Surgical Release of Established Intrinsic Muscle Contractures of the Hand
Key Takeaway
The release of established intrinsic muscle contractures of the hand requires precise surgical intervention to restore digital kinematics. The Littler technique involves the selective excision of the oblique fibers of the extensor aponeurosis while meticulously preserving the transverse fibers to prevent metacarpophalangeal hyperextension. Severe thumb web space contractures necessitate comprehensive release of the skin, fascia, adductor musculature, and carpometacarpal capsule, often requiring local flaps or skin grafting for adequate coverage.
INTRODUCTION TO INTRINSIC MUSCLE CONTRACTURES
Established intrinsic muscle contractures of the hand present a formidable reconstructive challenge to the orthopaedic surgeon. The intrinsic musculature—comprising the lumbricals, dorsal and volar interossei, and the hypothenar and thenar groups—plays a critical role in the complex kinematics of the hand. When these muscles become fibrotic and contracted, they produce a classic "intrinsic-plus" deformity, characterized by severe flexion of the metacarpophalangeal (MCP) joints and hyperextension of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints.
The etiology of intrinsic contractures is multifactorial. It frequently arises from ischemic conditions (such as compartment syndrome of the hand), severe crush injuries, deep space infections, thermal or electrical burns, rheumatoid arthritis, spastic neurological disorders, and prolonged faulty immobilization. Left untreated, the intrinsic-plus hand severely compromises grip strength, fine pinch, and overall hand dexterity.
This comprehensive guide details the surgical management of established intrinsic contractures, focusing on the classic Littler release for the digits and the complex, multi-structural release required for severe thumb web space contractures.
PATHOANATOMY AND BIOMECHANICS
To successfully correct an intrinsic contracture, the surgeon must possess an intimate understanding of the extensor aponeurosis and the precise insertions of the intrinsic muscles.
The intrinsic tendons approach the MCP joint volar to the axis of rotation, acting as primary flexors of the MCP joint. As they continue distally, they fan out into the extensor aponeurosis, dividing into two distinct functional components:
1. Transverse Fibers (Sagittal Bands): These fibers insert into the base of the proximal phalanx and the extensor hood. Their primary function is to flex the MCP joint.
2. Oblique Fibers (Lateral Bands): These fibers continue dorsally and distally, joining the central slip and the terminal tendon to extend the PIP and DIP joints.
In an intrinsic contracture, the resting length of the muscle-tendon unit is pathologically shortened. This constant tension flexes the MCP joint and rigidly extends the PIP joint.
Clinical Pearl: The Bunnell Intrinsic Tightness Test
Before proceeding with surgery, intrinsic tightness must be differentiated from extrinsic extensor tightness or capsular contracture.
- Step 1: Hold the MCP joint in passive extension. Attempt to passively flex the PIP joint. If PIP flexion is restricted, intrinsic tightness or capsular contracture is present.
- Step 2: Flex the MCP joint. If the PIP joint can now be passively flexed, the diagnosis is intrinsic muscle contracture (the intrinsic tendons are relaxed when the MCP is flexed). If the PIP joint remains stiff, a joint capsular contracture is the primary pathology.
THE LITTLER RELEASE FOR DIGITAL INTRINSIC CONTRACTURES
The Littler intrinsic release is the gold standard procedure for isolated digital intrinsic contractures. The fundamental principle of this operation is the selective excision of the oblique fibers of the extensor aponeurosis, which eliminates the pathological extension force on the PIP joint, while meticulously preserving the transverse fibers to maintain MCP joint flexion and stability.
Indications
- Positive Bunnell intrinsic tightness test with functional impairment.
- Intrinsic-plus deformity secondary to trauma, ischemia, or rheumatoid arthritis.
- Spastic intrinsic contractures (e.g., cerebral palsy, stroke) where conservative management (splinting, botulinum toxin) has failed.
Surgical Technique: Step-by-Step
1. Positioning and Preparation
The patient is positioned supine with the operative arm on a radiolucent hand table. Regional anesthesia (brachial plexus block) or general anesthesia is utilized. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
2. Incision and Exposure
- Make a single, longitudinal midline incision on the dorsum of the proximal phalanx. The incision should extend from the level of the metacarpophalangeal joint distally to the proximal interphalangeal joint.
- Surgical Rationale: A midline dorsal incision provides excellent, simultaneous exposure of both the radial and ulnar sides of the extensor aponeurosis while remaining safely dorsal to the neurovascular bundles.
- Elevate full-thickness skin flaps radially and ulnarly. Retract the skin using fine skin hooks to expose the underlying extensor mechanism.
3. Identification of the Extensor Aponeurosis
- Identify the central extensor tendon.
- Trace the intrinsic lateral bands as they sweep dorsally to join the extensor mechanism.
- Clearly delineate the transverse fibers (proximal) and the oblique fibers (distal).
4. Excision of the Oblique Fibers
- Incise the insertion of the oblique fibers of the extensor aponeurosis into the extensor tendon.
- The incision must be made strictly parallel with the central extensor tendon.
- Resect a triangular wedge of the oblique fibers on both the radial and ulnar sides of the digit.
🚨 SURGICAL WARNING: Preservation of Transverse Fibers
It is absolutely critical to preserve the transverse fibers of the intrinsic mechanism. Inadvertent excision of the transverse fibers will result in the loss of primary MCP flexion, leading to hyperextension of the metacarpophalangeal joint, a resultant iatrogenic clawhand deformity, and secondary limitation of interphalangeal joint extension.
5. Intraoperative Verification
- After adequate excision of the oblique fibers, perform an intraoperative Bunnell test.
- With the metacarpophalangeal joint held in neutral extension, the proximal interphalangeal joint should now demonstrate full, unrestricted passive flexion.
- If residual tightness remains, carefully inspect for remaining oblique fibers or secondary PIP joint capsular contracture.
6. Closure
- Deflate the tourniquet and achieve meticulous hemostasis using bipolar electrocautery.
- Close the dorsal skin incision with interrupted 5-0 non-absorbable monofilament sutures.
Postoperative Protocol
- Immediate Post-op: Apply a volar plaster splint extending from the proximal forearm (or elbow, depending on patient compliance) to the middle of the proximal phalanges.
- Positioning: The splint must immobilize the metacarpophalangeal joints in extension while leaving the proximal and distal interphalangeal joints completely free.
- Rehabilitation: Active motion of the interphalangeal joints is initiated on postoperative day one. This early mobilization prevents fibrinous adhesions and ensures the newly released PIP joints maintain their flexion arc.
- Suture Removal: The splint and sutures are removed at 10 to 14 days, followed by progressive strengthening and dynamic splinting if necessary.
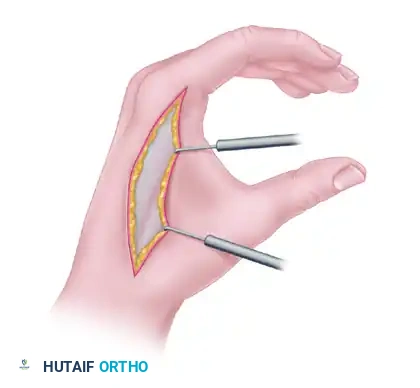
MANAGEMENT OF THUMB WEB SPACE CONTRACTURES
The thumb web space is a complex, three-dimensional anatomical region comprising skin, subcutaneous fat, deep fascia, the adductor pollicis muscle, the first dorsal interosseous muscle, and the carpometacarpal (CMC) joint capsule.
A contracture of the thumb web space (adduction contracture) is devastating to hand function, as it obliterates the ability to perform opposition, wide grasp, and key pinch.
Pathoanatomy and Etiology
Contracture of any single tissue layer within the web space rapidly induces secondary contractures in adjacent structures. Rarely does a severe contracture involve only one anatomical layer.
Common etiologies include:
- Hypertrophic scarring from lacerations or surgical incisions.
- Deep thermal or electrical burns.
- Severe crush injuries and compartment syndrome.
- Deep space infections.
- Congenital webbing (syndactyly).
- Paralysis of the median or radial nerves leading to unopposed adductor tone.
- Dupuytren's contracture.
- Faulty immobilization (casting the thumb in adduction).
Surgical Strategies Based on Severity
The proper treatment of a contracted web is dictated entirely by which structures are involved. Little to no functional improvement is accomplished by releasing the skin alone when deeper structures (muscle, fascia, or joint capsule) are also contracted.
1. Mild Contractures (Skin Only)
When the contracture is strictly limited to the skin—often presenting as a linear hypertrophic scar along the border of the web following a laceration—it can frequently be released using local tissue rearrangement.
- Z-plasty: A standard or multiple Z-plasty effectively lengthens the linear scar and deepens the web.
- Four-Flap Z-plasty: Provides a deeper, more rounded web space contour compared to a standard Z-plasty.
2. Severe Contractures (Deep Fibrosis)
Crushing injuries, deep space infections, or severe burns result in extensive, unyielding fibrosis that permeates the entire thumb web. These cannot be treated by skin release alone. The scarred components of the skin, muscle, fascia, and CMC capsule must be systematically excised.
Surgical Technique: Deep Web Space Release
1. Incision and Exposure
Design a dorsal incision over the first web space, tailored to the planned method of soft tissue coverage (e.g., dorsal rotation flap or skin graft).

2. Deep Dissection and Release
- Fascial Release: Incise and resect the thickened fascia overlying the first dorsal interosseous and the adductor pollicis muscles.
- Muscle Release: In severe cases, the fibrotic bands within the adductor pollicis and first dorsal interosseous must be fractionally lengthened or released from their origins on the third metacarpal and their insertions on the proximal phalanx.
- Capsulotomy: If the thumb cannot be fully abducted and pronated after muscle release, a dorsal and radial capsulotomy of the trapeziometacarpal (CMC) joint must be performed.
🚨 SURGICAL WARNING: The Radial Artery
During deep excision of the scarred adductor and interosseous musculature, extreme caution must be exercised as the dissection approaches the carpometacarpal joint. The radial artery passes dorsally through the anatomical snuffbox and dives volarly between the two heads of the first dorsal interosseous muscle. Iatrogenic injury to the radial artery in a traumatized hand can lead to catastrophic digital ischemia.
3. Skeletal Stabilization
Following a radical release, the thumb must be held in the newly achieved position of wide abduction and pronation.
- Drive one or two smooth Kirschner wires (K-wires) transversely from the first metacarpal into the second metacarpal to rigidly maintain the web space dimension.
4. Soft Tissue Coverage and Skin Grafting
The radical excision of deep fibrotic tissue inevitably produces a deep, gaping fissure between the thumb and index finger. This void must be filled with healthy, pliable skin and subcutaneous fat to provide an elastic, functioning web. Primary closure is impossible and should never be attempted, as it will instantly recreate the contracture.
- Local Flaps: A dorsal rotation flap or a sliding flap is the preferred method to bring vascularized, sensate tissue into the depth of the web space.
- Skin Grafting: The secondary defects created by flap mobilization, or the remaining raw surfaces of the web space, are covered with full-thickness or thick split-thickness skin grafts. Full-thickness grafts are preferred as they undergo significantly less secondary contracture.
- Distant Flaps: If the adjacent dorsal skin is heavily scarred or unsuitable for transfer, a cross-arm flap or a pedicled groin flap may be considered. When utilizing a cross-arm flap, it should be fashioned as a double triangle—one on the dorsal surface and one on the volar surface of the web—to eliminate any linear scar paralleling the border of the web space.
Salvage Procedures for the Thumb Web Space
Carpometacarpal Arthrodesis
When severe articular destruction or irreversible capsular contracture prevents the restoration of functional motion at the carpometacarpal joint, soft tissue release alone will fail. In these salvage scenarios, the CMC joint must be arthrodesed. The first metacarpal is fused to the trapezium in a functional position of palmar abduction (40 degrees) and radial abduction (20 degrees) to permanently maintain the new position of the thumb and allow for key pinch.
The Index Fillet Flap
Occasionally, a severe crush injury or burn leaves the patient with a contracted web space and a severely traumatized, stiff, and functionally useless index finger. In this highly specific scenario, the useless index finger can be amputated (ray resection) and its soft tissue envelope utilized as a filleted pedicle flap. This provides a massive amount of highly vascularized, sensate, glabrous skin to perfectly reconstruct the thumb web space without the need for distant donor sites.
Management of Paralytic Contractures
Paralysis of the muscles of opposition (e.g., median nerve palsy) can result in secondary contracture of the skin, joint capsule, and thumb web due to the unopposed pull of the adductor pollicis and extensor pollicis longus.
- Release requires a Z-plasty or local flap combined with a skin graft, as described by Brand and Milford.
- Contracted fascia and muscle bands must be released, and a CMC capsulotomy performed simultaneously.
- Once passive motion in the carpometacarpal joint is restored and the web space is healed, tendon transfers for opposition (e.g., Huber transfer, FDS transfer) can be performed as a staged secondary procedure to restore dynamic function.
Postoperative Protocol for Thumb Web Space Reconstruction
- Immobilization: The hand is immobilized in a bulky, non-compressive dressing with a thumb spica splint. The K-wires maintain the skeletal architecture, protecting the flaps and grafts from shear forces.
- Graft Care: The initial dressing is typically taken down at 5 to 7 days to inspect the skin grafts and flaps.
- K-wire Removal: The transmetacarpal K-wires are generally left in place for 3 to 4 weeks to allow the soft tissues to heal in their lengthened state.
- Rehabilitation: Following K-wire removal, aggressive occupational therapy is initiated. Custom thermoplastic splinting (a C-bar web spacer) must be worn at night for up to 6 months to prevent late scar contracture and recurrence of the adduction deformity. Active and passive range of motion exercises focus on maintaining CMC abduction and restoring opposition.
You Might Also Like
