Surgical Restoration of Intrinsic Finger Function: Biomechanics and Tendon Transfers
Key Takeaway
The restoration of intrinsic finger function addresses the debilitating clawhand deformity caused by ulnar and median nerve palsies. By preventing metacarpophalangeal hyperextension, the long extensors can effectively extend the interphalangeal joints. This guide details the biomechanics, indications, and step-by-step surgical techniques for dynamic tendon transfers and static capsulodesis procedures to restore synchronized grasp and pinch kinematics.
Introduction to Intrinsic Paralysis of the Hand
The loss of intrinsic muscle function in the fingers is a profoundly disabling condition, most commonly resulting from paralytic diseases (such as Hansen's disease) or low median and ulnar nerve lesions. In these low nerve lesions, the intrinsic muscles undergo selective paralysis, while the long extrinsic muscles—innervated more proximally in the forearm—are spared. This creates a severe biomechanical imbalance where the extrinsics act unopposed, culminating in the classic "clawhand" deformity.
The primary goal of surgical intervention is the restoration of intrinsic finger function, which is essential for synchronized digital flexion, powerful grasp, and stable pinch kinematics. This comprehensive guide details the pathomechanics of intrinsic minus hands, preoperative considerations, and the textbook surgical techniques for dynamic tendon transfers and static stabilization.
Pathomechanics of the Clawhand Deformity
To effectively reconstruct the intrinsically paralyzed hand, the surgeon must possess a flawless understanding of digital biomechanics. Loss of intrinsic muscle power leads to hyperextension of the metacarpophalangeal (MCP) joints in a mobile hand. However, MCP hyperextension itself is not the most disabling aspect of this paralysis; rather, it is the profound loss of grasp mechanics.
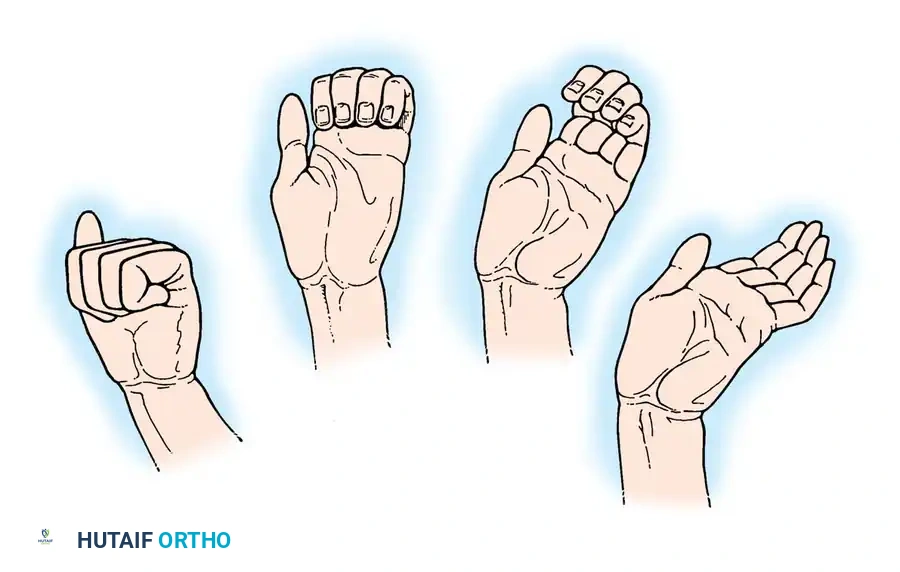
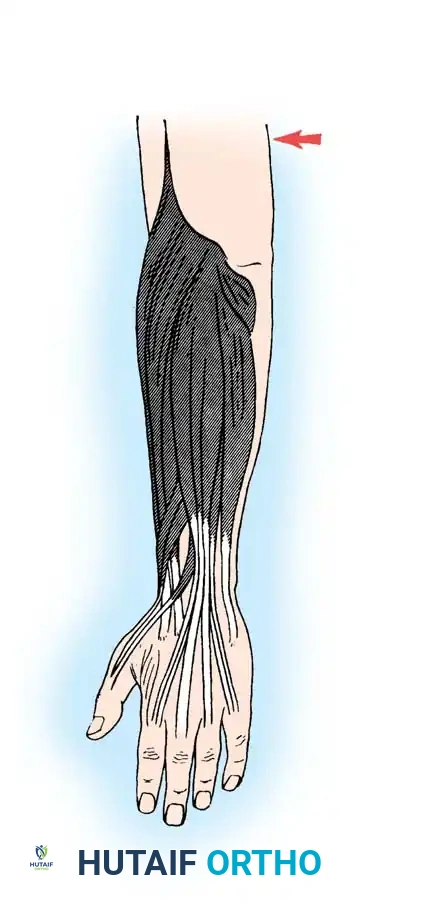
Fig. 68-16 Low median and ulnar nerve palsy. Action of extrinsic flexors of fingers when all intrinsic muscles are paralyzed. From right to left, these long flexors flex first the distal interphalangeal joints, then the proximal interphalangeal joints, and finally the metacarpophalangeal joints.
Clinical studies demonstrate that with intrinsic paralysis, overall grip strength is diminished by 50% or more. This weakness is directly attributable to the absence of primary flexion power at the MCP joints. Furthermore, the paralysis induces asynchronous movement during digital flexion.
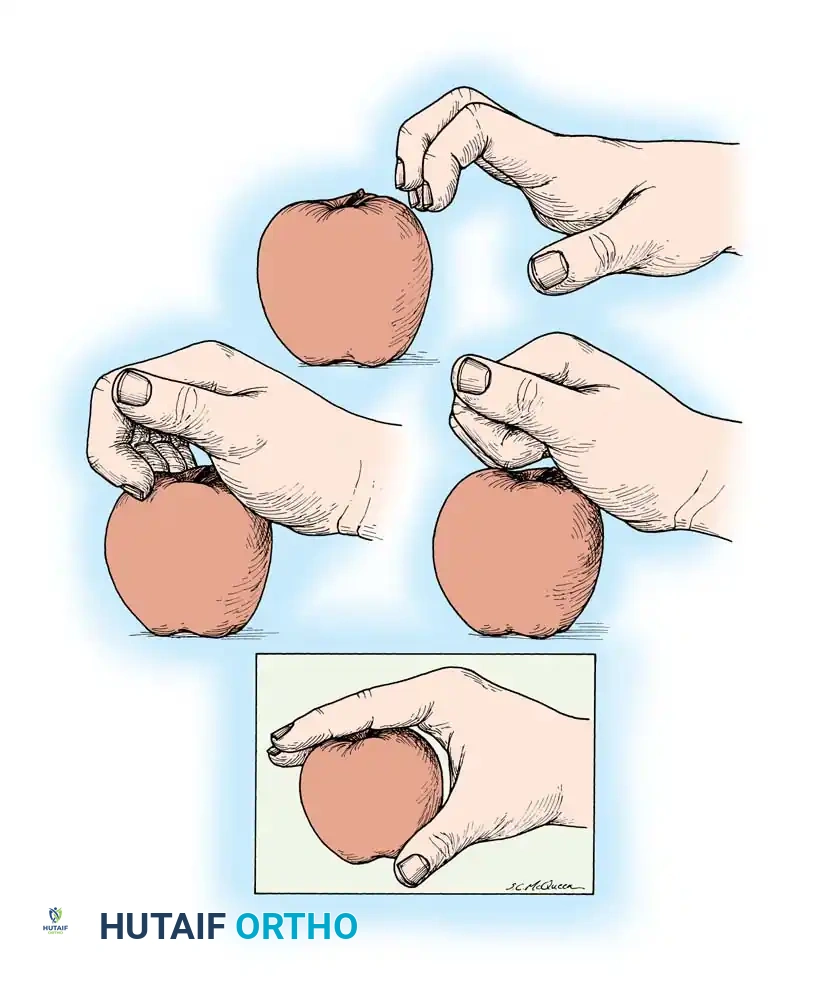
Fig. 68-17 Intrinsic muscle palsy. Flexion of metacarpophalangeal joints occurs only after interphalangeal joints are fully flexed. Fingers curl into the hand and push away any large object they attempt to grasp.
This asynchronous movement is clinically observed as the "roll-up maneuver." Because the intrinsic muscles (lumbricals and interossei) normally initiate MCP flexion while extending the interphalangeal (IP) joints, their absence forces the long flexors to act alone. Consequently, the IP joints flex first, followed sequentially by the MCP joints. This out-of-phase flexion causes the fingers to curl prematurely, effectively pushing large objects out of the palm rather than grasping them.
The Loss of Pinch Power and Lateral Stability
In addition to diminished grasp, the power of pinch is severely compromised. This is compounded by the paralysis of the thenar musculature (in combined median/ulnar lesions). Biomechanically, the collateral ligaments of the MCP joints are lax when the joint is in extension. Without the stabilizing force of the intrinsic musculature, the digits lose lateral stability.
When the long extensor tendons fire, divergence of the fingers is automatic. Conversely, due to the anatomical alignment of the long finger flexors, convergence of the fingertips during grasping is also automatic. The intrinsic muscles are therefore absolute prerequisites for stabilizing the fingers in extension at the MCP joint—especially to provide resistance in the index finger against the pinch pressure exerted by the thumb.
Core Principles of Surgical Reconstruction
The foundational principle of intrinsic reconstruction relies on a specific biomechanical truth: The long finger extensors are fully capable of extending the interphalangeal joints, provided that the metacarpophalangeal joints are stabilized and prevented from hyperextending.
Clinical Pearl: All operations designed to correct intrinsic paralysis—whether dynamic tendon transfers or static blocks—are fundamentally based on preventing MCP hyperextension to allow the extrinsic extensors to transmit their force distally to the IP joints.
The MCP joints can be stabilized via several methods:
* Capsuloplasty (Capsulodesis): e.g., Zancolli procedure.
* Tenodesis: e.g., Riordan or Fowler static tethers.
* Bone Block: e.g., Mikhail procedure.
* Arthrodesis: Reserved for severe, rigid deformities.
* Dynamic Tendon Transfers: The gold standard for restoring active, synchronized grasp.
The selection of the proper operation depends entirely on the availability of expendable donor muscles, the degree of passive motion present in the digital and radiocarpal joints, and the surgeon's expertise.
Dynamic Tendon Transfers: Surgical Techniques
Tendon transfers to replace intrinsic function are among the most variable, biomechanically complex, and surgically demanding procedures in upper extremity reconstruction. No single procedure is universally accepted, as every paralytic hand presents a unique constellation of available donors and specific functional deficits.
The Bunnell Transfer and Modifications
Originally described in 1942, Bunnell's technique involved detaching the flexor digitorum superficialis (FDS) tendon from each finger, splitting it, and routing one slip to each side of the extensor aponeurosis via the lumbrical canals.
Surgical Warning: The classic Bunnell transfer removes a powerful flexor of the proximal interphalangeal (PIP) joint and converts it into an extensor. In supple hands, this transfer is frequently too strong, progressively pulling the PIP joints into rigid extension and creating a debilitating iatrogenic "intrinsic-plus" deformity.
To mitigate this, a modified Bunnell procedure is utilized, wherein only a single FDS tendon (usually from the middle or ring finger) is harvested, split into four slips, and transferred to all four fingers. This is particularly useful in clawhands that already exhibit some preoperative restriction of motion in the PIP joints.
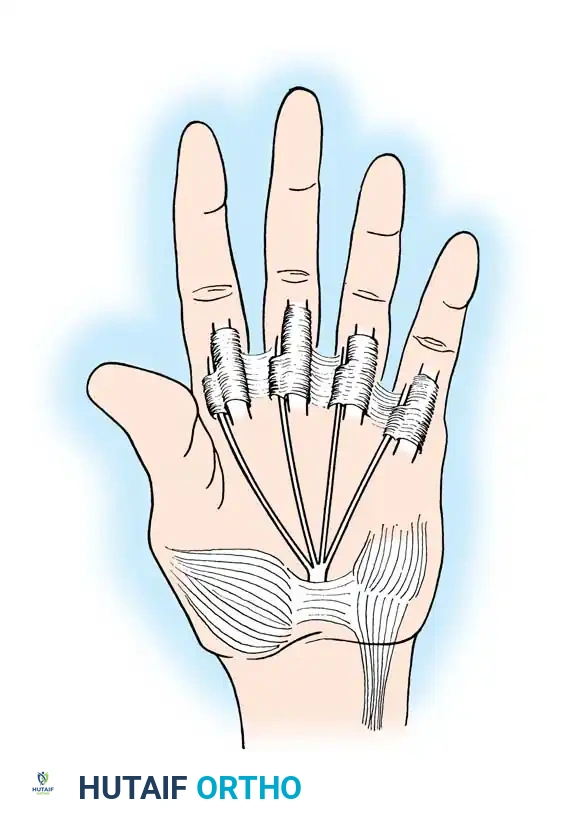
Fig. 68-18 Modification of the Bunnell transfer. A single sublimis tendon is split and routed to restore intrinsic function across multiple digits, reducing the risk of intrinsic-plus deformity.
The Fowler Transfer
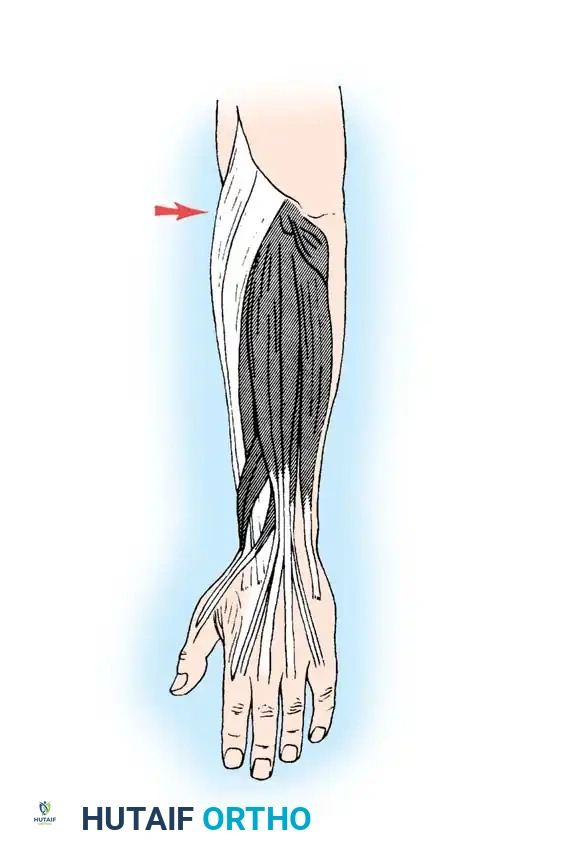
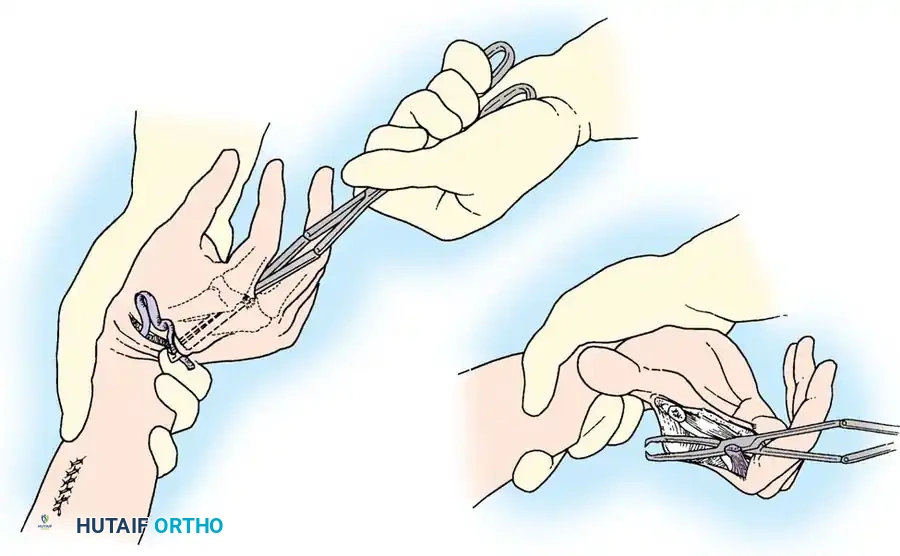
Fowler devised a transfer utilizing the extensor indicis proprius (EIP) and extensor digiti minimi (EDQ). The tendons are split to form four slips. Crucially, these slips must be passed volar to the deep transverse metacarpal ligament to effectively flex the MCP joint before inserting into the extensor aponeurosis.
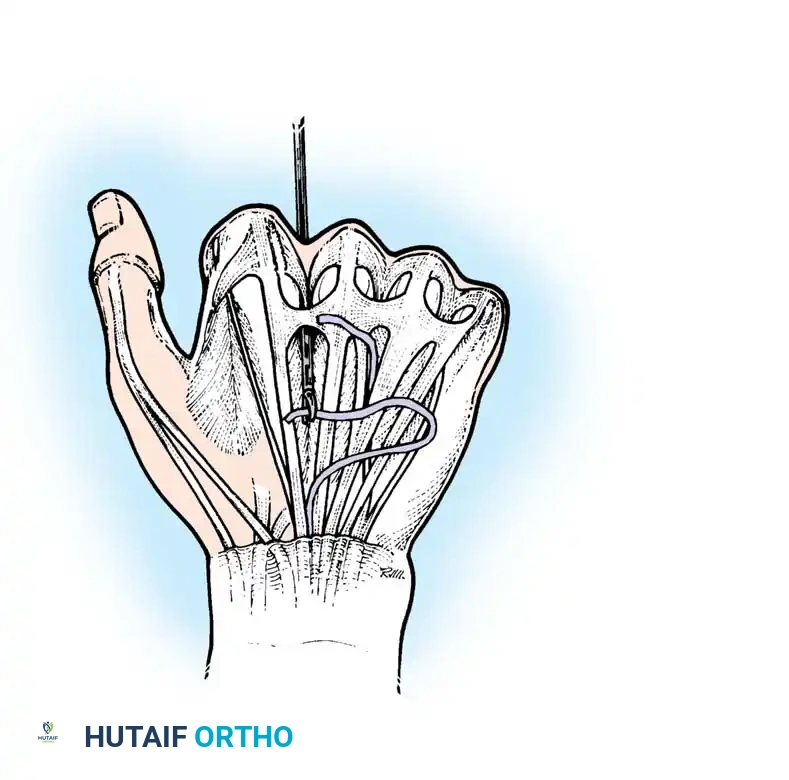
Site of the extensor indicis proprius tendon harvest.
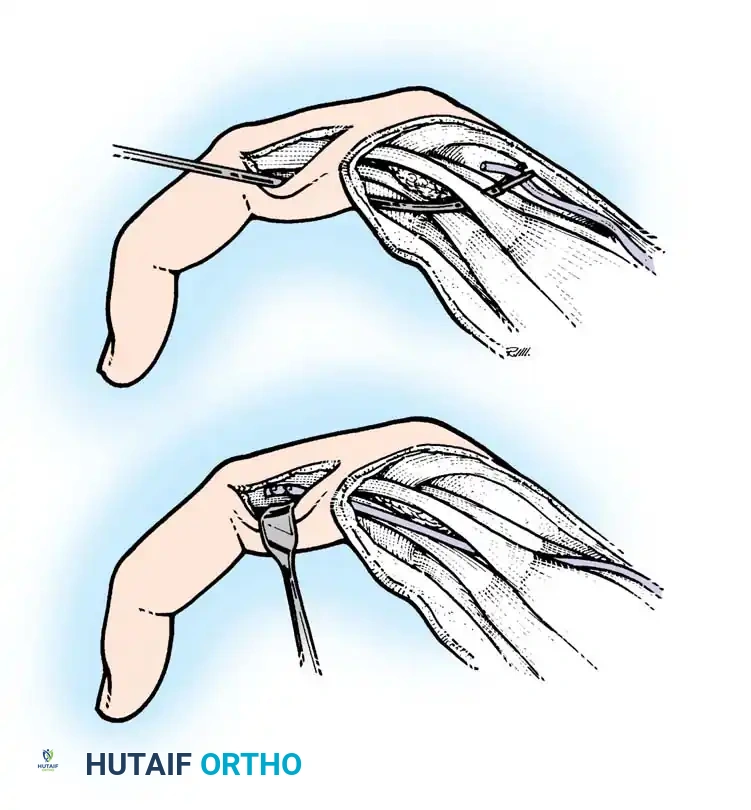
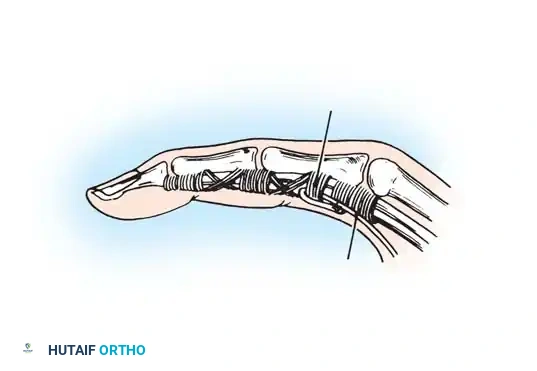
Fig. 68-19 & 68-20: Clamp threading the graft through the interosseous space. Any tendon transferred from the dorsum of the hand to restore intrinsic function must pass volar to the deep transverse metacarpal ligament.
While highly efficient and benefiting from a tenodesing effect during wrist flexion, the Fowler transfer requires the tendon slips to be advanced approximately 2.5 cm to reach their insertion sites. This places the transfer under considerable tension, occasionally leading to intrinsic overpull.
The Riordan Transfers
To avoid the excessive tension inherent in the Fowler transfer, Riordan introduced several modifications utilizing free tendon grafts.
In one variation, the detached EIP is split into two slips, passed volar to the deep transverse metacarpal ligament, and attached to the radial side of the ring and little fingers. A free tendon graft (such as palmaris longus or plantaris) is then sutured to the musculotendinous junction of the EIP. The distal end of this graft is split into two slips and routed to the middle and index fingers.
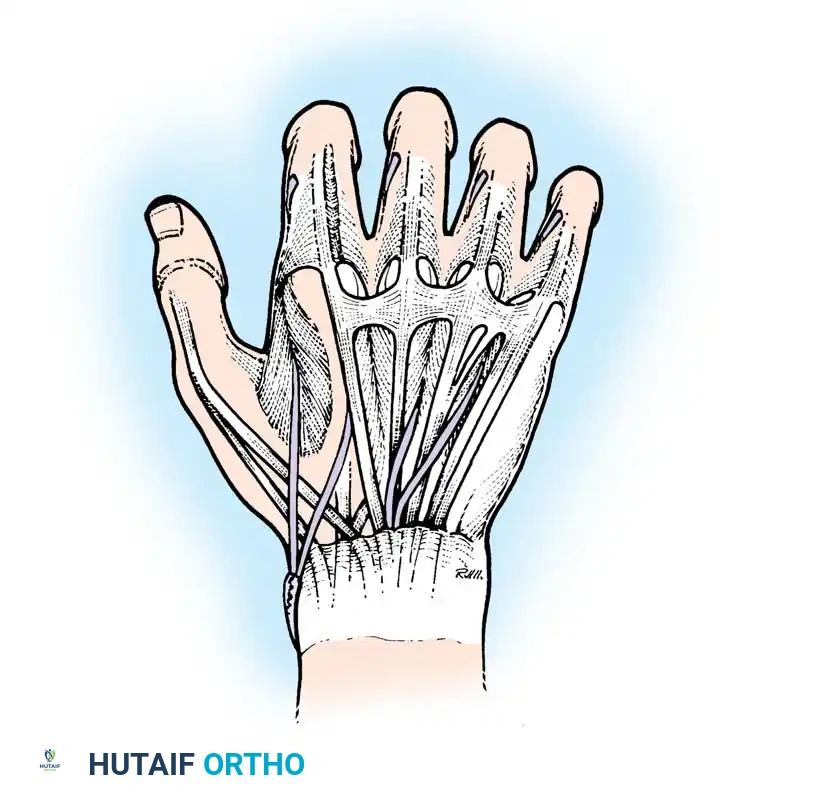
Fig. 68-21 Riordan transfer utilizing a palmaris longus or plantaris graft to the index and middle fingers, while the EIP is rerouted to the ring and little fingers.
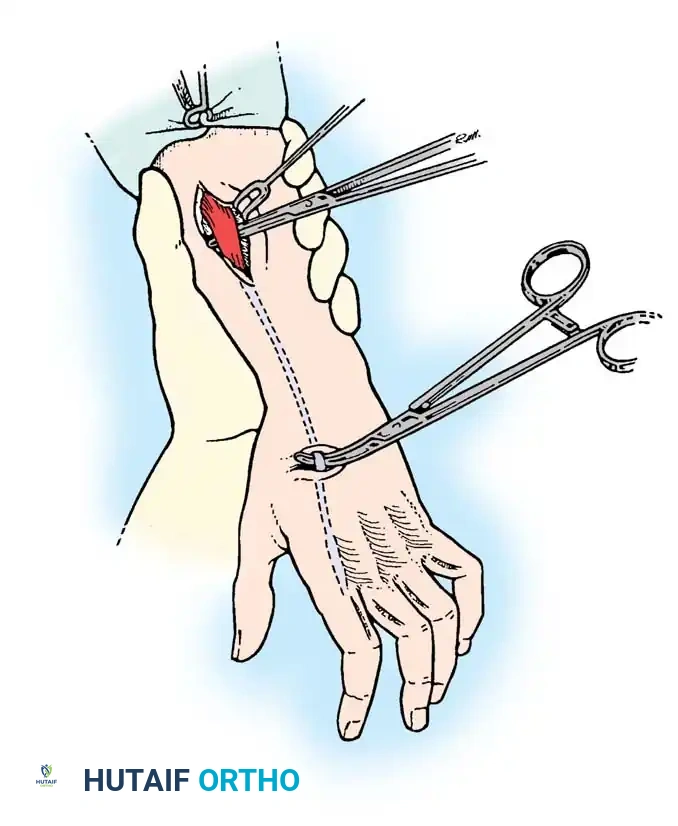
For patients with severe clawing who have developed a chronic habit of flexing the wrist to passively extend the digits, Riordan advised transferring the flexor carpi radialis (FCR). The FCR insertion is freed, transferred to the dorsum of the wrist, and prolonged with a four-tailed plantaris graft.
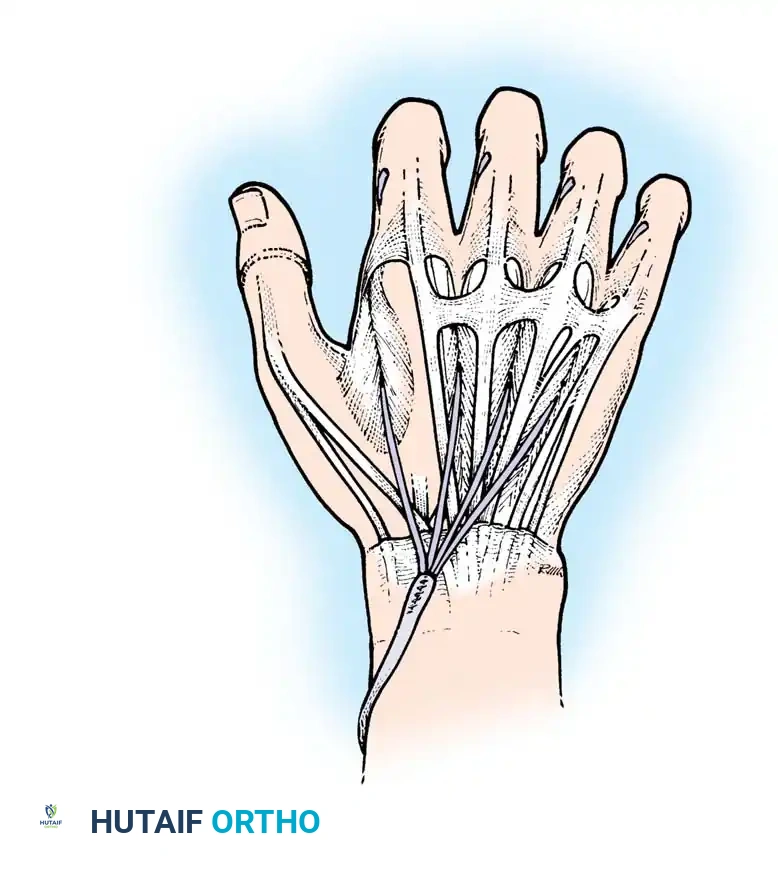
Fig. 68-25 Riordan transfer: A four-tailed plantaris tendon graft is meticulously sutured to the tendon of the flexor carpi radialis muscle.
The Brand Transfers
Paul Brand, drawing from extensive experience treating Hansen's disease, developed highly reliable transfers using the wrist extensors. His preferred technique utilizes the extensor carpi radialis brevis (ECRB), lengthened by a free plantaris graft.
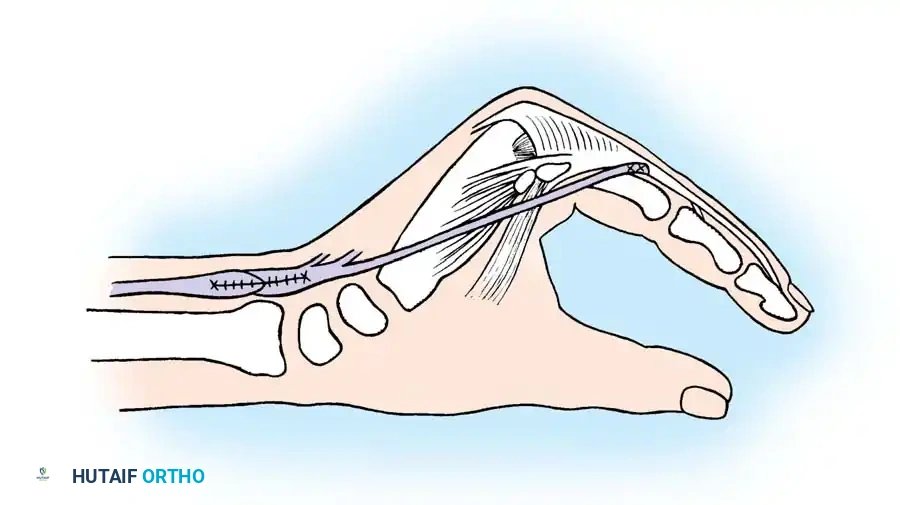
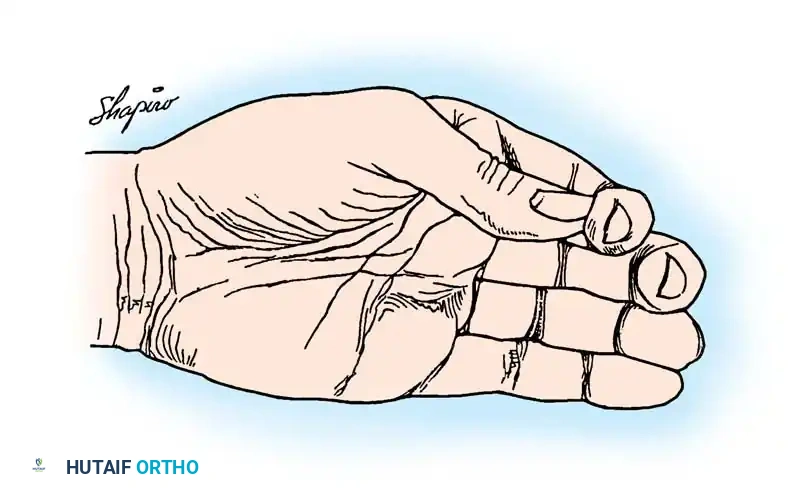
Fig. 68-22 Brand transfer of the ECRB tendon, prolonged with a free graft to restore intrinsic function. The graft is split into four tails.
Each tail is passed volar to the deep transverse metacarpal ligament. For the middle, ring, and little fingers, the slips are attached to the radial side of the extensor aponeurosis. However, for the index finger, Brand advocated attaching the slip to the ulnar side.
Biomechanical Pearl: Attaching the transfer to the ulnar lateral band of the index finger places the digit in adduction during pinch. This provides a much firmer and more stable platform against the thumb compared to radial attachment, which would promote abduction.
Brand also described a variation where the extensor carpi radialis longus (ECRL) or ECRB is transferred to the volar aspect of the forearm, extended by a four-tailed graft through the carpal tunnel, and routed through the lumbrical canals.
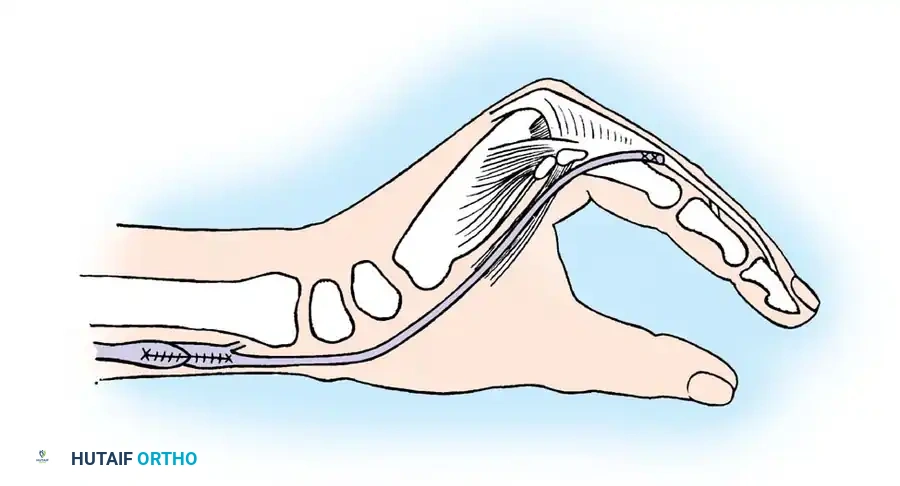
Fig. 68-24 Brand transfer routed to the volar side of the forearm and passed through the carpal tunnel. Note: This crowds the carpal tunnel and risks median nerve compression if the nerve is still functioning.
Advanced Tendon Routing and Graft Preparation
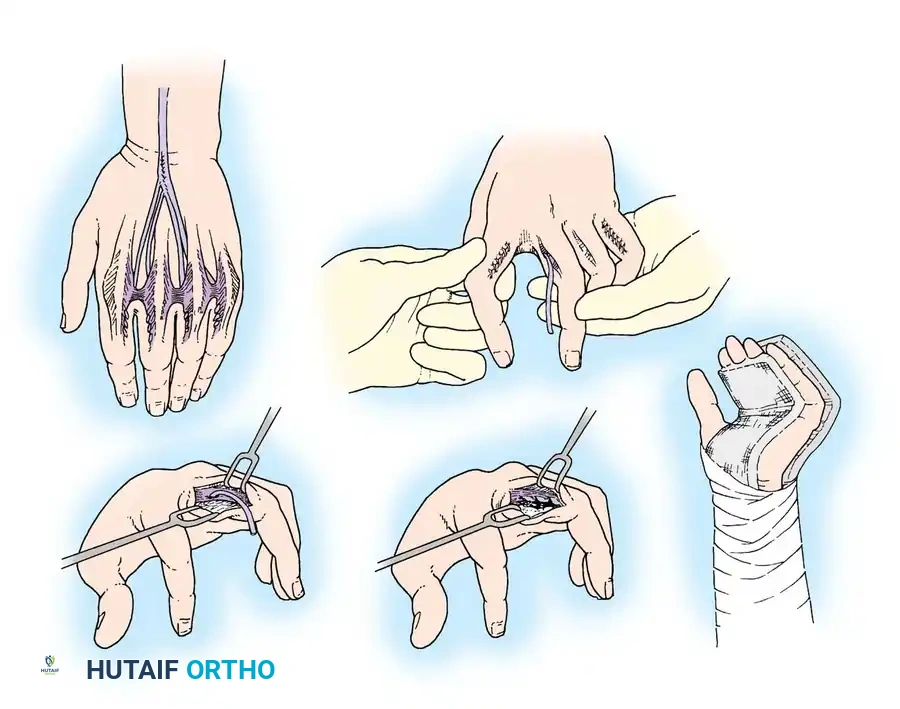
The success of any intrinsic tendon transfer relies heavily on the meticulous preparation of the tendon grafts and the precise anatomical routing of the slips. The grafts must be woven smoothly to prevent adhesions and ensure seamless gliding through the interosseous spaces.
Meticulous preparation and suturing of the multi-tailed tendon graft. A Pulvertaft weave is often employed to ensure a biomechanically secure junction between the donor motor and the free graft.
The routing pathways must strictly adhere to the volar aspect of the transverse metacarpal ligament to recreate the flexion moment arm at the MCP joint.
Intraoperative routing diagrams demonstrating the passage of tendon slips through the interosseous spaces. The slips must glide without impingement.

You Might Also Like


