Orthopedic Reconstructi Review | Dr Hutaif Hip & Knee R -...
14 Apr 2026
48 min read
89 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Reconstructi Review | Dr Hutaif Hi...
00:00
Start Quiz
Question 1High Yield
What is the most appropriate orthosis for hallux rigidus?
Explanation
A Morton’s extension limits excursion of the first metatarsophalangeal joint. It also functions as a ground reaction stabilizer during the toe-off phase of gait and thus reduces torque and joint reaction force at the first metatarsophalangeal joint. The metatarsal arch pad and full-length semi-rigid longitudinal arch support may help by dorsiflexing the first metatarsal relative to the phalanx and thus decompress the first metatarsophalangeal joint. However, they are not as biomechanically effective as the Morton’s extension. Both medial hindfoot and lateral forefoot posting are contraindicated because they increase ground reaction at the first metatarsophalangeal joint.
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Watson AD, Wapner KL: Foot and ankle reconstruction, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, p 635.
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Watson AD, Wapner KL: Foot and ankle reconstruction, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, p 635.
Question 2High Yield
Placing a plate too anteriorly against the lateral aspect of the bicipital groove while performing open reduction and internal fixation (ORIF) of a proximal humerus fracture has an increased risk of what complication?
Explanation
DISCUSSION
There are two major arteries that supply the humeral head. One is the ascending branch of the anterior humeral circumflex artery, which runs up the lateral aspect of the bicipital groove terminating in the arcuate artery. The other is the posterior humeral circumflex artery, which more recently has been demonstrated to supply a significant portion of the blood supply to the humeral head. Capsular arteries also play a role in humeral head perfusion. Care should be taken to preserve all intact arterial supply when performing ORIF, as injury to these arteries may result in avascular necrosis. In general, the most common complications of locked plating include loss of reduction with penetration of the joint by the screws, particularly with initial varus positioning of the humeral head. Placement of the plate in the position described, however, should not have an impact on any of
the other complications noted.
DISCUSSION
There are two major arteries that supply the humeral head. One is the ascending branch of the anterior humeral circumflex artery, which runs up the lateral aspect of the bicipital groove terminating in the arcuate artery. The other is the posterior humeral circumflex artery, which more recently has been demonstrated to supply a significant portion of the blood supply to the humeral head. Capsular arteries also play a role in humeral head perfusion. Care should be taken to preserve all intact arterial supply when performing ORIF, as injury to these arteries may result in avascular necrosis. In general, the most common complications of locked plating include loss of reduction with penetration of the joint by the screws, particularly with initial varus positioning of the humeral head. Placement of the plate in the position described, however, should not have an impact on any of
the other complications noted.
Question 3High Yield
A 45-year-old man presents to your clinic with a closed mid-shaft humerus fracture after a fall 1 week prior. He is neurovascularly intact. After a discussion of his treatment options, he is adamant about proceeding with surgical management. With respect to open reduction and internal fixation with a plate versus intramedullary nailing, what advice can you offer him?

Explanation
Current literature on the management of humeral shaft fractures shows no difference in the rate of radial nerve palsy between nailing (IMN) or with plate fixation (ORIF).
Both ORIF and IMN are appropriate means of definitive fixation of diaphyseal humeral fractures. Numerous studies have directly compared the risks and
outcomes associated with each of the two methods, and the current literature supports that there is no difference in the rates of fracture union, radial nerve palsy, or surgical site infection. Findings on overall complication rates have varied among the literature. In some studies however, IMN has been associated with an increased rate of shoulder pain and as a result a higher reoperation rate as compared to ORIF, though functional outcomes at 1-year show no difference.
Zhao et al. performed a systematic review of recent meta-analyses of randomized clinical trials (RCTs) to compare IMN and plate fixation for treatment humeral shaft fractures. The authors concluded that there was no difference between IMN and plate fixation with respect to fracture union, radial nerve injury, or infection. But they did note that IMN significantly increased the risk of shoulder complications (shoulder impingement and shoulder ROM) and reoperation.
Chen et al. performed a retrospective cohort study evaluating the incidence of humeral shaft fractures within the non-cancer Medicare population and comparing differences between IMN and plate fixation with respect to procedure times, secondary operations, and 1-year mortality. The authors found that IMN was performed more often than plate fixation most years over a 15-year period and was associated with significantly less anesthesia time (27.1 minutes, P < 0.0001). They concluded that there were no significant differences in the complication rates between the 2 groups as measured by the incidence of secondary operations and 1-year mortality.
Bisaccia et al. compared IMN, ORIF, and external fixation for the treatment of midshaft humeral fractures in 79 patients with a median follow-up of 11.5 months. The authors performed clinical and radiographic evaluation at 6 weeks, 6 months and 12 months. They found no differences in the duration of hospitalization, SF-36 scores, or complications between the 3 treatment arms. There were 2 cases of non-union in the ORIF group, 1 case in the IMN group and no cases in the external fixation group, and there was one case of transient radial nerve palsy in the IMN cohort.
Figure A is a radiograph showing a displaced transverse midshaft humeral fracture.
Incorrect Answers:
Answer 1: Though some studies have suggested an increased rate of shoulder-related complications with IMN fixation, there is not significant difference in the rate of surgical site infections for humeral shaft fractures when treated with IMN or ORIF.
Answer 2: There is no significant difference in the rate of radial nerve palsy among humeral shaft fractures treated with IMN or ORIF.
Answer 3: There is no difference in the rate of fracture union for humeral shaft fractures treated with IMN or ORIF.
Answer 3: Some studies have found an increased rate of shoulder complications such as pain and impingement with IMN fixation, leading to an increased rate of revision surgery. However many large meta-analyses contradict these findings.
Both ORIF and IMN are appropriate means of definitive fixation of diaphyseal humeral fractures. Numerous studies have directly compared the risks and
outcomes associated with each of the two methods, and the current literature supports that there is no difference in the rates of fracture union, radial nerve palsy, or surgical site infection. Findings on overall complication rates have varied among the literature. In some studies however, IMN has been associated with an increased rate of shoulder pain and as a result a higher reoperation rate as compared to ORIF, though functional outcomes at 1-year show no difference.
Zhao et al. performed a systematic review of recent meta-analyses of randomized clinical trials (RCTs) to compare IMN and plate fixation for treatment humeral shaft fractures. The authors concluded that there was no difference between IMN and plate fixation with respect to fracture union, radial nerve injury, or infection. But they did note that IMN significantly increased the risk of shoulder complications (shoulder impingement and shoulder ROM) and reoperation.
Chen et al. performed a retrospective cohort study evaluating the incidence of humeral shaft fractures within the non-cancer Medicare population and comparing differences between IMN and plate fixation with respect to procedure times, secondary operations, and 1-year mortality. The authors found that IMN was performed more often than plate fixation most years over a 15-year period and was associated with significantly less anesthesia time (27.1 minutes, P < 0.0001). They concluded that there were no significant differences in the complication rates between the 2 groups as measured by the incidence of secondary operations and 1-year mortality.
Bisaccia et al. compared IMN, ORIF, and external fixation for the treatment of midshaft humeral fractures in 79 patients with a median follow-up of 11.5 months. The authors performed clinical and radiographic evaluation at 6 weeks, 6 months and 12 months. They found no differences in the duration of hospitalization, SF-36 scores, or complications between the 3 treatment arms. There were 2 cases of non-union in the ORIF group, 1 case in the IMN group and no cases in the external fixation group, and there was one case of transient radial nerve palsy in the IMN cohort.
Figure A is a radiograph showing a displaced transverse midshaft humeral fracture.
Incorrect Answers:
Answer 1: Though some studies have suggested an increased rate of shoulder-related complications with IMN fixation, there is not significant difference in the rate of surgical site infections for humeral shaft fractures when treated with IMN or ORIF.
Answer 2: There is no significant difference in the rate of radial nerve palsy among humeral shaft fractures treated with IMN or ORIF.
Answer 3: There is no difference in the rate of fracture union for humeral shaft fractures treated with IMN or ORIF.
Answer 3: Some studies have found an increased rate of shoulder complications such as pain and impingement with IMN fixation, leading to an increased rate of revision surgery. However many large meta-analyses contradict these findings.
Question 4High Yield
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients.
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 5High Yield
A patient with a history of rheumatoid arthritis reports a painful total hip arthroplasty 3 years after the index procedure. Radiographs reveal loosening of the femoral component. Preoperative blood work shows an erythrocyte sedimentation rate (ESR) of 38 mm/h (normal 0-29 mm/h) and a C-reactive protein (CRP) of 8.9 (0.2- 8.0). What is the most appropriate action at this time?

Explanation
DISCUSSION: The question centers on the appropriate work-up for a failed total hip arthroplasty prior to revision surgery. The preoperative ESR is elevated and the CRP is at the upper end of normal. If either the ESR or CRP is elevated, further investigations are required to exclude infection as a cause of loosening, particularly in a patient only 3 years after the index procedure. A technetium scan alone is nonspecific and will show increased uptake because of the loose femoral component. An intraoperative frozen section is a helpful confirmatory investigation, but whenever possible the diagnosis should be made preoperatively to allow for appropriate surgical planning. Recently, investigators have shown the value of FDG-PET scanning as a useful investigation for diagnosing infection; however, it is no more accurate than the combined use of an ESR and CRP, and does not allow for identification of an infecting organism. At this point, a hip aspiration for culture is the most appropriate investigation.
REFERENCES: Bauer TW, Parvizi J, Kobayashi N, et al: Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-882.
Pill SG, Parvizi J, Tang PH, et al: Comparison of fiuorodeoxyglucose positron emission tomography and (111
)indium-white blood cell imaging in the diagnosis of periprosthetic infection of the hip. J Arthroplasty 2006;21:91-97.
Spangehl MJ, Masri BA, O’Connell JX, et al: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am 1999;81:672-683.
Figure 5a Figure 5b
REFERENCES: Bauer TW, Parvizi J, Kobayashi N, et al: Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-882.
Pill SG, Parvizi J, Tang PH, et al: Comparison of fiuorodeoxyglucose positron emission tomography and (111
)indium-white blood cell imaging in the diagnosis of periprosthetic infection of the hip. J Arthroplasty 2006;21:91-97.
Spangehl MJ, Masri BA, O’Connell JX, et al: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am 1999;81:672-683.
Figure 5a Figure 5b
Question 6High Yield
..A 35-year-old man fell off of a roof and sustained an extra-articular supracondylar elbow fracture. He had normal sensation in all fingers after the injury and before undergoing surgery to repair the fracture. The ulnar nerve was not transposed, but it was inspected prior to wound closure. Ten days after surgery, the patient has numbness in his small finger and is unable to cross his fingers. His elbow range of motion is between 40 degrees and 100 degrees. What is the next appropriate treatment step?
Explanation
- Observation
Question 7High Yield
A tall, thin 17-year-old basketball player and his parents request an evaluation of his flexible (hypermobile) pes planus/planovalgus foot deformities. As part of his evaluation, the orthopaedic surgeon notes pectus excavatum, disproportionately long arms, and scoliosis. In addition to providing treatment of his feet, what test or evaluation should the patient be referred for?

Explanation
The current diagnostic criteria for Marfan syndrome, called the Ghent criteria, are based on clinical findings and family history. The role of genetic testing in establishing the diagnosis is limited,because testing for FBN1 mutations is neither sensitive nor specific for Marfan syndrome. By making the diagnosis and arranging for cardiovascular evaluation, the orthopaedic surgeon can help prevent sudden death in these patients. The cardiovascular manifestations, including dissection and dilation of the ascending aorta and mitral valve prolapse, are responsible for nearly all of the precocious deaths of patients with Marfan syndrome. Patients with Marfan syndrome do have problems with protrusion acetabuli, scoliosis, and opthalmologic problems but the life-threatening problem that must be considered is the risk of cardiovascular sudden death.
---
---
Question 8High Yield
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure?
---
---








Explanation
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette _of the shoulder and is a stabilizer of the humeral head._
Question 9High Yield
What is the most appropriate next step in the treatment of increasing forearm pain and new numbness?
Explanation
- Obtain forearm compartment pressure measurements_
Question 10High Yield
Figures below show the AP and lateral radiographs obtained from a 54-year-old woman who has worsening
groin pain 18 months after a primary left total hip arthroplasty. The pain is worst when climbing stairs, when rising from a seated position, and during resisted hip flexion. Her pain improved early after surgery but did
not completely resolve. Her C-reactive protein and erythrocyte sedimentation rate results of less than 1 mg/dL
and 10 mm/hr, respectively, were obtained in the office. What is the best next step?
groin pain 18 months after a primary left total hip arthroplasty. The pain is worst when climbing stairs, when rising from a seated position, and during resisted hip flexion. Her pain improved early after surgery but did
not completely resolve. Her C-reactive protein and erythrocyte sedimentation rate results of less than 1 mg/dL
and 10 mm/hr, respectively, were obtained in the office. What is the best next step?

Explanation
Iliopsoas impingement is a potential cause of persistent groin pain after a total hip arthroplasty. This patient’s history gives groin pain with resisted hip flexion and during activities that require this level of function. The radiographs depict an acetabular component with substantial retroversion. Typical options for the management of iliopsoas tendon impingement include injections, tenotomy, and acetabular revision. Recently, Chalmers and associates reported more predictable groin pain resolution with 8 mm or more of anterior acetabular component when overhang was revised. The radiographs clearly show more retroversion, with a cup prominence of more than 8 mm anteriorly. MRI with MARS could potentially help in the diagnosis of this impingement but would not help in management (option A). An ultrasound- guided injection would need to be administered into the iliopsoas tendon sheath to be of help and, in this case, would likely be performed for diagnostic purposes due to the extreme anterior overhang (option C). Option D would be useful for mild cases of iliopsoas impingement but likely would not help much in this more extreme case.
Question 11High Yield
Figure below shows the radiograph obtained from a 76-year-old woman who has sharp pain in her groin,
thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best
to proceed. What is the best next step?
thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best
to proceed. What is the best next step?

Explanation
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the
injection.
injection.
Question 12High Yield
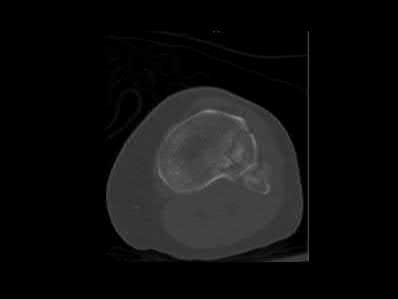
Figures 1 through 7 are the radiograph, MRI, and CT scans of a 21-year-old developmentally delayed woman who complains of urinary urgency, low back pain, and gait disturbance. What is the most appropriate treatment at this time?


Explanation
■
The patient has a low-grade but high-dysplastic spondylolisthesis (vertical and domed sacrum) with severe spinal canal stenosis. The MRI scan shows the dysplastic sacrum and severe central stenosis associated with an intact pars interarticularis, bulging L5-S1 disk, and domed posterior sacrum. Although many treatments are available for low-grade isthmic spondylolisthesis, this spondylolisthesis condition requires a complete laminectomy and possible sacral dome resection because of the severe central stenosis with an intact pars interarticularis (no lysis) in a patient with early neurological signs (Figures 6 and 7 are CT scans of the L5 pars without evidence of a lysis). Patients with dysplastic spondylolisthesis without a lysis can develop cauda equina syndrome with loss of bowel/ bladder function and weakness of the gastrocsoleus muscles (sacral nerve roots) and should be recognized and treated with appropriate laminectomy decompression followed by spinal fusion, typically with posterior instrumentation and interbody fusion. A “Gill” laminectomy is described as removal of the lamina from pars interarticularis lysis and including the abnormal inferior facets. There is no lysis in this patient, and while laminectomy is needed, a Gill laminectomy is not possible. Transforaminal interbody fusion and percutaneous instrumentation does not address the central spinal stenosis.
The patient has a low-grade but high-dysplastic spondylolisthesis (vertical and domed sacrum) with severe spinal canal stenosis. The MRI scan shows the dysplastic sacrum and severe central stenosis associated with an intact pars interarticularis, bulging L5-S1 disk, and domed posterior sacrum. Although many treatments are available for low-grade isthmic spondylolisthesis, this spondylolisthesis condition requires a complete laminectomy and possible sacral dome resection because of the severe central stenosis with an intact pars interarticularis (no lysis) in a patient with early neurological signs (Figures 6 and 7 are CT scans of the L5 pars without evidence of a lysis). Patients with dysplastic spondylolisthesis without a lysis can develop cauda equina syndrome with loss of bowel/ bladder function and weakness of the gastrocsoleus muscles (sacral nerve roots) and should be recognized and treated with appropriate laminectomy decompression followed by spinal fusion, typically with posterior instrumentation and interbody fusion. A “Gill” laminectomy is described as removal of the lamina from pars interarticularis lysis and including the abnormal inferior facets. There is no lysis in this patient, and while laminectomy is needed, a Gill laminectomy is not possible. Transforaminal interbody fusion and percutaneous instrumentation does not address the central spinal stenosis.
Question 13High Yield
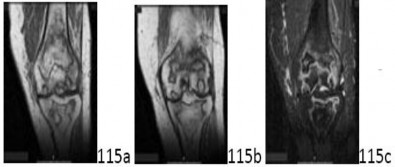
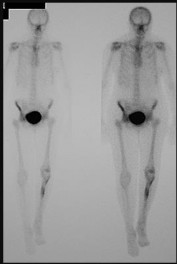
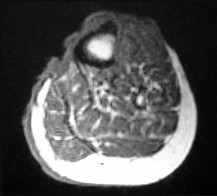
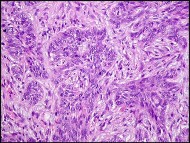
Figure 68a is the clinical photograph of a 59-year-old woman who has had a long-standing fungating ulcer on her left lower leg. She states that the ulcer began as a small reddened area and gradually enlarged during the last 4 years. Anteroposterior (AP) and lateral radiographs of her left leg are shown in Figures 68b and 68c. A whole-body bone scan is shown in Figure 68d. An axial T1-weighted MR image is shown in Figure 68e. A CT scan of the pelvis at the level of the groin is shown in Figure 68f. A histologic specimen is shown in Figure 68g. Based on the clinical, radiographic, and histologic information, the diagnosis is






Explanation
The clinical photograph reveals a large ulcerated lesion of the anterior leg. The AP and lateral radiographs reveal the soft-tissue abnormality, and the bone scan reveals increased metabolic activity of the underlying tibia. T1-weighted MR imaging reveals the lesion wrapping around the anterior tibia with loss of subcutaneous tissue. A CT scan of the pelvis reveals an inguinal lymph node. The histology reveals nests of polyhedral cells surrounded by reactive fibrosis. The diagnosis is poorly differentiated squamous cell carcinoma, and the patient has the characteristic findings of a long-standing squamous cell carcinoma with poor differentiation and likely regional lymph node metastasis. The history of a small reddened area does not suggest any of the other diagnoses. Although keratin pearls are not shown in this histologic field, nests of polyhedral cells indicate squamous cell carcinoma. A small subset of patients with squamous cell carcinoma will have advanced disease. Size and differentiation, as well as type of surgical procedure and margins of resection, are of prognostic significance. Sentinel node evaluation for patients at high risk has been suggested, including evaluations for lesions that are larger in size and with poor differentiation, perineural invasion, or compromised immunologic states. The nonpreferred responses are not associated with the clinical presentation of squamous cell carcinoma. Squamous cell carcinomas are keratin positive on immunohistochemistry.
RECOMMENDED READINGS
33. [Kwon S, Dong ZM, Wu PC. Sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma: clinical experience and review of literature. World J Surg Oncol. 2011 Jul 19;9:80. doi: 10.1186/1477-7819-9-80. Review. PubMed PMID: 21771334.](http://www.ncbi.nlm.nih.gov/pubmed/21771334)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21771334)
34. [North JH Jr, Spellman JE, Driscoll D, Velez A, Kraybill WG, Petrelli NJ. Advanced cutaneous squamous cell carcinoma of the trunk and extremity: analysis of prognostic factors. J Surg Oncol. 1997 Mar;64(3):212-7. PubMed PMID: 9121152.](http://www.ncbi.nlm.nih.gov/pubmed/9121152)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9121152)
CLINICAL SITUATION FOR QUESTIONS 69 AND 70
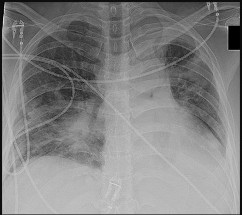
Figure 69a is the radiograph of a 39-year-old woman with metastatic lung cancer who underwent a prophylactic right intramedullary nail procedure. There were no intraoperative or immediate postsurgical problems. Ten hours after surgery, the patient became increasingly confused and agitated. An examination was notable for altered mentation, tachycardia, and new-onset hypoxemia. Chest radiographs were obtained before surgery (Figure 69b) and immediately after symptom onset (Figure 69c).
RECOMMENDED READINGS
33. [Kwon S, Dong ZM, Wu PC. Sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma: clinical experience and review of literature. World J Surg Oncol. 2011 Jul 19;9:80. doi: 10.1186/1477-7819-9-80. Review. PubMed PMID: 21771334.](http://www.ncbi.nlm.nih.gov/pubmed/21771334)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21771334)
34. [North JH Jr, Spellman JE, Driscoll D, Velez A, Kraybill WG, Petrelli NJ. Advanced cutaneous squamous cell carcinoma of the trunk and extremity: analysis of prognostic factors. J Surg Oncol. 1997 Mar;64(3):212-7. PubMed PMID: 9121152.](http://www.ncbi.nlm.nih.gov/pubmed/9121152)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9121152)
CLINICAL SITUATION FOR QUESTIONS 69 AND 70
Figure 69a is the radiograph of a 39-year-old woman with metastatic lung cancer who underwent a prophylactic right intramedullary nail procedure. There were no intraoperative or immediate postsurgical problems. Ten hours after surgery, the patient became increasingly confused and agitated. An examination was notable for altered mentation, tachycardia, and new-onset hypoxemia. Chest radiographs were obtained before surgery (Figure 69b) and immediately after symptom onset (Figure 69c).
Question 14High Yield
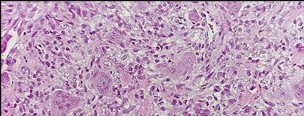
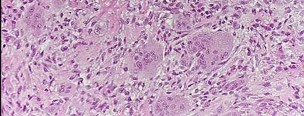
Figures 98a and 98b are the radiograph and biopsy specimen of a 20-year-old man who is being evaluated for the first time for foot pain. Treatment should include

Explanation
This pathology is most consistent with giant-cell tumor. Note the presence of multinucleated cells and stroma of spindlelike cells with pale staining cytoplasm and nuclei. Giant-cell tumors typically occur in patients ages 20 to 40. Common sites include the epiphysis of the distal femur or proximal tibia (50% of the time). Although it is a benign lesion, giant-cell tumors have a tendency for bone destruction, recurrence, and, rarely, metastasis. The initial treatment of choice is curettage with grafting or cementation. For recurrent or stage III tumors, wide excision may be necessary. Chemotherapy or radiation therapy are not indicated as initial treatment, especially if this is an isolated primary lesion.
RECOMMENDED READINGS
106. [Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006 Jan;37(1):35-51. Review. PubMed PMID: 16311110.](http://www.ncbi.nlm.nih.gov/pubmed/16311110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16311110)
107. [Eckardt JJ, Grogan TJ. Giant cell tumor of bone. Clin Orthop Relat Res. 1986 Mar;(204):45-58. Review. PubMed PMID: 3514036.](http://www.ncbi.nlm.nih.gov/pubmed/3514036)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3514036)
RECOMMENDED READINGS
106. [Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006 Jan;37(1):35-51. Review. PubMed PMID: 16311110.](http://www.ncbi.nlm.nih.gov/pubmed/16311110)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16311110)
107. [Eckardt JJ, Grogan TJ. Giant cell tumor of bone. Clin Orthop Relat Res. 1986 Mar;(204):45-58. Review. PubMed PMID: 3514036.](http://www.ncbi.nlm.nih.gov/pubmed/3514036)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3514036)
Question 15High Yield
A 27-year-old male is involved in a motor vehicle accident and sustains the injury shown in Figures A through E. The articular surface is depressed 2 mm while there is 3 mm of condylar widening. Valgus instability of the knee is noted. Which of the following is most important to long-term success in surgical treatment of this case?







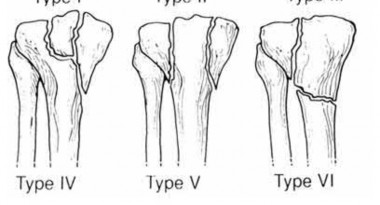
Explanation
The clinical presentation and imaging studies are consistent with a tibial plateau fracture. Restoration of joint stability has been shown to be the strongest predictor of long term outcomes.
Honkonen reviewed 131 tibial condyle fractures and determined that articular stepoff <3mm and tibial widening <5mm did not negatively effect outcomes. In contrast, 70% of knees with moderate to severe malalignment went on to functionally unacceptable outcomes. They suggested operative fixation for all medial uni and bicondylar fractures, any lateral fractures with >5 degrees of
valgus tilt, >3mm of articular depression, >5mm of condylar widening, or >5 degrees of valgus malalignment.
In the Marsh et al JAAOS symposium review, the authors noted that fractures with up to 10mm of articular depression and joint stability obtained acceptable functional outcomes. They also cited a 20 year follow-up which indicated that articular step-off alone was not a predictor of poor long-term results. More importantly, when instability is present with other factors, including step-off and central depression, poor results followed.
Illustrations A and B show the intraoperative films. Illustration C reviews the Schatzker classification system.
Honkonen reviewed 131 tibial condyle fractures and determined that articular stepoff <3mm and tibial widening <5mm did not negatively effect outcomes. In contrast, 70% of knees with moderate to severe malalignment went on to functionally unacceptable outcomes. They suggested operative fixation for all medial uni and bicondylar fractures, any lateral fractures with >5 degrees of
valgus tilt, >3mm of articular depression, >5mm of condylar widening, or >5 degrees of valgus malalignment.
In the Marsh et al JAAOS symposium review, the authors noted that fractures with up to 10mm of articular depression and joint stability obtained acceptable functional outcomes. They also cited a 20 year follow-up which indicated that articular step-off alone was not a predictor of poor long-term results. More importantly, when instability is present with other factors, including step-off and central depression, poor results followed.
Illustrations A and B show the intraoperative films. Illustration C reviews the Schatzker classification system.
Question 16High Yield
With the use of perineural catheters, improvement in all of the following outcomes can be anticipated except:
Explanation
Double blind placebo controlled randomized trials the use of perineural catheters led to improved pain scores, decreased narcotiCusage and narcotiCrelated side effects, and fewer sleep disturbances.
Length of stay was shortened by the use of perineural catheters as compared to epidural or IV PCA analgesia in several studies. In pilot studies, the use of perineural catheters in carefully selected patients allowed ambulatory total shoulder arthroplasty and single day admissions for total hip arthroplasty and total knee arthroplasty
Length of stay was shortened by the use of perineural catheters as compared to epidural or IV PCA analgesia in several studies. In pilot studies, the use of perineural catheters in carefully selected patients allowed ambulatory total shoulder arthroplasty and single day admissions for total hip arthroplasty and total knee arthroplasty
Question 17High Yield
Figure 1 is the MR image of a 43-year-old man who has left shoulder pain and weakness after a fall. An examination reveals active forward elevation at 120° and positive Yergason and lift-off test examination findings. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time?
---
---
Explanation
The MR image shows medial subluxation of the biceps tendon, which can be confused with an articular loose body. In the clinical scenario of biceps instability/subluxation, the rationale regarding tenodesis is to address the painful dislocation and subluxation of the biceps tendon from the bicipital groove. Biceps tendon subluxation is most frequently associated with subscapularis tendon pathology, which is indicated by the MRI and by a positive lift-off test. The MR image does not show a loose body or Bankart lesion. Patients with irreparable rotator cuff tears with a severe external rotation deficit and a deficient teres minor _may experience a better functional result with latissimus dorsi transfer._
Question 18High Yield
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?
Explanation
Long-term outcomes following tibial plafond fractures treated with ORIF are satisfactory in most patients despite a high incidence of posttraumatic osteoarthritis. If ORIF is delayed until 10 to 20 days following injury, the major difference in outcomes is fewer complications associated with wound healing. Ankle strength, pain, range of motion, and the development of arthritis are equal regardless of the time until fixation.
REFERENCES: Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
REFERENCES: Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 19High Yield
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?


Explanation
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
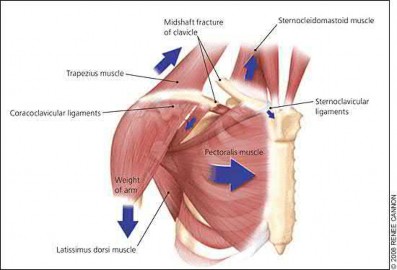
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
Answer 1: Diaphyseal fractures were demonstrated to have the lowest rate of nonunion when compared to lateral third fractures and medial clavicle fractures.
Answer 3: Advancing age was found to be an independent predictor of nonunion.
Answer 4: Female gender was found to be an independent predictor of nonunion.
Answer 5: Injury to the dominant hand was not found to be associated with an increased risk of non-union.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
Answer 1: Diaphyseal fractures were demonstrated to have the lowest rate of nonunion when compared to lateral third fractures and medial clavicle fractures.
Answer 3: Advancing age was found to be an independent predictor of nonunion.
Answer 4: Female gender was found to be an independent predictor of nonunion.
Answer 5: Injury to the dominant hand was not found to be associated with an increased risk of non-union.
Question 20High Yield
A 45-year-old man sustained the injury shown in Figures 36a and 36b. The involved side is his dominantside. What is the most appropriate management?
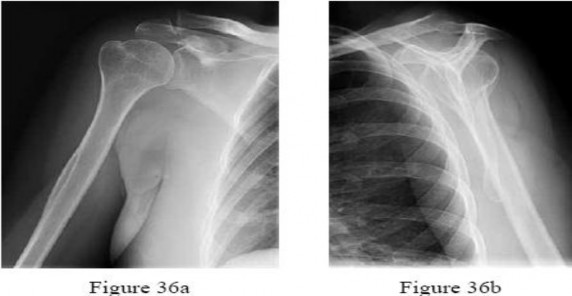
Explanation
No detailed explanation provided for this question.
Question 21High Yield
This shoulder deformity often is associated with an abnormal connection between the scapula and the
Explanation
- spine.
Question 22High Yield
Which of the following is most important to achieve a good outcome following a Syme amputation?
Explanation
A Syme amputation is effectively a tibiotalar disarticulation, which provides an end-bearing stump that could potentially allow ambulation without a prosthesis over short distances. It works better for tumor and trauma, but the heel pad must be viable. The two most common problems are 1) skin sloughing from compromised vascular supply and 2) migration of the heel pad due to instability. A hypermobile heel pad can cause difficulty with prosthesis wear and damage to the soft tissues which can eventually lead to failure. Both malleoli are usually removed in the procedure, except in children or during the first stage procedure of a diabetic or infection case. The tibialis anterior is usually tenodesed to the anterior heel pad along with the EDL tendon to avoid posterior migration of the heel pad.
Question 23High Yield
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty
to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 24High Yield
Figures 1 through 4 are the AP and lateral radiographs and MR images of a 12-year-old postmenarchal girl who injured her right knee playing basketball 2 weeks ago. She developed significant swelling and pain and was unable to bear weight. How should the family be counseled regarding expectations and outcomes following this injury?

Explanation
■
Historically, anterior cruciate ligament (ACL) injuries in skeletally immature patients were treated nonsurgically with bracing, physical therapy, and activity modification because of concerns about risk to the physis during ACL reconstruction. Current evidence suggests that patients treated surgically have less knee instability, higher rates of return to activity, higher functional scores, and lower rates of subsequent meniscal tear. One of the most common complications encountered after ACL reconstruction in this patient population is secondary injury of the same or the contralateral knee, which has been found to be >5 times greater than that of healthy controls. Nearly 30% of athletes in one cohort sustained a second ACL injury within 24 months of return to sport, with approximately one-third of these injuries occurring in the ipsilateral knee and twothirds occurring in the contralateral knee. Thus, although most young athletes are able to return to sports after reconstruction of their ACL, they have a significantly higher risk of secondary ACL injury (ipsilateral or contralateral) compared with the adult population.
■
Historically, anterior cruciate ligament (ACL) injuries in skeletally immature patients were treated nonsurgically with bracing, physical therapy, and activity modification because of concerns about risk to the physis during ACL reconstruction. Current evidence suggests that patients treated surgically have less knee instability, higher rates of return to activity, higher functional scores, and lower rates of subsequent meniscal tear. One of the most common complications encountered after ACL reconstruction in this patient population is secondary injury of the same or the contralateral knee, which has been found to be >5 times greater than that of healthy controls. Nearly 30% of athletes in one cohort sustained a second ACL injury within 24 months of return to sport, with approximately one-third of these injuries occurring in the ipsilateral knee and twothirds occurring in the contralateral knee. Thus, although most young athletes are able to return to sports after reconstruction of their ACL, they have a significantly higher risk of secondary ACL injury (ipsilateral or contralateral) compared with the adult population.
Question 25High Yield
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is
Explanation
Diabetes mellitus has been associated with resistant cases of adhesive capsulitis. With other causes of onset, adhesive capsulitis frequently responds to nonsurgical management such as stretching exercises or, when this fails, manipulation under anesthesia and/or arthroscopic release. Manipulation is rarely successful for the treatment of adhesive capsulitis associated with diabetes mellitus, and arthroscopic release may be preferred.
REFERENCES: Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146.
Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
REFERENCES: Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146.
Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 26High Yield
A 29-year-old female has sustained the acute injury shown in Figure A. Which of the following is an indication for open reduction internal fixation in this patient?

Explanation
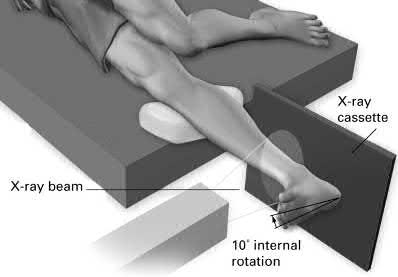
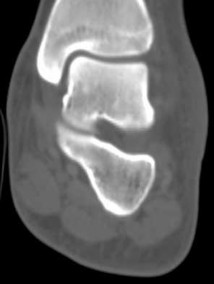
Figure A shows a minimally displaced Weber B ankle fracture. The need for operative treatment would be dependent on fracture stability. A gravity stress test would best demonstrate fracture displacement, syndesmotic injury and medial sided ligamentous integrity.
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were
not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Answers 1-2: Differentiation between stage-II and stage-IV supination-external rotation fractures (Lauge-Hansen Classification) is clinically relevant as an intact deltoid ligament stabilizes the ankle mortise and open reduction is thought to be unnecessary. The best way to determine deltoid integrity would be to perform a gravity stress radiograph.
Asnwer 3: The cotton test is an intra-operative test to assess for syndesmotic injury. It would not be used in an awake patient for this purpose.
Answer 5: A positive squeeze test is suggestive of a syndesmotic injury. However, this test has a lower sensitivity for detecting syndesmotic injury in comparison to stress radiographs.
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were
not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Answers 1-2: Differentiation between stage-II and stage-IV supination-external rotation fractures (Lauge-Hansen Classification) is clinically relevant as an intact deltoid ligament stabilizes the ankle mortise and open reduction is thought to be unnecessary. The best way to determine deltoid integrity would be to perform a gravity stress radiograph.
Asnwer 3: The cotton test is an intra-operative test to assess for syndesmotic injury. It would not be used in an awake patient for this purpose.
Answer 5: A positive squeeze test is suggestive of a syndesmotic injury. However, this test has a lower sensitivity for detecting syndesmotic injury in comparison to stress radiographs.
Question 27High Yield
Schwannomas are differentiated from neurofibromas by all of the following except:
Explanation
Schwann cells contribute to schwannoma and neurofibroma.
Question 28High Yield
Which of the following cell type-cell function pairings is false:
Explanation
Osteoclasts resorb bone by attaching to the bone surface, releasing enzymes, and dissolve the organiCmineral phases of bone. Osteoclasts do not have hormone receptors
Question 29High Yield
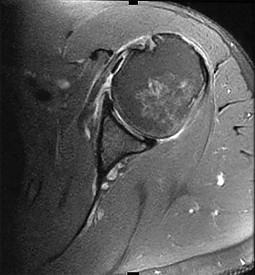
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
Explanation
The axial MRI scan reveals a subluxated biceps tendon. In the study by Koh and associates, 85% of patients with a biceps subluxation on MRI were found to have a subscapularis tear at the time of arthroscopy. These are not always obvious on the MRI, and close inspection of the leading edge/upper border of the subscapularis tendon at the time of arthroscopy is necessary. Although supraspinatus tears, SLAP tears, and Bankart tears can all occur in conjunction with a biceps subluxation, none have been shown to be strongly correlated with this pathology, nor as specific to this pathology.
57
57
Question 30High Yield
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
Anteromedial displacement of the tibial tubercle unloads the distal and lateral facets of the patella and shifts the forces to the proximal and medial facets. Therefore, if findings indicate arthrosis predominately in the medial and proximal areas of the patella, this is considered a relative contraindication because it may accentuate arthritic symptoms.
REFERENCES: Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181.
Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Kuroda R, Kambic H, Valdevit A, et al: Articular cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med 2001;29:403-409.
REFERENCES: Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181.
Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Kuroda R, Kambic H, Valdevit A, et al: Articular cartilage contact pressure after tibial tuberosity transfer: A cadaveric study. Am J Sports Med 2001;29:403-409.
Question 31High Yield
What is the primary goal of the initial (acute) rehabilitation phase of an overhead athlete’s shoulder?
Explanation
DISCUSSION: The goal in the initial phase of shoulder rehabilitation is to improve flexibility, reestablish baseline dynamic stability, normalize muscle balance, and restore proprioception. In the advanced strengthening and final phase, the goals are to initiate aggressive strengthening drills, enhance power and endurance, perform functional drills, and to gradually initiate throwing activities.
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Wilk KE, Arrigo C: Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther 1993;18:365-378.
DISCUSSION: The goal in the initial phase of shoulder rehabilitation is to improve flexibility, reestablish baseline dynamic stability, normalize muscle balance, and restore proprioception. In the advanced strengthening and final phase, the goals are to initiate aggressive strengthening drills, enhance power and endurance, perform functional drills, and to gradually initiate throwing activities.
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Wilk KE, Arrigo C: Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther 1993;18:365-378.
Question 32High Yield
All of the following are true statements regarding elbow involvement in ulnar club hand except:
Explanation
Elbow instability does not correspond with severity of involvement. Fifty percent of patients with total aplasia have radiohumeral synostosis, which provides adequate stability.
Question 33High Yield
Dupuytrenâs cord tissue is characterized by what change from normal:
Explanation
C ompared to normal palmar fascia, the fibrous bands in Dupuytrenâs disease have an increased ratio of type III to type I
collagen, and an overall increase in the amount of type III collagen.
collagen, and an overall increase in the amount of type III collagen.
Question 34High Yield
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include
Explanation
The patient has a displaced radial neck fracture. Displaced radial neck fractures with angulation of more than 30° to 45° require reduction. Methods of attempted closed reduction include wrapping the arm with an Esmarch’s bandage and applying direct pressure over the maximum deformity of the radial head. More aggressive methods include a Kirschner wire used as a joystick or intramedullary reduction as described by the Metaizeau technique. Open reduction should be avoided because of complications such as stiffness or osteonecrosis. Indications for open reduction are irreducible displacement of more than 45° with severe restriction of forearm rotation.
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
Question 35High Yield
Which of the following portions of a gene directly codes for the messenger RNA for eventual translation into proteins on the ribosome:
Explanation
The human genome is composed of approximately 30,000 unique genes. Each gene is composed of a promotor or regulator region and a transcriptional or coding region. Regulatory proteins or transcription factors bind to the promoter region of the gene
to signal the beginning of transcription of the DNA into RNA or repress the expression of the gene. The coding region contains both introns and exons. Exon sequences of the gene directly code for the proteins, and the introns are spacers. The intron sequences are enzymatically removed from the newly transcribed messenger RNA by a splicing mechanism
to signal the beginning of transcription of the DNA into RNA or repress the expression of the gene. The coding region contains both introns and exons. Exon sequences of the gene directly code for the proteins, and the introns are spacers. The intron sequences are enzymatically removed from the newly transcribed messenger RNA by a splicing mechanism
Question 36High Yield
Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?

Explanation
No detailed explanation provided for this question.
Question 37High Yield
During surgical hip dislocation for the management of femoral acetabular impingement, preservation of what structure is paramount to maintaining vascularity to the femoral head? ](http://www.orthobullets.com/anatomy/10123/hip-blood-supply)
Explanation
No detailed explanation provided for this question.
Question 38High Yield
A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:



Explanation
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:
Answer 1: A surgical delay of greater than 48 hours has not been found to increase intraoperative time when patients get to surgery.
Answer 3: A surgical delay of greater than 48 hours has been shown to increase the rate of postoperative pneumonia.
Answer 4: A surgical delay of greater than 48 hours has not been associated with higher rates of blood transfusion.
Answer 5: A surgical delay of greater than 48 hours has not been associated with an increased risk of post-operative infection.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:
Answer 1: A surgical delay of greater than 48 hours has not been found to increase intraoperative time when patients get to surgery.
Answer 3: A surgical delay of greater than 48 hours has been shown to increase the rate of postoperative pneumonia.
Answer 4: A surgical delay of greater than 48 hours has not been associated with higher rates of blood transfusion.
Answer 5: A surgical delay of greater than 48 hours has not been associated with an increased risk of post-operative infection.
Question 39High Yield
When total knee replacement surgery is complete, the alignment of the knee must be:
Explanation
The tibial cut is perpendicular to the tibial axis, the femoral cut is made in 4° to 6° valgus, and the knee aligned in 4° to 6° of valgus provided the ligaments are balanced
Question 40High Yield
-Decreased sun exposure leads to decreased bone health via what mechanism?
Explanation
No detailed explanation provided for this question.
Question 41High Yield
Figures 1 through 5 are the AP and lateral radiographs and MR images of a 16-year-old boy who has a 1-year history of low back pain. The pain bothers him only at night, and it awakens him from sleep. NSAIDs allow him to return to sleep. What is the most appropriate next step in treatment?


Explanation
■
The history and imaging are consistent with an osteoid osteoma of the posterior sacrum. Percutaneous ablation techniques have become the standard first-line treatment for most extremity lesions. Concern exists about the use of radiofrequency ablation (RFA) in spinal lesions because of the potential for thermal injury of adjacent neurovascular structures, particularly in the absence of intact cortex surrounding the lesion. RFA should be avoided when neurovascular structures would be within 1 cm of the electrode. As such, excision would be preferable. There is no role for chemotherapy or radiation therapy in the management of osteoid osteomas.
■
The history and imaging are consistent with an osteoid osteoma of the posterior sacrum. Percutaneous ablation techniques have become the standard first-line treatment for most extremity lesions. Concern exists about the use of radiofrequency ablation (RFA) in spinal lesions because of the potential for thermal injury of adjacent neurovascular structures, particularly in the absence of intact cortex surrounding the lesion. RFA should be avoided when neurovascular structures would be within 1 cm of the electrode. As such, excision would be preferable. There is no role for chemotherapy or radiation therapy in the management of osteoid osteomas.
Question 42High Yield
Which of the following statements best describes how unicompartmental knee arthroplasty (UKA) differs from total knee arthroplasty (TKA)?
Explanation
DISCUSSION: Because UKA does not require cruciate sacrifice, patellofemoral resurfacing, or rotational changes to the femur or tibia, it reliably recreates normal knee kinematics. UKAs have generally demonstrated higher reoperation rates than TKAs at intermediate and long-term follow-up, due in part to progression of arthritis in the nonresurfaced compartments. Mobile bearings have been clinically successful in both UKA and TKA.
REFERENCES: Patil S, Colwell CW Jr, Ezzet KA, et al: Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 2005;87:332-338.
Gioe TJ, Killeen KK, Hoeffel DP, et al: Analysis of unicompartmental knee arthroplasty in a community- based implant registry. Clin Orthop Relat Res 2003;416:111-119.
REFERENCES: Patil S, Colwell CW Jr, Ezzet KA, et al: Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 2005;87:332-338.
Gioe TJ, Killeen KK, Hoeffel DP, et al: Analysis of unicompartmental knee arthroplasty in a community- based implant registry. Clin Orthop Relat Res 2003;416:111-119.
Question 43High Yield
Figures 5a through 5h
A B
C
6
D E F
G
H
A B
C
6
D E F
G
H







Explanation
- Calcaneonavicular (CN) coalition
Question 44High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury.
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 45High Yield
Which compartment pressure measurement combinations are concerning for compartment syndrome?
Explanation
- 20 mm Hg absolute, 10 mm Hg lower than diastolic blood pressure_
Question 46High Yield
Which of the following is the most appropriate clinical scenario to utilize locking plate and screw technology?
Explanation
Conventional plating provides stable internal fixation when fractures are anatomically reduced. Stability of this type of fixation relies on the plate/bone interface and the friction that develops between this interface. Locked plates rely on the plate/screw interface, and each provides not only axial stability but also angular stability; each screw acts as a fixed angle device. Indications for locked plating for indirect reduction include: 1. metaphyseal/diaphyseal fractures 2. comminuted diaphyseal fractures 3. comminuted metaphyseal fractures. 4. short segment fixation. Locked plates are not indicated for displaced articular fractures unless anatomic rigid fixation of the articular surface is done first (locking technology cannot reduce fractures/lag segments together).
The referenced article by Gardner et al reviews locking technology and reminds us that compression technology using non-locking screws and plates is still needed for many fractures and is even required for proper treatment of some fractures.
The referenced article by Wagner is an instructional paper on how to use hybrid plating technology and reviews concepts such as the necessity of lag screw fixation before locking.
The referenced study by Egol et al is a review paper that notes that locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. They report that locked plates are indicated for: indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, and with bridging severely comminuted fractures.
The referenced article by Gardner et al reviews locking technology and reminds us that compression technology using non-locking screws and plates is still needed for many fractures and is even required for proper treatment of some fractures.
The referenced article by Wagner is an instructional paper on how to use hybrid plating technology and reviews concepts such as the necessity of lag screw fixation before locking.
The referenced study by Egol et al is a review paper that notes that locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. They report that locked plates are indicated for: indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, and with bridging severely comminuted fractures.
Question 47High Yield
This pathology most likely causes mechanical low-back pain.
Explanation
- Figure 72e Figure 72f
Question 48High Yield
Estrogen deficiency results in which of the following:
Explanation
Estrogen deficiency results in increased bone resorption. An increase in IL-6 expression stimulates osteoclasts to resorb bone.
An increase in M-CSF and RANKL results in increased osteoclastiCactivity. OPG decreases osteoclastiCactivity as a decoy inhibitor of RANK
An increase in M-CSF and RANKL results in increased osteoclastiCactivity. OPG decreases osteoclastiCactivity as a decoy inhibitor of RANK
Question 49High Yield
Which of the following conditions is not associated with an increased incidence of congenital vertical talus:
Explanation
Patients with cerebral palsy do not have an increased risk of congenital vertical talus, but they may develop an acquired neuromuscular vertical talus.
Patients with myelomeningocele have approximately a 5% to 10% risk of vertical talus, far above that of the general population.
Arthrogryposis is associated with an increased risk of vertical talus.
Nail patella syndrome and Larsen syndrome are associated with an increased risk of vertical talus.
Patients with myelomeningocele have approximately a 5% to 10% risk of vertical talus, far above that of the general population.
Arthrogryposis is associated with an increased risk of vertical talus.
Nail patella syndrome and Larsen syndrome are associated with an increased risk of vertical talus.
Question 50High Yield
An 88-year-old nursing home resident is seen in the emergency department after a fall. At the time of admission, physical examination of the affected extremity reveals absent pulses and inadequate capillary refill. A radiograph is seen in Figure 48. Appropriate management includes which of the following?
Explanation
The patient has a Vancouver type B3 periprosthetic femur fracture (fracture around a total hip prosthesis with a loose stem and poor proximal bone stock). This type of periprosthetic fracture necessitates revision of the femoral component as well as fracture fixation. This patient has diminished blood flow in the extremity that necessitates emergent vascular surgical evaluation.
REFERENCES: Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215-220,
Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for the treatment of periprosthetic fractures. J
Bone Joint Surg Am 2005;87:1777-1781. Question 49
An otherwise healthy 58-year-old woman reports hip pain after undergoing total hip arthroplasty 8 months ago. She gives a history of prolonged wound drainage after surgery treated with antibiotics.
Hip aspiration is positive for methicillin-resistant coagulase-negative staphylococcus. Appropriate management at this point includes which of the following?
1. Arthroscopic irrigation followed by appropriate antibiotic treatment
2. Treatment with 6 weeks of IV vancomycin and oral rifampin
3. Treatment with 6 weeks of IV vancomycin and oral rifampin, followed by indefinite oral antibiotic suppression
4. Open debridement with exchange of the polyethylene insert, followed by appropriate antibiotic
treatment
5. Open debridement with removal of the implants and insertion of an antibiotic spacer
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a late chronic periprosthetic infection. The history points to a missed postoperative infection where the patient was treated with antibiotics for prolonged wound drainage. A low virulent organism, such as coagulase-negative staphylococcus, is often the pathogen. In an otherwise healthy patient with a reasonable life expectancy, the goal of treatment should be cure of the infection. Treatment for late chronic infection requires removal of the implants. Treatment with antibiotics alone, or debridement without removal of the implants is generally unsuccessful. Controversy exists regarding one- stage treatment with immediate reimplantation versus two-stage treatment with delayed reimplantation. Generally, a higher cure rate is achieved with a two-stage reimplantation (approximately 90% to 93%) than with one-stage reimplantation (75% to 80%).
REFERENCES: Hanssen AD, Spangehl MJ: Treatment of the infected hip replacement. Clin Orthop Relat Res 2004;420:63-71.
Isiklar ZU, Demirors H, Akpinar S, et al: Two-stage treatment of chronic staphylococcal orthopaedic
implant-related infections using vancomycin impregnated PMMA spacer and rifampin containing antibiotic protocol. Bull Hosp Jt Dis 1999;58:79-85.
REFERENCES: Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215-220,
Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for the treatment of periprosthetic fractures. J
Bone Joint Surg Am 2005;87:1777-1781. Question 49
An otherwise healthy 58-year-old woman reports hip pain after undergoing total hip arthroplasty 8 months ago. She gives a history of prolonged wound drainage after surgery treated with antibiotics.
Hip aspiration is positive for methicillin-resistant coagulase-negative staphylococcus. Appropriate management at this point includes which of the following?
1. Arthroscopic irrigation followed by appropriate antibiotic treatment
2. Treatment with 6 weeks of IV vancomycin and oral rifampin
3. Treatment with 6 weeks of IV vancomycin and oral rifampin, followed by indefinite oral antibiotic suppression
4. Open debridement with exchange of the polyethylene insert, followed by appropriate antibiotic
treatment
5. Open debridement with removal of the implants and insertion of an antibiotic spacer
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a late chronic periprosthetic infection. The history points to a missed postoperative infection where the patient was treated with antibiotics for prolonged wound drainage. A low virulent organism, such as coagulase-negative staphylococcus, is often the pathogen. In an otherwise healthy patient with a reasonable life expectancy, the goal of treatment should be cure of the infection. Treatment for late chronic infection requires removal of the implants. Treatment with antibiotics alone, or debridement without removal of the implants is generally unsuccessful. Controversy exists regarding one- stage treatment with immediate reimplantation versus two-stage treatment with delayed reimplantation. Generally, a higher cure rate is achieved with a two-stage reimplantation (approximately 90% to 93%) than with one-stage reimplantation (75% to 80%).
REFERENCES: Hanssen AD, Spangehl MJ: Treatment of the infected hip replacement. Clin Orthop Relat Res 2004;420:63-71.
Isiklar ZU, Demirors H, Akpinar S, et al: Two-stage treatment of chronic staphylococcal orthopaedic
implant-related infections using vancomycin impregnated PMMA spacer and rifampin containing antibiotic protocol. Bull Hosp Jt Dis 1999;58:79-85.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon