Orthopedic With Answer Hip Review | Dr Hutaif Hip & Kne -...
14 Apr 2026
175 min read
88 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer Hip Review | Dr Hutaif...
00:00
Start Quiz
Question 1High Yield
Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when**
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided.
REFERENCES: Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146.
Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Bailes JE, Hadley MN, Quigley MR, Sonntag VK, Cerullo LJ: Management of athletic injuries of the cervical spine and spinal cord. Neurosurgery 1991;29:491-497.
REFERENCES: Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146.
Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Bailes JE, Hadley MN, Quigley MR, Sonntag VK, Cerullo LJ: Management of athletic injuries of the cervical spine and spinal cord. Neurosurgery 1991;29:491-497.
Question 2High Yield
A 50-year-old woman reports a burning sensation on the plantar aspect of her left forefoot, distal to the metatarsal heads between her third and fourth digits. Palpation of the third web space recreates her symptoms. Which of the following will most accurately aid in confirming a diagnosis?
Explanation
The diagnosis of an interdigital neuroma is best made by a thorough history and careful physical examination. Radiographs are helpful in excluding other pathologic processes such as a metatarsal stress fracture. MRI and ultrasound have both been reported to aid in the diagnosis of an interdigital neuroma.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 145-151.
TJ, Jacobson JA, Craig JG, et al: Sonography of Morton’s neuromas. Am J Roentgenol 2000;174:1723-1728.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 145-151.
TJ, Jacobson JA, Craig JG, et al: Sonography of Morton’s neuromas. Am J Roentgenol 2000;174:1723-1728.
Question 3High Yield
The patient in Figure 96 has medial pain at the first metatarsophalangeal (MTP) joint and no other pain.

Explanation
- Distal metatarsal osteotomy with a modified McBride procedure_
Question 4High Yield
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
Nonsurgical management of OCD of the talus in skeletally immature individuals frequently results in a fairly rapid decrease in symptoms, but radiographic abnormalities can frequently be found even 6 months after treatment. Spontaneous resolution of this condition is rare. Hyperbaric oxygen treatment has not been shown to be beneficial for this condition. Progression of the condition to the point of requiring ankle fusion is rare.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 5High Yield
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries.
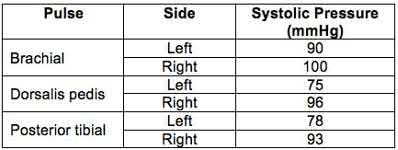
Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Explanation
The ankle-brachial index (ABI) of left and right limbs are 0.78 and 0.96 respectively. CT angiography (or conventional angiography) of the left lower extremity is indicated because of abnormal ABI <0.9. It is sufficient to observe the right lower extremity (ABI >0.9).
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI <0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Answer 1: If vascular exam is normal and ABI >0.9, neurovascular checks every 2-4 hours for 48 hours is appropriate. As ABI is abnormal on the left, CT angiogram is necessary.
Answer 2: Anticoagulation has not been shown to stop thrombus formation for non-flow limiting intimal flap tears.
Answer 3: CT angiography is indicated if ABI is abnormal post reduction. CT angiography for the right lower extremity is unnecessary as ABI >0.9.
Answer 5: Surgery is indicated if CT angiography (or conventional angiography) demonstrates intimal flap tears that are flow limiting (but not if the intimal flap is NOT flow limiting), if distal pulses are absent, or if distal ischemia, active hemorrhage, or expanding pulsatile hematoma are present.
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI <0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Answer 1: If vascular exam is normal and ABI >0.9, neurovascular checks every 2-4 hours for 48 hours is appropriate. As ABI is abnormal on the left, CT angiogram is necessary.
Answer 2: Anticoagulation has not been shown to stop thrombus formation for non-flow limiting intimal flap tears.
Answer 3: CT angiography is indicated if ABI is abnormal post reduction. CT angiography for the right lower extremity is unnecessary as ABI >0.9.
Answer 5: Surgery is indicated if CT angiography (or conventional angiography) demonstrates intimal flap tears that are flow limiting (but not if the intimal flap is NOT flow limiting), if distal pulses are absent, or if distal ischemia, active hemorrhage, or expanding pulsatile hematoma are present.
Question 6High Yield
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of**
Explanation
The PA view of the wrist shows a pisiform fracture. Pisiform fractures constitute 1% to 3% of all carpal bone fractures. This fracture can be further evaluated with a carpal tunnel view or a supination oblique view of the wrist. Initial management should consist of immobilization with a short arm cast. If nonsurgical measures fail, bony excision is warranted.
REFERENCES: Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
REFERENCES: Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
Question 7High Yield
What is the most common complication after distal biceps tendon repair at the elbow?
Explanation
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
incarceration with endobutton repair.
Question 8High Yield
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
Question 9High Yield
Glucose control assessment is best achieved by ordering which blood test?
Explanation
- Hemoglobin A1C
Question 10High Yield
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to**
Explanation
Studies examining the impact of graded water debt have clearly shown that the magnitude of core temperature and heart rate increase accompanying work are proportional to the magnitude of water debt at the onset of exercise. Though added thermal burden from hot climates is a factor, it appears to be less significant.
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
Question 11High Yield
A 19-year-old collegiate lacrosse player stumbles to the sideline after a collision with an opposing player during the first quarter of a game. She complains of dizziness and is disoriented to place and time. She initially shows disturbances in balance. The player is diagnosed as having sustained a concussion and is removed from the rest of the game. What should the coaching staff be advised of regarding the player’s return to activity?
Explanation
Concussions can be defined as a traumatically induced transient disturbance of brain function. There is currently no consensus regarding the definition of a concussion, nor is a there a defined biomechanical threshold of a concussion. Concussions occur when either linear and/or rotational forces are transmitted to the brain. A complex disturbance in neurometabolic activity follows. Until normal metabolic activity is restored, a second injury can result in worsening metabolic changes and significant cognitive defects. Given this reasoning, under no circumstances should an athlete be allowed same-day return to physical activity. In terms of return to play, studies have shown that strict rest may actually delay recovery and prolong symptoms. Most studies recommend a 24 to 48 hour period of symptom limited cognitive and physical rest, followed by sub-symptom threshold light aerobic activity.
20
20
Question 12High Yield
When reconstructing the anterior cruciate ligament (ACL) with autograft, what is the most common
source of surgical failure?
source of surgical failure?
Explanation
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause for technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. Although graft choice is an important factor when planning an ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position.
Question 13High Yield
A 55-year-old woman with degenerative joint disease underwent total shoulder arthroplasty (TSA). She was doing well without complications at her 2-week visit (Figures 1 and 2). She returned at 6 weeks with increased pain, shoulder clicking, and difficulty with forward elevation and internal rotation. She recalls slipping, and to prevent a fall, moved her arm suddenly to grab a rail. New radiographs are shown in Figures 3 and
Explanation
the radiographs at her 6-week appointment show anterior subluxation of the glenohumeral joint indicative of subscapularis insufficiency. Subscapularis repair is the next best step in management, especially in this age group, with well-fixed and well-aligned components.
3
3
Question 14High Yield
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed?
Explanation
DISCUSSION: Herpes simplex virus (HSV) can cause serious outbreaks on athletic teams, especially wrestling. HSV is highly contagious; it is secreted from active blisters, saliva, and mucous membranes. For wrestlers, the NCAA states that the athlete must be free from systemic symptoms and any new blisters for 72
hours before being allowed to participate. Also, all lesions must be dry and crusted and at least 120 hours of antiviral therapy should have been instituted.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 301-309.
Johnson R: Herpes Gladiatorium and other skin diseases. Clin Sports Med 2004;23:473-484.
DISCUSSION: Herpes simplex virus (HSV) can cause serious outbreaks on athletic teams, especially wrestling. HSV is highly contagious; it is secreted from active blisters, saliva, and mucous membranes. For wrestlers, the NCAA states that the athlete must be free from systemic symptoms and any new blisters for 72
hours before being allowed to participate. Also, all lesions must be dry and crusted and at least 120 hours of antiviral therapy should have been instituted.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 301-309.
Johnson R: Herpes Gladiatorium and other skin diseases. Clin Sports Med 2004;23:473-484.
Question 15High Yield
What finding would most likely be present on an AP radiograph of a nondislocated elbow with an anteromedial coronoid fracture?
Explanation
No detailed explanation provided for this question.
Question 16High Yield
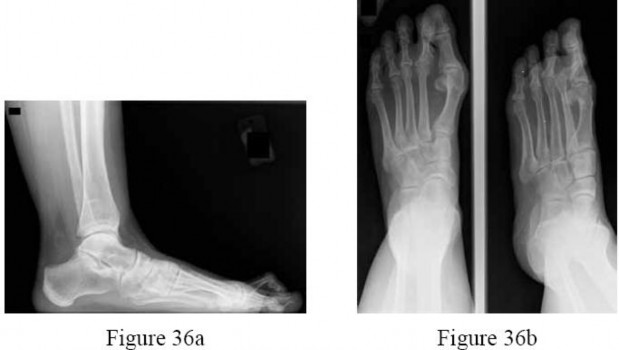
Figures 36a and 36b are the AP and lateral radiographs of a 65-year-old woman who has a dislocated second toe and a prominent bunion. Besides repairing the bunion, what procedures are recommended to address the fixed second hammertoe and the resulting metatarsalgia?
---
---
Explanation
The patient has a subluxated second metatarsophalangeal (MTP) joint, but no evidence of second metatarsal head destruction. The patient also has a fixed claw toe. The claw toe is repaired with a PIP resection arthroplasty or a PIP fusion. The likelihood of
completely correcting the MTP joint dislocation with just these two procedures, however, is small and the addition of the Weil osteotomy is more likely to allow decompression of the joint and complete relocation of the MTP joint. The flexor to extensor transfer is indicated for a flexible hammertoe. A metatarsal head excision is a salvage option of the toe that still cannot be reduced after the Weil osteotomy, but this may lead to transfer lesions.The DuVries arthroplasty will not help reduce the MTP joint. Combined metatarsal head excision and proximal phalanx resection would be extreme and is not recommended.
completely correcting the MTP joint dislocation with just these two procedures, however, is small and the addition of the Weil osteotomy is more likely to allow decompression of the joint and complete relocation of the MTP joint. The flexor to extensor transfer is indicated for a flexible hammertoe. A metatarsal head excision is a salvage option of the toe that still cannot be reduced after the Weil osteotomy, but this may lead to transfer lesions.The DuVries arthroplasty will not help reduce the MTP joint. Combined metatarsal head excision and proximal phalanx resection would be extreme and is not recommended.
Question 17High Yield
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
Explanation
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
Question 18High Yield
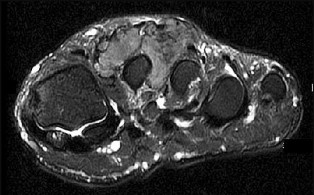
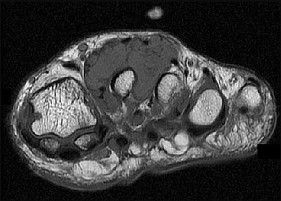
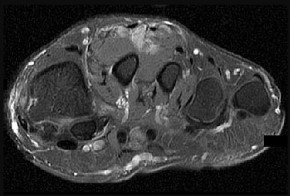
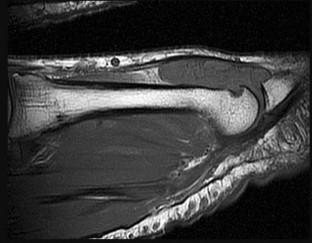
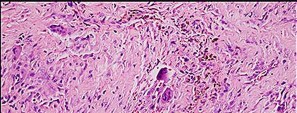
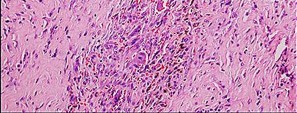
Figure 46a is the lateral radiograph of a 54-year-old man who has had a painless soft-tissue mass on his right foot that has been growing slowly for about 1 year. MR sequences are shown in Figures 46b through 46e. A biopsy is performed, and a low-power hematoxylin and eosin photomicrograph is seen in Figure 46f. The most appropriate treatment for this lesion is

Explanation
This is a giant-cell tumor of the tendon sheath. A solid lesion larger than 1.5 cm in the hand or foot warrants biopsy to rule out malignancy. The 3 most common benign tumors of the foot are ganglion cysts, giant-cell tumors of tendon sheath, and hemangiomas. Radiographs are nonspecific but may reveal extrinsic erosions of bone by a giant-cell tumor of the tendon sheath. MR findings of prominent low-signal intensity (seen with T2 weighting) and “blooming” artifact from the hemosiderin (seen with gradient-echo sequences) are nearly pathognomonic of this diagnosis, as
seen here. Pathology shows hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
29. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1493-
[518/. doi: 10.1148/rg.285085134. PubMed PMID: 18794322. ](http://www.ncbi.nlm.nih.gov/pubmed/18794322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18794322)
30. [Ruggieri P, Angelini A, Jorge FD, Maraldi M, Giannini S. Review of foot tumors seen in a university tumor institute. J Foot Ankle Surg. 2014 May-Jun;53(3):282-5. doi: 10.1053/j.jfas.2014.01.015. Review. PubMed PMID: 24751209. ](http://www.ncbi.nlm.nih.gov/pubmed/24751209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24751209)
seen here. Pathology shows hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
29. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008 Sep-Oct;28(5):1493-
[518/. doi: 10.1148/rg.285085134. PubMed PMID: 18794322. ](http://www.ncbi.nlm.nih.gov/pubmed/18794322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18794322)
30. [Ruggieri P, Angelini A, Jorge FD, Maraldi M, Giannini S. Review of foot tumors seen in a university tumor institute. J Foot Ankle Surg. 2014 May-Jun;53(3):282-5. doi: 10.1053/j.jfas.2014.01.015. Review. PubMed PMID: 24751209. ](http://www.ncbi.nlm.nih.gov/pubmed/24751209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24751209)
Question 19High Yield
Macrodactyly affects:
Explanation
Although this is controversial, the majority of surgeons believe that macrodactyly affects bones, fat, and nerves.
Question 20High Yield
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 21High Yield
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?
Explanation
Functional improvement after revision rotator cuff surgery is most likely to occur in patients with an intact deltoid, good-quality rotator cuff tissue, preoperative active elevation alone to 90 degrees, and only one prior rotator cuff repair. In this patient, the compromised deltoid origin might make functional improvement less likely.
REFERENCES: Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855.
Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases.
J Shoulder Elbow Surg 1992;1:283-286.
REFERENCES: Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855.
Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases.
J Shoulder Elbow Surg 1992;1:283-286.
Question 22High Yield
The infant underwent Ponseti casting for 5 weeks. Afterward, a heel cord release was done 1 cm proximal to the insertion site of the Achilles tendon and was casted in long-leg casts with the knee flexed and an external rotation mold on the leg for 3 weeks. Straight-last shoes with an abduction bar set at 70 degrees of external rotation were fitted. The infant’s feet remained in the corrected position at a 1-month check, but, at a 3-month check, ankle equinus and forefoot varus were present. Recurrence of the deformity is most likely attributable to
Explanation
- noncompliance with postsurgical bracing.
Question 23High Yield
A 12-year-old boy at 5’5”, 180 pounds comes to the outpatient clinic with 2 months of left anterior knee pain without discrete injury. He has a slight antalgic gait on the left, has full knee range of motion, stable ligaments, and mild tenderness at his tibial tubercle. He has restricted hip internal rotation and worsening knee pain with hip motion. Knee radiographs are negative. What is the best next step in treatment?
Explanation
■
Knee pain in an overweight adolescent patient is a classic presentation for stable slipped capital femoral epiphysis (SCFE). Recognizing the exacerbation of knee pain with hip motion makes radiographic evaluation of the hip the appropriate next step in evaluation. Delaying the diagnosis with treatment focused on the knee such as the other answer options suggest, risks progression of the SCFE and potential long-term consequences.
Knee pain in an overweight adolescent patient is a classic presentation for stable slipped capital femoral epiphysis (SCFE). Recognizing the exacerbation of knee pain with hip motion makes radiographic evaluation of the hip the appropriate next step in evaluation. Delaying the diagnosis with treatment focused on the knee such as the other answer options suggest, risks progression of the SCFE and potential long-term consequences.
Question 24High Yield
A 20-year-old man presents with erythema, swelling, and pain at the left sternoclavicular joint shown in Figure A. His temperature is
38.9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?
38.9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?


Explanation
This patient has sternoclavicular joint septic arthritis with gram positive organisms. Although there is an increased incidence of Pseudomonas aeruginosa infection in IV drug users, S. aureus is still the most common organism.
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
Question 25High Yield
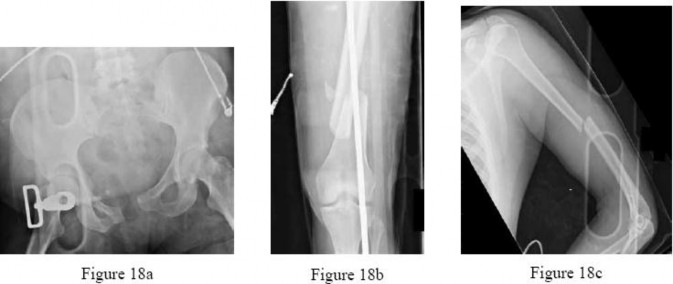
Figures 18a through 18c show injuries sustained by a 22-year-old woman after falling 45 feet while mountain climbing. After being airlifted to the nearest trauma center, her arterial blood gas was 7.21, pO2 84, pCO2 48, and base arterial blood gas was 7.21, pO2 84, pCO2 48, and delta base -11 mmol/L. Her Hg is
8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?
8.7 and her resuscitation is ongoing. Based on this data, what would be the best management of her orthopaedic injuries?
Explanation
No detailed explanation provided for this question.
Question 26High Yield
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
[Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. ](http://www.ncbi.nlm.nih.gov/pubmed/17548882)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548882)
[Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. ](http://www.ncbi.nlm.nih.gov/pubmed/10797219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10797219)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
RECOMMENDED READINGS
[Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. ](http://www.ncbi.nlm.nih.gov/pubmed/17548882)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548882)
[Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. ](http://www.ncbi.nlm.nih.gov/pubmed/10797219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10797219)
[Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. ](http://www.ncbi.nlm.nih.gov/pubmed/2613128)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2613128)
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 27High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
In this patient, what other potential injury can be associated with this fracture pattern and is commonly overlooked?
---
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
In this patient, what other potential injury can be associated with this fracture pattern and is commonly overlooked?
---

Explanation
The patient sustained a posterior wall fracture dislocation. For acetabular fractures, the position of the limb in space at the time of impact (in terms of the amount of flexion/extension, internal/external rotation, and adduction/abduction) will dictate the fracture pattern. For posterior wall fracture patterns, the limb is in some degree of flexion, adduction, and internal rotation. Other combinations are possible to contribute to an acetabular fracture but not likely to contribute to a posterior wall pattern.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage,
there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage,
there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
Question 28High Yield
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Explanation
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
[Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. ](http://www.ncbi.nlm.nih.gov/pubmed/23116090)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116090) [Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[View ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20858377)
[Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[View](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24688334)
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
[Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. ](http://www.ncbi.nlm.nih.gov/pubmed/23116090)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116090) [Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[View ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20858377)
[Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[View](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24688334)
Question 29High Yield
**ONLINE ORTHOPEDIC MCQS UPPER LIMB08**
**1**. A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results?
**1**. A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results?
Explanation
The radiographs and CT scan reveal osteoarthritis with posterior subluxation and posterior bone loss. Total shoulder arthroplasty with reaming of the high side to neutralize the glenoid surface has been shown to yield better results than hemiarthroplasty. The amount of bone loss in this patient does not require posterior glenoid augmentation. Reverse total shoulder arthroplasty is indicated for rotator cuff tear arthropathy; therefore, it is not applicable. Arthroscopic debridement has yielded poor results with advanced osteoarthritis and posterior subluxation. Results from glenoid osteotomy have been variable and glenoid osteotomy is not indicated with associated osteoarthritis.**
**
**
Scientific References
- : Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.**
**Rodosky MW, Bigliani LU: Indications for glenoid resurfacing in shoulder arthroplasty.
J Shoulder Elbow Surg 1996;5:231-248.**
**2****. A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
1- She was noncompliant in physical therapy.
2- The original surgery should have included resurfacing the glenoid.
3- The humeral head was too large.
4- The humeral component was placed too proud.
5- The tuberosities are malpositioned.
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement.**
**REFERENCES: Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748.**
**Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.**
**Tanner MW, Cofield RH: Prosthetic arthroplasty for fractures and fracture-dislocations of the proximal humerus. Clin Orthop Relat Res 1983;179:116-128.**
**3****. Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?
1- Increase in internal rotation, decrease in external rotation
2- Increase in internal rotation, increase in external rotation
3- Decrease in internal rotation, decrease in external rotation
4- Decrease in internal rotation, increase in external rotation
5- Decrease in forward flexion, increase in external rotation
PREFERRED RESPONSE: 4**
**DISCUSSION: Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture.**
**REFERENCES: Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.**
**Crockett HC, Gross LB, Wilk KE, et al: Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med 2002;30:20-26.**
**4****. A 40-year-old woman underwent an arthroscopic acromioplasty and mini-open rotator cuff repair 4 weeks ago. At follow-up examination, the incision is painful, erythematous, and draining fluid. The patient is febrile and has an elevated WBC count. What infectious organism should be under high suspicion of causing this outcome?
1- Escherichia coli
2- Streptococcus viridans
3- Oxalophagus oxalicus
4- Proprionobacter acnes
5- Enterococcus faecalis
PREFERRED RESPONSE: 4**
**DISCUSSION: Proprionobacter acnes has been a leading cause of indolent shoulder infections. During shoulder arthroscopy, the arthroscopic fluid may actually dilute the shoulder preparation and lead to a higher rate of infection during subsequent mini-open rotator cuff repair surgery. The remaining bacteria listed are rarely associated with shoulder infections after arthroscopy.**
**REFERENCES: Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.**
**Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 551-557.**
**5****. What ligament is the primary stabilizer of the wrist following a proximal row carpectomy?
1- Dorsal radiocarpal
2- Dorsal intercarpal
3- Radioscaphocapitate
4- Ulnocapitate
5- Ulnotriquetral
PREFERRED RESPONSE: 3**
**DISCUSSION: The radioscaphocapitate ligament is the prime stabilizer between the radius and capitate, preventing ulnar translocation of the carpus. Its oblique orientation prevents the carpus from drifting ulnarly. This stout ligament must be protected when excising the scaphoid.**
**REFERENCES: Stern PJ, Agabegi SS, Kiefhaber TR, et al: Proximal row carpectomy. J Bone Joint Surg Am 2005;87:166-174.**
**Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of wrist arthritis. J Am Acad Orthop Surg 2003;11:227-281.**
**6****. A 30-year-old right hand-dominant woman is seen in the trauma unit after a high-speed motor vehicle accident. She sustained a right shoulder anterior dislocation that is gently reduced under sedation. A CT scan is shown in Figure 3. If left untreated, the patient is at greatest risk for
1- axillary neuropathy.
2- recurrent instability.
3- shoulder girdle weakness.
4- luxatio erecta.
5- biceps tendinitis.
PREFERRED RESPONSE: 2**
**DISCUSSION: Large, displaced anterior inferior glenoid rim fractures predispose patients to recurrent anterior instability due to loss of the normal concavity compression effect of the glenoid. These defects require open reduction and internal fixation to reestablish shoulder stability. Although intra-articular fractures may lead to arthrosis, recurrent instability is
more common. **
**REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.**
**Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med 1998;26:41-45.**
**7****. Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of
1- humeral head arthroplasty.
2- observation.
3- arthroscopic capsular release.
4- grafting of the humeral head defect.
5- electrical stimulation.
PREFERRED RESPONSE: 2**
**DISCUSSION: This rare complication occurs after fracture-dislocation and has been seen after surgical stabilization in the adolescent. In most reported cases, prolonged observation has been shown to result in revascularization.**
**REFERENCES: Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.**
**Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.**
**8****. A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
1- repair of the superior labrum.
2- isolated supraspinatus repair.
3- biceps recentering.
4- subscapularis repair and biceps tenodesis.
5- subscapularis repair and recentering of the biceps tendon.
PREFERRED RESPONSE: 4**
**DISCUSSION: The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure.**
**REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.**
**Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.**
**Walch G, Nove-Josserand L, Boileau P, et al: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.**
**9****. A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?
1- Total elbow arthroplasty
2- Open reduction and internal fixation
3- Radial head arthroplasty
4- Sling and swathe
5- Bone stimulator
PREFERRED RESPONSE: 1**
**DISCUSSION: Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening.**
**REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.**
**Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than age 65. J Orthop Trauma 2003;17:473-480.**
**10****. An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
1- Rupture of the medial collateral ligament
2- Rupture of the lateral collateral ligament
3- Intra-articular loose body
4- Flexor-pronator injury
5- Extensor origin avulsion
PREFERRED RESPONSE: 1**
**DISCUSSION: MRI arthrography is the imaging study of choice for evaluation of medial collateral ligament injuries.**
**REFERENCES: Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.**
**Munshi M, Pretterklieber ML, Chung CB, et al: Anterior bundle of ulnar collateral ligament: Evaluation of anatomic relationships by using MR imaging, MR arthrography, and gross anatomic and histologic analysis. Radiology 2004;231:797-803.**
**11****. A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?
1- Cervical C6-7 radiculopathy
2- Impingement
3- Rotator cuff tear
4- Brachial neuritis
5- Adhesive capsulitis
PREFERRED RESPONSE: 4**
**DISCUSSION: The definition of brachial neuritis or Parsonage-Turner syndrome is a rare disorder of unknown etiology that causes pain or weakness of the shoulder and upper extremity. The loss of active motion excludes cervical C6-7 radiculopathy and impingement. A normal MRI scan and full passive motion exclude a rotator cuff tear and adhesive capsulitis, respectively.**
**REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.**
**McCarty EC, Tsairis P, Warren RF: Brachial neuritis. Clin Orthop Relat Res 1999;368:37-43.**
**12****. A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?
1- Adhesive capsulitis
2- Sling immobilization
3- Thermal chondrolysis
4- Subacromial impingement
5- Axillary nerve injury
PREFERRED RESPONSE: 5**
**DISCUSSION: Treatment of shoulder instability with thermal devices has lead to numerous complications including recurrent instability, chondrolysis, stiffness, and capsular necrosis. This patient’s findings are consistent with a heat-induced axillary nerve injury. Normal radiographs exclude extensive chondrolysis.**
**REFERENCES: Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.**
**McCarty EC, Warren RF, Deng XH, et al: Temperature along the axillary nerve during radiofrequency-induced thermal shrinkage. Am J Sports Med 2004;32:909-914.
13. Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow?
1- Infraspinatus
2- Teres minor
3- Subscapularis
4- Long head of triceps
5- Latissimus dorsi
PREFERRED RESPONSE: 2
DISCUSSION: The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor.
REFERENCES: Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears.
J Shoulder Elbow Surg 2003;12:550-554.**
**Agur AM (ed): Grant’s Atlas of Anatomy, ed 9. Baltimore, MD, Lippincott Williams & Wilkins, 1991, p 394.**
**14****. A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation
4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?
1- Anterior shoulder dislocation
2- Humeral component loosening
3- Glenoid component loosening
4- Glenoid component catastrophic fracture
5- Rotator cuff tear
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis.**
**REFERENCES: Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.**
**Sperling JW, Potter HG, Craig EV, et al: Magnetic resonance imaging of painful shoulder arthroplasty. J Shoulder Elbow Surg 2002;11:315-321.**
**15****. A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
1- Arthroscopic debridement alone of the partial rotator cuff tear
2- Repair of the partial rotator cuff tear and subacromial decompression
3- Arthroscopic debridement combined with subacromial decompression
4- Arthroscopic subacromial decompression
5- Biceps tenotomy
PREFERRED RESPONSE: 2**
**DISCUSSION: Although arthroscopic debridement with or without subacromial decompression is a reasonable response, the patient has positive impingement signs. Several recent studies regarding the surgical treatment of partial rotator cuff tears have demonstrated good to excellent results after repair of tears involving more than 50% of the tendon thickness. This was shown specifically for bursal-sided tears and joint-side tears. Biceps tenotomy is not indicated in a young patient.**
**REFERENCES: Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears.
Am J Sports Med 2005;33:1405-1417.**
**Fukuda H: The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br 2003;85:3-11.**
**16****. The condition shown in Figures 9a and 9b is most likely the result of
1- infection.
2- uric acid deposition.
3- trauma.
4- a virus.
5- severe cold exposure.
PREFERRED RESPONSE: 2**
**DISCUSSION: The clinical photograph and radiograph show gout, which is the result of urate deposition in the joint and soft tissues. Radiographs frequently reveal periarticular erosions. The crystals are intracellular and negatively birefringent under the polarized microscope. Treatment for acute flares include colchicines, indomethacin, and corticosteroids (including injections). Medications such as allopurinol help prevent recurrent flares. Tophi such as that seen in this patient are often confused with and associated with infection.**
**REFERENCES: Wortmann RL, Kelley WM: Crystal-induced inflammation: Gout and hyperuricemia, in Harris ED, Budd RC, Firestein GS, et al (eds): Kelley’s Textbook of Rheumatology, ed 7. New York, NY, Elsevier Science, 2005, pp 1402-1429.**
**Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.**
**Louis DS, Jebson PJ: Mimickers of hand infections. Hand Clin 1998;14:519-529.**
**17****. A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
1- Complex regional pain syndrome
2- Wartenberg’s syndrome
3- Carpal tunnel syndrome
4- Palmar cutaneous nerve injury
5- C7 radiculopathy
PREFERRED RESPONSE: 4**
**DISCUSSION: The palmar cutaneous branch of the median nerve separates from the median nerve approximately 4 to 6 cm proximal to the wrist crease and travels between the median nerve and the flexor carpi radialis tendon. It supplies the skin of the thenar region. This nerve is at risk for injury with retraction of the digital flexor tendons in plating the distal radius. Wartenberg’s syndrome is compression of the superficial radial nerve which innervates the dorsum of the thumb and the first dorsal web space. Carpal tunnel syndrome causes dysesthesias of the thumb, index, and/or middle fingers. C7 radiculopathy affects the index and middle fingers.**
**REFERENCES: Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.**
**Hoppenfield S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 156-176.**
**18****. Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?
1- Arthroscopic debridement
2- Arthrodesis
3- Resection arthroplasty
4- Hemiarthroplasty
5- Cortisone injection
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown.**
**REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.**
**Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.**
**Loebenberg MI, Plate AM, Zuckerman JD: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.**
**19****. Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?
1- Percutaneous pins
2- Cannulated screws
3- Cerclage wire
4- Balser plate
5- AO locking plate
PREFERRED RESPONSE: 1**
**DISCUSSION: Numerous reports have documented serious complications including death from migration of intact or broken Kirschner wires or Steinmann pins into hilar structures such as the heart, pulmonary artery, and the aorta.**
**REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.**
**Lyons FA, Rockwood CA Jr: Migration of pins used in operations of the shoulder. J Bone Joint Surg Am 1990;72:1262-1267.**
**20****. Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a “lump” at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?
1- Unreduced posterior sternoclavicular dislocation
2- Congenital hypoplasia of the medial clavicle
3- Postmenopausal arthritis of the sternoclavicular joint
4- Sternoclavicular hyperostosis
5- Spontaneous subluxation of the right sternoclavicular joint
PREFERRED RESPONSE: 5**
**DISCUSSION: Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management.**
**REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 1078-1079.**
**Rockwood CA, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.**
**21****. Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
1- Direct nerve repair
2- Sural nerve graft
3- Pectoralis major transfer
4- Levator scapula and rhomboid transfer
5- Scapulothoracic fusion
PREFERRED RESPONSE: 4**
**DISCUSSION: Injury to the spinal accessory nerve can occur after penetrating trauma to the shoulder. Blunt trauma may also cause loss of trapezius function. Most commonly, surgical dissection in the posterior triangle of the neck, such as lymph node biopsy, may expose the nerve to possible damage. Surgical repair of the nerve may be considered up to 1 year after injury; after this time muscle transfer is usually associated with a better functional outcome.**
**REFERENCES: Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.**
**Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop Relat Res 1999;368:5-16.**
**22****. What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?
1- Loosening of the humeral component
2- Loosening of the glenoid component
3- Infection
4- Brachial plexus injury
5- Rotator cuff tear
PREFERRED RESPONSE: 5**
**DISCUSSION: In an article in the Journal of Shoulder and Elbow, 431 total shoulder arthroplasties were performed with a cemented all-polyethylene glenoid component between 1990 and 2000. Follow-up averaged 4.2 years. In total, 53 surgical complications occurred in 53 patients (12%). Of these, 32 were major complications (7.4%), with 17 of these requiring reoperation. Index complications in order of frequency included rotator cuff tearing, postoperative glenohumeral instability, and periprosthetic humeral fracture. Notably, glenoid and humeral component loosening requiring reoperation occurred in only one shoulder. Data from the contemporary patient group suggest that there are fewer complications of shoulder arthroplasty and less need for reoperation. Especially striking is the near absence of component revision because of loosening or other mechanical factors. Complications involving the brachial plexus have been reported following total shoulder arthroplasty but are not as common of a cause for failure.**
**REFERENCES: Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.**
**Hasan SS, Leith JM, Campbell B, et al: Characteristics of unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg 2002;11:431-441.**
**23****. A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in
Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?
1- Hip radiograph
2- Knee radiograph
3- MRI of both shoulders
4- Cervical spine radiographs, including flexion and extension views
5- Arthrography of both shoulders
PREFERRED RESPONSE: 4**
**DISCUSSION: Rheumatoid arthritis is sometimes associated with radiographic evidence of instability of the cervical spine. In a study by Grauer and associates, radiographs of the cervical spine of patients with rheumatoid arthritis who had undergone total joint arthroplasty over a
5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority.**
**REFERENCES: Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.**
**Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.**
**24****. A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear
3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of
1- continued physical therapy that focuses on stretching and advances to strengthening in 4 weeks.
2- a cortisone injection into the subacromial space.
3- revision rotator cuff repair.
4- a sling with an abduction pillow for 2 weeks, followed by a stretching program.
5- open rotator cuff debridement without repair.
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has retorn his rotator cuff repair. This traumatic retear is different from a chronic tear and should be treated similar to an acute rotator cuff tear. Because the patient is younger than age 65 and has a small, single tendon tear, a revision rotation cuff repair is indicated with an expected tendon healing rate of greater than 95%. A physical therapy program is not indicated, and further delay in repair compromises his functional recovery. A cortisone injection is not indicated for this repairable tendon tear. Immobilization will not allow the tendon to heal once it has retorn. A debridement procedure is not indicated on this repairable tendon tear; this procedure is indicated in painful, chronic, irreparable tendon tears.**
**REFERENCES: Boileau P, Brassart N, Watkinson DJ, et al: Arthroscopic repair of full-thickness tears of the supraspinatus: Does the tendon really heal? J Bone Joint Surg Am 2005;87:1229-1240.**
**Jost B, Zumstein M, Pfirrmann CWA, et al: Long-term outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2006;88:472-479.**
**Fuchs B, Gilbart MK, Hodler J, et al: Clinical and structural results of open repair of an isolated one-tendon tear of the rotator cuff. J Bone Joint Surg Am 2006;88:309-316.**
**25****. A 49-year-old woman with serologically proven rheumatoid arthritis has Larsen grade II radiographic changes in the elbow. Examination reveals a preoperative arc of flexion of less than 90 degrees and there is no instability. Nonsurgical management has failed to provide relief. What is the best treatment option?
1- Semiconstrained total elbow arthroplasty
2- Unlinked total elbow arthroplasty
3- Fascial arthroplasty
4- Open synovectomy
5- Arthroscopic synovectomy
PREFERRED RESPONSE: 5**
**DISCUSSION: Larsen grade I and II rheumatoid arthritis is best treated with synovectomy with arthroplasty reserved for later stages, especially in younger patients. Open synovectomy with or without a radial head excision has yielded good results for pain and function, with arthroscopic synovectomies yielding similar results. Arthroscopic synovectomy has been shown to be more effective in restoring function in patients with a flexion arc of less than 90 degrees.**
**REFERENCES: Tanaka N, Sakahashi H, Hirose K, et al: Arthroscopic and open synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2006;88:521-525.**
**Horiuchi K, Momohara S, Tomatsu T, et al: Arthroscopic synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2002;84:342-347.**
**Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.**
**26****. A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management?
1- MRI
2- Electromyography
3- Open repair of the supraspinatus
4- Arthrography
5- Arthroscopic labral repair
PREFERRED RESPONSE: 1**
**DISCUSSION: In patients older than age 40 years, a high suspicion of a rotator cuff tear should be kept in those patients with weakness after shoulder dislocation. Both posterior rotator cuff and subscapularis injuries have been documented. The next most appropriate step in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.**
**REFERENCES: Stayner LR, Cumming J, Andersen J, et al: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239.**
**Neviaser RJ, Neviaser TJ, Neviaser JS: Concurrent rupture of the rotator cuff and anterior dislocation of the shoulder in the older patient. J Bone Joint Surg Am 1988;70:1308-1311.**
**27****. A 65-year-old woman fell onto her outstretched right arm and immediately had pain.
She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include
1- splint immobilization and early range-of-motion exercises.
2- radial head excision.
3- anatomic metallic radial head arthroplasty.
4- radial head open reduction and internal fixation.
5- anconeus interposition arthroplasty.
PREFERRED RESPONSE: 3**
**DISCUSSION: Comminuted, displaced radial head fractures (Hotchkiss type 3) require anatomic metallic radial head arthroplasty to regain function. Radial head excision has led to catastrophic sequelae including chronic wrist pain, elbow instability, and proximal radius migration. Immobilization, internal fixation, or anconeus arthroplasty are not recommended at this time because of the potentially poorer outcomes.**
**REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.**
**Beredjiklian PK, Nalbantoglu U, Potter HG, et al: Prosthetic radial head components and proximal radial morphology: A mismatch. J Shoulder Elbow Surg 1999;8:471-475.**
**28****. A 68-year-old woman with serologically proven rheumatoid arthritis underwent an open synovectomy and radial head resection 10 years ago. She now has severe pain that has failed to respond to nonsurgical management. Examination reveals a flexion arc of greater than 90 degrees. Radiographs are shown in Figures 15a and 15b. What is the most appropriate management?
1- Semiconstrained total elbow arthroplasty
2- Unconstrained total elbow arthroplasty
3- Fascial arthroplasty
4- Open synovectomy
5- Arthroscopic synovectomy
PREFERRED RESPONSE: 1**
**DISCUSSION: The radiographs reveal severe arthritic changes with no joint space, and the AP view shows a progressive malalignment secondary to the radial head resection. A prosthetic arthroplasty is indicated given the severe arthritis (Larsen grade III). Unconstrained arthroplasties have not performed as well as semiconstrained arthroplasties after previous radial head resections. However, both types of arthroplasties performed better in native elbows. Synovectomies should be reserved for less advanced disease states.**
**REFERENCES: Whaley A, Morrey BF, Adams R: Total elbow arthroplasty after previous resection of the radial head and synovectomy. J Bone Joint Surg Br 2005;87:47-53.**
**Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.**
**Schemitsch EH, Ewald FC, Thornhill TS: Results of total elbow arthroplasty after excision of the radial head and synovectomy in patients who had rheumatoid arthritis. J Bone Joint Surg Am 1996;78:1541-1547.**
**29****. Which of the following conditions is associated with palmoplantar pustulosis?
1- Condensing osteitis
2- Sternoclavicular hyperostosis
3- Friedreich’s disease
4- Scleroderma
5- Reiter syndrome
PREFERRED RESPONSE: 2**
**DISCUSSION: Sternoclavicular hyperotosis is a seronegative and HLA-B27 negative rheumatic disease. In this condition, hyperostosis may appear in the spine, long bones, sacroiliac joints, and the sternoclavicular region. This entity is also associated with palmoplantar pustulosis.**
**REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.**
**Sonozaki H, Azuma A, Okai K, et al: Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg 1979;95:13-22.**
**30****. A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results?
1- Physical therapy and nonsteroidal anti-inflammatory drugs
2- Local corticosteroid injection and physical therapy
3- Open repair of the long head of the biceps
4- Open repair of the sternocostal portion of the pectoralis major tendon
5- Open repair of the clavicular portion of the pectoralis major tendon
PREFERRED RESPONSE: 4**
**DISCUSSION: The MRI scans show a rupture of the sternocostal portion of the pectoralis major tendon. This is the most common site of rupture and bench pressing is the most common etiology. Surgical repair yields better functional outcomes and patient satisfaction for tears not only at the tendon/bone interface but also at the myotendinous junction.**
**REFERENCES: Bak K, Cameron EA, Henderson IJ: Rupture of the pectoralis major: A
meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-119.**
**Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.**
**31****. A patient sustained a sharp laceration to the base of his left, nondominant thumb
4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?
1- Interphalangeal joint fusion
2- Intercalary tendon graft
3- Silicone rod placement
4- Primary flexor pollicis longus repair
5- Flexor digitorum superficialis transfer
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation.**
**REFERENCES: Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.**
**Posner MA: Flexor superficialis tendon transfers to the thumb: An alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am 1983;8:876-881.**
**32****. A 17-year-old javelin thrower reports medial-sided elbow pain and diminished grip strength while throwing. He has decreased sensation in the little and ring fingers of his throwing hand only while throwing. The sensory deficits resolve at rest. Examination of the elbow reveals no instability and full motion. He has a positive Tinel’s sign over the cubital tunnel and a positive elbow flexion test. Radiographs are normal. What is the next most appropriate step in management?
1- Anterior ulnar nerve transposition
2- Cortisone injection
3- Nighttime elbow extension splinting
4- Medial collateral ligament reconstruction
5- Ulnar nerve decompression in situ
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient’s symptoms and examination findings are consistent with ulnar neuritis/cubital tunnel syndrome, most probably exacerbated by javelin throwing. The first step includes rest and extension splinting. Surgical intervention should only be considered after failure of nonsurgical management.**
**REFERENCES: Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.**
**Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 65-69.**
**33****. What are the most likely symptoms and examination findings related to the mass in zone 2 of Guyon’s canal seen in Figure 17?
1- Numbness and tingling in the little finger and the ulnar side of the ring finger
2- Weakness and atrophy of the first dorsal interosseous
3- Hypothenar muscle atrophy
4- Dorsal ulnar hand numbness and tingling
5- Weakness of the interossei of the hand and numbness and tingling of the little finger and the ulnar side of the ring finger
PREFERRED RESPONSE: 2**
**DISCUSSION: The lesion lies in zone II of the ulnar tunnel. In that zone the deep motor branch of the ulnar nerve is susceptible to compression. Distal to the hook of the hamate, the motor branch of the ulnar nerve dives deep to innervate the interossei as it begins to move from an ulnar to radial direction. Because of its course, it has little or no give in response to a mass effect from the floor of Guyon’s canal. Ganglions are the most common cause of ulnar nerve entrapment in the wrist. Lesions in zone I can affect both sensory and motor aspects of the ulnar nerve as well as the motor innervation of the hypothenar muscles. Lesions at the elbow or mid-to-proximal forearm are associated with dorsal hand numbness and tingling.**
**REFERENCES: Kuschner SH, Gelberman RH, Jennings C: Ulnar nerve compression at the wrist. J Hand Surg Am 1988;13:577-580.**
**Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.**
**34****. A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
1- Superior labral detachment
2- Engaging Hill-Sachs lesion
3- Large glenoid rim fracture
4- Avulsion of the inferior glenohumeral ligament from the humerus
5- Avulsion of the anterior inferior glenoid labrum
PREFERRED RESPONSE: 5**
**DISCUSSION: In an acute first-time dislocation, arthroscopy has been shown to reveal a Bankart lesion in most shoulders. The classic finding of labral detachment from the anterior inferior glenoid along with occasional hemorrhage within the inferior glenohumeral ligament is the most common sequelae of a traumatic anterior inferior dislocation. Acute treatment, if chosen, is repair of the labral tissue back to the glenoid plus or minus any capsular plication to address potential plastic deformation of the glenohumeral ligament. Acute treatment of a patient sustaining a first-time dislocation remains controversial. The potential indications may be patients whose dislocation occurs at the end of a season and when the desire to minimize risk of future instability outweighs the risks of surgical intervention.**
**REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.**
**DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.**
**Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic,
first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.**
**35****. Examination of a hand with compartment syndrome is most likely to reveal which of the following?
1- Clenched fist
2- Intrinsic minus posturing
3- Pain with passive stretch
4- Compression of the superficial arch
5- Pallor
PREFERRED RESPONSE: 2**
**DISCUSSION: In a study of 19 patients with compartment syndrome of the hand, all had tense swollen hands with elevated compartment pressures. Most patients were neurologically compromised so pain with passive stretch may be difficult to illicit. Arterial inflow is present in the arch and thus pallor is not present. The typical posture of the hand is not clenched, rather it is an intrinsic minus posture of metacarpophalangeal joint extension and flexion of the proximal and distal interphalangeal joints.**
**REFERENCES: Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.**
**Dellaero DT, Levin LS: Compartment syndrome of the hand: Etiology, diagnosis, and treatment. Am J Orthop 1996;25:404-408.**
**36****. A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause
1- anterior translation of the humeral head.
2- loss of external rotation.
3- excessive tightening of the biceps tendon.
4- superior migration of the humeral head.
5- no excessive changes.
PREFERRED RESPONSE: 2**
**DISCUSSION: If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur.**
**REFERENCES: Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.**
**Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology, and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.**
**37****. Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a
21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient’s diagnosis?
1- Shortening of 3 cm
2- Severity of trauma
3- Duration of immobilization
4- Type of immobilization
5- Closed reduction
PREFERRED RESPONSE: 2**
**DISCUSSION: The more severe the trauma, the higher the rate of subsequent clavicular nonunion. Neither duration nor type of immobilization has been clearly demonstrated to be a causative factor in the development of nonunion. Similarly, closed reduction has not been found to alter the healing course in midshaft clavicular fractures.**
**REFERENCES: Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.**
**White RR, Anson PS, Kristiansen T, et al: Adult clavicle fractures: Relationship between mechanism of injury and healing. Orthop Trans 1989;13:514-515.**
**38****. A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values show a WBC count of 11,400/mm3 and an erythrocyte sedimentation rate of 52mm/h. What is the most appropriate action?
1- Begin a stretching program.
2- Obtain shoulder radiographs and aspirate the shoulder joint.
3- Obtain an MRI scan to evaluate for a rotator cuff tear.
4- Schedule for irrigation and debridement.
5- Schedule for revision shoulder arthroplasty.
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has the preliminary diagnosis of an infected shoulder arthroplasty; therefore, shoulder radiographs and joint aspiration for organism identification should be the first steps in the work-up. The patient is at risk for hematogenous spread given the recent history of pneumonia and her history of diabetes mellitus. Although she has stiffness, a stretching program is not indicated with the possibility of infection. Scheduling for revision arthroplasty, or irrigation and debridement will depend on multiple factors including identification of the infecting organism, the organism’s susceptibility to antibiotics, and implant stability. An MRI scan to evaluate for a rotator cuff tear is not indicated at this time.**
**REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 953-954.**
**Stinchfield FE, Bigliani LU, Neu HC, et al: Late hematogenous infection of total joint replacement. J Bone Joint Surg Am 1980;62:1345-1350.**
**39****. The usual presentation of traumatic subscapularis tears is most often seen after forced
1- internal rotation.
2- external rotation.
3- extension.
4- abduction.
5- forward flexion.
PREFERRED RESPONSE: 2**
**DISCUSSION: The typical mechanism of injury is a fall and the patient grasps something to prevent the fall. This maneuver forces the arm into external rotation against resistance.**
**REFERENCES: Kreuz PC, Remiger A, Erggelet C, et al: Isolated and combined tears of the subscapularis tendon. Am J Sports Med 2005;33:1831-1837.**
**Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.**
**40****. A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?
1- Arthroscopic reduction and fixation
2- Percutaneous pinning
3- Open reduction and internal fixation
4- Hemiarthroplasty with tuberosity reconstruction
5- Reverse shoulder arthroplasty
PREFERRED RESPONSE: 3**
**DISCUSSION: In this young patient, every attempt must be made to retain the native proximal humerus; therefore, open reduction and internal fixation should be attempted of both the articular segment and tuberosities to the humeral shaft. This is best accomplished through an open approach. Shoulder arthroplasty should be reserved for the elderly and for failed internal fixation.**
**REFERENCES: Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.**
**Aschauer E, Resch H: Four-part proximal humeral fractures: ORIF, in Warner JP, Iannotti JP, Flatow EL (eds): Complex and Revision Problems in Shoulder Surgery, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 289-309. **
**41****. A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?
1- Semitendinosis figure-of-eight graft
2- Subclavius tendon transfer
3- Medial clavicular osteotomy
4- Medial clavicular resection
5- Sternoclavicular arthrodesis
PREFERRED RESPONSE: 1**
**DISCUSSION: Improved peak-to-load failure data have been demonstrated by reconstruction of the sternoclavicular joint using a semitendinosis graft in a figure-of-eight pattern through the clavicle and manubrium. Resection of the medial clavicle, which compromises the integrity of the costoclavicular ligament, results in medial clavicular instability.**
**REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.**
**Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.**
**42****. Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
1- Sickle cell disease
2- Associated malunion
3- Alcoholic-induced disease
4- Previously received high-dose steroids
5- Postradiation necrosis
PREFERRED RESPONSE: 1**
**DISCUSSION: The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use.**
**REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.**
**Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.**
**43****. A 26-year-old right hand-dominant man has had right shoulder pain for the past
6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O’Brien’s active compression test. What is the next most appropriate step in the diagnosis of this patient?
1- Diagnostic arthroscopy
2- MRI-arthrography
3- Stress radiographs
4- CT
5- Weighted radiographs of the arm
PREFERRED RESPONSE: 2**
**DISCUSSION: MRI-arthrography has been shown to be an accurate technique for assessing the glenoid labrum in patients with suspected labral tears. Often standard MRI technique will not identify labral lesions. The use of MRI-arthrography with an intra-articular injection of gadolinium provides improved visualization of labral lesions. Bencardino and associates demonstrated a sensitivity of 89%, a specificity of 91%, and an accuracy of 90% in detecting labral lesions. SLAP lesions can be visualized on coronal oblique sequences as a deep cleft between the superior labrum and the glenoid that extends well around and below the biceps anchor. Often, contrast will diffuse into the labral fragment, causing it to appear ragged or indistinct.**
**REFERENCES: Applegate GR, Hewitt M, Snyder SJ, et al: Chronic labral tears: Value of magnetic resonance arthrography in evaluating the glenoid labrum and labral-bicipital complex. Arthroscopy 2004;20:959-963.**
**Bencardino JT, Beltran J, Rosenberg ZS, et al: Superior labrum anterior-posterior lesions: Diagnosis with MR arthrography of the shoulder. Radiology 2000;214:267-271.**
**Nam EK, Snyder SJ: The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:798-810.**
**44****. A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month follow-up appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in
Figure 21. What is the most likely diagnosis?
1- Flexor pollicis longus rupture
2- Median nerve palsy
3- Ulnar nerve palsy
4- Anterior interosseous nerve palsy
5- Posterior interosseous nerve palsy
PREFERRED RESPONSE: 4**
**DISCUSSION: The photograph shows the characteristic attitude of the hand when an anterior interosseous nerve palsy is present. The patient is unable to flex the interphalangeal joint to the joint of the thumb. Anterior interosseous nerve palsies are often misdiagnosed as tendon ruptures.**
**REFERENCES: Schantz K, Reigels-Nielsen P: The anterior interosseous nerve syndrome.
J Hand Surg Br 1992;17:510-512.**
**Seror P: Anterior interosseous nerve lesions: Clinical and electrophysiological features. J Bone Joint Surg Br 1996;78:238-241.**
**45****. A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow
9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
1- Bracing
2- Physiotherapy
3- Cortisone injection
4- Conversion to total elbow arthroplasty
5- Revision interposition arthroplasty
PREFERRED RESPONSE: 4**
**DISCUSSION: In a series reported by Blaine and associates, 12 patients were converted from interposition to total elbow arthroplasty. This procedure was successful in 10 out of 12 patients.**
**REFERENCES: Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.**
**Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.**
**46****. What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?
1- Lateralization of the center of rotation, lengthening the deltoid, and decreasing the deltoid moment arm
2- Lateralization of the center of rotation, shortening the deltoid, and decreasing acromial stress
3- Lateralization of the center of rotation, lengthening the deltoid, and increasing the transverse force couple
4- Medialization of the center of rotation, lengthening the deltoid, and increasing the deltoid moment arm
5- Medialization of the center of rotation, shortening the deltoid, and decreasing acromial stress
PREFERRED RESPONSE: 4**
**DISCUSSION: The Grammont reverse total shoulder arthroplasty is designed to medialize the center of rotation, thereby increasing the deltoid moment arm and lengthening the deltoid.**
**REFERENCES: Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.**
**Rittmeister M, Kerschbaumer M: Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg 2001;10:17-22.**
**47****. A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?
1- Pedicled vascularized bone graft
2- Long arm thumb spica cast
3- Percutaneous screw fixation
4- Corticocancellous bone grafting via a volar approach (Matti-Russe)
5- Open reduction and differential pitch screw placement via a dorsal approach
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures.**
**REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.**
**Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.**
**48****. A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
1- Hemiarthroplasty
2- Arthroscopic debridement
3- Total shoulder arthroplasty with a cemented all-polyethelene glenoid component
4- Reverse total shoulder arthroplasty
5- Total shoulder arthroplasty with a metal-backed glenoid component
PREFERRED RESPONSE: 3**
**DISCUSSION: Most studies have shown that total shoulder arthroplasties yield better pain relief and improved forward elevation when compared to hemiarthroplasty in patients with rheumatoid arthritis. Although rotator cuff tears are more common in this patient population, this patient has good forward elevation and no significant superior migration of the humeral head; therefore, a reverse arthroplasty is not indicated. The arthritis is too advanced in this patient to consider arthroscopy, but in less advanced cases it can improve range of motion and decrease pain. Metal-backed glenoid components have shown higher rates of loosening.**
**REFERENCES: Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496.**
**Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.**
**Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.**
**49****. A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented
all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?
1- Maintain sling immobilization for 6 weeks, and then begin a global
range-of-motion program.
2- Maintain sling immobilization for 3 weeks, and then begin a global
range-of-motion program.
3- Immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side.
4- Immediately begin a passive range-of-motion program for forward elevation only; no external rotation is allowed for 6 weeks.
5- Immediately begin active range of motion in forward elevation and external rotation to the side with a progression to full rotator cuff strengthening in
3 weeks.
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient needs to immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side. Sling immobilization without stretching for either 3 or 6 weeks will result in severe stiffness that will compromise her ultimate range of motion. Since she has a good quality subscapularis tendon, there is no need to avoid beginning external rotation to the side. However, starting a strengthening program
at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal. **
**REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.**
**Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.**
**50****. A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
1- Calcific tendinitis
2- Poliomyelitis
3- Diskogenic cervical spine disease
4- Impingement
5- Brachial neuritis
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has symptoms and examination findings of acute brachial neuritis which is often a diagnosis of exclusion. The recent viral flu-like symptoms have shown a correlation with the development of this disorder. The acute, severe shoulder weakness excludes calcific tendinitis, impingement, and poliomyelitis. A normal cervical spine examination makes cervical disk disease unlikely.**
**REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.**
**Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.**
**51****. A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?
1- Open reduction and internal fixation
2- External bone stimulator
3- Ninety-degree abduction splint
4- Arthroscopic acromioplasty
5- Fragment excision
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient has a displaced scapular spine fracture that has resulted in shoulder weakness from a poor deltoid lever arm. The downward tilt may lead to subacromial impingement and rotator cuff dysfunction. Open reduction and internal fixation would best allow normal deltoid and shoulder function. Bone stimulators and abduction bracing may lead to healing but in a malunited position. Arthroscopic acromioplasty and fragment excision should be avoided.**
**REFERENCES: Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine.
J Shoulder Elbow Surg 1997;6:544-548.**
**Ada Jr, Miller ME: Scapular fractures: Analysis of 113 cases. Clin Orthop Relat Res 1991;269:174-180.**
**52****. A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
1- UCL repair and nighttime elbow extension splinting
2- UCL repair with ulnar nerve decompression in situ
3- Allograft UCL reconstruction with interference screws
4- Autograft UCL reconstruction with ulnar nerve transposition
5- Autograft UCL reconstruction using a docking technique
PREFERRED RESPONSE: 4**
**DISCUSSION: High-level pitchers with symptomatic UCL tears require reconstruction, with autograft being the best studied graft selection. With concomitant ulnar nerve symptoms, a simultaneous ulnar nerve transposition provides good results. Ligament “repairs” and allograft reconstructions have not shown good long-term results.**
**REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.**
**Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.**
**53****. A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?
1- Closed reduction and cast immobilization for 4 weeks, followed by therapy directed at regaining motion
2- Open reduction and internal fixation of the olecranon fracture, functional bracing of the humeral fracture, and therapy directed at regaining motion initiated at 2 weeks after surgery
3- Open reduction and internal fixation of the olecranon and humeral fractures, followed by therapy directed at regaining motion
4- Open reduction and internal fixation of the olecranon and humeral fractures, and splint immobilization for 4 weeks followed by therapy directed at regaining motion
5- Open reduction and internal fixation of the olecranon fracture, functional bracing of the humeral fracture, and therapy directed at regaining motion initiated at 4 weeks after surgery
PREFERRED RESPONSE: 3**
**DISCUSSION: The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended.**
**REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.**
**Yokoyama K, Itoman M, Kobayashi A, et al: Functional outcomes of “floating elbow” injuries in adult patients. J Orthop Trauma 1998;12:284-290.**
**54****. A patient who underwent open reduction and internal fixation of an olecranon fracture
2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?
1- Continued observation and home therapy
2- Radiation therapy, followed by aggressive range-of-motion exercises
3- Formal physical therapy and static progressive splinting
4- Revision open reduction and internal fixation and capsular release
5- Manipulation under anesthesia
PREFERRED RESPONSE: 3**
**DISCUSSION: The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern.**
**REFERENCES: Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res
2005;431:26-35.**
**King GJ, Faber KJ: Posttraumatic elbow stiffness. Orthop Clin North Am 2000;31:129-143.**
**55****. A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of
25 degrees. The O’Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
1- MRI-arthrogram to evaluate the rotator cuff
2- Rotator cuff strengthening program
3- Posterior capsular stretching program
4- Shoulder arthroscopy with SLAP repair
5- Shoulder arthroscopy with posterior capsular release
PREFERRED RESPONSE: 3**
**DISCUSSION: Throwing athletes with symptomatic internal rotation deficits often benefit from an intensive posterior capsular stretching program. Patients that fail to respond to nonsurgical management may benefit from an arthroscopic posterior capsular release.**
**REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.**
**Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.**
**56****. A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
1- Arthroscopic debridement
2- Arthroscopic rotator cuff repair
3- Hemiarthroplasty with rotator cuff repair
4- Total shoulder arthroplasty
5- Reverse shoulder arthroplasty
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains.**
**REFERENCES: Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.**
**Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.**
**57****. A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended?
1- No external rotation stretching for the first 6 weeks.
2- No external rotation stretching for the first 3 weeks.
3- Limit external rotation to the side to 60 degrees for the first 6 weeks.
4- Limit external rotation to the side to 60 degrees for the first 3 weeks.
5- No restrictions on external rotation stretching.
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient needs restrictions on his external rotation to allow healing of the subscapularis tendon repair. Limitation to 60 degrees is common if the tendon repair is robust and shows no evidence of tension on range-of-motion testing during the surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery.**
**REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.**
**Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.**
**58****. A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in
Figures 28a and 28b. What is the most likely diagnosis?
1- Adhesive capsulitis
2- Calcific tendinitis
3- Anterior shoulder dislocation
4- Posterior shoulder dislocation
5- Glenohumeral osteoarthritis
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation.**
**REFERENCES: Robinson CM, Aderinto J: Posterior shoulder dislocations and
fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.**
**Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.**
**59****. A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?
1- Pedicled vascularized bone graft
2- Long arm thumb spica cast
3- Percutaneous screw fixation
4- Corticocancellous bone grating via a volar approach (Matti-Russe)
5- Open reduction and differential pitch screw placement via a dorsal approach
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient has a nonunion of the proximal pole of the scaphoid. Acutely, this can be repaired with a screw alone, but as a nonunion the proximal pole has very poor healing potential. Vacularized bone grafts have been successful for these challenging nonunions, particularly in adolescents. A cast can be used for nondisplaced acute waist fractures, and corticocancellous grafts can be used for nonunions of the waist.**
**REFERENCES: Waters PM, Stewart SL: Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84:915-920.**
**Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391-401.**
**60****. A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?
1- Osteonecrosis of the humeral head
2- Partial-thickness supraspinatus tendon tear
3- Full-thickness supraspinatus tendon tear
4- Glenohumeral septic arthritis
5- Rheumatoid arthritis
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient has osteonecrosis of the humeral head. The radiographs show increased density in the superior subchondral region of the humeral head. The MRI scans reveal a central collapse of the humeral head. The patient’s history of severe asthma and long-term prednisone use predisposes her to this condition. The MRI scans show no evidence of a full- or partial-thickness rotator cuff tear. Without a history of fevers, chills, or other systemic signs or symptoms, there is no indication of septic arthritis. The radiographs do not reveal periarticular erosions, commonly seen in rheumatoid arthritis.**
**REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.**
**Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.**
**61****. A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
1- Resurfacing hemiarthroplasty
2- Resurfacing hemiarthroplasty with fascial glenoid resurfacing
3- Resurfacing hemiarthroplasty with cemented glenoid component
4- Stemmed hemiarthroplasty
5- Stemmed total shoulder arthroplasty
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future.**
**REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.**
**Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.**
**62****. A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
1- Vascularized fibular graft
2- Locked intramedullary rodding
3- Tricortical iliac crest grafting and compression plating
4- Cancellous autograft and plating
5- BMP-7
PREFERRED RESPONSE: 4**
**DISCUSSION: In an atrophic nonunion with a good soft-tissue envelope, adequate plating with cancellous bone graft can be used to span defects of up to 6 cm. Cortical graft from the fibula or iliac crest is not necessary. BMP-7 is a bone graft substitute and should not be used alone in this patient because the hardware is loose.**
**REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.**
**63****. A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
1- Anterior glenoid rim fracture tear
2- Anterior inferior labral tear
3- Posterior labral tear
4- Total capsular laxity
5- Osteochondral defect of the humeral head
PREFERRED RESPONSE: 3**
**DISCUSSION: Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers.
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability. **
**REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.**
**Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.**
**Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.**
**64****. A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
1- Immobilization in a sling and swathe
2- Open capsular shift
3- Arthroscopic capsular plication
4- Thermal capsulorrhaphy
5- Physical therapy and home exercises
PREFERRED RESPONSE: 5**
**DISCUSSION: Multidirectional instability of the shoulder is defined as symptomatic instability in two or more directions (anterior, posterior) but must include a component of inferior instability. Initial treatment should always include physical therapy and instruction in a home exercise program that emphasizes periscapular and rotator cuff strengthening to improve the dynamic stability of the glenohumeral joint. Immobilization has not been shown to be effective. Open capsular shift and arthroscopic capsular plication remain the surgical options when appropriate nonsurgical management fails (typically a minimum of 6 months of dedicated therapy and home program). Thermal capsulorrhaphy remains controversial but is not recommended by many clinicians because of reported complications including recurrent instability, axillary nerve injury, chondrolysis, and capsular injury.**
**REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.**
**D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.**
**Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.**
**Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.**
**65****. In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
1- Insulin dependence
2- Gram-positive organisms
3- Renal failure
4- Retinopathy
5- Peripheral neuropathy
PREFERRED RESPONSE: 3**
**DISCUSSION: Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections.**
**REFERENCES: Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686.**
**Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.**
**Kour AK, Looi KP, Phone MH, et al: Hand infections in patients with diabetes. Clin Orthop Relat Res 1996;331:238-244.**
**66****. A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
1- First rib
2- Intra-articular disk ligament
3- Costoclavicular ligament
4- Interclavicular ligament
5- Posterior sternoclavicular joint capsule
PREFERRED RESPONSE: 5**
**DISCUSSION: Through cadaveric study, Spencer and associates measured anterior and posterior translation of the sternoclavicular joint. The study demonstrated that the posterior sternoclavicular joint capsule is the most important structure for preventing both anterior and posterior translation of the sternoclavicular joint.**
**REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.**
**Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.**
**67****. Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?
1- Type I acromion
2- Type III acromion
3- Meso os acromiale
4- Meta os acromiale
5- Pre os acromiale
PREFERRED RESPONSE: 3**
**DISCUSSION: The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient.**
**REFERENCES: Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.**
**Sammarco VJ: Os acromiale: Frequency, anatomy, and clinical implications. J Bone Joint Surg Am 2000;82:394-400.**
**68****. What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
1- Ipsilateral total elbow arthroplasty
2- Contralateral wrist arthrodesis
3- Type III degenerative changes of the wrist
4- Age older than 55 years
5- Less than 30 degrees of wrist flexion/extension
PREFERRED RESPONSE: 2**
**DISCUSSION: The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty.**
**REFERENCES: Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204.**
**Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.**
**Carlson JR, Simmons BP: Total wrist arthroplasty. J Am Acad Orthop Surg 1998;6:308-315.**
**69****. What is the most likely cause of the lesion shown in Figures 35a and 35b?
1- Surgery
2- Contusion
3- Parathyroid tumor
4- Bisphosphonate use
5- Corticosteroid use
PREFERRED RESPONSE: 2**
**DISCUSSION: The most common cause of myositis ossificans is contusion. Certain regions, including the quadriceps and brachialis, are more commonly affected. The mechanisms of development have not been clearly established.**
**REFERENCES: Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.**
**Jarvinen TA, Jarvinen TL, Kaariainen M, et al: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33:745-764.**
**70****. During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
1- Tenosynovectomy
2- Recentering
3- Deepening of the bicipital groove
4- Tenodesis or tenotomy
5- Lysis of sheath adhesion
PREFERRED RESPONSE: 4**
**DISCUSSION: With subscapularis tendon ruptures that have biceps tendon pathology, treatment with tenodesis or tenotomy has improved clinical results. Subluxation or dislocation of the biceps tendon is common with subscapularis rupture. Dislocation of the biceps can occur either beneath the tendon, within the tendon, or extra-articularly. In all cases, the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears.**
**REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.**
**Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.**
**Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.**
**71****. What is the most common bacteria cultured from dog and cat bites to the upper extremity?
1- Pasteurella
2- Streptococcus
3- Staphylococcus
4- Bacteroides
5- Moraxella
PREFERRED RESPONSE: 1**
**DISCUSSION: To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.**
**REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.**
**72****. A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
1- Brachiocephalic
2- Innominate
3- Subclavian
4- Axillary
5- Circumflex scapular
PREFERRED RESPONSE: 4**
**DISCUSSION: The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.**
**REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.**
**73****. Which of the following structures may help maintain radial length after a radial head fracture?
1- Triangular fibrocartilage complex
2- Medial ulnar collateral ligament
3- Lateral ulnar collateral ligament
4- Annular ligament
5- Coronoid
PREFERRED RESPONSE: 1**
**DISCUSSION: Essex-Lopresti injuries affect axial stability of the forearm. Injury to the interosseous membrane or the triangular fibrocartilage complex can result in proximal migration of the radius.**
**REFERENCES: Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.**
**Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.**
**74****. An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
1- exploration and neurolysis/repair.
2- MRI of the arm.
3- functional electrical stimulation.
4- radial nerve tendon transfers.
5- observation.
PREFERRED RESPONSE: 5**
**DISCUSSION: In patients with radial nerve injuries with closed humeral fractures, it has been reported that 85% to 95% spontaneously recover. Based on this premise, most surgeons favor expectant management of these injuries. Even if there is no evidence of recovery at 6 weeks, repeat electromyography at 12 weeks is advocated. If there is no clinical or electromyographic signs of recovery at 6 months, exploration is recommended. If the nerve is in continuity at the time of exploration, nerve action potentials are useful in helping determine the need for neurolysis, excision, and grafting, or if excision and repair is the best option.**
**REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.**
**Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.**
**75****. A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
1- Shoulder fusion
2- Arthroscopic subscapularis repair
3- Intra-articular corticosteroid injection
4- Open subscapularis repair
5- Pectoralis major transfer
PREFERRED RESPONSE: 5**
**DISCUSSION: Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function.**
**REFERENCES: Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.**
**Resch H, Povacz P, Ritter E, et al: Transfer of the pectoralis major muscle for the treatment of irreparable rupture of the subscapularis tendon. J Bone Joint Surg Am 2000;82:372-382.**
**76****. Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
1- The amount of change in the score over time
2- Sensitivity of the measure in evaluating a problem
3- The ability of the instruments to actually measure what it intends to measure
4- The measure of change over the course of treatment
5- The reproducibility of the measurements either between repeated tests or between observers
PREFERRED RESPONSE: 5**
**DISCUSSION: The recent JBJS article by Kocher and associates defines the different psychometric properties that are used in outcome measures. Reliability is a measure of how reproducible a test is. This can be interobserver reliability (ie, reliability between people), or intraobserver reliability (ie, reliability for the same person doing the outcome measure at different occasions).**
**REFERENCE: Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.**
**77****. With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
1- Coracohumeral
2- Superior glenohumeral
3- Middle glenohumeral
4- Anterior band of the inferior glenohumeral ligament complex
5- Posterior band of the inferior glenohumeral ligament complex
PREFERRED RESPONSE: 4**
**DISCUSSION: With the arm in the abducted, externally rotated position, the anterior band of the inferior glenohumeral ligament complex moves anteriorly, preventing anterior humeral head translation. Both the coracohumeral ligament and the superior glenohumeral ligament restrain the humeral head to inferior translation of the adducted arm, and to external rotation in the adducted position. The middle glenohumeral ligament is a primary stabilizer to anterior translation with the arm abducted to 45 degrees. The posterior band of the inferior glenohumeral ligament complex resists posterior translation of the humeral head when the arm is internally rotated.**
**REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.**
**Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.**
**78****. Figure 37 shows a coronal T2-weighted MRI scan. What is the name of the labeled torn structure?
1- Brachialis tendon
2- Biceps tendon
3- Flexor/pronator origin
4- Medial collateral ligament (MCL)
5- Lateral collateral ligament (LCL)
PREFERRED RESPONSE: 5**
**DISCUSSION: The labeled structure is the LCL, and it is avulsed from the lateral humeral epicondyle. This is the most common site of injury for the LCL. The biceps and brachialis tendon insertions are not well visualized in this section. The MCL and flexor/pronator origin
are intact.**
**REFERENCES: Potter HG, Weiland AJ, Schatz JA, et al: Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology 1997;204:185-189.**
**King JC, Spencer EE: Lateral ligamentous instability: Techniques of repair and reconstruction. Techniques in Orthopaedics 2000;8:93-104.**
**79****. The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with
1- anterior superior escape.
2- rheumatoid arthritis.
3- an acromial stress fracture.
4- a centered head and an external rotation lag sign of 50 degrees.
5- active forward elevation of 130 degrees.
PREFERRED RESPONSE: 1**
**DISCUSSION: Reverse total shoulder arthroplasty is relatively contraindicated in patients with acromial stress fractures and rheumatoid arthritis. A patient with active forward elevation to
130 degrees is better treated with a hemiarthroplasty because the motion already exceeds the average forward elevation attained in most studies using the reverse prosthesis. A centered case of rotator cuff tear arthropathy is also better treated with a hemiarthroplasty, especially in patients with a large external rotation lag sign because the reverse prosthesis has been shown to decrease active external rotation. However, hemiarthroplasties have not performed well in patients with anterior superior escape and in this group of patients, the reverse prosthesis is best.**
**REFERENCES: Rittmeister M, Kerschbaumer M: Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg 2001;10:17-22.**
**Visotosky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.**
**Werner CM, Steinmann PA, Gilbart M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis.
J Bone Joint Surg Am 2005;87:1476-1486.**
**80****. Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
1- Dorsal comminution
2- Volar comminution
3- Radial comminution
4- Intra-articular fracture
5- Physeal fracture
PREFERRED RESPONSE: 2**
**DISCUSSION: Intrafocal pinning allows the Kirschner wires to be placed through a site of comminution and then drilled through intact cortex. Generally Kapandji intrafocal pinning is done for dorsal comminuted extra-articular dorsal bending fractures, but it also may be used to elevate and buttress radial comminution. Simple intra-articular fractures can also be treated with pinning alone. Intrafocal pinning works best as a dorsal or radial buttress to prevent shortening. When there is volar comminution, the fracture is prone to shortening and supplemental external fixation or plating is recommended.**
**REFERENCES: Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394.**
**Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.**
**Weil WM, Trumble TE: Treatment of distal radius fractures with intrafocal (Kapandji) pinning and supplemental skeletal stabilization. Hand Clin 2005;21:317-328.**
**81****. Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?
1- Reverse shoulder arthroplasty
2- Hemiarthroplasty
3- Resurfacing of the humeral head
4- Arthroscopic debridement
5- Shoulder fusion
PREFERRED RESPONSE: 1**
**DISCUSSION: The authors of several studies conducted in Europe have reported promising results in the short- and medium-term with use of a reversed or inverted shoulder implant. The most recent investigation, a multicenter study in Europe in which 77 patients (80 shoulders) with glenohumeral osteoarthritis and a massive rupture of the rotator cuff were treated with the Delta III prosthesis, described an improvement in the mean constant score of 42 points, an increase of 65 degrees in forward elevation, and minimal or no pain in 96% of the patients. Hemiarthroplasty, the “nonconstrained” option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform.**
**REFERENCES: Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268.**
**Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.**
**Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.**
**82****. An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
1- Improved superior stability
2- Fixed fulcrum kinematics
3- Creates a metal-to-bone articulation with the acromion
4- Increased deltoid moment arm
5- Increased glenohumeral offset
PREFERRED RESPONSE: 3**
**DISCUSSION: The theoretic advantage of a metal-to-bone articulation with the acromion is that there is a greater arc in which a smooth metal surface contacts the glenoid and acromion. This may improve pain and function, but no studies have evaluated this to date. One study showed results comparable to that of a standard hemiarthroplasty. There are no other biomechanic advantages.**
**REFERENCES: Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.**
**Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.**
**83****. A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder “slip out” when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management?
1- Echocardiography
2- Abdominal ultrasound
3- Skeletal survey
4- Glenoid osteotomy
5- Physical therapy
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs show glenoid hypoplasia. The common radiographic findings of glenoid hypoplasia include an inferior and posterior glenoid deficiency, enlargement of the distal end of the clavicle, and sometimes an indentation in the glenoid. It is usually bilateral and rarely associated with other syndromes; therefore, an echocardiogram, abdominal ultrasound, or a skeletal survey is unnecessary unless the patient has stigmata of a syndrome such as Holt-Oram or Apert’s. Although posterior instability has been reported, the results of glenoid osteotomy have been variable and should not be considered initially. Physical therapy is the mainstay of initial management, but the patient should be counseled that this may be a recurrent problem with early osteoarthritis developing in many patients. Radiographs of the contralateral side should be obtained because this is usually bilateral.**
**REFERENCES: Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.**
**Smith SP, Bunker TD: Primary glenoid dysplasia: A review of twelve patients. J Bone Joint Surg Br 2001;83:868-872.**
**84****. A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?
1- Closed reduction and casting for 4 weeks
2- Closed reduction and bracing with immediate range of motion
3- Open reduction, lateral collateral ligament repair, and open reduction and internal fixation or metallic replacement of the radial head
4- Open reduction, radial head silastic arthroplasty, and lateral collateral ligament repair
5- Open reduction, lateral collateral ligament repair, and radial head excision
PREFERRED RESPONSE: 3**
**DISCUSSION: The radiographs show an elbow dislocation associated with a comminuted radial head fracture. In the setting of comminution and instability, factures of the radial head are best managed with an arthroplasty rather than open reduction and internal fixation. Resection of the radial head will worsen the instability and is not recommended. Silastic radial head replacements are contraindicated.**
**REFERENCES: Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.**
**O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. Instr Course Lect
2001;50:89-102.**
**85****. Osteochondritis dissecans of the capitellum is a source of elbow pain and most commonly occurs in what patient population?
1- Swimmers and divers
2- Football lineman
3- Rugby players
4- Gymnasts and throwing athletes
5- Cyclists
PREFERRED RESPONSE: 4**
**DISCUSSION: The etiology of osteochondritis dissecans of the capitellum is somewhat unclear. However, trauma has been implicated in this disease process. Gymnasts who load their upper extremities during tumbling and throwing athletes with repetitive trauma during the throwing motion are common patient subgroups in which osteochondritis dissecans of the elbow is seen. This often occurs in the adolescent age population.**
**REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998;26:520-523.**
**Takahara M, Ogino T, Fukushima S, et al: Nonoperative treatment of osteochondritis dissecans of the humeral capitellum. Am J Sports Med 1999;27:728-732.**
**86****. An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
1- Surgical fixation with percutaneous pins
2- Surgical fixation with a hemiarthroplasty with tuberosity repair
3- Surgical fixation with a total shoulder arthroplasty
4- Sling immobilization for 6 weeks followed by active range of motion
5- Sling immobilization with daily pendulum exercises
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has a displaced four-part proximal humerus fracture. Given her age and the presence of osteopenia, a cemented hemiarthroplasty is the treatment of choice. The glenoid is uninjured so a total shoulder arthroplasty is not indicated. Percutaneous pinning in younger individuals with good bone quality may be indicated but not in an 82-year-old woman with osteopenia. Sling immobilization and immediate pendulum exercises will lead to a nonunion. Sling immobilization for 6 weeks followed by active range of motion will result in a nonunion or malunion with unacceptable functional results.**
**REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.**
**Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.**
**87****. Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
1- Vigorous physical therapy
2- Manipulation under anesthesia
3- Arthroscopic capsular release
4- Hemiarthroplasty
5- Arthroscopic capsular plication
PREFERRED RESPONSE: 4**
**DISCUSSION: Appropriate treatment is based on multiple considerations, which include the chronicity of the dislocation, the amount of humeral head involvement, the medical condition, and functional limitations of the patient. It has been shown that shoulder arthroplasty for locked posterior dislocation provides pain relief and improved motion. Transfer of the lesser tuberosity with its attached subscapularis tendon into the defect is recommended for anteromedial humeral defects that are smaller than approximately 40% of the joint surface. Subscapularis transfer as described by McLaughlin and the modification thereof later described by Hawkins and associates in which the lesser tuberosity is transferred into the defect, have yielded good results if the defect is less than 40% of the humeral head. Prosthetic replacement is preferred for larger defects. If the dislocation is less than 3 weeks old and has less than 25% of humeral head involvement, closed reduction with the patient under general anesthesia should be attempted and the stability assessed by internally rotating the arm. If the arm can be safely internally rotated to the abdomen, then 6 weeks of immobilization in an orthosis that maintains the shoulder in slight extension and external rotation can yield a good result. If the dislocation has been present for more than 3 weeks, closed reduction becomes exceedingly difficult.**
**REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.**
**Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.**
**Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.**
**Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.**
**McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.**
**88****. In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
1- Extensor digiti quinti
2- Abductor pollicis longus
3- Extensor pollicis longus
4- Extensor carpi radialis brevis
5- Extensor carpi ulnaris
PREFERRED RESPONSE: 1**
**DISCUSSION: The tendon most prone to rupture in a patient with rheumatoid arthritis of the wrist is the extensor digiti quinti. It can be a silent injury since the extensor digitorum communis can provide extension to the fifth finger. The extensor digiti quinti is at high risk since it is overlying the ulnar head where it is prone to attritional rupture (Vaughan-Jackson syndrome).**
**REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.**
**Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.**
**89****. A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?
1- Nonsteroidal anti-inflammatory drugs, cortisone injection, and physical therapy
2- Total shoulder arthroplasty
3- Shoulder fusion
4- Arthroscopic debridement and capsular release
5- Humeral head resurface arthroplasty
PREFERRED RESPONSE: 1**
**DISCUSSION: The patient is a young laborer with osteoarthritis. Initial treatment should begin with nonsurgical management that may include anti-inflammatory drugs, cortisone injections, and physical therapy to diminish pain and improve motion. The other choices may eventually be necessary but should only follow a course of nonsurgical management.**
**REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.**
**Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.**
**90****. What is the most appropriate surgical treatment for a stage III symptomatic scapholunate advanced collapsed (SLAC) wrist?
1- Radioscapholunate arthrodesis
2- Scaphotrapeziotrapezoid arthrodesis
3- Scaphocapitate arthrodesis
4- Proximal row carpectomy
5- Scaphoid excision and capitate-lunate-triquetrum-hamate arthrodesis
PREFERRED RESPONSE: 5**
**DISCUSSION: SLAC is the end result of chronic scapholunate instability. The arthritis follows a predictable pattern. Stage I disease involves cartilage loss between the waist of the scaphoid and the radial styloid. In stage II, the arthritis progresses to include the proximal pole of the scaphoid and the scaphoid fossa of the radius. Finally, stage III goes on to include arthritis of the capitolunate joint. The only treatment option that addresses all of the sites of arthritis is the scaphoid excision and four corner fusion.**
**REFERENCES: Ashmead DT IV, Watson HK, Damon C, et al: Scapholunate advanced collapse wrist salvage. J Hand Surg Am 1994;19:741-750.**
**Sauerbier M, Trankle M, Linsner G, et al: Midcarpal arthrodesis with complete scaphoid excision and interposition bone graft in the treatment of advanced carpal collapse (SNAC/SLAC wrist): Operative technique and outcome assessment. J Hand Surg Br 2000;25:341-345.**
**91****. A 25-year-old man shot himself at the base of the right index finger while cleaning his handgun. Examination reveals that the finger is cool and cyanotic. A clinical photograph and radiograph are shown in Figures 44a and 44b. What is the recommended treatment?
1- Open reduction and internal fixation and arterial reconstruction
2- Crossed pinning with Kirschner wires
3- Open (Guillotine) finger amputation
4- Index ray amputation
5- Application of an external fixator
PREFERRED RESPONSE: 4**
**DISCUSSION: The gunshot wound has caused injury to multiple systems: bone, vascular, skin, and tendon; therefore, the treatment of choice is amputation. An immediate ray amputation allows for a more rapid return to activities and less time off work.**
**REFERENCES: Peimer CA, Wheeler DR, Barrett A, et al: Hand function following single ray amputation. J Hand Surg Am 1999;24:1245-1248.**
**Neumeister MW, Brown RE: Mutilating hand injuries: Principles and management. Hand Clin 2003;19:1-15.**
**92****. What are the two terminal branches of the lateral cord of the brachial plexus?
1- Musculocutaneous and median
2- Musculocutaneous and axillary
3- Median and axillary
4- Ulnar and median
5- Ulnar and medial pectoral
PREFERRED RESPONSE: 1**
**DISCUSSION: The lateral cord divides into the musculocutaneous and median nerves. The posterior cord terminates into the axillary and radial nerves. The medial cord divides into the ulnar and median nerves.**
**REFERENCES: Hollinshead WH: Anatomy for Surgeons, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.**
**Shin AY, Spinner RJ, Steinmann SP, et al: Adult traumatic brachial plexus injuries. J Am Acad Orthop Surg 2005;13:382-396.**
**93****. A 32-year-old patient reports progressively increasing pain and stiffness after undergoing arthroscopic shoulder stabilization 1 year ago. The stabilization procedure was a Bankart repair with anchor fixation and supplemented with the heat probe. Radiographs are shown in Figures 45a and 45b. What is the most likely diagnosis?
1- Subscapularis failure
2- Frozen shoulder
3- Recurrent instability
4- Loose body
5- Chondrolysis
PREFERRED RESPONSE: 5**
**DISCUSSION: Postshoulder stabilization chondrolysis is a rare but devastating complication. It has been implicated with the use of the radiofrequency heat probe in some patients.**
**REFERENCES: Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.**
**Petty DH, Jazrawi LM, Estrada LS, et al: Glenohumeral chondrolysis after shoulder arthroscopy: Case reports and review of the literature. Am J Sports Med 2004;32:509-515.**
**94****. A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management?
1- Total shoulder arthroplasty
2- Hemiarthroplasty with glenoid interposition
3- Surface replacement hemiarthroplasty
4- Arthroscopic debridement
5- Anti-inflammatory drugs and a range-of-motion stretching program
PREFERRED RESPONSE: 5**
**DISCUSSION: New onset pain and stiffness in the young arthritic shoulder is a difficult problem to treat. Initial management should be aimed at reducing pain and improving motion in all planes. This patient’s activities and age preclude a shoulder arthroplasty at this time. If nonsurgical management fails to provide relief, then arthroscopic debridement and capsular release may be beneficial.**
**REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.**
**Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.**
**95****. A 23-year-old man who is a competitive overhead athlete has shoulder pain. Based on the pathology shown in Figure 47, what treatment option would yield the highest satisfaction and return to overhead sports?
1- Biceps tenodesis
2- Biceps tenotomy
3- Labral debridement
4- Labral repair
5- Rotator cuff debridement
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a classic type II SLAP tear that will respond best to arthroscopic repair. Labral debridement has been shown to lead to predictably poor results, and biceps tenodesis and tenotomy may be appropriate for an older patient who is not a competitive overhead athlete.**
**REFERENCES: Snyder SJ, Karzel RP, Del Pizzo W, et al: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.**
**Altchek DW, Warren RF, Wickiewicz TL, et al: Arthroscopic labral debridement: A three-year follow-up study. Am J Sports Med 1992;20:702-706.**
**96****. Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
1- subglenoid dislocation.
2- subcoracoid dislocation.
3- fracture of the greater tuberosity.
4- fracture of the greater tuberosity and glenoid rim.
5- pediatric-age patients.
PREFERRED RESPONSE: 4**
**DISCUSSION: Redislocation following acute dislocation occurs in approximately 3% of patients. This redislocation tends to occur in middle-aged and elderly patients. A higher incidence of redislocation occurs when there are accompanying fractures of the glenoid rim and the greater tuberosity.**
**REFERENCES: Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment.
J Bone Joint Surg Am 2002;84:1552-1559.**
**Bigliani LU, Newton PM, Steinmann SP, et al: Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. J Sports Med 1998;26:41-45.**
**97****. A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis?
1- Flexor-pronator avulsion
2- Ulnar nerve subluxation
3- Medial collateral ligament injury
4- Lateral ulnar collateral ligament rupture
5- Triceps tendon subluxation
PREFERRED RESPONSE: 3**
**DISCUSSION: The milking test, as seen in the photograph, elicits pain when a tear is present in the medial collateral ligament. Complete rupture is possible but unlikely when there is no history of trauma and the patient is able to throw pain-free for several innings. Subluxation of the ulnar nerve and triceps tendon subluxation present as a painful snapping over the medial aspect of the elbow.**
**REFERENCES: Williams RJ III, Urquhart ER, Altchek DW: Medial collateral ligament tears in the throwing athlete. Instr Course Lect 2004;53:579-586.**
**Cain EL Jr, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.**
**98****. A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
1- she can expect to have good pain relief following surgery.
2- active forward elevation and external rotation are reliably obtained postoperatively.
3- with her current anterosuperior escape, she is likely to have a poor surgical result.
4- postoperatively, significant muscular atrophy in the latissimus dorsi commonly occurs.
5- no advancement in glenohumeral arthritic changes should occur following surgery.
PREFERRED RESPONSE: 3**
**DISCUSSION: Latissimus dorsi tendon transfer is considered a surgical option for treatment in patients with chronic supraspinatus and infraspinatus tendon tears. Preoperative subscapularis function is necessary for good clinical results. Additionally, men with active elevation to shoulder level and active external rotation to 20 degrees have predictably good results. Women with active shoulder elevation limited to below chest level have poor results from this procedure and should not be considered candidates. Postoperatively they lack pain control, active elevation, and active external rotation. Muscular atrophy in the latissimus dorsi does not occur, and glenohumeral arthritic changes frequently develop postoperatively.**
**REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.**
**Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.**
**99****. A patient undergoes an arthroscopic debridement for lateral epicondylitis. Postoperatively she reports pain and a sense of clicking of the elbow. Examination reveals apprehension to supination, load, and extension. What structure has been injured resulting in the clinical presentation?
1- Medial collateral ligament
2- Annular ligament
3- Lateral ulnar collateral ligament
4- Extensor carpi radialis brevis
5- Extensor carpi radialis longus
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has an iatrogenic injury to the lateral ulnar collateral ligament following the arthroscopic procedure. Failure to adhere to known anatomic landmarks can lead to this devastating complication. The examination findings are classic for posterolateral elbow instability.**
**REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 318.**
**O’ Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.**
**100****. A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
1- Tenotomy with medial transfer
2- Tenotomy with soft-tissue tenodesis
3- Tenotomy with tenodesis using suture anchors
4- Tenotomy with tenodesis using bone tunnels
5- Tenotomy with tenodesis using an interference screw
PREFERRED RESPONSE: 5**
**DISCUSSION: Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown.**
**REFERENCES: Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.**
**Richards DP, Burkhart SS: A biomechanical analysis of two biceps tenodesis fixation techniques. Arthroscopy 2005;21:861-866.**
**101****. A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
1- Broad-spectrum parenteral antibiotics
2- Repeat aspirations
3- Irrigation and debridement
4- Hyperbaric oxygen
5- Resection of the sternoclavicular joint
PREFERRED RESPONSE: 5**
**DISCUSSION: Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.**
**REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.**
**102****. A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
1- Modified posterior approach with elevation of the medial and lateral heads of the triceps
2- Posterior triceps-splitting approach
3- Posterior triceps-splitting approach with radial nerve mobilization
4- Posteromedial approach
5- Lateral approach with radial nerve mobilization
PREFERRED RESPONSE: 1**
**DISCUSSION: The modified posterior approach with elevation of the medial and lateral heads of the triceps can provide exposure of 94% of the humeral shaft. The traditional posterior triceps-splitting approach exposes 55% of the humeral shaft.**
**REFERENCES: DeFranco MJ, Lawton JN: Radial nerve injuries associated with humeral fractures. J Hand Surg Am 2006;31:655-663.**
**Gerwin M, Hotchkiss RN, Weiland AJ: Alternative operative exposure of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am 1996;78:1690-1695.**
**103****. A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?
1- Axillary nerve palsy
2- Spinal accessory nerve palsy
3- Deltoid avulsion
4- Rotator cuff tear
5- Unreduced posterior glenohumeral dislocation
PREFERRED RESPONSE: 4**
**DISCUSSION: Patients older than age 40 years at the time of initial anterior dislocation have low rates of redislocation; however, 15% of these patients experience a rotator cuff tear. Moreover, there is a dramatic increase (up to 40%) in the incidence of rotator cuff tears in patients older than age 60 years. Axillary nerve injury may occur but is less common than rotator cuff tear.**
**REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 273-284.**
**Neviaser RJ, Neviaser TJ, Neviaser JS: Anterior dislocation of the shoulder and rotator cuff rupture. Clin Orthop Relat Res 1993;291:103-106.**
**104****. What is the most common complaint in patients with a developmental radial head dislocation?
1- Pain
2- Recurrent elbow subluxation
3- Limitation of extension
4- Cosmetic deformity
5- Locking
PREFERRED RESPONSE: 4**
**DISCUSSION: Developmental dislocation of the radial head most frequently presents as a painless mass over the posterior aspect of the elbow. Patients do not have feelings of elbow subluxation but may report pain or clicking. Limitation of motion is most frequently found in the pronation and supination arc rather than in flexion and extension.**
**REFERENCES: Lloyd-Roberts GC, Bucknill TM: Anterior dislocation of the radial head in children-etiology: Natural history and management. J Bone Joint Surg Am 1977;58:402.**
**Hamilton W, Parks JC II: Isolated dislocation of the radial head without fracture of the ulna. Clin Orthop Relat Res 1973;97:94-96.**
**105****. Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
1- A curve-backed pegged cemented polyethylene glenoid component
2- A curve-backed keeled cemented polyethylene glenoid component design
3- A flat-backed keeled cemented polyethylene glenoid component
4- An oversized pegged cemented glenoid component
5- A superiorly placed pegged glenoid component
PREFERRED RESPONSE: 1**
**DISCUSSION: According to a recent study, cemented pegged glenoid components had fewer radiolucent lines initially and at 2-year follow-up when compared to a cemented keeled design. Curve-backed designs have also shown fewer radiolucent lines when compared to flat-backed designs. Oversizing the glenoid can lead to impaired rotator cuff function and decreased range of motion. An off-centered glenoid can lead to early loosening.**
**REFERENCES: Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257.**
**Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.**
**Mileti J, Boardman ND III, Sperling JW, et al: Radiographic analysis of polyethylene glenoid components using modern cementing techniques. J Shoulder Elbow Surg 2004;13:492-498.**
**106****. What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
1- Ulnar nerve
2- Radial nerve
3- Posterior interosseous nerve
4- Superficial radial nerve
5- Median nerve
PREFERRED RESPONSE: 2**
**DISCUSSION: The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region.**
**REFERENCES: Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.**
**Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.**
**107****. Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
1- Unlinked elbow arthroplasty
2- Linked elbow arthroplasty
3- Interposition arthroplasty
4- Arthroscopic or open debridement
5- Radial head excision
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has symptomatic primary osteoarthritis of the elbow with multiple loose bodies. Given his age and occupation, an elbow arthroplasty is not an option. Arthroscopic debridement and removal of loose bodies has been shown to be effective for osteoarthritis of the elbow.**
**REFERENCES: Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.**
**Steinmann SP, King GJ, Savoie FH III, et al: Arthroscopic treatment of the arthritic elbow.
J Bone Joint Surg Am 2005;87:2114-2121.**
**108****. A 35-year-old man sustained the closed injury shown in Figure 52 in his dominant extremity. Neurologic function is normal. Treatment should consist of
1- functional bracing.
2- a sling and swathe.
3- intramedullary nail fixation.
4- open reduction and internal fixation.
5- iliac crest bone graft.
PREFERRED RESPONSE: 1**
**DISCUSSION: Functional bracing has been demonstrated to have a very high rate of healing without any functional limitations in a large series of patients. Surgery is reserved for “floating elbows,” open injuries, neurovascular injuries, and those fractures that go on to nonunion.**
**REFERENCES: Sarmiento A, Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-486.**
**Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 267.**
**109****. A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?
1- Arthroscopic removal of osteophytes and soft-tissue release
2- Soft-tissue interpositional arthroplasty
3- Reverse total shoulder arthroplasty
4- Hemiarthroplasty
5- Total shoulder arthroplasty
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has end-stage shoulder arthritis with posterior glenoid erosion and large humeral osteophyte formation. Since the rotator cuff is likely intact, the reverse total shoulder arthroplasty is unnecessary. All the remaining procedures may provide symptomatic relief in appropriate patients; however, for most patients, total shoulder arthroplasty has been associated with the most predictive pain relief and functional improvements.**
**REFERENCES: Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systemic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956.**
**Edwards TB, Kadakia NR, Boulahia A, et al: A comparison of hemiarthroplasty and total shoulder arthroplasty in the treatment of primary glenohumeral osteoarthritis: Results of a multicenter study. J Shoulder Elbow Surg 2003;12:207-213.**
**Gartsman GM, Roddey TS, Hammerman SM: Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. J Bone Joint Surg Am 2000;82:26-34.**
**110****. The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
1- Compression plate
2- Tension band plate
3- Bridge plate
4- Buttress plate
5- Spring plate
PREFERRED RESPONSE: 3**
**DISCUSSION: There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.**
**REFERENCE: Ruedi T, Murphy WM (eds): AO Principles of Fracture Management. New York, NY, Thieme, 2000, p 221.**
**111****. Which of the following antibiotics is contraindicated in children?
1- Penicillin
2- Cephalexin
3- Tetracycline
4- Erythromycin
5- Ampicillin
PREFERRED RESPONSE: 3**
**DISCUSSION: The tetracycline family of medications can stain teeth and bone in skeletally immature patients and as a result should be avoided in those patients. The remaining antibiotics have no known specific contraindication to use in children.**
**REFERENCE: Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.**
**112****. Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
1- Prior shoulder surgery
2- History of deep venous thrombosis
3- Controlled seizure disorder
4- Respiratory insufficiency
5- Obesity
PREFERRED RESPONSE: 4**
**DISCUSSION: A common side effect of interscalene nerve block for shoulder surgery is the blockade of the ipsilateral phrenic nerve. This, in turn, results in paresis of the diaphragm and up to a 30% reduction in pulmonary function volumes. Therefore, interscalene nerve block generally is not recommended for patients whose respiratory function is compromised. Other relative and absolute contraindications for interscalene nerve blocks include allergy to local anesthetics, infection at the injection site, uncontrolled seizure disorder, coagulation abnormality, and preexisting neurologic injury.**
**REFERENCES: Chelly JE: Indications for upper extremity blocks, in Chelly JE (ed): Peripheral Nerve Blocks, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 19-27.**
**Misamore GW, Sallay PI: A prospective analysis of the safety and efficacy of interscalene brachial plexus block anesthesia for shoulder surgery. J Shoulder Elbow Surg 2007;16:e39.**
Question 30High Yield
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure

Explanation
■
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
Question 31High Yield
During open reduction and internal fixation of a both bone forearm fracture, restoration of the radial bow has been most associated with which of the following?
Explanation
Restoration of the anatomy of the radial bow directly correlates with the range of motion postoperatively (pronation-supination).
The referenced study by Schemitsch et al found that restoration of the normal radial bow was related to the functional outcome. A good functional result
(more than 80 percent of normal rotation of the forearm) was associated with restoration of the normal amount and location of the radial bow. Similarly, the recovery of grip strength was associated with restoration of the location of the radial bow toward normal.
The referenced study by Schemitsch et al found that restoration of the normal radial bow was related to the functional outcome. A good functional result
(more than 80 percent of normal rotation of the forearm) was associated with restoration of the normal amount and location of the radial bow. Similarly, the recovery of grip strength was associated with restoration of the location of the radial bow toward normal.
Question 32High Yield
A 32-year-old football coach has had a 4-month history of increasing right wrist pain, particularly during blocking exercises, and he reports significant pain with range of motion and gripping activities. He denies any history of trauma. Examination reveals dorsal wrist tenderness and boggy fullness over the dorsum of the wrist. No erythema is noted. Grip strength is 60% compared with the opposite side. Radiographs are shown in Figures 5a and 5b. What is the most likely diagnosis?
Explanation
The patient has Kienbock’s disease (osteonecrosis of the lunate), which presents with boggy synovitis of the wrist, decreased range of motion, and often normal radiographs. The patient’s radiographs reveal small fragments from the lunate, with increased density in the lunate body. While a traumatic event may precede the patient’s pain, often an insidious increase in pain is found. Repetitive trauma has been suggested as a possible cause. This disease process is classically associated with an ulnar-negative variant. An MRI scan, revealing a low-intensity signal in the lunate, is the best diagnostic tool for early Kienbock’s disease.
REFERENCES: Green DP, Hotchkiss RN, Pederson WC: Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 837-848.
Gerwin M, Weiland AJ: Avascular necrosis of the carpals. Hand Clin 1993, p 761.
REFERENCES: Green DP, Hotchkiss RN, Pederson WC: Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 837-848.
Gerwin M, Weiland AJ: Avascular necrosis of the carpals. Hand Clin 1993, p 761.
Question 33High Yield
The newborn foot deformity seen in Figures 64a and 64b should initially treated with

Explanation
DISCUSSION: Mild to moderate metatarsus adductus is best treated with observation and possible passive stretching exercises because most of these feet will self correct. Numerous types of shoes, braces, and splints have been devised but the efficacy of these have not been determined. Serial casting is reserved for severe metatarsus adductus in the infant, although a medial surgical release may be indicated if the deformity is symptomatic and persists beyond age 4 years.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academ _A_ y _L-_ o _M_ f _ad_ O _en_ r _a_ th _C_ o _o_ p _p_ a _y_ edic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
2010 Pediatric Orthopaedic Examination Answer Book • 53
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
1. ##### Arthroscopy
2. ##### Antinuclear antibody
3. ##### MRI
4. ##### Bone scan
5. ##### HLA-B27 PREFERRED RESPONSE: 2
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American
College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love**l** and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa**l** ing. Prenatal and birth history are otherwise unremarkable. The child’s growth and
54 • American Academy of Orthopaedic Surgeons
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
1. ##### No treatment because internal tibial torsion slowly resolves on its own
2. ##### Immediate treatment with a Denis-Browne bar
3. ##### Distal tibial osteotomies
4. ##### Proximal femoral derotational osteotomies
5. ##### Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.
Figure 67
DISCUSSION: Mild to moderate metatarsus adductus is best treated with observation and possible passive stretching exercises because most of these feet will self correct. Numerous types of shoes, braces, and splints have been devised but the efficacy of these have not been determined. Serial casting is reserved for severe metatarsus adductus in the infant, although a medial surgical release may be indicated if the deformity is symptomatic and persists beyond age 4 years.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academ _A_ y _L-_ o _M_ f _ad_ O _en_ r _a_ th _C_ o _o_ p _p_ a _y_ edic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
2010 Pediatric Orthopaedic Examination Answer Book • 53
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
1. ##### Arthroscopy
2. ##### Antinuclear antibody
3. ##### MRI
4. ##### Bone scan
5. ##### HLA-B27 PREFERRED RESPONSE: 2
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American
College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love**l** and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa**l** ing. Prenatal and birth history are otherwise unremarkable. The child’s growth and
54 • American Academy of Orthopaedic Surgeons
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
1. ##### No treatment because internal tibial torsion slowly resolves on its own
2. ##### Immediate treatment with a Denis-Browne bar
3. ##### Distal tibial osteotomies
4. ##### Proximal femoral derotational osteotomies
5. ##### Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.
Figure 67
Question 34High Yield
Following surgical stabilization and fixation of the distal fibula, what is the most appropriate next step?
Explanation
- Perform a stress examination of the syndesmosis.
Question 35High Yield
A 65-year-old female sustains a fall onto her outstretched right hand. The injury is closed and she is neurovascularly intact. There is no median nerve paresthesias. Radiographs are shown in Figures A and B. What is the next best step in management of this patient?


Explanation
Based on the presentation and radiographic findings, the next best step is to place the patient into a rigid splint (ie. sugar tong) and have the patient followup in clinic. It is important to closely follow this patient, to assess the stability of the reduced fracture.
Distal radius fractures can be successfully managed when the articular surface has been appropriately reduced and when anatomic relationships have been restored. Indications for closed reduction and rigid immobilization include extra-articular fractures, fractures with less than 5 mm of radial shortening,
and fractures with dorsal angulation of less than 5 degrees. Based on the AAOS Clinical Practice Guidelines, this fracture does not meet criteria for operative intervention.
Lichtman et al. discuss the AAOS Clinical Practice Guidelines for managing distal radius fractures. There were only five moderate strength recommendations, which included: 1) surgical fixation for fractures that had a post-reduction radial shortening > 3 mm, dorsal tilt > 10 degrees and intraarticular step off > 2 mm, 2) rigid immobilization for non operative treatment,
3) use of a true lateral to assess the DRUJ, 4) beginning early range of motion of the wrist after stable fixation and 5) use vitamin C to help mitigate intractable pain.
LaFontaine et al. reviewed greater than 100 cases of consecutively treated distal radius fractures. Acute management involved reduction of the fracture and placement in to a plaster cast. Fractures that were more likely to displace were found to have 1) dorsal angulation of > 20 degrees, 2) comminution of the dorsal cortex, 3) intra-articular radiocarpal fractures, 4) an associated ulnar fracture or 5) age greater than 60 years of age. They recommend that patients with 3 or more of these factors should have closer radiologic follow up to guide definitive treatment.
Figures A and B demonstrate a non-displaced, extra-articular distal radius fracture. Because the fracture is appropriately aligned, the patient can be placed into a rigid splint.
Incorrect Answers
Answer 1: This patient does not have evidence of acute median nerve compression.
Answers 2, 5: Because the reduction is within the limits set forth by the AAOS guidelines, operative intervention is not warranted, even in the outpatient setting.
Answer 3: The guidelines indicate that rigid mobilization is warranted when treating distal fractures non-operatively.
Distal radius fractures can be successfully managed when the articular surface has been appropriately reduced and when anatomic relationships have been restored. Indications for closed reduction and rigid immobilization include extra-articular fractures, fractures with less than 5 mm of radial shortening,
and fractures with dorsal angulation of less than 5 degrees. Based on the AAOS Clinical Practice Guidelines, this fracture does not meet criteria for operative intervention.
Lichtman et al. discuss the AAOS Clinical Practice Guidelines for managing distal radius fractures. There were only five moderate strength recommendations, which included: 1) surgical fixation for fractures that had a post-reduction radial shortening > 3 mm, dorsal tilt > 10 degrees and intraarticular step off > 2 mm, 2) rigid immobilization for non operative treatment,
3) use of a true lateral to assess the DRUJ, 4) beginning early range of motion of the wrist after stable fixation and 5) use vitamin C to help mitigate intractable pain.
LaFontaine et al. reviewed greater than 100 cases of consecutively treated distal radius fractures. Acute management involved reduction of the fracture and placement in to a plaster cast. Fractures that were more likely to displace were found to have 1) dorsal angulation of > 20 degrees, 2) comminution of the dorsal cortex, 3) intra-articular radiocarpal fractures, 4) an associated ulnar fracture or 5) age greater than 60 years of age. They recommend that patients with 3 or more of these factors should have closer radiologic follow up to guide definitive treatment.
Figures A and B demonstrate a non-displaced, extra-articular distal radius fracture. Because the fracture is appropriately aligned, the patient can be placed into a rigid splint.
Incorrect Answers
Answer 1: This patient does not have evidence of acute median nerve compression.
Answers 2, 5: Because the reduction is within the limits set forth by the AAOS guidelines, operative intervention is not warranted, even in the outpatient setting.
Answer 3: The guidelines indicate that rigid mobilization is warranted when treating distal fractures non-operatively.
Question 36High Yield
Figures 97a through 97d are the radiographs and MR images of a 21-year-old man with symptoms of a left medial thigh mass. Upon examination, you palpate a firm, fixed, deep, nontender mass of the medial proximal left thigh. No other masses are found during the examination. The patient fears metastatic disease. What is the risk for malignant transformation throughout this patient’s lifetime?


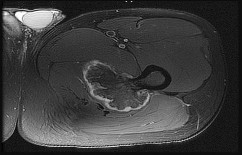
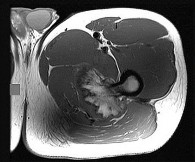
Explanation
The images reveal a solitary pedunculated osteochondroma. Malignant degeneration of solitary osteochondromas occurs in fewer than 1% of patients. A reasonable approach would be to inform the patient of the rare (less than 1%) incidence of malignant degeneration and to return for evaluation if symptoms develop or if the patient notices growth of the lesion.
RECOMMENDED READINGS
104. Schwartz AJ. Benign cartilage tumors. In: Biermann JS, ed. _Orthopaedic Knowledge Update Musculoskeletal Tumors 3_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013:97-106.
105. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926.](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
RECOMMENDED READINGS
104. Schwartz AJ. Benign cartilage tumors. In: Biermann JS, ed. _Orthopaedic Knowledge Update Musculoskeletal Tumors 3_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013:97-106.
105. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926.](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
Question 37High Yield
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 1 and

Explanation
■
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis. The cord compression is noted to be not only at the disk levels but also at the midvertebral body levels, and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1C2 on flexion-extension radiographs and subaxial subluxations.
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis. The cord compression is noted to be not only at the disk levels but also at the midvertebral body levels, and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1C2 on flexion-extension radiographs and subaxial subluxations.
Question 38High Yield
Intraarticular fracture fragments should be removed from the joint, but if they make up a substantial portion of the joint surface, they should be incorporated in the fixation construct to obtain the goal of anatomic reduction of the joint surface
What is the most appropriate next step in management?
What is the most appropriate next step in management?




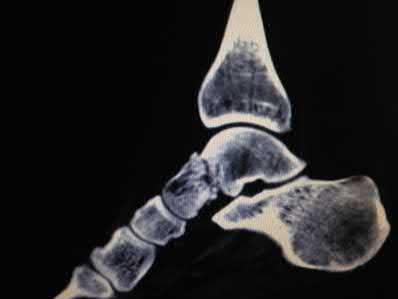






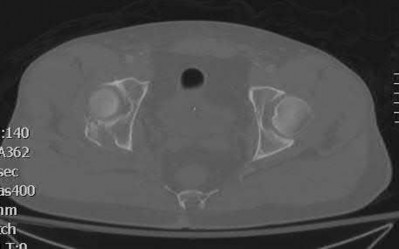











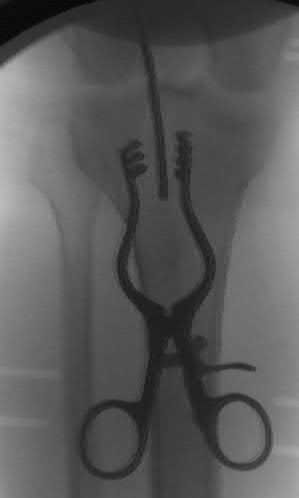
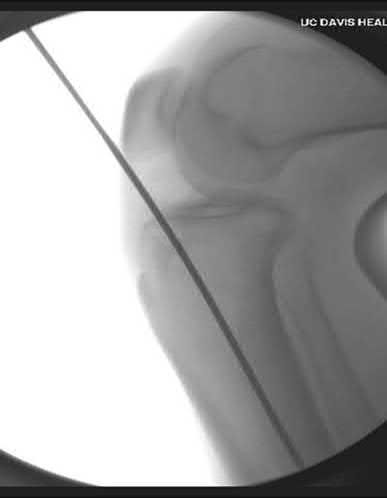
Explanation
This patient has a large posterior wall fracture of the right acetabulum with an unstable hip. The most appropriate next step in treatment is open reduction and internal fixation.
Fixation of acetabular fractures during pregnancy is not contraindicated in the setting of stable fetal heart rate and no abnormalities on pelvic ultrasound.
There is, however, an increased risk of complications for the mother and fetus. Injury severity and mechanism are most closely associated with increased rate of fetal complications. The trimester of pregnancy is not associated with increased risk of complications.
Leggon et al. reviewed 101 cases of pelvic and acetabular fractures in pregnant patients and found mechanism of injury and injury severity were associated with higher mortality for both mother and fetus. Trimester of pregnancy was not associated with increased mortality.
Flik et al. reviewed orthopaedic trauma in a pregnant patients and recommended fetal ultrasound for assessment of fetal well-being in all pregnant patients.
Desai et al. investigated orthopaedic trauma during pregnancy and reported minimal radiation risk to the fetus when obtaining x-rays. They also advocate for LMWH as one of the safest choices for anticoagulation.
Figure A is an x-ray showing a right posterior wall acetabular fracture. Figures B and C are Judet views of the pelvis focusing on the right hip. A large posterior wall fragment is visible in Figure B.
Incorrect Answers:
,3,5: ORIF is the most appropriate treatment for this posterior wall fracture. There is no contraindication to ORIF.
Answer 4: There is no indication to delay treatment as the fetal heart rate is normal and ultrasound shows no abnormalities.
Figure A is radiograph of a 50-year-old male science teacher that was involved in a motor vehicle accident. He underwent closed reduction as seen in Figure B and C. What would be the most appropriate treatment?
1) Open reduction and internal fixation with medial bridge plate and lateral screw in non-lagging mode
2) Tibiotalocalcaneal arthrodesis
3) Open reduction and internal fixation with lateral and medial screw in lagging mode
4) Closed reduction and internal fixation with medial and lateral screw in non-lagging mode
5) Closed reduction with percutaneous pins
This patient is presenting with a Hawkins II talar neck fracture with medial wall comminution. The most appropriate treatment of this patient would be open reduction internal fixation with medial plate and lateral screw in non-lagging mode.
The treatment of talar fractures is based on the severity of the fracture, soft-tissues, and patient factors. The fracture and subluxation of the subtalar joint should be reduced and stable anatomical fixation should be obtained. When there is comminution of either the superior, lateral or medial aspects of the talus, one should avoid shortening the medial wall as this will cause a varus malunion. The use of a medial or lateral plate can help to re-establish column length, which can often prevent this potential complication.
Sanders et al. showed significant complications after fixation of talar neck fractures. They showed the incidence of secondary reconstructive procedures following talar neck fractures increased from 24% +/- 5% at 1 year to 48%
+/- 10% at 10 years post-injury.
Vallier et al. retrospectively reviewed the records of 39 fractures of the talar neck treated with open reduction and internal fixation. Twenty-one (54%) of thirty-nine patients had development of posttraumatic arthritis, which was more common after comminuted fractures (p
A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?
1) Age less than 30
2) Marijuana use
3) Use of negative pressure wound therapy
4) Male gender
5) Ability to return to work
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
1-4: These options are not as strong of a factor of patient satisfaction in longterm follow up after trauma-induced lower extremity amputation.
A 34 year-old male falls off of motorcycle on an outstretched hand suffering the injuries shown in Figures A and B. He is brought to the operating room and undergoes radial head replacement and fixation and repair of the coronoid and the lateral collateral ligament (LCL). Prior to closing, the elbow is still unstable upon testing range of motion. What is the next best step in management?
1) Exchange radial head for larger implant
2) Complete resection of radial head
3) Cast at 90 degrees of flexion for 6-8 weeks
4) Reinforce LCL repair with non-absorbable suture
5) Repair the ulnar collateral ligament
Following complete fixation and repair of a terrible triad, a final range of motion test should be performed prior to closure. If still unstable, the next step should be to assess and repair the ulnar collateral ligament. Another option
would be to placed a hinged external fixator.
Operative reconstruction of a terrible triad injury should be performed in a systematic fashion, working from deep to superficial. Working through a lateral incision and through the radial head fracture, the coronoid should be fixed first, followed by radial head fixation or replacement and then repair/reconstruction of the LCL. If still unstable, the medial side should be addressed, or the patient placed in a hinged external fixator.
Mathew et al review the anatomic, biomechanic, and operative principles (why the above step-by-step method works) to achieving appropriate stability in order to obtain early range of motion to maximize clinical outcome.
Pugh et al. in this retrospective, multi-center study report outcomes on 36 terrible triad injuries fixed with the standard protocol described above. The authors recommend following this systematic approach to achieve the best results.
Figures A and B are AP and lateral radiographs exhibiting a terrible triad elbow fracture-dislocation.
Incorrect answers:
Answer 1. Overstuffing the radial head should be avoided.
Answer 2. Resection of the radial head is contraindicated in an unstable elbow. Answer 3. While casting the extremity may provide initial immobilization, you are unable to monitor the wound and truly assess stability, especially when swelling subsides.
Answer 4. Reinforcing the LCL will not make increase any stability not already achieved.
When treating the pathology depicted in Figures A through D, which of the following is necessary to preserve the blood supply to the femoral head?
1) Dissection of the gluteal musculature off the iliac crest
2) Ligation of the ascending branches of the lateral femoral circumflex artery
3) Greater trochanteric osteotomy
4) Identification and detachment of the piriformis tendon
5) Supine positioning
Figures A-D show a femoral head with associated acetabular fracture (Pipkin IV). Both the posterior wall fracture and the femoral head fracture can be addressed through a surgical dislocation via greater trochanteric osteotomy.
Pipkin IV femoral head fracture (with associated acetabular fractures) are somewhat problematic in that the femoral head fracture is usually anterior, while the acetabular fracture usually involves the posterior wall. A Kocher-Langenbeck approach gives good access to the posterior wall but limited access to the articular surface and femoral head avascular necrosis (AVN) is a concern. A Smith-Peterson approach provides good access to the femoral head
but not to the posterior wall. Combined approaches significantly increase the amount of surgical dissection. Surgical dislocation with trochanteric flip osteotomy provides access to the femoral head and posterior wall while preserving blood supply to the femoral head.
Solberg et al. retrospectively reviewed 12 patients with Pipkin IV injuries treated via a trochanteric flip osteotomy. All patients healed their acetabular fractures. Eleven of 12 patients healed their femoral head fractures and one patient (8.3%) developed osteonecrosis.
Henle et al. likewise treated 12 patients with Pipkin IV injuries through a trochanteric flip osteotomy. Two of 12 patients (16.7%) developed osteonecrosis. The remaining 10 patients (83.3%) had good or excellent results. Heterotopic ossification occurred in five patients, causing significant range of motion loss in four of these.
Figure A is a pre-reduction AP pelvis in which the posterior wall fracture is apparent. Figure B is a post-reduction AP pelvis in which an infra-foveal femoral head fracture is apparent (Pipkin IV). Figure C is an axial CT cut which further characterizes the posterior wall fracture. Figure D is an obturator oblique showing femoral head dislocation and posterior wall fracture. The video shows a surgical hip dislocation technique.
Incorrect Answers:
Answer 1: The extended iliofemoral approach exposes the entire innominate bone, which is not necessary to treat this injury.
Answer 2: The Smith-Peterson anterior approach provides access to the anterior femoral head but not the posterior wall of the acetabulum.
Answer 4: Detachment of the short external rotators is not necessary for surgical dislocation.
Answer 5: Surgical dislocation with greater trochanteric osteotomy is described in the lateral position. Supine positioning is not necessary.
A 42-year-old male presents to your clinic for the first time with the radiographs seen in Figure A. He sustained the injury 4 weeks ago while skiing overseas and treatment was provided by the local orthopaedic surgeon. The operative note states that he sustained an Gustilo Type I open fracture. After surgical fixation of this type of injury, what is the most common complication requiring reoperation?
1) Chronic elbow instability
2) Post-traumatic arthritis
3) Infection
4) Heterotopic ossification
5) Loss of elbow range of motion
This patient sustained a terrible triad elbow fracture-dislocation. Reduced range of motion of the elbow joint is the most common complication REQUIRING reoperation with these injuries.
Terrible triad elbow fracture-dislocations are characterized by posterolateral dislocation/lateral collateral ligament (LCL) injury, radial head fracture and coronoid fracture. Displaced fractures result in elbow instability. Acute radial head stabilization, coronoid open reduction and internal fixation, and LCL +/-medial collateral ligament (MCL) repair/reconstruction is considered the most appropriate treatment for displaced fractures. Operative complications include elbow stiffness, recurrent instability, arthritis, failure of hardware, heterotopic ossification, posterior interosseous nerve palsy and infection.
Egol et al. looked at the functional outcomes of 27 patients that underwent fixation of terrible triad injuries. At one year follow-up, the average flexion-extension arc of elbow motion was 109 degrees +/- 27 degrees, and the average pronation-supination arc was 128 degrees +/- 44 degrees. Grip strength averaged 72% of the contralateral extremity. Although operative fixation led to functional elbow stability, results were poor.
They included a reference to McKee et al. to highlight that intra-articular fractures of the elbow have high rates of stiffness. While not specific to terrible
triads, they looked at the effectiveness of the posterior elbow approach in 25 patients that underwent internal fixation of intra-articular distal humerus fractures. They showed poor outcomes at a mean follow-up of 36 months with reduced range-of-motion, decreased strength and high re-operation rates.
Figure A shows AP fluoroscopic image of a terrible triad injury that has undergone operative fixation. The radial head and coronoid have undergone open reduction internal fixation, and the MCL bony avulsion has been repaired.
Incorrect Answers:
Answer 1: Chronic elbow instability is more common following type I or II coronoid fracture when not operatively managed.
Answer 2: Post-traumatic arthritis results from chondral damage at time of injury and/or residual instability.
Answer 3: Infection is more prevalent with open fractures, however Type I injuries are usually not associated with increase in infection rates.
Answer 4: Heterotopic ossification is a common complication after fixation of these injuries. However, it does not always necessitate reoperation.
Figure A is a radiograph from a 59-year-old male that was transferred to a Level I trauma center five hours after a motor vehicle accident. Closed reduction and skeletal traction was successfully performed in the trauma bay. Which of the following factors has been shown to increase the risk of unsatisfactory clinical outcome for this patient?
1) Need for skeletal traction
2) Mechanism of injury
3) Gender
4) Age
5) Time to reduction
Age greater than 55-years-old has been found to be an independent risk factor for inferior clinical outcome in patients with combined acetabular fractures and hip dislocations.
The most important initial step in management following resuscitation involves urgent reduction of the dislocated hip. This should be followed by a preoperative CT scan and ultimately surgical fixation of the combined acetabular fracture. Hip dislocations should be reduced within 6-12 hours for optimal outcome, although different critical times have been cited, particularly for dislocations with concomitant acetabular fractures. Skeletal traction may be required to maintain hip reduction.
Moed et. al. present a Level 3 retrospective review of 100 patients who had been treated with open reduction internal fixation of an acetabular fracture. The authors found that factors associated with unsatisfactory clinical outcomes included age greater than 55, intra-articular comminution, osteonecrosis, and delay of greater than 12 hours for reduction of an associated hip dislocation.
Additionally, they showed that there was a strong association of clinical outcome and final radiographic grade.
Figure A demonstrates an acetabular fracture with concomitant hip dislocation. Incorrect Answers:
Answer 1-3, and 5: Placement and need for skeletal traction, mechanism of
injury, male gender, and time to reduction
A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?
1) Varus malunion
2) Nonunion
3) Valgus malunion
4) Malrotation
5) Superficial peroneal nerve injury
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Fixation of acetabular fractures during pregnancy is not contraindicated in the setting of stable fetal heart rate and no abnormalities on pelvic ultrasound.
There is, however, an increased risk of complications for the mother and fetus. Injury severity and mechanism are most closely associated with increased rate of fetal complications. The trimester of pregnancy is not associated with increased risk of complications.
Leggon et al. reviewed 101 cases of pelvic and acetabular fractures in pregnant patients and found mechanism of injury and injury severity were associated with higher mortality for both mother and fetus. Trimester of pregnancy was not associated with increased mortality.
Flik et al. reviewed orthopaedic trauma in a pregnant patients and recommended fetal ultrasound for assessment of fetal well-being in all pregnant patients.
Desai et al. investigated orthopaedic trauma during pregnancy and reported minimal radiation risk to the fetus when obtaining x-rays. They also advocate for LMWH as one of the safest choices for anticoagulation.
Figure A is an x-ray showing a right posterior wall acetabular fracture. Figures B and C are Judet views of the pelvis focusing on the right hip. A large posterior wall fragment is visible in Figure B.
Incorrect Answers:
,3,5: ORIF is the most appropriate treatment for this posterior wall fracture. There is no contraindication to ORIF.
Answer 4: There is no indication to delay treatment as the fetal heart rate is normal and ultrasound shows no abnormalities.
Figure A is radiograph of a 50-year-old male science teacher that was involved in a motor vehicle accident. He underwent closed reduction as seen in Figure B and C. What would be the most appropriate treatment?
1) Open reduction and internal fixation with medial bridge plate and lateral screw in non-lagging mode
2) Tibiotalocalcaneal arthrodesis
3) Open reduction and internal fixation with lateral and medial screw in lagging mode
4) Closed reduction and internal fixation with medial and lateral screw in non-lagging mode
5) Closed reduction with percutaneous pins
This patient is presenting with a Hawkins II talar neck fracture with medial wall comminution. The most appropriate treatment of this patient would be open reduction internal fixation with medial plate and lateral screw in non-lagging mode.
The treatment of talar fractures is based on the severity of the fracture, soft-tissues, and patient factors. The fracture and subluxation of the subtalar joint should be reduced and stable anatomical fixation should be obtained. When there is comminution of either the superior, lateral or medial aspects of the talus, one should avoid shortening the medial wall as this will cause a varus malunion. The use of a medial or lateral plate can help to re-establish column length, which can often prevent this potential complication.
Sanders et al. showed significant complications after fixation of talar neck fractures. They showed the incidence of secondary reconstructive procedures following talar neck fractures increased from 24% +/- 5% at 1 year to 48%
+/- 10% at 10 years post-injury.
Vallier et al. retrospectively reviewed the records of 39 fractures of the talar neck treated with open reduction and internal fixation. Twenty-one (54%) of thirty-nine patients had development of posttraumatic arthritis, which was more common after comminuted fractures (p
A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?
1) Age less than 30
2) Marijuana use
3) Use of negative pressure wound therapy
4) Male gender
5) Ability to return to work
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
1-4: These options are not as strong of a factor of patient satisfaction in longterm follow up after trauma-induced lower extremity amputation.
A 34 year-old male falls off of motorcycle on an outstretched hand suffering the injuries shown in Figures A and B. He is brought to the operating room and undergoes radial head replacement and fixation and repair of the coronoid and the lateral collateral ligament (LCL). Prior to closing, the elbow is still unstable upon testing range of motion. What is the next best step in management?
1) Exchange radial head for larger implant
2) Complete resection of radial head
3) Cast at 90 degrees of flexion for 6-8 weeks
4) Reinforce LCL repair with non-absorbable suture
5) Repair the ulnar collateral ligament
Following complete fixation and repair of a terrible triad, a final range of motion test should be performed prior to closure. If still unstable, the next step should be to assess and repair the ulnar collateral ligament. Another option
would be to placed a hinged external fixator.
Operative reconstruction of a terrible triad injury should be performed in a systematic fashion, working from deep to superficial. Working through a lateral incision and through the radial head fracture, the coronoid should be fixed first, followed by radial head fixation or replacement and then repair/reconstruction of the LCL. If still unstable, the medial side should be addressed, or the patient placed in a hinged external fixator.
Mathew et al review the anatomic, biomechanic, and operative principles (why the above step-by-step method works) to achieving appropriate stability in order to obtain early range of motion to maximize clinical outcome.
Pugh et al. in this retrospective, multi-center study report outcomes on 36 terrible triad injuries fixed with the standard protocol described above. The authors recommend following this systematic approach to achieve the best results.
Figures A and B are AP and lateral radiographs exhibiting a terrible triad elbow fracture-dislocation.
Incorrect answers:
Answer 1. Overstuffing the radial head should be avoided.
Answer 2. Resection of the radial head is contraindicated in an unstable elbow. Answer 3. While casting the extremity may provide initial immobilization, you are unable to monitor the wound and truly assess stability, especially when swelling subsides.
Answer 4. Reinforcing the LCL will not make increase any stability not already achieved.
When treating the pathology depicted in Figures A through D, which of the following is necessary to preserve the blood supply to the femoral head?
1) Dissection of the gluteal musculature off the iliac crest
2) Ligation of the ascending branches of the lateral femoral circumflex artery
3) Greater trochanteric osteotomy
4) Identification and detachment of the piriformis tendon
5) Supine positioning
Figures A-D show a femoral head with associated acetabular fracture (Pipkin IV). Both the posterior wall fracture and the femoral head fracture can be addressed through a surgical dislocation via greater trochanteric osteotomy.
Pipkin IV femoral head fracture (with associated acetabular fractures) are somewhat problematic in that the femoral head fracture is usually anterior, while the acetabular fracture usually involves the posterior wall. A Kocher-Langenbeck approach gives good access to the posterior wall but limited access to the articular surface and femoral head avascular necrosis (AVN) is a concern. A Smith-Peterson approach provides good access to the femoral head
but not to the posterior wall. Combined approaches significantly increase the amount of surgical dissection. Surgical dislocation with trochanteric flip osteotomy provides access to the femoral head and posterior wall while preserving blood supply to the femoral head.
Solberg et al. retrospectively reviewed 12 patients with Pipkin IV injuries treated via a trochanteric flip osteotomy. All patients healed their acetabular fractures. Eleven of 12 patients healed their femoral head fractures and one patient (8.3%) developed osteonecrosis.
Henle et al. likewise treated 12 patients with Pipkin IV injuries through a trochanteric flip osteotomy. Two of 12 patients (16.7%) developed osteonecrosis. The remaining 10 patients (83.3%) had good or excellent results. Heterotopic ossification occurred in five patients, causing significant range of motion loss in four of these.
Figure A is a pre-reduction AP pelvis in which the posterior wall fracture is apparent. Figure B is a post-reduction AP pelvis in which an infra-foveal femoral head fracture is apparent (Pipkin IV). Figure C is an axial CT cut which further characterizes the posterior wall fracture. Figure D is an obturator oblique showing femoral head dislocation and posterior wall fracture. The video shows a surgical hip dislocation technique.
Incorrect Answers:
Answer 1: The extended iliofemoral approach exposes the entire innominate bone, which is not necessary to treat this injury.
Answer 2: The Smith-Peterson anterior approach provides access to the anterior femoral head but not the posterior wall of the acetabulum.
Answer 4: Detachment of the short external rotators is not necessary for surgical dislocation.
Answer 5: Surgical dislocation with greater trochanteric osteotomy is described in the lateral position. Supine positioning is not necessary.
A 42-year-old male presents to your clinic for the first time with the radiographs seen in Figure A. He sustained the injury 4 weeks ago while skiing overseas and treatment was provided by the local orthopaedic surgeon. The operative note states that he sustained an Gustilo Type I open fracture. After surgical fixation of this type of injury, what is the most common complication requiring reoperation?
1) Chronic elbow instability
2) Post-traumatic arthritis
3) Infection
4) Heterotopic ossification
5) Loss of elbow range of motion
This patient sustained a terrible triad elbow fracture-dislocation. Reduced range of motion of the elbow joint is the most common complication REQUIRING reoperation with these injuries.
Terrible triad elbow fracture-dislocations are characterized by posterolateral dislocation/lateral collateral ligament (LCL) injury, radial head fracture and coronoid fracture. Displaced fractures result in elbow instability. Acute radial head stabilization, coronoid open reduction and internal fixation, and LCL +/-medial collateral ligament (MCL) repair/reconstruction is considered the most appropriate treatment for displaced fractures. Operative complications include elbow stiffness, recurrent instability, arthritis, failure of hardware, heterotopic ossification, posterior interosseous nerve palsy and infection.
Egol et al. looked at the functional outcomes of 27 patients that underwent fixation of terrible triad injuries. At one year follow-up, the average flexion-extension arc of elbow motion was 109 degrees +/- 27 degrees, and the average pronation-supination arc was 128 degrees +/- 44 degrees. Grip strength averaged 72% of the contralateral extremity. Although operative fixation led to functional elbow stability, results were poor.
They included a reference to McKee et al. to highlight that intra-articular fractures of the elbow have high rates of stiffness. While not specific to terrible
triads, they looked at the effectiveness of the posterior elbow approach in 25 patients that underwent internal fixation of intra-articular distal humerus fractures. They showed poor outcomes at a mean follow-up of 36 months with reduced range-of-motion, decreased strength and high re-operation rates.
Figure A shows AP fluoroscopic image of a terrible triad injury that has undergone operative fixation. The radial head and coronoid have undergone open reduction internal fixation, and the MCL bony avulsion has been repaired.
Incorrect Answers:
Answer 1: Chronic elbow instability is more common following type I or II coronoid fracture when not operatively managed.
Answer 2: Post-traumatic arthritis results from chondral damage at time of injury and/or residual instability.
Answer 3: Infection is more prevalent with open fractures, however Type I injuries are usually not associated with increase in infection rates.
Answer 4: Heterotopic ossification is a common complication after fixation of these injuries. However, it does not always necessitate reoperation.
Figure A is a radiograph from a 59-year-old male that was transferred to a Level I trauma center five hours after a motor vehicle accident. Closed reduction and skeletal traction was successfully performed in the trauma bay. Which of the following factors has been shown to increase the risk of unsatisfactory clinical outcome for this patient?
1) Need for skeletal traction
2) Mechanism of injury
3) Gender
4) Age
5) Time to reduction
Age greater than 55-years-old has been found to be an independent risk factor for inferior clinical outcome in patients with combined acetabular fractures and hip dislocations.
The most important initial step in management following resuscitation involves urgent reduction of the dislocated hip. This should be followed by a preoperative CT scan and ultimately surgical fixation of the combined acetabular fracture. Hip dislocations should be reduced within 6-12 hours for optimal outcome, although different critical times have been cited, particularly for dislocations with concomitant acetabular fractures. Skeletal traction may be required to maintain hip reduction.
Moed et. al. present a Level 3 retrospective review of 100 patients who had been treated with open reduction internal fixation of an acetabular fracture. The authors found that factors associated with unsatisfactory clinical outcomes included age greater than 55, intra-articular comminution, osteonecrosis, and delay of greater than 12 hours for reduction of an associated hip dislocation.
Additionally, they showed that there was a strong association of clinical outcome and final radiographic grade.
Figure A demonstrates an acetabular fracture with concomitant hip dislocation. Incorrect Answers:
Answer 1-3, and 5: Placement and need for skeletal traction, mechanism of
injury, male gender, and time to reduction
A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?
1) Varus malunion
2) Nonunion
3) Valgus malunion
4) Malrotation
5) Superficial peroneal nerve injury
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Question 39High Yield
Which intervention most effectively prevents surgical-site infections following spine surgery?
Explanation
The use of IV antibiotics for prophylaxis of surgical-site infection is supported by Level 1 evidence in spine surgery. It has been given a "B" recommendation by the North American Spine Society. The use of specific bathing solutions the day of surgery may be beneficial, but the evidence in spine surgery is lacking. Similarly, evidence for use of vancomycin (either topically or IV) is not supported by high-level studies, although retrospective and basic science studies support topical vancomycin use.
RECOMMENDED READINGS
[Brown MD, Brookfield KF. A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine (Phila Pa 1976). 2004 May 15;29(10):1066-8. PubMed PMID: 15131430. ](http://www.ncbi.nlm.nih.gov/pubmed/15131430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15131430)
Diab M, Smucny M, Dormans JP, Erickson MA, Ibrahim K, Lenke LG, Sucato DJ, Sanders JO. Use and outcomes of wound drain in spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012 May 15;37(11):966-73. doi: 10.1097/BRS.0b013e31823bbf0b.
[PubMed PMID: 22037527. ](http://www.ncbi.nlm.nih.gov/pubmed/22037527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22037527)
[Evaniew N, Khan M, Drew B, Peterson D, Bhandari M, Ghert M. Intrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysis. Eur Spine J. 2014 May 18. [Epub ahead of print] PubMed PMID: 24838506. ](http://www.ncbi.nlm.nih.gov/pubmed/24838506)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24838506) Rubinstein E, Findler G, Amit P, Shaked I. Perioperative prophylactic cephazolin in spinal surgery. A double-blind placebo-controlled trial. J Bone Joint Surg Br. 1994 Jan;76(1):99-
[102/. PubMed PMID: 8300691. ](http://www.ncbi.nlm.nih.gov/pubmed/8300691)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8300691)
[Savage JW, Anderson PA. An update on modifiable factors to reduce the risk of surgical site infections. Spine J. 2013 Sep;13(9):1017-29. doi:10.1016/j.spinee.2013.03.051. Epub 2013 May 24. Review. PubMed PMID: 23711958. ](http://www.ncbi.nlm.nih.gov/pubmed/23711958)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23711958)
[Shaffer WO, Baisden JL, Fernand R, Matz PG; North American Spine Society. An evidence-based clinical guideline for antibiotic prophylaxis in spine surgery. Spine J. 2013 Oct;13(10):1387-92. doi: 10.1016/j.spinee.2013.06.030. Epub 2013 Aug 27. Review. PubMed PMID: 23988461. ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23988461)
RECOMMENDED READINGS
[Brown MD, Brookfield KF. A randomized study of closed wound suction drainage for extensive lumbar spine surgery. Spine (Phila Pa 1976). 2004 May 15;29(10):1066-8. PubMed PMID: 15131430. ](http://www.ncbi.nlm.nih.gov/pubmed/15131430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15131430)
Diab M, Smucny M, Dormans JP, Erickson MA, Ibrahim K, Lenke LG, Sucato DJ, Sanders JO. Use and outcomes of wound drain in spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2012 May 15;37(11):966-73. doi: 10.1097/BRS.0b013e31823bbf0b.
[PubMed PMID: 22037527. ](http://www.ncbi.nlm.nih.gov/pubmed/22037527)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22037527)
[Evaniew N, Khan M, Drew B, Peterson D, Bhandari M, Ghert M. Intrawound vancomycin to prevent infections after spine surgery: a systematic review and meta-analysis. Eur Spine J. 2014 May 18. [Epub ahead of print] PubMed PMID: 24838506. ](http://www.ncbi.nlm.nih.gov/pubmed/24838506)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24838506) Rubinstein E, Findler G, Amit P, Shaked I. Perioperative prophylactic cephazolin in spinal surgery. A double-blind placebo-controlled trial. J Bone Joint Surg Br. 1994 Jan;76(1):99-
[102/. PubMed PMID: 8300691. ](http://www.ncbi.nlm.nih.gov/pubmed/8300691)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8300691)
[Savage JW, Anderson PA. An update on modifiable factors to reduce the risk of surgical site infections. Spine J. 2013 Sep;13(9):1017-29. doi:10.1016/j.spinee.2013.03.051. Epub 2013 May 24. Review. PubMed PMID: 23711958. ](http://www.ncbi.nlm.nih.gov/pubmed/23711958)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23711958)
[Shaffer WO, Baisden JL, Fernand R, Matz PG; North American Spine Society. An evidence-based clinical guideline for antibiotic prophylaxis in spine surgery. Spine J. 2013 Oct;13(10):1387-92. doi: 10.1016/j.spinee.2013.06.030. Epub 2013 Aug 27. Review. PubMed PMID: 23988461. ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23988461)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23988461)
Question 40High Yield
Slide 1
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
Explanation
A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
Question 41High Yield
Figures 1 and 2 are the radiographs of a 6-year-old boy who came to the emergency department with a twisting injury to the right leg sustained while skiing. He is nonweightbearing, has no pain with passive motion of his ankle and toes, and remains neurovascularly intact. What is the most appropriate next step in the management of his injury?

Explanation
■
The images demonstrate a mildly displaced tibial shaft fracture that meets criteria for nonoperative management. At his age, these parameters are typically fracture shortening <1cm, coronal angulation <10°, sagittal angulation <15°, and rotation <10°. Options for operative management should be reserved for injuries that fail nonoperative treatment, open fractures, and potentially fractures with initial shortening >2 cm. Having an intact fibula is a relative indication for surgery; however, recent studies show no difference in operative and nonoperative treatment for this pattern.
■
The images demonstrate a mildly displaced tibial shaft fracture that meets criteria for nonoperative management. At his age, these parameters are typically fracture shortening <1cm, coronal angulation <10°, sagittal angulation <15°, and rotation <10°. Options for operative management should be reserved for injuries that fail nonoperative treatment, open fractures, and potentially fractures with initial shortening >2 cm. Having an intact fibula is a relative indication for surgery; however, recent studies show no difference in operative and nonoperative treatment for this pattern.
Question 42High Yield
A 72-year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph
is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg
length, what is the most appropriate surgical plan?
is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg
length, what is the most appropriate surgical plan?

Explanation
---
DISCUSSION:
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
DISCUSSION:
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 43High Yield
The anterior approach to the hip (iliofemoral or Smith-Peterson) puts which of the following anatomic structures at greatest risk?
Explanation
DISCUSSION: The anterior approach to the hip involves a dissection between the sartorius and the tensor fascia lata (TFL) superficially, followed by a deep dissection between the rectus femoris and gluteus medius. The lateral femoral cutaneous nerve generally enters the top of the thigh overlying the sartorius, and then usually crosses the interval between the sartorius muscle and the tensor fascia lata more distally. As the fascia between the sartorius and the TFL is incised, the nerve is at risk. The ascending branch of the lateral femoral circumflex artery is also at risk during this approach. The femoral nerve should not be in the plane of dissection as it lies medial to the sartorius.
REFERENCE: Hoppenfeld S, DeBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippinocott, 1984, pp 301-315.
REFERENCE: Hoppenfeld S, DeBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippinocott, 1984, pp 301-315.
Question 44High Yield
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness.Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities.Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following?
Explanation
The MRI scan shows advanced multilevel degenerative changes and moderate to severe stenosis at C3-C4 and C4-C5 with associated cord signal change. The patient has greater weakness in the upper extremities than in the lower extremities. This pattern is most compatible with central cord syndrome. Patients with brachial plexus injury will have unilateral weakness. Patients with anterior cord syndrome will have greater weakness in the legs than in the arms, and those with Brown-Séquard syndrome will have ipsilateral motor deficits and contralateral pain and temperature deficits.
Question 45High Yield
A 5-year-old boy has had a limp for the past 4 weeks with intermittent pain at the foot. He remains normally active and has no history of trauma. He has no fevers, rashes, or swelling. Examination reveals tenderness at the mid-dorsum of the foot medially. Radiographs are seen in Figures la and lb. Treatment should include which of the following?

Explanation
DISCUSSION: Osteochondrosis of the tarsal navicular is most commonly identified between the ages of 2 and 9 years. The condition is benign and self limited in nature. In patients with severe pain, a period of casting may be warranted, but otherwise management usually consists of observation or a supportive orthotic.
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
Question 46High Yield
Advanced imaging, to include MRI and CT, have been obtained in the workup of patients with low back pain. What imaging finding has been associated with reasons for back pain?
Explanation
■
Low back pain remains a common presenting condition to not only primary care physicians, but to subspecialists. Studies assessing the anatomy of the spine, to include the intervertebral disks, vertebral body morphology, facet joints, and the paraspinal muscles have been performed. Spinal stenosis is the only advanced imaging finding that has been associated with reproducible reasons for back pain.
Low back pain remains a common presenting condition to not only primary care physicians, but to subspecialists. Studies assessing the anatomy of the spine, to include the intervertebral disks, vertebral body morphology, facet joints, and the paraspinal muscles have been performed. Spinal stenosis is the only advanced imaging finding that has been associated with reproducible reasons for back pain.
Question 47High Yield
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
Explanation
DISCUSSION: Approximately 5% of female recruits incur a stress fracture during the 13 weeks of Marine Corps basic training. Approximately 40% of these were femoral or pelvic stress fractures that were more severe than in civilian athletes or male military recruits. Only women who reported no menses during the previous year had a greater likelihood of femoral or pelvic stress fractures than did women who reported 10 to
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
Question 48High Yield
In the arthroscopic photograph shown in Figure 5, the structure labeled “A” functions primarily as a restraint to translation of the humeral head in what direction?
Explanation
The superior glenohumeral ligament identified as “A” in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation.
REFERENCES: Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Owen MD, Kregel KC, Wall PT, Gisolfi CV: Effects of ingesting carbohydrate beverages during exercise in the heat. Med Sci Sports Exerc 1986;18:568-575.
REFERENCES: Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Owen MD, Kregel KC, Wall PT, Gisolfi CV: Effects of ingesting carbohydrate beverages during exercise in the heat. Med Sci Sports Exerc 1986;18:568-575.
Question 49High Yield
Scoliosis in Marfan syndrome, as compared to idiopathic scoliosis, is characterized by which of the following:
Explanation
Scoliosis curves are much more likely to begin in the juvenile period than idiopathic scoliosis.
There is no significant difference in the likelihood of left thoracic curves in Marfan syndrome. Brace treatment is less likely to be successful in Marfan syndrome than in idiopathic scoliosis. Marfan patients with scoliosis are more likely to have back pain.
Marfan curves are more likely to progress in adulthood.
There is no significant difference in the likelihood of left thoracic curves in Marfan syndrome. Brace treatment is less likely to be successful in Marfan syndrome than in idiopathic scoliosis. Marfan patients with scoliosis are more likely to have back pain.
Marfan curves are more likely to progress in adulthood.
Question 50High Yield
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of
Explanation
Throwers and in particular, pitchers, are prone to high valgus loads to the elbow. A constellation of medial elbow pathology can develop, including medial epicondylitis, ulnar nerve neuritis, medial ulnar collateral ligament injuries, and posteromedial osteophytes of the olecranon. The MRI scans show significant increases in signal intensing as well as fiber disruption of the medial collateral ligament, indicating a complete tear. The common flexor origin shows a homogeneous signal and normal morphology. Therefore, excision of posterior osteophytes and debridement of the common flexor origin are not indicated. Likewise, this patient’s symptoms do not indicate ulnar nerve pathology; therefore ulnar nerve transposition is not indicated. Primary repair of medial collateral ligament tears of the elbow lead to unpredictable results with an unacceptable rate of reoperation. The most predictable result in treating this high-demand athlete is reconstruction of the medial collateral ligament with autogenous tissue.
REFERENCES: Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
Hyman J, Breazeale NM, Altchek DW: Valgus instability of the elbow in athletes. Clin Sports Med 2001;20:11-24.
REFERENCES: Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
Hyman J, Breazeale NM, Altchek DW: Valgus instability of the elbow in athletes. Clin Sports Med 2001;20:11-24.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon