Proximal Interphalangeal Arthroplasty & Ulnar Drift
Key Takeaway
Proximal interphalangeal (PIP) joint arthroplasty through an anterior palmar approach provides excellent exposure for implant insertion while preserving the dorsal extensor apparatus. This technique is highly effective for rheumatoid deformities. Concomitant management of distal interphalangeal (DIP) joint deformities and metacarpophalangeal (MCP) ulnar drift requires a comprehensive understanding of hand biomechanics, intrinsic muscle balance, and capsuloligamentous attenuation to restore optimal digital function and alignment.
INTRODUCTION TO RHEUMATOID HAND RECONSTRUCTION
The surgical management of the rheumatoid hand requires a profound understanding of complex biomechanics, progressive capsuloligamentous attenuation, and intrinsic muscle imbalance. The proximal interphalangeal (PIP), distal interphalangeal (DIP), and metacarpophalangeal (MCP) joints are frequently compromised by aggressive synovial proliferation, leading to predictable patterns of deformity such as swan-neck, boutonnière, and ulnar drift.
Reconstructive efforts must be meticulously staged and executed. This masterclass details the anterior (palmar) approach for PIP joint arthroplasty, the management of DIP joint deformities, and the intricate pathoanatomy and surgical correction of MCP joint ulnar drift.
PROXIMAL INTERPHALANGEAL JOINT ARTHROPLASTY THROUGH AN ANTERIOR (PALMAR) APPROACH
The anterior (palmar) approach to the PIP joint, popularized by Lin, Wyrick, Stern, and Schneider, offers distinct biomechanical advantages over dorsal approaches. By accessing the joint volarly, the delicate dorsal extensor apparatus (central slip and lateral bands) remains entirely undisturbed. This significantly reduces the risk of postoperative extensor lag and allows for immediate, aggressive postoperative mobilization.
Indications and Preoperative Planning
Implant arthroplasty of the PIP joint is primarily indicated for patients with severe rheumatoid arthritis or osteoarthritis presenting with debilitating pain, restricted range of motion, and joint destruction (Larsen grade III or higher) where the surrounding soft tissue envelope remains viable.
Surgical Warning: PIP joint arthroplasty is contraindicated in the presence of active infection, profound flexor tendon rupture that cannot be reconstructed, or severe bone stock depletion that precludes stable implant seating. In such cases, arthrodesis remains the salvage procedure of choice.
Anesthesia and Positioning
- Anesthetic Selection: Select an appropriate anesthetic modality based on patient comorbidities and surgical goals. Lin et al. advocate for an intermetacarpal block combined with intravenous sedation. This "wide-awake" approach (WALANT principles) allows the surgeon to assess active PIP joint motion intraoperatively after implant insertion.
- Tourniquet: A sterile wrist tourniquet or a well-padded forearm tourniquet is utilized to maintain a bloodless surgical field. Exsanguination is achieved via Esmarch bandage elevation.
- Positioning: The patient is positioned supine with the operative extremity extended on a radiolucent hand table. Loupe magnification (2.5x to 3.5x) is highly recommended for precise handling of the flexor sheath and collateral ligaments.
Surgical Technique: Step-by-Step
- Incision and Exposure: Approach the joint through a V-shaped (Bruner-type) or similar zigzag incision, precisely centered at the PIP joint crease. This prevents postoperative flexion contractures associated with straight longitudinal incisions.
- Flexor Sheath Management: Carefully elevate the skin flaps, protecting the neurovascular bundles bilaterally. Identify the flexor tendon sheath. Incise the A3 pulley on the side corresponding to the apex of the skin flap. This preserves the critical A2 and A4 pulleys, preventing postoperative flexor tendon bowstringing.
- Tendon Retraction and Volar Plate Detachment: Gently retract both the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons laterally using a smooth retractor. Identify the palmar (volar) plate. Detach the palmar plate proximally from its origin on the proximal phalanx, reflecting it distally to expose the articular surfaces.
- Collateral Ligament Release: Release the collateral ligaments partially or completely from their origins on the condyles of the proximal phalanx. This critical step allows the joint to be "shotgunned," providing nearly 180 degrees of joint extension and unparalleled visualization of the articular surfaces.
- Bone Resection: Utilizing an oscillating micro-saw, perform a transverse osteotomy through the neck of the proximal phalanx, resecting the diseased condyles.
Clinical Pearl: Do not resect the base of the middle phalanx. Preserving the middle phalangeal base is paramount to maintaining digital length and preserving the distal insertions of the collateral ligaments and the central slip.
- Canal Preparation: Prepare the medullary canals of both the proximal and middle phalanges using specialized square broaches. The square geometry is critical; it creates a matching cavity for the implant stems, preventing postoperative malrotation and toggling of the prosthesis.
- Provisional Sizing and Trialing: Insert provisional "sizing" implants. Reduce the joint and assess the range of motion, soft tissue tension, and digital alignment. If the joint is too tight, additional minimal bone resection from the proximal phalanx may be required.
- Implant Insertion: Once the correct size is determined, insert the permanent silicone elastomer implant. In this specific technique, the implant is inserted without metal grommets.
- Soft Tissue Reconstruction:
- If anatomically possible, reattach the collateral ligaments to the proximal phalanx using micro-drill holes or suture anchors to restore lateral stability.
- Split the detached palmar plate longitudinally. Suture these split halves to reinforce the collateral ligaments, creating a robust volar-lateral restraint against subluxation.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with non-absorbable monofilament sutures. Apply a nonadherent gauze bandage supported by a bulky, well-padded volar resting splint.
Postoperative Rehabilitation Protocol
The success of a palmar approach PIP arthroplasty relies heavily on strict adherence to a structured rehabilitation protocol.
- Week 1: The initial bulky dressing is removed within the first 5 to 7 days. A dynamic PIP dorsal outrigger extension splint, incorporating a middle phalangeal block, is fabricated and applied.
- Weeks 1-4: The dynamic splint is worn continuously. Active flexion against the resistance of the rubber bands allows for graduated strengthening of the flexor apparatus while the dynamic extension assists in preventing extensor lag. Active and passive exercises are initiated under the guidance of a certified hand therapist. Blocking techniques and resting extension splints are utilized at night to prevent flexion contractures.
- Weeks 4-6: The dynamic extension splint is gradually discontinued based on the patient's active range of motion and joint stability.
- Months 1-3: Side-to-side "buddy" taping to the adjacent digit is strongly encouraged for up to 3 months during strenuous activities to provide collateral support and prevent rotational stress on the healing capsule.
Alternative: Volar Plate Interposition Arthroplasty
Volar plate interposition into the PIP joint remains a viable biological alternative to silicone implant arthroplasty, particularly in younger patients or those with a history of infection. Although technically more demanding—requiring meticulous mobilization of the volar plate and secure dorsal fixation—long-term outcome studies suggest this technique provides durable clinical results with a lower risk of catastrophic failure compared to synthetic implants.
DISTAL INTERPHALANGEAL JOINT DEFORMITIES
Rheumatoid involvement of the distal interphalangeal (DIP) joint frequently presents as a mallet deformity (hyperflexed DIP joint) or a hyperextensible DIP joint.
Pathoanatomy
- Rheumatoid Mallet Finger: This hyperflexed posture may occur in isolation due to the attenuation or rupture of the terminal extensor tendon at its insertion on the distal phalanx. Alternatively, it may present as a secondary compensatory mechanism in conjunction with a swan-neck deformity (PIP hyperextension leading to profound profundus tension and terminal slip laxity).
- Hyperextensible DIP Joint: This deformity is typically related to the severe attenuation of the volar capsuloligamentous structures or secondary to an unrecognized flexor digitorum profundus (FDP) tendon rupture.
Surgical Management
The gold standard for painful, unstable, or severely deformed rheumatoid DIP joints is arthrodesis. Fusion provides a stable, pain-free pinch grip. The joint is typically fused in neutral to 5 degrees of flexion using headless compression screws, dorsal tension band wiring, or crossed Kirschner wires.
Strategic Surgical Decision Making: In a patient who has already undergone, or is concurrently undergoing, a PIP joint arthrodesis, a mild to moderate DIP joint mallet deformity might be intentionally left untreated. The small amount of residual mobility remaining in the unfused DIP joint can contribute significantly to overall fingertip function and spatial adaptation during pinch activities.
ULNAR DRIFT AND METACARPOPHALANGEAL JOINT DEVIATION
Ulnar drift (deviation of the fingers at the MCP joints) is the hallmark deformity of the rheumatoid hand, though it can be observed in other connective tissue disorders. It is a complex, multi-planar deformity involving ulnar deviation, volar subluxation, and pronation of the proximal phalanges.

Clinical presentation of severe ulnar deviation of the fingers in a patient with advanced rheumatoid arthritis.
Biomechanical Predisposing Factors in the Normal Hand
Even in the absence of systemic disease, the normal human hand possesses inherent anatomical asymmetries that predispose the digits to ulnar drift under pathological stress:
- Inherent Ulnar Deviation: The normal resting posture of the MCP joints naturally favors slight ulnar deviation, particularly in the index finger.
- Asymmetrical Metacarpal Heads: The metacarpal heads are asymmetrical; the ulnar condyles are smaller and exhibit a steeper slope compared to the radial condyles, especially in the index and middle fingers, providing less bony resistance to ulnar translation.
- Tendon Approach Angles: Both the long flexor and extensor tendons approach the MCP joints from a slightly ulnar angle originating from the wrist, creating a constant ulnar-directed vector force during active contraction.
- Ligamentous Kinematics: When the MCP joints are flexed, the radial collateral ligaments permit a greater degree of ulnar deviation than the ulnar collateral ligaments permit radial deviation.
- Intrinsic Muscle Imbalance: The ulnar-sided intrinsic muscles (abductor digiti quinti and flexor digiti quinti) possess greater cross-sectional area and contractile strength than their radial counterparts (e.g., the third volar interosseous).
The Pathological Cascade in the Rheumatoid Hand
In rheumatoid arthritis, aggressive synovitis acts as the catalyst, amplifying these normal predisposing factors into a destructive cascade:
- Capsular Distension: Florid MCP joint synovitis physically distends and weakens the dorsoradial capsular restraints and the radial collateral ligament.
- Volar Displacement: The volarly directed vector forces of the powerful flexor tendons stretch the weakened collateral ligaments, permitting volar subluxation of the proximal phalanges.
- Flexor Tendon Shift: Stretching of the accessory collateral ligaments and the flexor tunnels permits the long flexor tendons to displace ulnarly within their sheaths, exacerbating the ulnar deforming force during every power grip.
- Intrinsic Contracture: Chronic inflammation leads to interosseous muscle contracture. This intrinsic tightness causes profound ulnar deviation and PIP joint hyperextension (initiating a swan-neck deformity), alongside MCP joint flexion and eventual fixed subluxation.
- Sagittal Band Attenuation: The radial sagittal bands become attenuated and eventually rupture, allowing the long extensor tendons to slide ulnarward into the intermetacarpal valleys (webs). Once displaced volarly to the axis of rotation, the extensors paradoxically act as flexors and ulnar deviators.
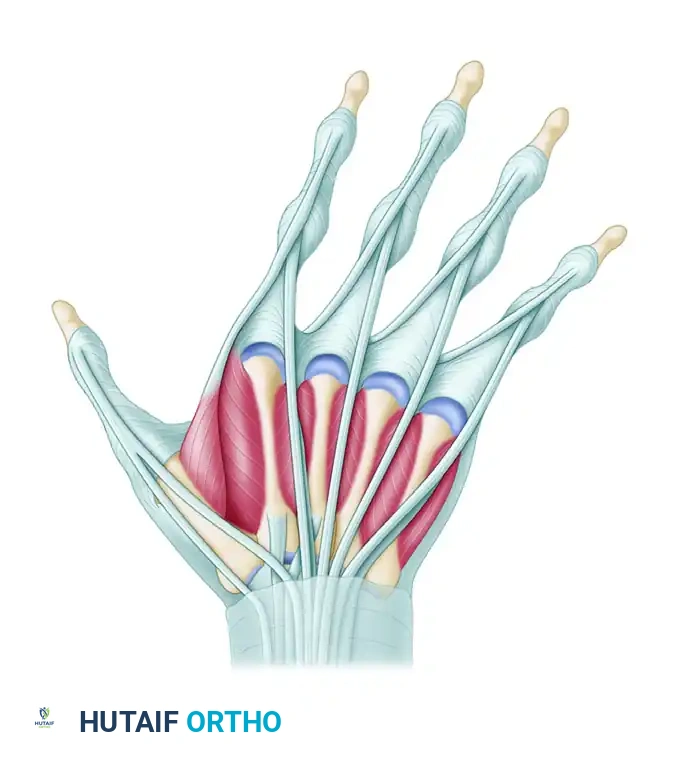
Anatomical diagram demonstrating the attenuation of the radial sagittal bands, allowing the extensor tendons to shift ulnarward into the intermetacarpal webs, exacerbating the deforming forces.
- Wrist Level Ruptures: Long extensor tendon rupture at the level of the wrist (often due to attrition over a prominent distal ulna, known as Vaughan-Jackson syndrome) further destabilizes the extensor apparatus, increasing the probability of complete MCP joint dislocations.
Surgical Management of Mild-to-Moderate Ulnar Drift
In the surgical treatment of mild-to-moderate ulnar drift, reasonable success is possible only when the major deforming forces have been properly evaluated and addressed. "Mild-to-moderate" implies the absence of severely destroyed articular cartilage and the absence of fixed, irreducible joint dislocations.
Often, the flexor and extensor tendons are already displaced ulnarward, the intrinsic muscles are imbalanced, and the joints remain swollen with active pannus.
Indicated Soft Tissue Procedures:
* MCP Joint Synovectomy: Meticulous removal of the destructive synovial pannus to halt capsular distension and cartilage degradation.
* Extensor Tendon Realignment: Relocation of the ulnarly subluxated extensor tendons back to the dorsal apex of the metacarpal head, often requiring reefing or reconstruction of the radial sagittal band and release of the ulnar sagittal band.
* Intrinsic Release or Transfer: Release of the tight ulnar intrinsic insertions (e.g., the ulnar lateral band of the index finger) to eliminate the deforming pull. In some cases, the released ulnar intrinsic tendon can be transferred to the radial aspect of the adjacent ulnar digit to augment radial stability (crossed intrinsic transfer).
Surgical Pitfall: While dorsal and intrinsic rebalancing is highly effective, no reliable, long-lasting operation has been devised to easily realign volarly and ulnarly displaced flexor tendons and their sheaths. Surgeons must rely on correcting the dorsal and intrinsic forces to counteract the flexor vectors.
Surgical Management of Severe Deformity
In cases of severe, fixed ulnar drift with advanced articular destruction and irreducible volar subluxation, soft tissue rebalancing alone is insufficient.

Radiographic progression: (A) Severe subluxation and ulnar drift of the metacarpophalangeal joints in advanced rheumatoid arthritis. (B) Postoperative result following resection arthroplasty of the metacarpal heads, indicated when intrinsic release and soft tissue realignment provide insufficient correction for fixed bony deformities.
For these advanced stages, Silicone Metacarpophalangeal Joint Arthroplasty (Swanson technique or similar) combined with comprehensive soft tissue reconstruction (extensor centralization and intrinsic release) remains the gold standard. Resecting the metacarpal heads decompresses the joint, corrects the volar subluxation, and provides a stable, aligned fulcrum for the reconstructed soft tissue envelope to function against, dramatically improving hand function and cosmesis.
You Might Also Like

