Orthopedic Adult Reconstructive Surgery MCQs & Review | Hip & Knee Arthroplasty Exam Prep
14 Apr 2026
50 min read
79 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Adult Reconstructive Surgery MCQs ...
00:00
Start Quiz
Question 1High Yield
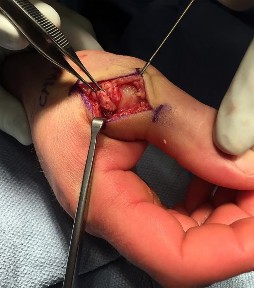
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?
Explanation
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block _the UCL with this type of injury._
Question 2High Yield
Figure 1 is the CT scan of a 12-month-old boy who has a neck injury from a motor vehicle accident. He is neurologically intact without any other injuries. Following successful closed reduction of the fracture, what is the best next step in management?

Explanation
■
The patient has sustained a displaced odontoid fracture through the dentocentral synchondrosis. Reduction of the fracture can usually be achieved by extending the neck under fluoroscopic control. An irreducible fracture may be successfully reduced by transoral digital manipulation. After closed reduction, immobilization in a Minerva cast, halo cast, or halo vest are good options.
A cervical collar will not adequately immobilize the upper cervical spine to maintain reduction of an unstable odontoid fracture. Anterior odontoid fixation or posterior C1-C2 instrumented arthrodesis should be reserved for irreducible fractures or a rare pediatric odontoid fracture nonunion.
The patient has sustained a displaced odontoid fracture through the dentocentral synchondrosis. Reduction of the fracture can usually be achieved by extending the neck under fluoroscopic control. An irreducible fracture may be successfully reduced by transoral digital manipulation. After closed reduction, immobilization in a Minerva cast, halo cast, or halo vest are good options.
A cervical collar will not adequately immobilize the upper cervical spine to maintain reduction of an unstable odontoid fracture. Anterior odontoid fixation or posterior C1-C2 instrumented arthrodesis should be reserved for irreducible fractures or a rare pediatric odontoid fracture nonunion.
Question 3High Yield
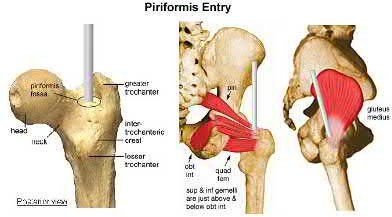
The greatest amount of iatrogenic injury to the piriformis tendon is associated with which of the following?
Explanation
There is an increased rate of injury to the piriformis tendon, medial femoral circumflex artery branches, gluteus minimus, and superior gluteal nerve branches are noted with the piriformis starting site. Increased injury to the gluteus medius is seen with a greater trochanteric starting point.
The referenced study by Dora et al noted increased injury to the piriformis tendon with a piriformis starting point (as compared to a more lateral insertion site).
The classic referenced article by Johnson et al notes that anterior placement of the starting point >6mm over the recommended start leads to increased hoop stresses and possible burst-type fractures.
The classic referenced study by Winquist et al reviewed their series of 520 femur fractures treated by antegrade nailing; they report a 99.1% union rate.
The referenced study by Dora et al noted increased injury to the piriformis tendon with a piriformis starting point (as compared to a more lateral insertion site).
The classic referenced article by Johnson et al notes that anterior placement of the starting point >6mm over the recommended start leads to increased hoop stresses and possible burst-type fractures.
The classic referenced study by Winquist et al reviewed their series of 520 femur fractures treated by antegrade nailing; they report a 99.1% union rate.
Question 4High Yield
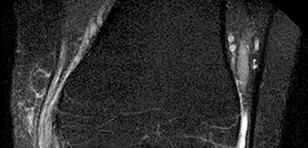
Figures 1 through 5 are the AP and lateral radiographs and MR images of a 16-year-old boy who has a 1-year history of low back pain. The pain bothers him only at night, and it awakens him from sleep. NSAIDs allow him to return to sleep. What is the most appropriate next step in treatment?


Explanation
■
The history and imaging are consistent with an osteoid osteoma of the posterior sacrum. Percutaneous ablation techniques have become the standard first-line treatment for most extremity lesions. Concern exists about the use of radiofrequency ablation (RFA) in spinal lesions because of the potential for thermal injury of adjacent neurovascular structures, particularly in the absence of intact cortex surrounding the lesion. RFA should be avoided when neurovascular structures would be within 1 cm of the electrode. As such, excision would be preferable. There is no role for chemotherapy or radiation therapy in the management of osteoid osteomas.
■
The history and imaging are consistent with an osteoid osteoma of the posterior sacrum. Percutaneous ablation techniques have become the standard first-line treatment for most extremity lesions. Concern exists about the use of radiofrequency ablation (RFA) in spinal lesions because of the potential for thermal injury of adjacent neurovascular structures, particularly in the absence of intact cortex surrounding the lesion. RFA should be avoided when neurovascular structures would be within 1 cm of the electrode. As such, excision would be preferable. There is no role for chemotherapy or radiation therapy in the management of osteoid osteomas.
Question 5High Yield
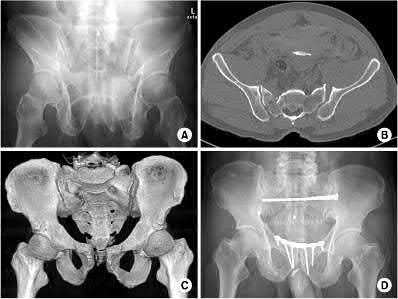
1250) Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?
Explanation
The posterior sacroiliac ligaments are not disrupted in an APC type II pelvic fracture.
Young and Burgess classification of pelvic ring injuries is largely based on the mechanism and energy of injury. An APC type I involves slight widening of
pubic symphysis and/or anterior sacroiliac (SI) joint. An APC II is a continuation of this force, and additionally involves a disrupted anterior SI joint, as well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Illustration A shows an APC-II injury pattern - (a) is an outlet radiograph, (b) is an axial CT cut, (c) is a 3-D CT cut, and (d) is a representative fixation construct.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Young and Burgess classification of pelvic ring injuries is largely based on the mechanism and energy of injury. An APC type I involves slight widening of
pubic symphysis and/or anterior sacroiliac (SI) joint. An APC II is a continuation of this force, and additionally involves a disrupted anterior SI joint, as well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Illustration A shows an APC-II injury pattern - (a) is an outlet radiograph, (b) is an axial CT cut, (c) is a 3-D CT cut, and (d) is a representative fixation construct.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 6High Yield
Slide 1 Slide 2
A 22-year-old man has experienced pain in his foot and ankle for 10 years. His radiographs are presented (Slide 1 and Slide 2). The foot is flexible, and pain is present in the sinus tarsi and along the medial border of the foot. With the subtalar joint held in a reduced neutral position, the forefoot is in 15° of supination. You attempt orthotic arch supports and when these do not
alleviate his pain, a brace is suggested. He refuses to wear a brace. You plan an osteotomy of the calcaneus with lengthening bone graft at the neck of the calcaneus (lateral column lengthening). The most common complication following this procedure is:
A 22-year-old man has experienced pain in his foot and ankle for 10 years. His radiographs are presented (Slide 1 and Slide 2). The foot is flexible, and pain is present in the sinus tarsi and along the medial border of the foot. With the subtalar joint held in a reduced neutral position, the forefoot is in 15° of supination. You attempt orthotic arch supports and when these do not
alleviate his pain, a brace is suggested. He refuses to wear a brace. You plan an osteotomy of the calcaneus with lengthening bone graft at the neck of the calcaneus (lateral column lengthening). The most common complication following this procedure is:
Explanation
This patient demonstrates the common finding of fixed forefoot varus associated with a flexible flatfoot deformity. It is likely that a gastrocnemius contracture is also present, but this is not always the case. Arthritis of the calcaneocuboid joint rarely occurs following a lengthening calcaneal osteotomy in an adult. C orrection of the forefoot varus is best accomplished with an opening wedge osteotomy of the medial cuneiform. Arthrodesis of the first tarsometatarsal joint may be performed in selected patients
with noted instability at this joint.
with noted instability at this joint.
Question 7High Yield
Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?

Explanation
No detailed explanation provided for this question.
Question 8High Yield
Slide 1
A 67-year-old obese patient presents for treatment of ankle pain. Twenty-five years ago, he underwent a total ankle replacement. He was asymptomatic for 15 years, and his symptoms have become intolerable. He has limited ankle motion, associated with pain in the ankle. His radiograph is presented (Slide). Which of the following is the preferred surgical procedure:
A 67-year-old obese patient presents for treatment of ankle pain. Twenty-five years ago, he underwent a total ankle replacement. He was asymptomatic for 15 years, and his symptoms have become intolerable. He has limited ankle motion, associated with pain in the ankle. His radiograph is presented (Slide). Which of the following is the preferred surgical procedure:
Explanation
Removal of the implant is necessary but will not be sufficient to alleviate pain from arthritis. In this obese patient, an arthrodesis is necessary. An extended hindfoot arthrodesis is only necessary when pain and arthritis are present in joints adjacent to the ankle. An ankle arthrodesis with interposition graft is sufficient.
Question 9High Yield
Which of the following statements best describes the relationship between tissue response to thermal capsulorrhaphy and the type of device used?
Explanation
Although radiofrequency devices and lasers differ fundamentally in the way they generate heat within a tissue, both classes of devices are capable of producing temperatures within the critical temperature range (65 to 75 degrees C) for collagen denaturation and subsequent tissue shrinkage. When it comes to cell viability and tissue response, heat is heat. Once critical temperatures are reached, cells will die at 45 degrees C, collagen will become denatured at 60 degrees C, and tissue ablation will occur at 100 degrees C no matter what the source of thermal energy. Therefore, claims of a better or different type of heat have little bearing on the biologic response of the tissue. Histologic, ultrastructural, and biomaterial alterations induced by laser and radiofrequency energy have been shown to be similar.
REFERENCES: Arnoczky SP, Aksan A: Thermal modification of connective tissues: Basic science considerations and clinical implications. J Am Acad Orthop Surg 2000;8:305-313.
Hayashi K, Markel MD: Thermal modification of joint capsule and ligamentous tissues: The use of thermal energy in sports medicine. Operative Techniques Sports Med 1998;6:120-125.
Naseef GS III, Foster TE, Trauner K, et al: The thermal properties of bovine joint capsule: The basic science of laser- and radiofrequency-induced capsular shrinkage. Am J Sports Med 1997;25:670-674.
REFERENCES: Arnoczky SP, Aksan A: Thermal modification of connective tissues: Basic science considerations and clinical implications. J Am Acad Orthop Surg 2000;8:305-313.
Hayashi K, Markel MD: Thermal modification of joint capsule and ligamentous tissues: The use of thermal energy in sports medicine. Operative Techniques Sports Med 1998;6:120-125.
Naseef GS III, Foster TE, Trauner K, et al: The thermal properties of bovine joint capsule: The basic science of laser- and radiofrequency-induced capsular shrinkage. Am J Sports Med 1997;25:670-674.
Question 10High Yield
What is the most likely cause of the deformity shown in Figures 39a through 39c?



Explanation
This is a Kirner deformity. Attributed to J. Kirner who described it in 1927, it is a rare congenital deformity of the distal phalanx of the small finger. It is often bilateral and sometimes familial. Radiographic appearance is characterized by narrow, apex-dorsal arching of the phalangeal shaft and a widened physis. The etiology is unknown, although several proposed mechanisms have proven unfounded with advanced imaging. This deformity usually is not associated with syndromes or other musculoskeletal abnormalities.
Clinically, the finger has a short distal phalangeal segment with a dorsally curved fingernail. Patients tend to seek an evaluation for this progressive deformity during adolescence. The deformity ceases to increase once a patient reaches skeletal maturity and the physis closes. This condition is frequently diagnosed as a partial growth arrest, but there is always a mysterious lack of a trauma history. Infection and inflammation are other possible causes, but laboratory studies and MRI do not show enhancement.
This deformity is largely cosmetic, although pain is occasionally reported. If patients find the deformity unacceptable, treatment is a palmarly based opening-wedge osteotomy. While this is an exceedingly rare condition, it is relevant for general orthopaedic surgeons to recognize the condition to avoid the consternation associated with misdiagnosis.
Vitamin D deficiency does not cause skeletal deformity in the hand. Frostbite typically is associated with wide, short phalanges with early growth arrest. Posttraumatic growth arrest occurs occasionally with a Seymour fracture but is most often a central or asymmetric arrest.
RECOMMENDED READINGS
5. [Dykes RG. Kirner's deformity of the little finger. J Bone Joint Surg Br. 1978 Feb;60(1):58-60. PubMed PMID: 627580.](http://www.ncbi.nlm.nih.gov/pubmed/627580)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/627580)
6. Khalid S, Khalid M, Zaheer S, Ahmad I, Ullah E. Kirner's Deformity Misdiagnosed as Fracture: A Case Report. Oman Med J. 2012 May;27(3):237-8. doi: 10.5001/omj.2012.53. PubMed PMID: 22811775.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22811775)
7. Lee J, Ahn JK, Choi SH, Koh EM, Cha HS. MRI findings in Kirner deformity: normal insertion of the flexor digitorum profundus tendon without soft-tissue enhancement. Pediatr Radiol. 2010 Sep;40(9):1572-5. doi: 10.1007/s00247-010-1628-4. Epub 2010 Mar 25. PubMed PMID: 20336287.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20336287)
Clinically, the finger has a short distal phalangeal segment with a dorsally curved fingernail. Patients tend to seek an evaluation for this progressive deformity during adolescence. The deformity ceases to increase once a patient reaches skeletal maturity and the physis closes. This condition is frequently diagnosed as a partial growth arrest, but there is always a mysterious lack of a trauma history. Infection and inflammation are other possible causes, but laboratory studies and MRI do not show enhancement.
This deformity is largely cosmetic, although pain is occasionally reported. If patients find the deformity unacceptable, treatment is a palmarly based opening-wedge osteotomy. While this is an exceedingly rare condition, it is relevant for general orthopaedic surgeons to recognize the condition to avoid the consternation associated with misdiagnosis.
Vitamin D deficiency does not cause skeletal deformity in the hand. Frostbite typically is associated with wide, short phalanges with early growth arrest. Posttraumatic growth arrest occurs occasionally with a Seymour fracture but is most often a central or asymmetric arrest.
RECOMMENDED READINGS
5. [Dykes RG. Kirner's deformity of the little finger. J Bone Joint Surg Br. 1978 Feb;60(1):58-60. PubMed PMID: 627580.](http://www.ncbi.nlm.nih.gov/pubmed/627580)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/627580)
6. Khalid S, Khalid M, Zaheer S, Ahmad I, Ullah E. Kirner's Deformity Misdiagnosed as Fracture: A Case Report. Oman Med J. 2012 May;27(3):237-8. doi: 10.5001/omj.2012.53. PubMed PMID: 22811775.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22811775)
7. Lee J, Ahn JK, Choi SH, Koh EM, Cha HS. MRI findings in Kirner deformity: normal insertion of the flexor digitorum profundus tendon without soft-tissue enhancement. Pediatr Radiol. 2010 Sep;40(9):1572-5. doi: 10.1007/s00247-010-1628-4. Epub 2010 Mar 25. PubMed PMID: 20336287.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20336287)
Question 11High Yield
A prospective outcome study is performed at a single institution to analyze the potential differences in treating intertrochanteric hip fractures with a plate/screw device versus an intramedullary device. No specific randomization is performed because an equal number of surgeons have preferences for the use of one of these devices and they are allowed to continue their preferred method. Hip- specific and general health-related outcome measures are used, an excellent follow-up rate of 85% of the patients at 2 years is accomplished, and there appears to be results that favor the intramedullary device but the confidence intervals are wide. This study would be considered to carry what level of evidence?
Explanation
**
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
Question 12High Yield
The magnitude of this deformity is directly affected by rotator cuff tear size.
Explanation
- Figure 59b is the radiograph of a 45-year-old man with acromiohumeral distance equal to 7 mm. He is able to actively raise his arm above shoulder level, has lateral arm pain, and abduction and external rotation weakness.
Question 13High Yield
Figures 1 and 2 are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared with traditional arthroscopic techniques when evaluating which outcome?








Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the two techniques.
Question 14High Yield
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
Explanation
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
1. Cortical thickening in the region of the lesion
2. Erosive metaphyseal lesion with loss of cortical integrity
3. Normal bony anatomy on radiographs
4. Diffuse articular erosion with loss of joint space
5. Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
6. Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
RESPONSES FOR QUESTIONS 57 THROUGH 62
1. Cortical thickening in the region of the lesion
2. Erosive metaphyseal lesion with loss of cortical integrity
3. Normal bony anatomy on radiographs
4. Diffuse articular erosion with loss of joint space
5. Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
6. Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
Question 15High Yield
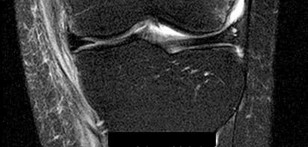
Figure 26 is a radiograph of an 11-year-old boy with insidious-onset anterior knee pain.
Explanation
- MRI
Question 16High Yield
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome?
Explanation
The only factor that is prognostic for outcomes is the quality of the reduction. None of the other factors has any effect on the outcome. Early range of motion or physical therapy may offer temporary effects, but these small advantages do not last beyond 3 months after surgery.
Question 17High Yield
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted.
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
Question 18High Yield
1242) A 32-year-old male sustains a closed head injury, a closed pelvic ring injury, as well as the bilateral open femoral fractures shown in Figures A-C. He remains borderline hypotensive with a base deficit of
4.9 after an exploratory laparatomy and splenectomy. After irrigation and debridement of his open fractures, what is the most appropriate treatment for this patient at this time?
4.9 after an exploratory laparatomy and splenectomy. After irrigation and debridement of his open fractures, what is the most appropriate treatment for this patient at this time?



Explanation
Figure A shows a complex pelvic ring injury, while Figures B and C show bilateral femur fractures. Appropriate treatment of an unstable, head-injured patient with the above injuries includes prompt, judicious external fixation of his bilateral femoral fractures and pelvic ring injury. The advantages of early fracture fixation in patients with multiple injuries have been challenged recently, particularly in patients with head injury. External fixation (EF) has been used to stabilize pelvic fractures after multiple injury. It potentially offers similar benefits to intramedullary nail (IMN) in long-bone fractures and may obviate some of the risks. EF is a viable alternative to attain temporary rigid stabilization in patients with multiple injuries. It is rapid, causes negligible blood loss, and can be followed safely by IMN when the patient is stabilized.
The referenced article by Scalea et al found that external fixation for femur fractures is a viable alternative to attain temporary rigid stabilization in patients with multiple injuries.
The referenced article by Scalea et al found that external fixation for femur fractures is a viable alternative to attain temporary rigid stabilization in patients with multiple injuries.
Question 19High Yield
What condition favors pollicization in hypoplasia of the thumb?
Explanation
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
Question 20High Yield
A 27-year-old man who was involved in a high-speed motor vehicle crash arrives at the trauma center with loss of consciousness, multiple posterior rib fractures, a left scapula body fracture, a left humerus fracture,
bilateral femoral shaft fractures, and an open right ankle fracture-dislocation. Initial vital signs are a blood pressure of 88/50 mm Hg, a pulse of 120 bpm, and respirations of 22/min. His injury severity score is 28 and lactate levels are 2.7. CT scans of the head and abdomen are negative for hemorrhage, and after initial resuscitation the patient is cleared for surgery. Initial orthopaedic management should consist of débridement and irrigation of the right ankle with
bilateral femoral shaft fractures, and an open right ankle fracture-dislocation. Initial vital signs are a blood pressure of 88/50 mm Hg, a pulse of 120 bpm, and respirations of 22/min. His injury severity score is 28 and lactate levels are 2.7. CT scans of the head and abdomen are negative for hemorrhage, and after initial resuscitation the patient is cleared for surgery. Initial orthopaedic management should consist of débridement and irrigation of the right ankle with



Explanation
No detailed explanation provided for this question.
Question 21High Yield
Osteomyelitis with 72 hours of symptoms
Explanation
- Normal bony anatomy on radiographs
Question 22High Yield
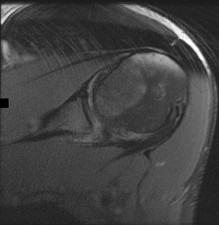
Figure 1 is the MRI scan of a 19-year-old man who has an acute anterior shoulder dislocation. The bony fragment occupies 10% of the glenoid articular surface. What is the most appropriate treatment?
---
---
Explanation
The MRI scan shows a bony Bankart lesion involving <20% of the glenoid joint surface. A recent series reported high success rates after arthroscopic treatment when the defect is incorporated into the repair. Anterior bony deficiencies occupying >25% to >30% of the glenoid joint surface treated with soft-tissue repair only are associated with high recurrence rates. In these patients, an open or arthroscopic coracoid transfer or structural iliac crest graft should be considered. Open reduction and internal fixation has been reported for treatment of large acute glenoid rim fractures but is not recommended for recurrent anterior shoulder instability in the setting of a 10% glenoid rim fracture.
Question 23High Yield
Figure 1 is the weight-bearing PA radiograph of a 67-year-old woman undergoing total knee arthroplasty (TKA). During surgery, it is observed that she remains tight laterally in extension only while trialing components. What is the most appropriate next step?
Explanation
Gap balance during TKA is best achieved with an understanding of which structures contribute to which gaps. Studies have shown that the popliteus tendon contributes to flexion gap tightness laterally and that the IT band contributes to extension gap tightness laterally.
49
Resecting additional femur would raise the joint line and would affect both the medial and lateral extension gaps equally. Release of the posterior capsule would also affect both gaps equally. Release of the lateral collateral ligament would likely require an increased level of constraint and, although it would affect only the lateral extension and flexion gaps, it is not the most appropriate next step.
49
Resecting additional femur would raise the joint line and would affect both the medial and lateral extension gaps equally. Release of the posterior capsule would also affect both gaps equally. Release of the lateral collateral ligament would likely require an increased level of constraint and, although it would affect only the lateral extension and flexion gaps, it is not the most appropriate next step.
Question 24High Yield
Which of the following precautionary measures should be taken to prevent a periprosthetiCfracture when removing components from a patient with a previous compression hip screw:
Explanation
Stress risers are generated when a screw is removed from the femur, weakening the bone for at least 4 weeks. Larger defects (50%) of the cortical width can reduce torsional strength up to 44%. Bypassing the defect by two cortical diameters with a cemented stem doubles the boneâs strength
Question 25High Yield
In cases of subacute scaphoid-lunate ligament injury with no arthrosis, all of the following are acceptable options except:
Explanation
In cases of subacute scaphoid-lunate ligament injury without arthrosis, it is acceptable to attempt reconstruction with bone anchors, allograft ligament repair, capsulodesis, bone-ligament-bone autograft, and the RASL procedure with a Herbert screw. In the presence of localized arthritis, one might consider one of the limited wrist fusions such as scaphotrapeziotrapezoid fusion.
Question 26High Yield
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?
---
---

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 27High Yield
An active 72-year-old man underwent a right hybrid total hip arthroplasty for osteoarthritis 4 years ago. His hip has functioned well until approximately 8 months ago. He now reports activity-related proximal thigh pain and groin pain. A current radiograph is shown in Figure 43a. A radiograph obtained prior to the onset of symptoms is shown in Figure 43b. What is the most likely cause of his symptoms?

Explanation
DISCUSSION: The radiograph shows a loose femoral component. The implant has debonded showing a radiolucent line at the lateral shoulder (zone 1), and also increased radiolucency at the bone cement interface medially. The patient’s symptoms are mechanical in nature with activity-related pain. Symptoms are not characteristic of psoas tendon irritation. Although osteolysis is present, in the absence of fracture it is generally asymptomatic. Additionally, in this patient the osteolysis involving the proximal femur is much more likely to be secondary to cement particulate debris and less likely related to polyethylene wear particles.
REFERENCES: Jasty M, Maloney WJ, Bragdon CR, et al: The initiation of failure in cemented femoral components of hip arthroplasties. J Bone Joint Surg Br 1991;73:551-558.
Kwong LM, Jasty M, Mulroy RD, et al: The histology of the radiolucent line. J Bone Joint Surg Br 1992;74:67-73.
Verdonschot N, Tanck E, Huiskes R: Effects of prosthesis surface roughness on the failure process of cemented hip implants after stem-cement debonding. J Biomed Mater Res 1998;42:554-559.
Figure 44
REFERENCES: Jasty M, Maloney WJ, Bragdon CR, et al: The initiation of failure in cemented femoral components of hip arthroplasties. J Bone Joint Surg Br 1991;73:551-558.
Kwong LM, Jasty M, Mulroy RD, et al: The histology of the radiolucent line. J Bone Joint Surg Br 1992;74:67-73.
Verdonschot N, Tanck E, Huiskes R: Effects of prosthesis surface roughness on the failure process of cemented hip implants after stem-cement debonding. J Biomed Mater Res 1998;42:554-559.
Figure 44
Question 28High Yield
A 4-week-old girl is referred for an evaluation of her hips. She was the product of a full-term uncomplicated pregnancy. She was delivered by Cesarean section because of breech presentation. She has an older sister treated for developmental dysplasia of the hip (DDH). On examination her hips are stable on Barlow and Ortolani testing. Her primary care practitioner obtained a bilateral dynamic hip ultrasonography. On the ultrasound exam, both hips are stable with stress. The alpha angles are 53°, and there is 48% femoral head coverage. What is the best next step in management?
Explanation
■
This child has a normal exam and significant risk factors for DDH (breech presentation and + family history). The ultrasound shows mildly decreased alpha angles or Graf type IIa hips. At age 4 weeks, this would be considered physiologic immaturity. Most of these hips will improve without treatment. Repeating the ultrasound in 4-6 weeks will either show improvement, in which case no treatment will be required, or worsening on the repeat study, for which treatment can be instituted.
Although application of a Pavlik harness could be instituted, given the natural history of possible improvement, this would be overtreatment. The same is true for closed reduction with spica cast application. Because there are significant risk factors, sending the child out without treatment or follow-up, could result in a missed opportunity to treat, if indeed there is worsening.
This child has a normal exam and significant risk factors for DDH (breech presentation and + family history). The ultrasound shows mildly decreased alpha angles or Graf type IIa hips. At age 4 weeks, this would be considered physiologic immaturity. Most of these hips will improve without treatment. Repeating the ultrasound in 4-6 weeks will either show improvement, in which case no treatment will be required, or worsening on the repeat study, for which treatment can be instituted.
Although application of a Pavlik harness could be instituted, given the natural history of possible improvement, this would be overtreatment. The same is true for closed reduction with spica cast application. Because there are significant risk factors, sending the child out without treatment or follow-up, could result in a missed opportunity to treat, if indeed there is worsening.
Question 29High Yield
Figures below demonstrate the radiographs obtained from a 63-year-old man who had right total hip
arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals a normal gait and painless range of motion with flexion of 70°, extension of 0°, internal rotation of 20°, external rotation of 20°, abduction of 10°, and adduction of 10°. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals a normal gait and painless range of motion with flexion of 70°, extension of 0°, internal rotation of 20°, external rotation of 20°, abduction of 10°, and adduction of 10°. His erythrocyte sedimentation rate and C-reactive protein level are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
Explanation
This patient presents with HO 4 months after undergoing THA. Symptomatic HO may complicate nearly
7% of primary THA cases. Improvement in pain is expected within 6 months, and most patients will not need surgical treatment. Surgical excision may be warranted for symptomatic patients after full maturation of the HO, usually 6 to 18 months after the surgery. Patients can be followed with repeated serum alkaline phosphatase levels, which are elevated initially and should return to normal upon maturation of the HO. Alternatively, a bone scan can show decreased activity after the HO has matured. Twenty-five milligrams of indomethacin 3 times daily for 6 weeks or 1 dose of irradiation at 700 to 800 Gy is effective in the prevention of HO but not for the treatment of established HO.
7% of primary THA cases. Improvement in pain is expected within 6 months, and most patients will not need surgical treatment. Surgical excision may be warranted for symptomatic patients after full maturation of the HO, usually 6 to 18 months after the surgery. Patients can be followed with repeated serum alkaline phosphatase levels, which are elevated initially and should return to normal upon maturation of the HO. Alternatively, a bone scan can show decreased activity after the HO has matured. Twenty-five milligrams of indomethacin 3 times daily for 6 weeks or 1 dose of irradiation at 700 to 800 Gy is effective in the prevention of HO but not for the treatment of established HO.
Question 30High Yield
Which organism is most likely responsible for a periprosthetic shoulder infection?
Explanation
_Propionibacterium acnes (P. acnes) has emerged as the most likely cause of infection associated with shoulder arthroplasty. A gram-positive, aerotolerant anaerobic rod that lives in the skin, not on the skin, it is more difficult to diagnose and treat than more conventional organisms. As an anaerobe, it does not create pus, but rather a turbid fluid, and is associated with humeral stem loosening when a clinically significant infection is present. P. acnes remains sensitive to most antibiotics, and, although some resistance to clindamycin has been reported, highly resistant strains have not yet evolved._
_P. acnes often remains a diagnostic challenge. Conventional tests measuring C-reactive protein, sedimentation rate, Interleukin-6, and white cell counts are not highly accurate. Even aspiration and culture of the affected joint is not reliable. Cultures should be kept at least 2 weeks to avoid false-negative results with slow-growing organisms. Some investigators have advocated diagnostic arthroscopy with biopsy as another diagnostic alternative._
Treatment of shoulder replacements infected with _P. acnes_ is evolving. For shoulders associated with low clinical suspicion for infection but an unexpected positive culture result, treatment can be 1-stage reconstruction without an extended course of intravenous antibiotics. Most commonly, an infected shoulder arthroplasty is treated with a 2-stage reconstruction similar to that seen in the setting of hip and knee arthroplasty.
RECOMMENDED READINGS
23. Kelly JD 2nd, Hobgood ER. Positive culture rate in revision shoulder arthroplasty. Clin Orthop Relat Res. 2009 Sep;467(9):2343-8. doi: 10.1007/s11999-009-0875-x. Epub 2009 May 12. PubMed PMID:
[19434469/. ](http://www.ncbi.nlm.nih.gov/pubmed/19434469)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19434469)
24. Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, Dicarlo E, Brause BD, Warren RF. Propionibacterium acnes infection after shoulder arthroplasty: a diagnostic challenge. J Shoulder Elbow Surg. 2010 Mar;19(2):303-7. doi: 10.1016/j.jse.2009.07.065. Epub 2009 Nov 1. PubMed PMID:
[19884021/. ](http://www.ncbi.nlm.nih.gov/pubmed/19884021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884021)
25. Grosso MJ, Sabesan VJ, Ho JC, Ricchetti ET, Iannotti JP. Reinfection rates after 1-stage revision shoulder arthroplasty for patients with unexpected positive intraoperative cultures. J Shoulder Elbow Surg. 2012 Jun;21(6):754-8. doi: 10.1016/j.jse.2011.08.052. Epub 2012 Feb 3. PubMed PMID:
[22305921/. ](http://www.ncbi.nlm.nih.gov/pubmed/22305921)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22305921)
26. [Pottinger P, Butler-Wu S, Neradilek MB, Merritt A, Bertelsen A, Jette JL, Warme WJ, Matsen FA 3rd. Prognostic factors for bacterial cultures positive for Propionibacterium acnes and other organisms in a large series of revision shoulder arthroplasties performed for stiffness, pain, or loosening. J Bone Joint Surg Am. 2012 Nov 21;94(22):2075-83. doi: 10.2106/JBJS.K.00861.](http://www.ncbi.nlm.nih.gov/pubmed/23172325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23172325)
_P. acnes often remains a diagnostic challenge. Conventional tests measuring C-reactive protein, sedimentation rate, Interleukin-6, and white cell counts are not highly accurate. Even aspiration and culture of the affected joint is not reliable. Cultures should be kept at least 2 weeks to avoid false-negative results with slow-growing organisms. Some investigators have advocated diagnostic arthroscopy with biopsy as another diagnostic alternative._
Treatment of shoulder replacements infected with _P. acnes_ is evolving. For shoulders associated with low clinical suspicion for infection but an unexpected positive culture result, treatment can be 1-stage reconstruction without an extended course of intravenous antibiotics. Most commonly, an infected shoulder arthroplasty is treated with a 2-stage reconstruction similar to that seen in the setting of hip and knee arthroplasty.
RECOMMENDED READINGS
23. Kelly JD 2nd, Hobgood ER. Positive culture rate in revision shoulder arthroplasty. Clin Orthop Relat Res. 2009 Sep;467(9):2343-8. doi: 10.1007/s11999-009-0875-x. Epub 2009 May 12. PubMed PMID:
[19434469/. ](http://www.ncbi.nlm.nih.gov/pubmed/19434469)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19434469)
24. Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, Dicarlo E, Brause BD, Warren RF. Propionibacterium acnes infection after shoulder arthroplasty: a diagnostic challenge. J Shoulder Elbow Surg. 2010 Mar;19(2):303-7. doi: 10.1016/j.jse.2009.07.065. Epub 2009 Nov 1. PubMed PMID:
[19884021/. ](http://www.ncbi.nlm.nih.gov/pubmed/19884021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884021)
25. Grosso MJ, Sabesan VJ, Ho JC, Ricchetti ET, Iannotti JP. Reinfection rates after 1-stage revision shoulder arthroplasty for patients with unexpected positive intraoperative cultures. J Shoulder Elbow Surg. 2012 Jun;21(6):754-8. doi: 10.1016/j.jse.2011.08.052. Epub 2012 Feb 3. PubMed PMID:
[22305921/. ](http://www.ncbi.nlm.nih.gov/pubmed/22305921)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22305921)
26. [Pottinger P, Butler-Wu S, Neradilek MB, Merritt A, Bertelsen A, Jette JL, Warme WJ, Matsen FA 3rd. Prognostic factors for bacterial cultures positive for Propionibacterium acnes and other organisms in a large series of revision shoulder arthroplasties performed for stiffness, pain, or loosening. J Bone Joint Surg Am. 2012 Nov 21;94(22):2075-83. doi: 10.2106/JBJS.K.00861.](http://www.ncbi.nlm.nih.gov/pubmed/23172325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23172325)
Question 31High Yield
A 10-year-old girl fell from her bike and now reports pain and swelling in the left knee and pain with weight bearing. Examination reveals a left knee effusion and pain with range of motion. A radiograph is shown in Figure 85. Treatment should consist of
Explanation
DISCUSSION: The child has a type III tibial spine avulsion fracture. When the avulsed fragment is completely displaced, the preferred treatment is open or arthroscopic reduction of the fragment and internal fixation with sutures or screws. Type I fractures are nondisplaced and can be treated with a long leg cast; type II fractures are hinged and can be treated in a long leg cast if closed reduction is successful. Many patients have some objective anterior cruciate ligament laxity after a tibial spine avulsion fracture; however, with adequate treatment most patients do not have symptomatic laxity.
REFERENCES: Mah JY, Adili A, Otsuka NY, et al: Follow-up study of arthroscopic reduction and fixation of type III tibial-eminence fractures. J Pediatr Orthop 1998; 18:475-477.
McLennen JG: Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 1995;15:59-62.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
72 • American Academy of Orthopaedic Surgeons
DISCUSSION: The child has a type III tibial spine avulsion fracture. When the avulsed fragment is completely displaced, the preferred treatment is open or arthroscopic reduction of the fragment and internal fixation with sutures or screws. Type I fractures are nondisplaced and can be treated with a long leg cast; type II fractures are hinged and can be treated in a long leg cast if closed reduction is successful. Many patients have some objective anterior cruciate ligament laxity after a tibial spine avulsion fracture; however, with adequate treatment most patients do not have symptomatic laxity.
REFERENCES: Mah JY, Adili A, Otsuka NY, et al: Follow-up study of arthroscopic reduction and fixation of type III tibial-eminence fractures. J Pediatr Orthop 1998; 18:475-477.
McLennen JG: Lessons learned after second-look arthroscopy in type III fractures of the tibial spine. J Pediatr Orthop 1995;15:59-62.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
72 • American Academy of Orthopaedic Surgeons
Question 32High Yield
The knee arthroplasty type associated with the highest 5-year revision rate is
Explanation
52
Revision rates for UKA at 10 years are lower than 5% at specialty centers. However, the 10-year revision rate associated with UKA in registries such as the National Joint Registry for England and Wales is 2 to 3 times that of TKA. Among partial knee replacements, patellofemoral arthroplasty is associated with the highest revision rate at every time interval.
Revision rates for UKA at 10 years are lower than 5% at specialty centers. However, the 10-year revision rate associated with UKA in registries such as the National Joint Registry for England and Wales is 2 to 3 times that of TKA. Among partial knee replacements, patellofemoral arthroplasty is associated with the highest revision rate at every time interval.
Question 33High Yield
Figures 85a through 85c are the sagittal and axial CT scans and sagittal T2 MR image of a 21-year-old man who was thrown from his motocross bike earlier in the day. He now has significant low-back pain; however, he is neurologically intact and has no trouble voiding urine. A standing plain radiograph obtained the next day is shown in Figure 85d. Treatment should involve
A
B
C D
A
B
C D




Explanation
Disruption of the posterior ligamentous complex is an important determinant of the stability of a burst fracture. This patient is neurologically intact and his MR images do not reveal posterior ligamentous complex (PLC) disruption. The standing radiograph confirms that overall alignment is acceptably and relatively preserved. Nonsurgical treatment with or without a brace is acceptable in this scenario; however, the patient should not be cleared to resume full activity until fracture healing, which may be as long as 3 months after the date of injury. Anterior or posterior surgery should be reserved for patients with PLC disruption, neurological injury, or, in some cases, multiple trauma.
RECOMMENDED READINGS
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16227897)
[Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15905761)
RESPONSES FOR QUESTIONS 86 THROUGH 89
1. Proximal junctional kyphosis (PJK)
2. Adjacent segment degeneration
3. Intraoperative neurological injury
4. Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
RECOMMENDED READINGS
[Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[View ](http://www.ncbi.nlm.nih.gov/pubmed/12728024)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12728024)
[Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Zeiller SC, Anderson DG, Bono CM, Stock GH, Brown AK, Kuklo T, Oner FC. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine (Phila Pa 1976). 2005 Oct 15;30(20):2325-33. PubMed PMID: 16227897. ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16227897)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16227897)
[Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA Jr, Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005 Jun;18(3):209-15. PubMed PMID: 15905761.](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[View ](http://www.ncbi.nlm.nih.gov/pubmed/15905761)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15905761)
RESPONSES FOR QUESTIONS 86 THROUGH 89
1. Proximal junctional kyphosis (PJK)
2. Adjacent segment degeneration
3. Intraoperative neurological injury
4. Postsurgical wound infection
Please select the complication listed above that most commonly is associated with a clinical scenario described below.
Question 34High Yield
Assuming that the fracture shown in this radiograph (Figure


Explanation
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous _pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints._
Question 35High Yield
Figures 1 through 5 show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old
collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain
with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. Approximately what percentage of asymptomatic
athletes have cam deformities of the hip?
collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain
with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. Approximately what percentage of asymptomatic
athletes have cam deformities of the hip?
Explanation
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 36High Yield
The most common risk factors for stress fractures is:
Explanation
Numerous risk factors for stress fracture exist. Most commonly, the scenario is doing âtoo much too soon.â Survey data have shown 86% of runners suffering stress fracture have had a change in duration, frequency, or intensity of training immediately prior to injury. The best independent predictors for stress fracture development in women appear to be age of menarche and calf girth
Question 37High Yield
Figures 1 through 3 show the CT and radiographs of a 45-year-old woman who has low back pain and severe left leg pain in the L5 distribution that is not responsive to nonoperative management (physical therapy, epidural injections, pain medications) for 9 months. What is an appropriate treatment option for this patient?

Explanation
■
The figures show a grade 1 spondylolisthesis at L4-L5 along with a left sided facet cyst in a patient with ongoing symptoms despite nonoperative management. A lumbar decompression with a fusion would be an appropriate treatment option in this patient. There is no evidence in the literature for a lateral lumbar interbody fusion without directly decompressing the spinal canal for treatment of spondylolisthesis in the presence of a large facet cyst. Such procedures have been shown to be successful for treatment in the presence of spinal stenosis from ligament hypertrophy, disk bulge, foraminal stenosis. However, there is no evidence for their effectiveness in the presence of a large facet cyst. Similarly facet cyst aspiration has no evidence for treatment of this pathology. A facetectomy and cyst removal may adequately decompress the L4-L5 level. However, this is likely to create further instability in the presence of a spondylolisthesis.
The figures show a grade 1 spondylolisthesis at L4-L5 along with a left sided facet cyst in a patient with ongoing symptoms despite nonoperative management. A lumbar decompression with a fusion would be an appropriate treatment option in this patient. There is no evidence in the literature for a lateral lumbar interbody fusion without directly decompressing the spinal canal for treatment of spondylolisthesis in the presence of a large facet cyst. Such procedures have been shown to be successful for treatment in the presence of spinal stenosis from ligament hypertrophy, disk bulge, foraminal stenosis. However, there is no evidence for their effectiveness in the presence of a large facet cyst. Similarly facet cyst aspiration has no evidence for treatment of this pathology. A facetectomy and cyst removal may adequately decompress the L4-L5 level. However, this is likely to create further instability in the presence of a spondylolisthesis.
Question 38High Yield
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
The treatment of choice for closed diaphyseal femoral fractures in adults is reamed intramedullary nailing with static interlocking. Reaming allows placement of a larger, stronger implant and offers better healing rates than unreamed nailing. Static interlocking ensures that there is no loss of reduction because of underappreciated fracture lines or comminution.
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 39High Yield
A right-hand-dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
DISCUSSION:
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on
the radial tuberosity.
DISCUSSION:
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on
the radial tuberosity.
Question 40High Yield
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
FOR QUESTIONS 108 THROUGH 110:**_
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 41High Yield
A 24-year-old right-hand-dominant professional baseball pitcher has valgus extension overload (VEO) syndrome of the right elbow, as seen in Figure 7. Which letter in the figure corresponds to the typical area of osteophyte formation in this condition?

Explanation
VEO most commonly is seen in throwers for whom valgus stress across the elbow causes impingement of the posteromedial olecranon tip against the medial wall of the olecranon fossa. With repeated impingement, a bony osteophyte may grow on the olecranon at the site of impingement in this posteromedial region of the olecranon. Bony growth within the olecranon
fossa also has been seen. The distinction between this condition and ulnar collateral ligament injury is difficult to make, but VEO often can be distinguished from UCL injury by determining the exact location of pain a patient experiences. With VEO, the pain typically occurs with direct palpation of the posterior medial tip of the olecranon. The valgus extension overload provocative test also aids in diagnosis. A supervised physical therapy program and arthroscopic surgical decompression when nonsurgical treatment is unsuccessful are typical treatments for this condition.
Locations C and D represent the origin and insertion, respectively, of the elbow medial collateral ligament (MCL) structure, and, although associated MCL pathology can exist in the setting of VEO syndrome, osteophyte formation is not typical in these areas. Location A is the radial head, and although the radiocapitellar joint is a known secondary stabilizer of elbow valgus stress, osteophyte formation in this area is less likely in this clinical scenario.
RECOMMENDED READINGS
8. [Reddy AS, Kvitne RS, Yocum LA, Elattrache NS, Glousman RE, Jobe FW. Arthroscopy of the elbow: a long-term clinical review. Arthroscopy. 2000 Sep;16(6):588-94. ](http://www.ncbi.nlm.nih.gov/pubmed/10976118)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976118)
9. [Andrews JR, Craven WM. Lesions of the posterior compartment of the elbow. Clin Sports Med. 1991 Jul;10(3):637-52. Review. PubMed PMID: 1868565.](http://www.ncbi.nlm.nih.gov/pubmed/1868565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1868565)
10. [Wilson FD, Andrews JR, Blackburn TA, McCluskey G. Valgus extension overload in the pitching elbow. Am J Sports Med. 1983 Mar-Apr;11(2):83-8. ](http://www.ncbi.nlm.nih.gov/pubmed/6846685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6846685)
fossa also has been seen. The distinction between this condition and ulnar collateral ligament injury is difficult to make, but VEO often can be distinguished from UCL injury by determining the exact location of pain a patient experiences. With VEO, the pain typically occurs with direct palpation of the posterior medial tip of the olecranon. The valgus extension overload provocative test also aids in diagnosis. A supervised physical therapy program and arthroscopic surgical decompression when nonsurgical treatment is unsuccessful are typical treatments for this condition.
Locations C and D represent the origin and insertion, respectively, of the elbow medial collateral ligament (MCL) structure, and, although associated MCL pathology can exist in the setting of VEO syndrome, osteophyte formation is not typical in these areas. Location A is the radial head, and although the radiocapitellar joint is a known secondary stabilizer of elbow valgus stress, osteophyte formation in this area is less likely in this clinical scenario.
RECOMMENDED READINGS
8. [Reddy AS, Kvitne RS, Yocum LA, Elattrache NS, Glousman RE, Jobe FW. Arthroscopy of the elbow: a long-term clinical review. Arthroscopy. 2000 Sep;16(6):588-94. ](http://www.ncbi.nlm.nih.gov/pubmed/10976118)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976118)
9. [Andrews JR, Craven WM. Lesions of the posterior compartment of the elbow. Clin Sports Med. 1991 Jul;10(3):637-52. Review. PubMed PMID: 1868565.](http://www.ncbi.nlm.nih.gov/pubmed/1868565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1868565)
10. [Wilson FD, Andrews JR, Blackburn TA, McCluskey G. Valgus extension overload in the pitching elbow. Am J Sports Med. 1983 Mar-Apr;11(2):83-8. ](http://www.ncbi.nlm.nih.gov/pubmed/6846685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6846685)
Question 42High Yield
A patient with a severe nickel allergy and degenerative joint disease of the hip would be best served by which of the following prosthetic options?
Explanation
DISCUSSION: Nickel is present in cobalt-chrome and stainless steel alloys used in orthopaedic surgery; therefore, these materials are not well suited for nickel-sensitive patients. Nickel is not present in titanium alloys or in ceramic components. Titanium is therefore the material of choice for the femoral and acetabular component.
Titanium is a poor option for the femoral head due to its susceptibility to abrasive wear. Titanium is also poorly suited to cemented applications in hip arthroplasty because it is less stiff than cobalt-chrome (and stainless steel), and therefore transmits greater stresses to the cement column. Titanium’s poor abrasion resistance can also leave the component susceptible to increased abrasive wear in the event of loosening and micromotion. Therefore, of the options available, a cementless titanium stem and socket with a ceramic head is the best choice. In nickel-sensitive total knee arthroplasty patients, cemented oxidized zirconium femoral components can be used in place of cobalt- chrome, and titanium tibial components (press-fit or cemented) have been used with success.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
Titanium is a poor option for the femoral head due to its susceptibility to abrasive wear. Titanium is also poorly suited to cemented applications in hip arthroplasty because it is less stiff than cobalt-chrome (and stainless steel), and therefore transmits greater stresses to the cement column. Titanium’s poor abrasion resistance can also leave the component susceptible to increased abrasive wear in the event of loosening and micromotion. Therefore, of the options available, a cementless titanium stem and socket with a ceramic head is the best choice. In nickel-sensitive total knee arthroplasty patients, cemented oxidized zirconium femoral components can be used in place of cobalt- chrome, and titanium tibial components (press-fit or cemented) have been used with success.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
Question 43High Yield
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex.
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 44High Yield
Hornerâs syndrome includes all of the following except:
Explanation
Hornerâs syndrome is caused by disruption of sympathetic innervation and is characterized by enophthalmosis, not exophthalmosis. Other symptoms include anhidrosis, miosis, and ptosis.
Question 45High Yield
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
Explanation
DISCUSSION: The purpose of this question is to draw attention to the early risks of therapeutic anticoagulation that will be instituted by an intensivist or pulmonologist to treat a life-threatening pulmonary embolus. The temporary vena cava filter is a recent innovation but will effectively reduce the risk of further pulmonary emboli. This requires reversal of anticoagulation for safe insertion of the filter and creates a safe situation for additional surgical solutions. Sciatic nerve compromise was caused by the expanding hematoma in this patient, which could be mitigated by exploration both to assess the nerve and to remove a large hematoma that presents its own long- term risks.
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, [www.aaos.org/research/guidelines/](http://www.aaos.org/research/guidelines/) PEguide.asp
DISCUSSION: The purpose of this question is to draw attention to the early risks of therapeutic anticoagulation that will be instituted by an intensivist or pulmonologist to treat a life-threatening pulmonary embolus. The temporary vena cava filter is a recent innovation but will effectively reduce the risk of further pulmonary emboli. This requires reversal of anticoagulation for safe insertion of the filter and creates a safe situation for additional surgical solutions. Sciatic nerve compromise was caused by the expanding hematoma in this patient, which could be mitigated by exploration both to assess the nerve and to remove a large hematoma that presents its own long- term risks.
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, [www.aaos.org/research/guidelines/](http://www.aaos.org/research/guidelines/) PEguide.asp
Question 46High Yield
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them?
Explanation
DISCUSSION: ACL injuries are five to eight times more common in young women. The highest incidence is associated with basketball and soccer. These sports require rapid directional and rotational changes. Use of neuromuscular training programs has not been associated with a decrease in ACL injuries. It is recommended that there be more frequent rests. ACL injuries are commonly associated with meniscal injury.
REFERENCES: Shea KG: ACL Injury: Epidemiology and Prevention Presented at Sports Related Injuries in the Skeletally Mature Athlete. POSNA: One Day Course, 2008.
Millett PJ, Willis AA, Warren RF: Associated injuries in pediatric and adolescent anterior cruciate
ligament tears: Does a delay in treatment increase the risk of meniscal tears? Arthroscopy 2002; 18:955- 959.
DISCUSSION: ACL injuries are five to eight times more common in young women. The highest incidence is associated with basketball and soccer. These sports require rapid directional and rotational changes. Use of neuromuscular training programs has not been associated with a decrease in ACL injuries. It is recommended that there be more frequent rests. ACL injuries are commonly associated with meniscal injury.
REFERENCES: Shea KG: ACL Injury: Epidemiology and Prevention Presented at Sports Related Injuries in the Skeletally Mature Athlete. POSNA: One Day Course, 2008.
Millett PJ, Willis AA, Warren RF: Associated injuries in pediatric and adolescent anterior cruciate
ligament tears: Does a delay in treatment increase the risk of meniscal tears? Arthroscopy 2002; 18:955- 959.
Question 47High Yield
A 34-year-old female is involved in a high-speed motor vehicle collision and sustains a traumatic proximal forearm amputation. She successfully undergoes debridement and closure, and six weeks later, is fitted with her temporary prosthesis. In order to optimize her
outcomes upon returning to work as a secretary, which of the following is recommended?
outcomes upon returning to work as a secretary, which of the following is recommended?

Explanation
Upper extremity trauma has serious, acute psychological effects that can linger long after the physical injury. These effects may negatively affect patient-reported outcomes, and may also be associated with worsening pain complaints. Coping and stress management techniques can be reviewed with formal psychological counseling, and should be offered to all patients who have underwent an amputation.
Richards et al surveyed 34 patients who had emergency upper extremity surgery and found high levels of psychological distress in patients, including 29% with high levels of both depression and post-traumatic stress disorder (PTSD). They also found that disability was strongly related to pain, depression, and PTSD symptoms.
Mallette et al assessed the attitudes of hand surgery patients and hand surgeons regarding psychologic influences on illness and compared their attitudes with those of the general population. They found that surgeons underestimated the openness of patients to discuss psychological issues and that patients believed in the strong effect of psychologic factors on healing and pain.
Illustration A shows a myoelectric prosthesis in a military veteran. Incorrect Answers:
Answer 1: Formal function capacity testing is not typically necessary unless
Workers' Compensation is involved or formal disability proceedings occur. Answer 2: Final prosthetic fitting is not necessary for full release.
Answer 3: Prosthetic use will vary according to needs and patient factors such as pain.
Answer 4: Return to work does not have to wait for full return of elbow range of motion.
Richards et al surveyed 34 patients who had emergency upper extremity surgery and found high levels of psychological distress in patients, including 29% with high levels of both depression and post-traumatic stress disorder (PTSD). They also found that disability was strongly related to pain, depression, and PTSD symptoms.
Mallette et al assessed the attitudes of hand surgery patients and hand surgeons regarding psychologic influences on illness and compared their attitudes with those of the general population. They found that surgeons underestimated the openness of patients to discuss psychological issues and that patients believed in the strong effect of psychologic factors on healing and pain.
Illustration A shows a myoelectric prosthesis in a military veteran. Incorrect Answers:
Answer 1: Formal function capacity testing is not typically necessary unless
Workers' Compensation is involved or formal disability proceedings occur. Answer 2: Final prosthetic fitting is not necessary for full release.
Answer 3: Prosthetic use will vary according to needs and patient factors such as pain.
Answer 4: Return to work does not have to wait for full return of elbow range of motion.
Question 48High Yield
Figures 1 through 3 depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a
concern.
81
concern.
81
Question 49High Yield
Figures 27a and 27b are the radiographs of a 2-month-old with a swollen ankle and abdominal bruising.
Explanation
- Plain radiographs
Question 50High Yield
Figure 61
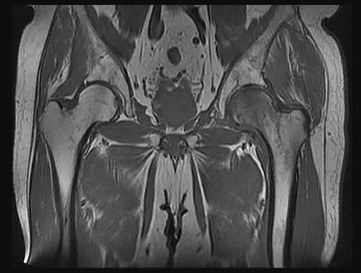
Explanation
- Transient osteoporosis of the hip_
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon