Management of Arterial Thrombosis and Special Vascular Disorders of the Hand
Key Takeaway
Acute arterial thrombosis in the hand threatens digital survival and requires prompt evaluation. Diagnosis relies on the Allen test, Doppler studies, and arteriography. While generalized vasospasm may respond to intra-arterial medications or sympathetic blocks, persistent ischemia necessitates microsurgical intervention. Resection of the thrombosed arterial segment followed by reversed interpositional vein grafting restores perfusion and prevents irreversible tissue necrosis.
Introduction to Special Hand Disorders
The management of special hand disorders—encompassing vascular anomalies, thermal and chemical injuries, and factitious syndromes—requires a profound understanding of upper extremity anatomy, microvascular hemodynamics, and tissue viability. Among these, aneurysm, thrombosis, and embolism in the radial, ulnar, and digital arteries represent critical pathologies that directly threaten digital survival.
Acute thrombosis often presents with severe vasospasm, exacerbating ischemia and accelerating tissue necrosis. The consulting orthopedic or hand surgeon must rapidly differentiate between reversible vasospasm and established arterial occlusion to initiate appropriate medical or microsurgical intervention. This comprehensive guide details the evidence-based protocols for diagnosing and surgically managing arterial thrombosis of the hand, alongside essential principles for other specialized hand injuries.
Pathophysiology of Arterial Thrombosis in the Hand
Arterial thrombosis in the upper extremity frequently arises from repetitive blunt trauma, leading to intimal damage, aneurysm formation, and subsequent in-situ thrombosis or distal embolization. The most classic presentation is Hypothenar Hammer Syndrome, wherein the superficial palmar arch or the ulnar artery is crushed against the hook of the hamate during repetitive striking motions.
Mechanisms of Ischemia
- Intimal Hyperplasia and Rupture: Repetitive microtrauma disrupts the internal elastic lamina, leading to subintimal hemorrhage and luminal narrowing.
- Aneurysmal Dilation: Weakening of the tunica media results in true or false aneurysms, which serve as a nidus for mural thrombi.
- Distal Embolization: Microemboli dislodge from the primary ulnar or radial artery lesion, showering the digital arteries and causing acute digital ischemia (often presenting as splinter hemorrhages or blue digits).
- Secondary Vasospasm: The presence of an intravascular thrombus triggers the release of potent vasoconstrictors (e.g., thromboxane A2, serotonin), causing profound vasospasm in collateral vessels, further compromising digital perfusion.
Clinical Pearl: Always evaluate the contralateral hand. While occupational trauma (like using the palm as a hammer) is typically unilateral, systemic conditions such as Buerger's disease (thromboangiitis obliterans) or autoimmune vasculitides often present bilaterally.
Clinical Evaluation and Diagnostic Modalities
The cornerstone of evaluating hand ischemia is a meticulous physical examination, heavily reliant on provocative vascular testing. If symptoms of acute thrombosis threaten digital survival, rapid diagnostic confirmation is mandatory.
The Allen Test for Radial and Ulnar Artery Patency
The Allen test is the gold standard bedside clinical examination for assessing the collateral circulation of the hand via the superficial and deep palmar arches.
Step-by-Step Execution:
1. The patient is instructed to elevate the hand and make a tight fist to exsanguinate the palmar vault.
2. The examiner firmly occludes both the radial and ulnar arteries at the wrist.
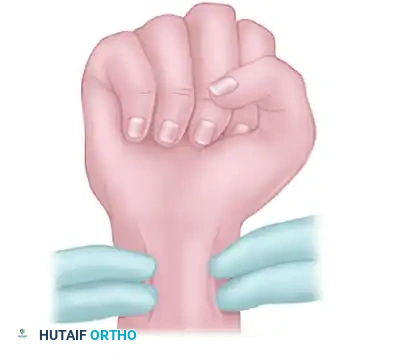
FIGURE 70-1A: Patient elevates hand and makes a fist while the examiner occludes the radial and ulnar arteries.
- The patient extends the fingers. The hand should appear blanched and pale due to the arterial occlusion.
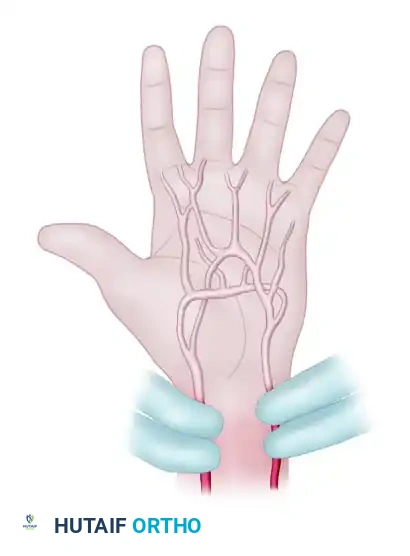
FIGURE 70-1B: Patient extends fingers, and blanching of the hand is seen.
- The examiner releases pressure on the radial artery alone. In a normal hand, capillary refill occurs rapidly (within 3-5 seconds), and the color returns to normal, indicating a patent radial artery.
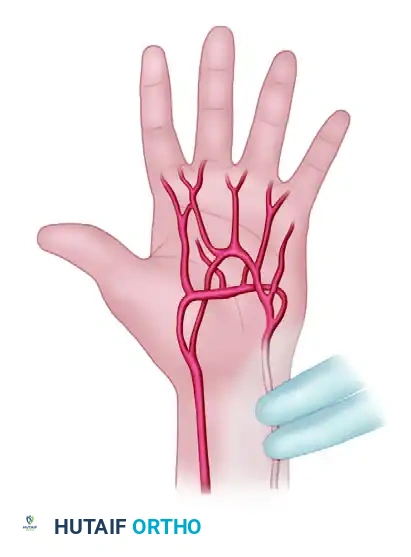
FIGURE 70-1C: Radial artery alone is released, and the color of the hand returns to normal.
- The test is repeated, this time releasing the ulnar artery alone. If the hand remains blanched, the test is positive for ulnar artery thrombosis or incomplete palmar arch collateralization.

FIGURE 70-1D: In thrombosis of the ulnar artery, the test is positive (hand remains blanched) when this artery alone is released.
The Digital Allen Test
When distal embolization or isolated digital artery thrombosis is suspected, the Digital Allen test is employed to assess the patency of the radial and ulnar proper digital arteries.
Step-by-Step Execution:
1. The examiner occludes both digital arteries at the base of the affected finger while the patient flexes the digit to exsanguinate it.

FIGURE 70-2A: Examiner occludes both digital arteries, and the patient flexes the finger.
- The patient extends the finger, revealing a blanched digit.
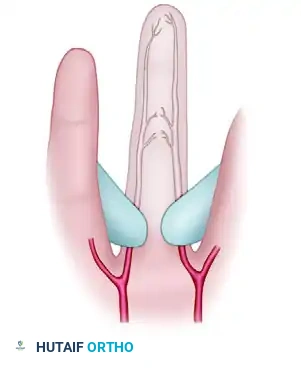
FIGURE 70-2B: Patient extends the finger, and blanching of the finger is seen.
- The examiner releases one digital artery. If patent, the color returns rapidly.
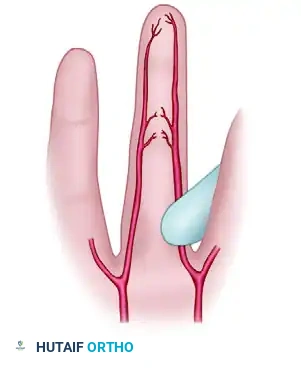
FIGURE 70-2C: When either artery is patent and it alone is released, the color of the finger returns to normal.
- If the released artery is thrombosed, the finger will remain blanched, confirming isolated digital vessel occlusion.
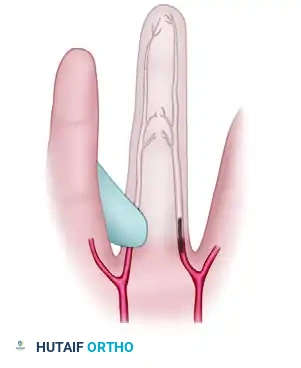
FIGURE 70-2D: When either artery is thrombosed and it alone is released, the finger remains blanched.
Advanced Diagnostic Imaging and Interventions
If the Allen test is positive, further objective data must be gathered to confirm the diagnosis and map the vascular anatomy prior to surgical intervention.
- Non-Invasive Studies: Thermography, temperature probes, Doppler ultrasound studies, and pulse volume recordings (PVR) are utilized to quantify the severity of ischemia. A digital-brachial index (DBI) of less than 0.7 is highly indicative of significant arterial compromise.
- Diagnostic/Therapeutic Blocks: A stellate ganglion block or brachial plexus block can be administered. These blocks provide profound sympatholysis. If the block relieves symptoms and restores perfusion, the primary pathology may be severe vasospasm, and the treatment defaults to observation and medical management.
- Arteriography: The definitive gold standard. Arteriography establishes the exact diagnosis, identifies the proximal and distal extent of the thrombosis, maps the collateral vascular disease, and determines the probable success of microsurgical reconstruction.
Surgical Warning: During arteriography, intra-arterial medications such as reserpine, tolazoline, or papaverine are usually administered. If symptoms diminish significantly after arteriography and vasodilator infusion, the patient can often be observed without immediate surgery.
Indications for Surgical Intervention
The decision to proceed with operative management hinges on the viability of the digits and the response to conservative measures.
Indications for Observation/Medical Management:
* Symptoms are relieved by stellate ganglion or brachial blocks.
* Symptoms diminish following diagnostic arteriography and intra-arterial vasodilators.
* Vascular disease is generalized (e.g., severe systemic atherosclerosis, advanced scleroderma) where localized resection would fail.
Indications for Surgery:
* Symptoms persist despite maximal medical therapy and sympathetic blocks.
* Digital survival is acutely in question (impending gangrene, rest pain).
* Presence of a symptomatic aneurysm acting as an embolic source.
Surgical Approach: Resection and Vein Grafting
When surgery is indicated, the objective is to resect the thrombosed or aneurysmal segment and restore pulsatile flow using a reversed interpositional vein graft.
1. Patient Positioning and Preparation
- The patient is positioned supine with the arm extended on a radiolucent hand table.
- A pneumatic tourniquet is applied to the proximal arm but is inflated only after exsanguination via elevation (avoiding Esmarch bandages that might dislodge further emboli).
- The operating room must be kept warm to prevent cold-induced vasospasm.
- An operating microscope or high-powered loupe magnification (minimum 3.5x to 4.5x) is essential.
2. Surgical Exposure
- A standard expansile incision is made over the affected artery (e.g., a zigzag or Brunner incision over the hypothenar eminence for the ulnar artery).
- The superficial palmar fascia is divided, and the ulnar nerve is carefully identified and protected. The ulnar artery is mobilized from Guyon's canal distally into the superficial palmar arch.
- The thrombosed or aneurysmal segment is identified. The vessel will typically appear dark, firm, and lack pulsatility.
3. Resection of the Thrombosed Segment
- Microvascular clamps (e.g., Acland clamps) are placed proximally and distally to the diseased segment in healthy, pliable tissue.
- The thrombosed segment is resected entirely.
- Crucial Step: The proximal clamp is temporarily released to assess inflow. If backflow is good and pulse volume is strong, the proximal vessel is deemed healthy. The distal clamp is similarly released to check for backbleeding, confirming distal patency.
4. Vein Graft Harvesting and Preparation
- A suitable donor vein is selected, typically from the volar forearm or the dorsal hand venous network.
- The vein is harvested meticulously, ligating all side branches with fine silk or hemoclips.
- Reversal: The vein graft must be reversed before interposition to ensure that the venous valves do not impede arterial flow.
- The graft is gently dilated with heparinized saline to overcome spasm and check for leaks.
5. Microsurgical Anastomosis
- The reversed vein graft is interposed into the arterial defect.
- Anastomoses are performed under the operating microscope using 8-0 or 9-0 non-absorbable monofilament suture (e.g., Nylon) in an interrupted fashion.
- The distal anastomosis is typically completed first, followed by the proximal anastomosis.
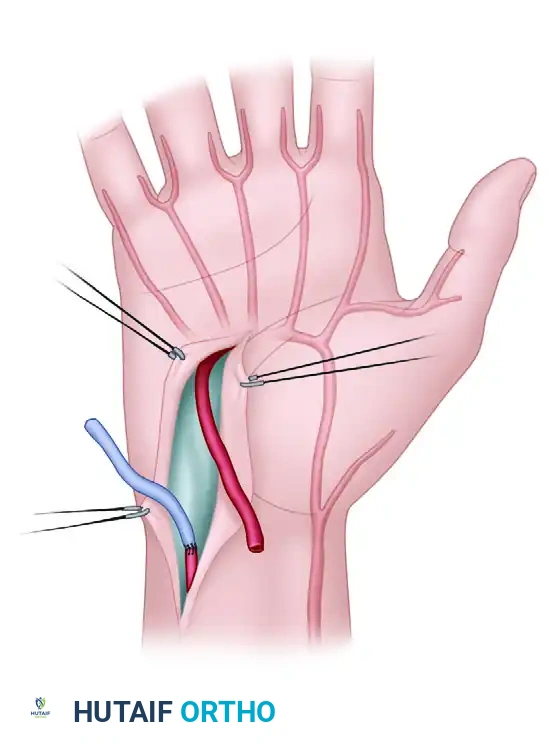
FIGURE 70-3: Resection of thrombosed segment and replacement with reversed vein graft. The thrombosed segment of the artery is removed, and the reversed vein graft is sutured in place to restore continuity.
6. Reperfusion and Closure
- The clamps are removed (distal first, then proximal).
- The anastomoses are inspected for leaks. Gentle pressure with a topical hemostatic agent or a single adventitial stitch may be required for minor leaks.
- The tourniquet is deflated. The surgeon must observe the return of pulsatile flow through the graft and the immediate pinking up of the previously ischemic digits.
- Topical vasodilators (e.g., papaverine or lidocaine) are applied to the graft to relieve any residual vasospasm.
- The wound is closed loosely to prevent any compression on the newly grafted vessel. A bulky, non-compressive soft dressing and a volar splint are applied.
Postoperative Protocol and Rehabilitation
The success of microvascular reconstruction relies heavily on meticulous postoperative care.
- Monitoring: The hand is kept elevated. Digital perfusion is monitored hourly for the first 24-48 hours using clinical observation (color, capillary refill, turgor), surface temperature probes, or implantable Doppler probes. A drop in digital temperature of >2°C compared to adjacent digits warrants immediate investigation.
- Anticoagulation: Protocols vary, but typically include intravenous Dextran 40 or a heparin infusion for 3-5 days, followed by daily aspirin (81-325 mg) for 3-6 months to prevent platelet aggregation at the anastomotic sites.
- Environment: The patient must be kept in a warm environment. Strict abstinence from smoking and caffeine is mandatory, as nicotine is a potent vasoconstrictor that can induce catastrophic graft failure.
- Therapy: Gentle, protected active range of motion (AROM) is initiated within the first week to prevent tendon adhesions, avoiding any extreme extension that might place tension on the arterial graft.
Overview of Other Special Hand Disorders
While vascular thrombosis represents a surgical emergency, the hand surgeon must also be adept at managing a variety of other complex environmental and factitious injuries.
Thermal, Electrical, and Chemical Burns
- Thermal Burns: Management depends on the depth. Superficial burns are treated with topical antimicrobials (e.g., silver sulfadiazine). Deep partial-thickness and full-thickness burns require early tangential excision and split-thickness skin grafting to prevent severe flexion contractures.
- Electrical Burns: Often deceptive, as the visible entry and exit wounds belie massive deep tissue necrosis along the path of least resistance (nerves and blood vessels). Compartment syndrome is highly likely; early and aggressive fasciotomies of the hand and forearm are frequently required.
- Chemical Burns: Immediate and copious irrigation with water or saline is the universal first step. Hydrofluoric acid burns are a notable exception, requiring topical or injected calcium gluconate to neutralize the fluoride ions and prevent profound systemic hypocalcemia and deep tissue liquefaction.
Frostbite
Frostbite results from the crystallization of intra- and extracellular water, leading to cellular dehydration, microvascular thrombosis, and tissue death.
* Treatment: Rapid rewarming in a water bath at 40°C to 42°C (104°F to 108°F) until the tissue becomes pliable and erythematous. Early surgical debridement is contraindicated; the surgeon must wait for clear demarcation of necrotic tissue, which may take weeks ("freeze in January, amputate in July").
High-Pressure Injection Injuries
A catastrophic surgical emergency. Paint, grease, or hydraulic fluid injected under high pressure (often >3,000 psi) via a pinpoint wound spreads rapidly along the flexor tendon sheaths.
* Treatment: Requires immediate, wide surgical exploration and radical debridement of all foreign material and necrotic tissue. Delay in surgery exponentially increases the risk of digital amputation.
Factitious Hand Syndromes and Dysfunctional Postures
- Psychoflexed and Psychoextended Hands: These are dysfunctional postures without an identifiable organic neurologic or musculoskeletal cause.
- Factitious Disorders: Patients intentionally produce symptoms (e.g., self-inflicted tourniquet ischemia, wound contamination) for primary psychological gain.
- Management: Diagnosis is often one of exclusion. Confrontation is generally counterproductive. Management requires a multidisciplinary approach involving psychiatry, hand therapy, and conservative orthopedic care, avoiding unnecessary surgical interventions.
Conclusion
The management of special hand disorders demands a high index of suspicion and a mastery of both clinical examination and microsurgical techniques. In cases of arterial thrombosis, the Allen test remains an invaluable bedside tool, guiding the need for advanced imaging and intervention. When conservative measures and sympathetic blocks fail to relieve critical ischemia, prompt resection and reversed vein grafting provide the most reliable means of restoring perfusion, salvaging the digit, and returning function to the compromised hand.
You Might Also Like
