation, hyperlipidemia treatment, coagulopathy management) is critical for both preventing AVN and optimizing outcomes post-intervention.
- Templating for Complex THA: For advanced AVN with collapse, pre-operative templating (both digital and manual) using X-rays and CT is non-negotiable. It allows for anticipation of bone defects (femoral head, acetabular rim), identification of canal morphology, and precise implant sizing and positioning, especially for managing leg length and offset.
- Femoral Head Preservation in Young Patients: For younger patients (under 50) with early-stage AVN, joint-preserving procedures are always the first consideration, provided the lesion size and articular integrity are favorable. Total hip arthroplasty, while effective, commits a young patient to a revision pathway.
- Reconstruction for Collapse: Once femoral head collapse and articular incongruity occur (Ficat-Arlet Stage III/IV), Total Hip Arthroplasty (THA) generally becomes the most reliable solution for pain relief and functional restoration. Do not delay definitive treatment once failure of joint preservation is evident, as prolonged pain impacts patient function and quality of life.
- Bearing Surface Selection: In young, active patients undergoing THA for AVN, consider advanced bearing surfaces (e.g., ceramic-on-ceramic or ceramic-on-polyethylene) to minimize wear and improve longevity. Large diameter heads can enhance stability but require careful consideration of associated risks.
- Surgical Approach: Be proficient in approaches that allow good exposure and facilitate reconstruction. The posterior approach offers excellent visualization for both femoral and acetabular components, and meticulous capsular repair significantly reduces dislocation rates.
- Sciatic Nerve Protection: During a posterior approach, constant vigilance is required to identify and protect the sciatic nerve, particularly during retraction and external rotator release/repair.
Pitfalls
- Delay in Diagnosis: Misinterpreting early AVN as transient osteoporosis, hip strain, or bursitis can lead to delayed diagnosis and progression to collapse, limiting joint-preserving options.
- Inadequate Core Decompression: If core decompression is performed too superficially or without adjuvant bone graft/BMAC in appropriate cases, it may not adequately relieve intraosseous pressure or stimulate revascularization, leading to early failure.
- Underestimation of Bone Loss: Advanced AVN often involves significant subchondral bone loss and cystic changes. Underestimating this pre-operatively can lead to challenges in achieving stable implant fixation, requiring unexpected bone grafting or specialized implants intra-operatively.
- Dislocation Post-THA: A common complication, particularly with the posterior approach if the posterior capsule and external rotators are not meticulously repaired. Failure to adhere to post-operative hip precautions (especially in the first 6-12 weeks) is another major risk factor.
- Leg Length Discrepancy: Incorrect restoration of leg length can lead to patient dissatisfaction, gait abnormalities, and sciatic nerve palsy (if lengthened significantly). Meticulous intra-operative measurement techniques are critical.
- Heterotopic Ossification (HO): Patients with AVN are at higher risk for HO post-THA, particularly after a posterior approach. Prophylaxis with NSAIDs or low-dose radiation should be considered in high-risk patients.
- Infection: As with any major arthroplasty, periprosthetic joint infection remains a devastating complication. Strict aseptic technique, appropriate antibiotic prophylaxis, and careful wound management are essential. Patients on chronic immunosuppression (e.g., for SLE) may be at increased risk.
- Failure to Address Etiology: For ongoing risk factors (e.g., continued high-dose corticosteroids, persistent alcohol abuse), discuss the importance of medical management with the patient and their primary care provider to prevent contralateral hip or other joint involvement.
Clinical & Radiographic Imaging
You Might Also Like