Clinical Case Study: Distal Femoral Osteosarcoma Diagnosis & Management
Key Takeaway
Diagnosing adolescent distal femoral osteosarcoma involves evaluating progressive bone pain, followed by comprehensive imaging. Radiographs show aggressive lytic/sclerotic lesions; MRI details local tumor extent and neurovascular involvement. CT chest screens for metastases. A CT-guided core needle biopsy provides the definitive histopathological diagnosis, essential for tailoring effective orthopedic oncology treatment.
Patient Presentation & History
A 16-year-old male presented to the orthopedic clinic with a chief complaint of progressive right distal thigh and knee pain for approximately 4 months. Initially, the pain was intermittent and activity-related, attributed by the patient to sports participation (basketball). However, over the past 6 weeks, the pain had become constant, insidious in onset, significantly worse at night, and was poorly controlled with over-the-counter analgesics, including NSAIDs. He reported waking frequently due to pain and experiencing an increasing limp, particularly with weight-bearing activities. He denied any specific traumatic event leading to the onset of symptoms, recent fevers, chills, or night sweats. There was no reported history of weight loss. His past medical history was unremarkable, and he was otherwise healthy and active. Family history was non-contributory for malignancy or genetic syndromes. He was a non-smoker and denied recreational drug use.
Clinical Examination
On general inspection, the patient appeared thin but in no acute distress at rest. An antalgic gait was noted upon ambulation. Local examination of the right lower extremity revealed subtle but noticeable swelling in the distal thigh region, specifically around the distal femur. There was no overt erythema or ecchymosis. Prominent superficial venous engorgement was observed over the anteromedial aspect of the distal thigh.
Palpation revealed a firm, fixed, and exquisitely tender mass palpable over the anterior and medial aspects of the distal right femur, approximately 5 cm proximal to the joint line. The mass measured roughly 8 x 6 cm. Localized warmth was present over the lesion. There was no regional lymphadenopathy.
Range of motion (ROM) of the right knee was limited by pain, particularly at the extremes of flexion (0-90 degrees, compared to 0-140 degrees on the contralateral side) and extension (lacked 5 degrees extension). Patellar tracking was grossly normal. Ligamentous stability testing was deferred due to significant pain and concern for structural compromise.
Neurological examination of the right lower extremity revealed intact motor strength (5/5) in all major muscle groups distal to the knee, including ankle dorsiflexion, plantarflexion, toe extension, and flexion. Sensation was intact to light touch in all dermatomes (L2-S1). Deep tendon reflexes (patellar and Achilles) were 2+ bilaterally and symmetric.
Vascular assessment demonstrated palpable pedal pulses (dorsalis pedis and posterior tibial) bilaterally, with good capillary refill in the toes of the affected limb. No bruits were audible over the mass or adjacent major vessels.
A comprehensive examination of the ipsilateral hip and contralateral lower extremity was unremarkable.
Imaging & Diagnostics
Initial diagnostic workup commenced with plain radiographs of the right knee and femur.
Radiographic findings
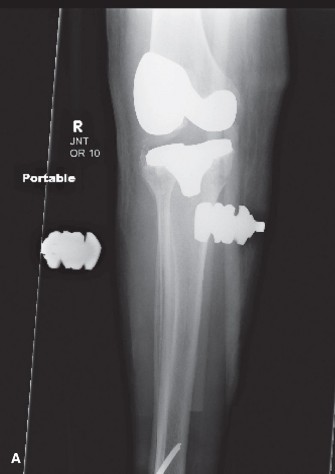
of the distal right femur demonstrated an aggressive, mixed lytic and sclerotic lesion centered in the metaphysis. Features included significant cortical destruction, spiculated periosteal reaction ("sunburst" pattern), and an ill-defined Codman's triangle along the anteromedial cortex. A large associated soft tissue mass was also evident, extending beyond the bone confines. There was no evidence of a pathologic fracture at this stage.
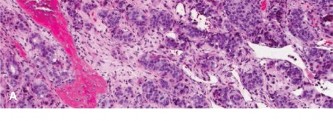
Figure 1: Anteroposterior radiograph of the distal femur demonstrating a mixed lytic and sclerotic lesion with extensive periosteal reaction and cortical breach.
Following the plain radiographs, further advanced imaging was immediately pursued. A Magnetic Resonance Imaging (MRI) scan of the entire right femur with contrast was performed for detailed local staging. The MRI confirmed a large, heterogeneous mass arising from the distal femoral metaphysis, measuring approximately 8.5 x 6.2 x 9.0 cm (AP x ML x CC). The lesion demonstrated aggressive features including:
* Extensive intramedullary involvement, extending from the articular surface proximally into the diaphysis, crossing the physis.
* Significant cortical destruction with a large extraosseous soft tissue component, demonstrating avid contrast enhancement.
* Peritumoral edema extending proximally along the marrow.
* Close proximity and likely encasement of the neurovascular bundle (femoral artery and nerve, specifically the saphenous nerve and artery within the adductor canal).
* No evidence of skip lesions within the ipsilateral femur.
* No joint effusion or intra-articular extension was noted.
Figure 2: Coronal T2-weighted MRI demonstrating the aggressive nature of the tumor, its intramedullary and extraosseous soft tissue extent, and relationship to the surrounding neurovascular structures.
A Computed Tomography (CT) scan of the chest was performed to screen for pulmonary metastases, which are the most common site for osteosarcoma dissemination. The CT chest was unremarkable, revealing no definitive lung nodules or other metastatic foci. A Technetium-99m bone scan was also performed to rule out other osseous metastases, which was negative.
Given the strong clinical and radiological suspicion for an aggressive primary bone sarcoma, a percutaneous core needle biopsy was performed under CT guidance. The biopsy was planned carefully to ensure the incision would be longitudinal and in line with any potential future definitive surgical incision, minimizing contamination of uninvolved tissue planes. Multiple cores were obtained from both the osseous and soft tissue components of the lesion.

Figure 3: CT-guided core needle biopsy of the distal femur lesion, demonstrating the precise targeting of the tumor for adequate tissue acquisition.
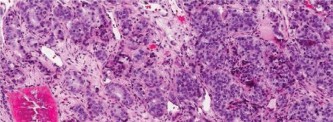
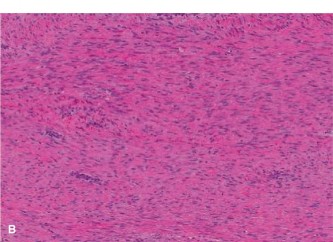
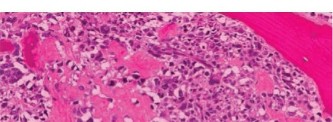
Histopathological examination of the biopsy specimens revealed malignant stromal cells producing osteoid and immature woven bone, characteristic of high-grade osteosarcoma. The cells exhibited marked pleomorphism, hyperchromatic nuclei, and frequent mitotic figures. Neoplastic osteoid was present directly from malignant cells.

Figure 4: High-power photomicrograph of the biopsy specimen showing malignant pleomorphic stromal cells producing osteoid matrix, confirming the diagnosis of osteosarcoma.
The final diagnosis was conventional high-grade osteosarcoma of the distal right femur, Stage IIB according to the Enneking surgical staging system (high-grade, intra-compartmental, no regional or distant metastases).
Differential Diagnosis
The clinical presentation and initial imaging findings necessitated a broad differential diagnosis for an aggressive bone lesion in an adolescent. Key differentials considered included:
| Feature | Osteosarcoma | Ewing Sarcoma | Chronic Osteomyelitis (Garre's Sclerosing) |
|---|---|---|---|
| Demographics | Bimodal (10-20 yrs, >60 yrs secondary); slightly male predominance. | Predominantly 10-20 yrs; slight male predominance. | Any age, often related to trauma, previous infection, or immunocompromise. |
| Location | Metaphysis of long bones (distal femur, proximal tibia, proximal humerus). | Diaphysis or metadiaphysis of long bones, pelvis, ribs. | Metaphysis of long bones (esp. tibia, femur), often related to growth plates. |
| Pain Character | Insidious, progressive, deep, constant, worse at night, unresponsive to NSAIDs. | Localized pain, often with systemic symptoms (fever, malaise, weight loss). | Localized pain, waxing and waning, warmth, swelling; potentially with sinus tract. |
| Systemic Sx | Rare. | Common (fever, leukocytosis, elevated ESR/CRP, anemia). | Common during acute exacerbations (fever, elevated inflammatory markers). |
| Radiographs | Mixed lytic/sclerotic, cortical destruction, sunburst/Codman's triangle periosteal reaction, soft tissue mass. | Lytic, permeative destruction, classic "onion-skin" periosteal reaction, large soft tissue mass. | Sclerosis, cortical thickening (involucrum), lucent areas (sequestrum), cloaca/fistula. |
| MRI | Heterogeneous signal, intramedullary extent, skip lesions, neurovascular encasement. | Large soft tissue component, periosteal elevation, bone marrow edema, neurovascular involvement. | Marrow edema, periosteal fluid/thickening, sinus tracts, phlegmon, abscess formation. |
| Biopsy | Malignant stromal cells producing osteoid matrix. High-grade pleomorphism. | Small round blue cell tumor; immunohistochemistry: CD99 positive. FISH for EWS-FLI1 translocation. | Inflammatory cells, necrosis, sequestrum; positive bacterial cultures. |
| Treatment | Neoadjuvant chemotherapy, wide en bloc resection, adjuvant chemotherapy. | Neoadjuvant chemotherapy, surgery and/or radiation, adjuvant chemotherapy. | Antibiotics (long-term), surgical debridement (sequestrectomy, involucrum removal). |
Surgical Decision Making & Classification
Given the diagnosis of high-grade conventional osteosarcoma of the distal femur (Enneking Stage IIB), a multimodal treatment approach was initiated. The primary goal was limb salvage with wide surgical margins, while addressing systemic micrometastases.
Neoadjuvant Chemotherapy:
The patient was commenced on a standard neoadjuvant chemotherapy regimen, typically consisting of regimens such as MAP (Methotrexate, Adriamycin (Doxorubicin), Cisplatin). The objectives of neoadjuvant chemotherapy are several-fold:
1.
Tumor Necrosis:
To reduce the viable tumor burden, making surgical resection easier and potentially achieving better margins.
2.
Shrinkage of Soft Tissue Component:
To decrease the overall tumor size, potentially converting a borderline resectable tumor into a definitively resectable one, and improving the safety margin around critical neurovascular structures.
3.
Treatment of Micrometastases:
To address any subclinical distant metastases, which are often present at diagnosis even if not radiologically evident.
4.
Assessment of Chemosensitivity:
To evaluate the tumor's response to chemotherapy, which is a critical prognostic indicator (≥90% tumor necrosis correlates with improved survival).
After three cycles of neoadjuvant chemotherapy, follow-up MRI demonstrated a significant reduction in the size of both the intraosseous and extraosseous components of the tumor, with evidence of sclerosis within the lesion. The tumor's proximity to the neurovascular bundle appeared less critical due to tumor shrinkage, suggesting a more favorable plane for dissection. This positive response indicated good chemosensitivity, which boded well for prognosis.
Surgical Planning:
The goal for definitive surgery was a
wide en bloc resection
with clear oncological margins. Based on the MRI findings post-chemotherapy and the anticipated extent of resection to achieve a wide margin, a segmental resection of the distal femur including the involved metaphysis, epiphysis, and a portion of the diaphysis was planned. The estimated bone defect would necessitate a custom or modular endoprosthetic reconstruction.
Reconstruction Options Considered:
*
Modular Endoprosthesis:
This was the preferred option due to its reliability, immediate stability, and predictable functional outcome for a patient of this age and activity level. It allows for length restoration and immediate weight-bearing (with appropriate precautions).
*
Allograft-Prosthesis Composite:
While offering biological fixation and potentially better long-term durability, the risks of non-union, infection, and allograft fracture are higher, and it requires a longer rehabilitation period.
*
Rotationplasty (Van Nes procedure):
An excellent option for very young children with distal femoral sarcomas, providing durable function and growth potential. However, for a 16-year-old, the psychological impact and cosmetic outcome are often less acceptable, and growth potential is no longer a primary concern.
*
Arthrodesis:
While oncologically sound, it results in significant functional limitations and was deemed undesirable for an active adolescent.
After multidisciplinary discussion involving the orthopedic oncologist, medical oncologist, and patient/family, a decision was made for a wide en bloc resection of the distal femur with reconstruction using a modular distal femoral endoprosthesis.
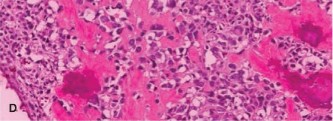
Figure 5: Pre-operative planning image, illustrating the proposed osteotomy lines for wide en bloc resection of the distal femur, ensuring adequate oncological margins (dashed lines).
Surgical Technique / Intervention
The patient was positioned supine on the operating table. A high thigh tourniquet was applied but not inflated initially, reserving its use for critical moments of dissection if necessary to reduce blood loss and enhance visualization of surgical planes, particularly around the neurovascular bundle. A sandbag was placed under the ipsilateral hip to allow for external rotation of the limb. Prophylactic intravenous antibiotics were administered.
A long anterior longitudinal incision was made, centered over the distal femur, extending from the mid-thigh proximally to just distal to the patella. The incision was designed to encompass the biopsy scar and ensure adequate exposure for both resection and reconstruction. Full thickness skin flaps were elevated carefully.
The vastus medialis and vastus lateralis were mobilized and retracted. The rectus femoris and vastus intermedius were carefully detached from the anterior femur proximally. The patella was everted laterally to expose the knee joint. The joint capsule was incised circumferentially, staying clear of any suspected tumor involvement.
Careful subperiosteal dissection was performed proximally to the planned osteotomy, meticulously separating musculature from the bone. The neurovascular bundle (femoral artery, vein, and saphenous nerve) in the adductor canal was identified and protected. Dissection around the tumor was performed with extreme caution, maintaining an adequate cuff of normal tissue surrounding the gross tumor to achieve wide margins. This was particularly critical on the posteromedial aspect where the bundle lies. Intraoperative frozen sections were considered if there was any doubt regarding margin adequacy, but were not deemed necessary in this case due to clear macroscopic margins.
The distal femoral osteotomy was performed proximally to the tumor, confirming clean bone via intraoperative imaging and visual inspection. The posterior knee capsule, cruciate ligaments, and collateral ligaments were incised or detached as appropriate to facilitate tumor removal. The entire distal femur, including the tumor, was then resected en bloc.
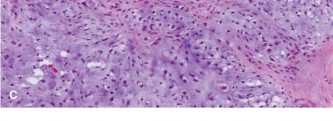
Figure 6: Intraoperative photograph showing the wide en bloc resection of the distal femur containing the osteosarcoma. Note the clear margins of surrounding healthy tissue.
Following tumor resection, attention turned to reconstruction. The femoral canal was prepared for the endoprosthetic stem. The modular distal femoral endoprosthesis components were assembled and trialed to ensure appropriate limb length and soft tissue tension. The proximal femoral stem was cemented into place using standard techniques. The prosthetic knee joint was then articulated, and the tibial component was cemented after preparing the tibial plateau. Care was taken to ensure correct rotational alignment and patellar tracking. The collateral ligaments, hamstring tendons, and quadriceps mechanism were meticulously reattached to the dedicated attachment sites on the prosthesis, optimizing knee stability and function. Soft tissue coverage of the prosthesis was paramount to minimize infection risk.
The wound was irrigated thoroughly, and two suction drains were placed. The incision was closed in layers, paying careful attention to restoring fascial integrity and achieving tension-free skin closure.
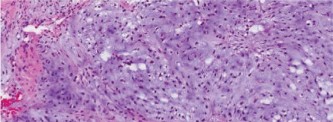
Figure 7: Post-operative radiograph confirming satisfactory placement of the modular distal femoral endoprosthesis, with excellent alignment and limb length restoration.
The resected specimen was sent for detailed histopathological analysis to assess tumor necrosis following neoadjuvant chemotherapy and confirm surgical margins. Post-operative pathology confirmed high-grade osteosarcoma with good tumor response (estimated 95% tumor necrosis) to chemotherapy, and wide, tumor-free surgical margins.
Adjuvant Chemotherapy: Following surgical recovery, the patient continued with adjuvant chemotherapy for several additional cycles, as per the established oncology protocol, to further eradicate any remaining microscopic disease.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period:
*
Pain Management:
Aggressive multimodal analgesia (IV PCA, regional nerve blocks, oral opioids, NSAIDs/acetaminophen) was initiated.
*
DVT Prophylaxis:
Low molecular weight heparin (LMWH) was administered, along with pneumatic compression devices.
*
Wound Care:
Daily wound checks and drain management. Drains were typically removed when output was less than 30 mL over 24 hours.
*
Early Mobilization:
The patient was encouraged to start gentle ankle pump exercises immediately. Out-of-bed to a chair was initiated on post-operative day 1, with assistance.
Rehabilitation Protocol:
*
Weight-Bearing:
Touch-down weight-bearing (TDWB) with crutches was initiated on post-operative day 2-3, gradually progressing to partial weight-bearing (PWB) over 4-6 weeks, and then full weight-bearing (FWB) as tolerated, guided by pain and prosthetic stability. The initial protected weight-bearing allows for soft tissue healing and integration around the prosthesis.
*
Range of Motion (ROM):
Continuous passive motion (CPM) machine was used for 4-6 hours daily, starting at 0-30 degrees and gradually increasing as tolerated to prevent arthrofibrosis. Active-assisted and active ROM exercises were initiated by physical therapy.
*
Strengthening:
Isometric quadriceps and hamstring exercises began early. Progressive resistance exercises were introduced once soft tissue healing was sufficient, typically around 6-8 weeks post-operatively. Focus was on quadriceps strengthening (to prevent extensor lag) and hip musculature.
*
Gait Training:
Intensive gait training with assistive devices was provided, progressing from crutches to a cane, and eventually independent ambulation. Balance and proprioception exercises were also incorporated.
*
Functional Training:
Specific exercises to improve activities of daily living (ADLs) and return to school/modified recreational activities were implemented.
Long-Term Follow-up and Surveillance:
*
Oncological Surveillance:
Regular follow-up with both orthopedic oncology and medical oncology teams.
* Chest CT scans: Typically every 3 months for the first 2 years, then every 6 months for the next 3 years, then annually, to detect pulmonary metastases.
* Plain radiographs of the reconstructed limb: Annually to monitor for prosthetic loosening, fracture, or other complications.
* Bone scan: Annually for 5 years to detect other bony metastases.
* Clinical examination: Regular assessment for local recurrence, pain, and function.
*
Prosthetic Surveillance:
Lifelong monitoring for aseptic loosening, infection, component failure, and polyethylene wear. Revision surgery may be required in the long term.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
*
Index of Suspicion:
Maintain a high index of suspicion for primary bone tumors in adolescents presenting with persistent, insidious, night pain, especially when unresponsive to conservative measures.
*
Biopsy is Key:
Never operate on a suspected bone sarcoma without a definitive pathological diagnosis.
*
Biopsy Planning:
The biopsy incision
must
be longitudinal and placed in line with the planned definitive surgical approach. An ill-conceived biopsy can compromise limb salvage or contaminate uninvolved compartments.
*
Multidisciplinary Approach:
Management of osteosarcoma requires a collaborative effort involving orthopedic oncologists, medical oncologists, radiation oncologists, musculoskeletal radiologists, and pathologists.
*
Neoadjuvant Chemotherapy:
Standard of care for high-grade osteosarcomas; it reduces tumor burden, treats micrometastases, and assesses tumor chemosensitivity (prognostic indicator).
*
Imaging for Staging:
MRI is indispensable for local staging (intramedullary extent, soft tissue involvement, neurovascular relationship) and surgical planning. CT chest and bone scan are crucial for systemic staging.
*
Wide Oncological Margins:
The primary goal of surgery for high-grade sarcomas is wide en bloc resection with clear margins to minimize local recurrence risk. This often necessitates sacrificing expendable structures.
*
Soft Tissue Reattachment:
Meticulous soft tissue reattachment during reconstruction is critical for joint stability, functional outcome, and preventing extensor lag in knee endoprostheses.
*
Prognostic Factors:
Tumor response to neoadjuvant chemotherapy (percentage of tumor necrosis) and presence of metastases are the most important prognostic factors.
Pitfalls:
*
Misdiagnosis/Delay in Diagnosis:
Attributing symptoms to "growing pains," sports injuries, or benign conditions, leading to delayed diagnosis and potentially advanced disease.
*
Inadequate Biopsy:
*
Transverse Incision:
A transverse biopsy incision can contaminate multiple compartments, making limb salvage challenging or impossible.
*
Poor Sampling:
Insufficient or non-representative tissue can lead to a false negative or incorrect diagnosis.
*
Contamination:
Spillage of tumor cells or biopsy through critical structures can compromise subsequent resection margins.
*
Operating Without Staging:
Performing definitive surgery before full local (MRI) and systemic (CT chest, bone scan) staging, which can lead to inadequate resection or missed metastases.
*
Inadequate Surgical Margins:
Attempting a marginal or intralesional resection for a high-grade sarcoma, which is associated with a high rate of local recurrence and poorer survival.
*
Neglecting Chemotherapy:
Failing to administer neoadjuvant or adjuvant chemotherapy, which is vital for systemic disease control and improving overall survival.
*
Pathologic Fracture:
A pathologic fracture significantly complicates management, often increasing the risk of local recurrence and systemic metastasis due to tumor spillage. It may necessitate more aggressive resection or even amputation.
*
Infection:
Endoprosthetic reconstruction carries a lifelong risk of periprosthetic joint infection, which can be devastating. Careful surgical technique, meticulous hemostasis, and antibiotic prophylaxis are crucial.
*
Neurovascular Injury:
Aggressive dissection in close proximity to the neurovascular bundle without adequate protection can lead to limb-threatening complications.
*
Ignoring Multidisciplinary Input:
Failure to engage the full oncology team can lead to suboptimal treatment plans and outcomes.
Clinical & Radiographic Imaging
You Might Also Like