Comprehensive Management of Painful Amputation Stumps and Hand Reconstruction
Key Takeaway
The management of painful amputation stumps and subsequent hand reconstruction requires a meticulous, evidence-based approach. Pain is frequently driven by terminal neuromas, inadequate soft-tissue coverage, or bony prominences. Reconstructive options range from local advancement flaps and neuroma excision to complex procedures like the Krukenberg operation and thumb pollicization. This guide provides a comprehensive overview of surgical indications, biomechanics, step-by-step operative techniques, and postoperative protocols to optimize functional outcomes in upper extremity amputees.
PATHOPHYSIOLOGY AND EVALUATION OF THE PAINFUL AMPUTATION STUMP
Revision surgery is a frequent and highly specialized elective procedure for the management of painful amputation stumps, particularly those resulting from high-energy traumatic injuries. The etiology of stump pain is multifactorial, but a terminal neuroma located in an unpadded, mechanically vulnerable area near the distal end of the stump remains the most common culprit.
Following nerve transection, Wallerian degeneration occurs distally, while the proximal stump attempts regeneration. Without a distal endoneurial tube to guide them, regenerating axons, Schwann cells, and fibroblasts form a disorganized, bulbous mass—the neuroma. When this mass is tethered to scar tissue or positioned directly beneath thin skin, normal tactile pressure translates into severe neuropathic pain.
Diagnostic Criteria
A well-localized area of extreme tenderness associated with a palpable small mass, usually in line with a native digital nerve, is pathognomonic for a symptomatic neuroma. A positive Tinel's sign at the stump apex, which may radiate proximally, further confirms the diagnosis. Diagnostic local anesthetic blocks can be utilized to differentiate neuroma-mediated pain from central phantom limb pain or proximal nerve compression.
Clinical Pearl: Pain in an amputation stump is not exclusively neurogenic. It can frequently be caused by bony prominences covered only by thin, non-glabrous skin (such as a split-thickness skin graft) or by skin rendered tight and ischemic by underlying scarring.
Non-Operative vs. Operative Management
While some painful neuromas can be managed conservatively through aggressive padding, prosthetic modifications, and rigorous desensitization therapies, surgical excision is frequently required for definitive relief.
When surgical intervention is indicated, the neuroma must be meticulously dissected free from the surrounding scar bed. The nerve is then placed under gentle traction and sharply divided at a more proximal level, allowing the newly transected end to retract into a healthy, well-padded soft-tissue bed (often deep into a muscle belly or transposed into a drilled bone hole).
An alternative technique involves suturing the radial and ulnar digital nerves end-to-end (centrocentral neurorrhaphy) to create a closed neural loop. While this end-to-end nerve union has been shown to reduce localized tenderness, it does so at the expense of distal touch sensibility and has not been definitively proven to reduce resting pain or cold intolerance compared to standard proximal resection.


SOFT TISSUE AND BONY CONTOURING
In instances where pain is driven by inadequate soft-tissue coverage over a bony prominence, revision surgery must address both the skeletal and integumentary components. Excising the thin skin or scar, shortening the underlying bone, and applying a sufficiently padded, sensate graft or flap is indicated.
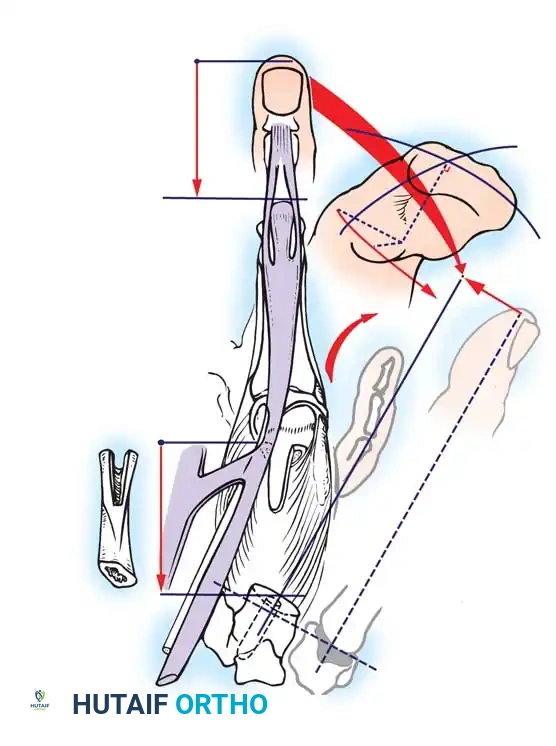
The Moberg Advancement Flap
Amputation stumps that are painful due to thin skin coverage at the pulp and nail junction can be significantly improved by utilizing a limited volar advancement flap, classically described by Moberg.


Surgical Principles of the Moberg Flap:
* Design: The flap is outlined over the volar aspect of the digit, incorporating both neurovascular bundles to ensure robust perfusion and preserved sensibility.
* Elevation: The flap is raised deep to the neurovascular bundles, separating them from the flexor tendon sheath.
* Advancement: The flap is advanced distally (typically up to 1.5 cm) to cover the terminal defect.
* Limitations: In the fingers (unlike the thumb), proximal dissection to develop these flaps should not extend proximal to the proximal interphalangeal (PIP) joint. Extending beyond this point risks devascularization and severe flexion contractures.
Surgical Warning: Painful cramping sensations in the hand and forearm can be caused by flexion contracture of a stump resulting from the overstretching of extensor tendons or the adherence of flexor tendons to the distal bone. Surgical release of any adherent tendons and restoration of the flexor-extensor balance is critical during stump revision.
RECONSTRUCTIONS AFTER AMPUTATION OF THE HAND
When amputation occurs at the level of the wrist or distal forearm, restoring prehension is the primary reconstructive goal. While myoelectric and body-powered prostheses are standard, the Krukenberg operation remains a highly functional, albeit cosmetically controversial, biologic alternative.
The Krukenberg Operation: Biomechanics and Indications
The Krukenberg procedure converts the forearm into a sensate pincer by separating the radius and ulna into two independent, opposing rays. Its primary advantage over prosthetic rehabilitation is the preservation of tactile sensibility and proprioception. This makes it an exceptionally valuable procedure for bilateral upper extremity amputees, particularly those who are blind, as it allows them to interact with their environment using direct sensory feedback.
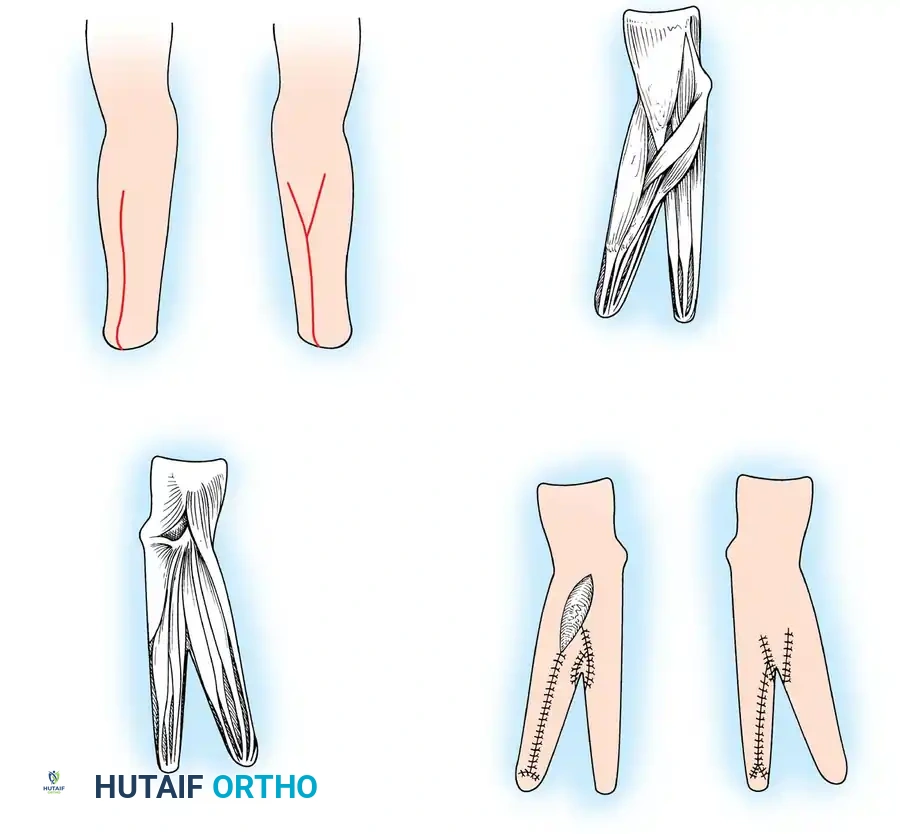
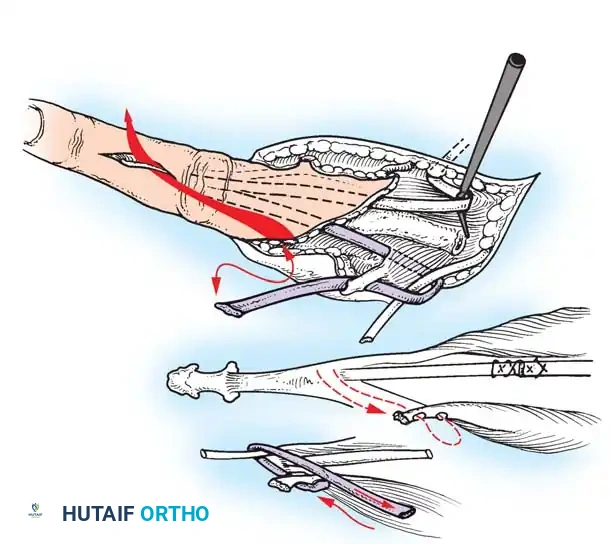
🔪 Surgical Technique: The Krukenberg Procedure (Technique 14-14)
- Incision and Flap Design: Make a longitudinal incision on the flexor surface of the forearm, biased slightly toward the radial side. Make a corresponding incision on the dorsal surface, biased toward the ulnar side. On the dorsal surface, elevate a V-shaped flap to form the new web space at the proximal junction of the rays.
- Muscle Separation: Systematically separate the forearm musculature into two distinct functional groups:
- Radial Ray (Adductors/Abductors): Comprises the radial wrist flexors and extensors, the radial half of the flexor digitorum sublimis (FDS), the radial half of the extensor digitorum communis (EDC), the brachioradialis, the palmaris longus, and the pronator teres.
- Ulnar Ray (Adductors/Abductors): Comprises the ulnar wrist flexors and extensors, the ulnar half of the FDS, and the ulnar half of the EDC.
- Debulking: If the muscle mass makes the stump too bulky or precludes tension-free skin closure, resect the pronator quadratus, flexor digitorum profundus (FDP), flexor pollicis longus (FPL), abductor pollicis longus (APL), and extensor pollicis brevis (EPB).
- Crucial Step: Take absolute care not to disturb the pronator teres, as it is the primary motor for the radial ray.
- Interosseous Membrane Division: Incise the interosseous membrane longitudinally along its ulnar attachment. Extreme caution must be exercised to preserve the anterior interosseous artery and nerve.
- Osteotomy and Alignment: The radial and ulnar rays should separate 6 to 12 cm at their tips. Motion occurs proximally at the radiohumeral and proximal radioulnar joints. The opposing distal ends of the rays must touch during active closure; if they do not, perform a corrective osteotomy of the radius or ulna.
- Skin Coverage: Excise excess subcutaneous fat. Rotate the skin around each ray and close it so that the suture lines do not lie on the opposing (contact) surfaces of the pincers. Apply split-thickness skin grafts to any remaining defects, ensuring the tactile contact surfaces are covered by sensate, full-thickness skin.
- Closure and Drainage: Suture the dorsal V-flap into the proximal junction to create the web. Insert small rubber drains, obtain meticulous hemostasis after tourniquet deflation, and apply a bulky compression dressing with the rays separated by at least 6 cm.
Postoperative Protocol: The limb is strictly elevated for 3 to 4 days to minimize edema. Sutures are removed at 14-21 days. Intensive rehabilitation begins at 2 to 3 weeks to train the patient in independent abduction and adduction of the newly formed rays.

RECONSTRUCTION AFTER AMPUTATION OF MULTIPLE DIGITS
Severe crush injuries or industrial accidents often result in the amputation of multiple digits. Once initial debridement and soft-tissue stabilization are achieved, several reconstructive avenues exist.
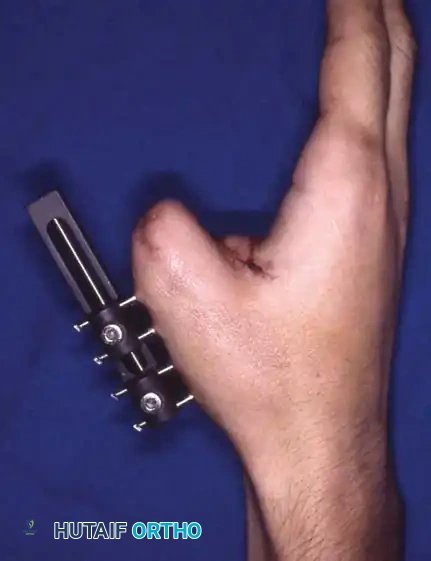
Digital lengthening by callotasis (distraction osteogenesis) is a viable option for lengthening short metacarpal or phalangeal stumps. When transposition of remaining digits is feasible, thumb pollicization may be required to restore opposition. The restoration of a functional grasp utilizing sensate, opposable digits often necessitates a protracted, multi-staged reconstructive course that challenges both the creativity of the surgeon and the psychological resilience of the patient.

RECONSTRUCTION OF THE THUMB
The thumb is the cornerstone of hand biomechanics. Traumatic or congenital absence of the thumb causes a severe deficiency in prehension, generally constituting a 40% disability of the hand as a whole.
Before committing to thumb reconstruction, the surgeon must evaluate the length of the remaining thumb segment, the functional status of the remaining digits, the patient's occupational demands, and the status of the contralateral hand. If the opposite thumb is entirely normal, the absolute necessity of complex reconstruction in an older patient may be questioned; however, in young, active patients, reconstruction is highly indicated.
The Five Pillars of Thumb Reconstruction
A successfully reconstructed thumb must meet five non-negotiable biomechanical and functional requirements:
1. Sensibility: The contact area must possess protective and tactile sensibility. While it need not be perfectly normal, it must be painless and sufficient for stereognosis during pinch.
2. Stability: The skeletal architecture must withstand pinch pressure without joint collapse, deviation, or shifting of the soft-tissue pad.
3. Mobility: The basal joint (CMC) must possess sufficient mobility to allow the thumb to pronate and oppose the fingers, and to extend to allow the hand to flatten.
4. Length: The thumb must be long enough to comfortably meet the opposing digital tips. In cases where the remaining fingers are stiff or amputated, a greater-than-normal thumb length may be required.
5. Cosmesis: The reconstruction must be cosmetically acceptable; a functionally adequate but aesthetically displeasing thumb will often be hidden by the patient and excluded from use.
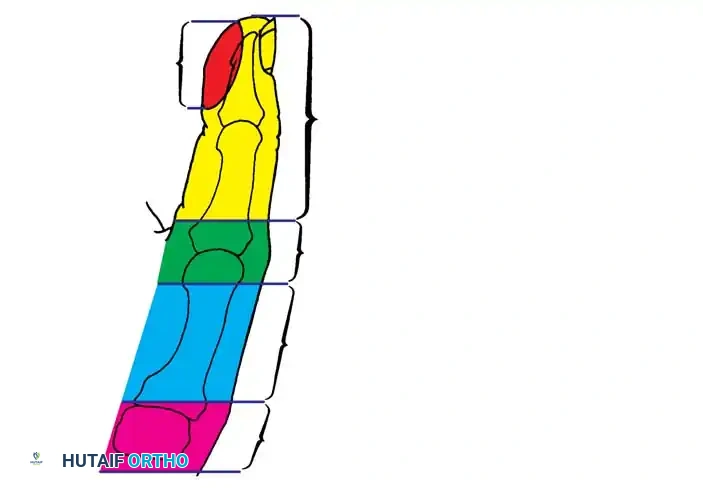
Levels of Amputation and Reconstructive Choice
- Distal to the IP Joint: Only appropriate soft-tissue coverage is necessary. If sensibility in the pinch area is grossly impaired, a neurovascular island transfer may be indicated.
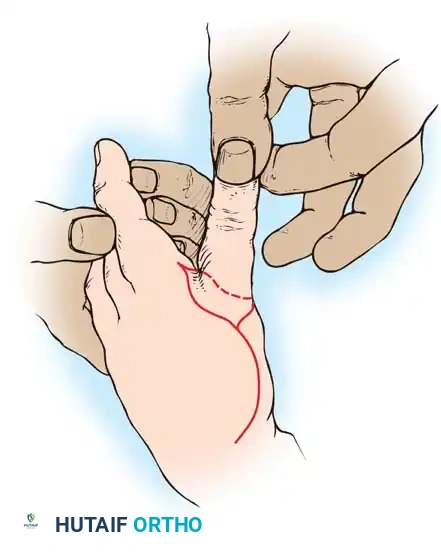
- At the MCP Joint or Proximal Phalanx: The thenar muscles usually remain intact, stabilizing the digit. Deepening of the thumb web via Z-plasty or lengthening of the metacarpal by bone grafting (Gillies-Millard technique) is indicated.
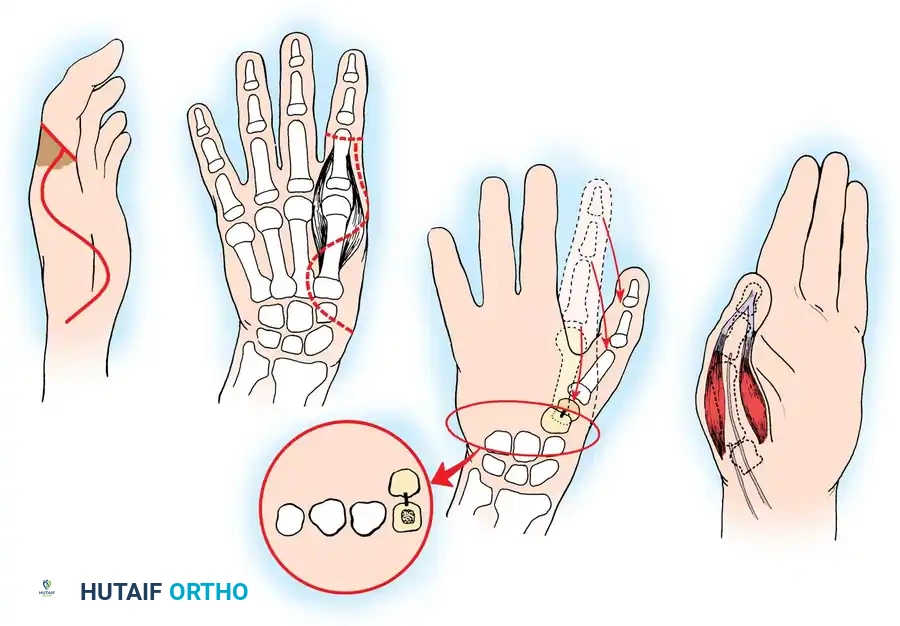
- Proximal Metacarpal/CMC Joint: Requires complex reconstruction such as pollicization of the index finger or microvascular toe-to-hand transfer.

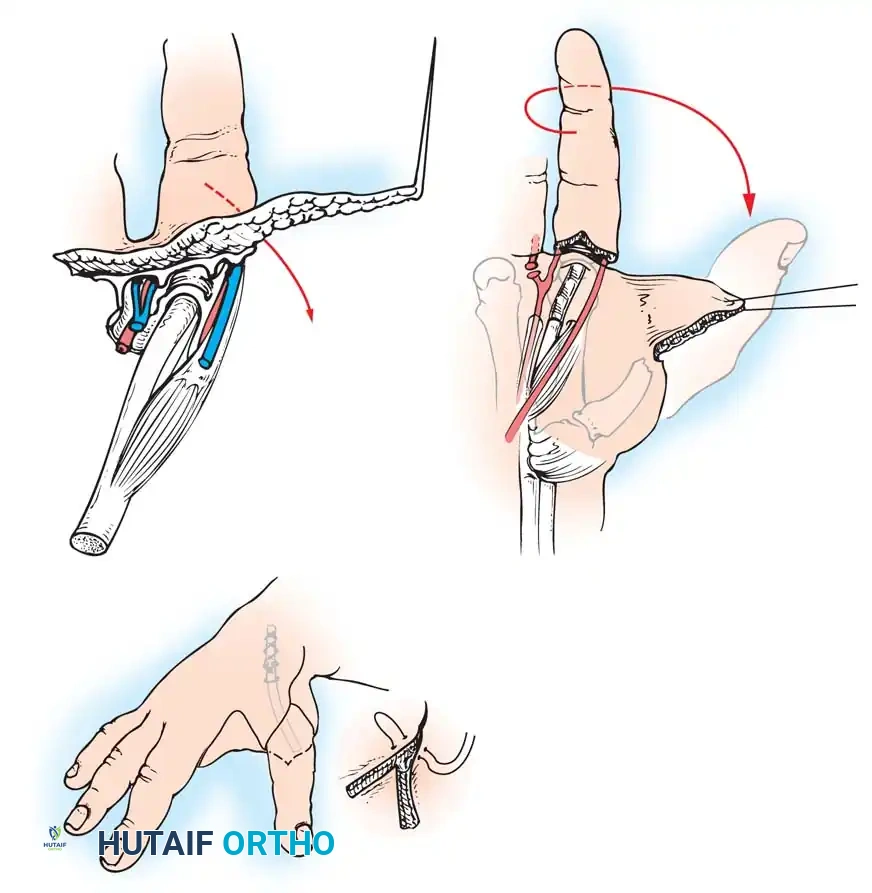
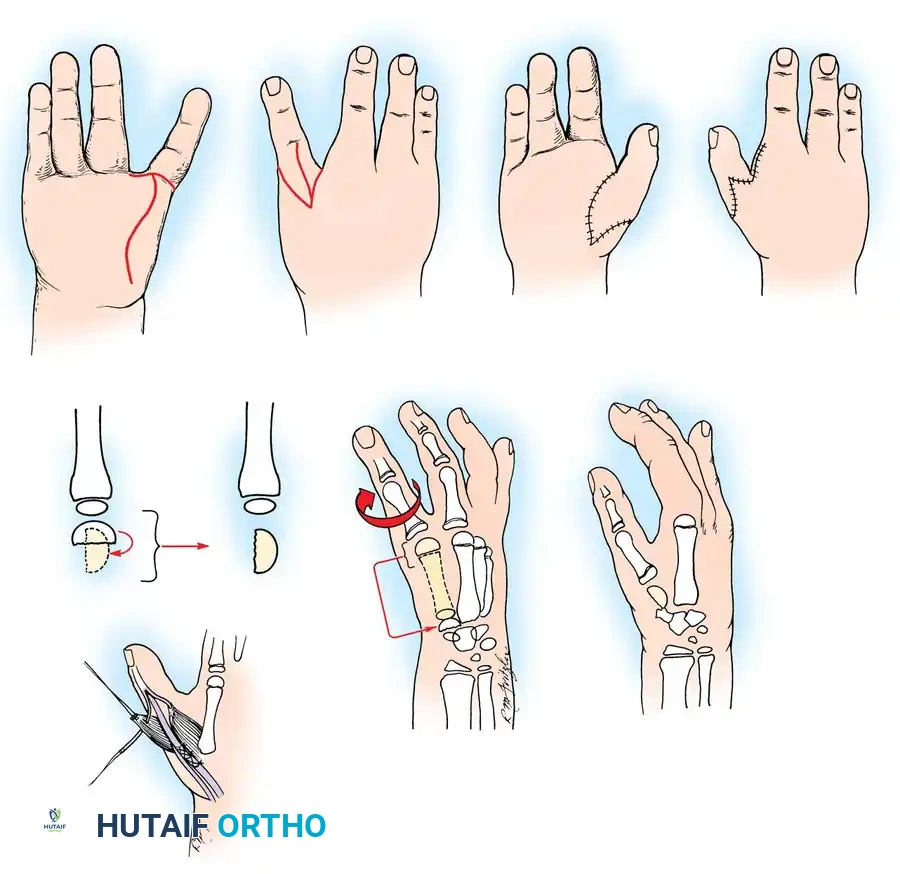
🔪 Surgical Technique: Metacarpal Lengthening and Local Flap (Gillies-Millard "Cocked Hat" Procedure)
When amputation occurs at the metacarpophalangeal joint or within the condylar area of the first metacarpal, the intrinsic thenar musculature is preserved. The Gillies-Millard technique lengthens the skeletal ray using a bone graft while advancing local sensate skin to cover the new tip.
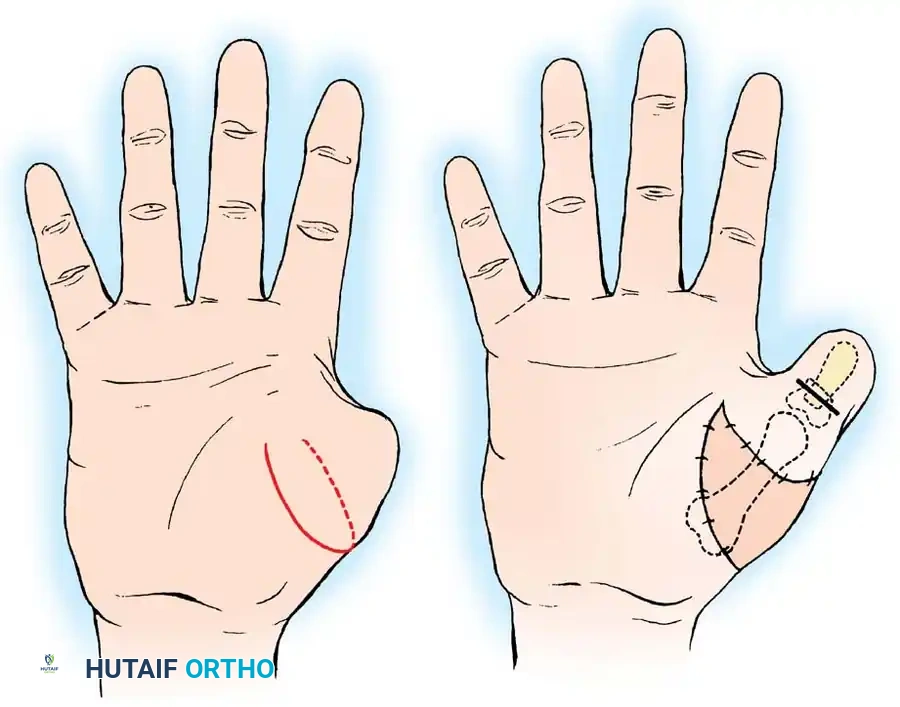
- Incision: Make a curved, horseshoe-shaped incision around the dorsal, radial, and volar aspects of the base of the thumb.
- Flap Elevation: Undermine the skin distally, staying strictly superficial to the main venous drainage network to prevent venous congestion and subsequent flap necrosis. Continue undermining until a hollow, thimble-like flap has been elevated and slipped off the end of the bony stump. The blood supply to this flap is maintained via the arborization of vessels around the base of the index finger in the thumb web.
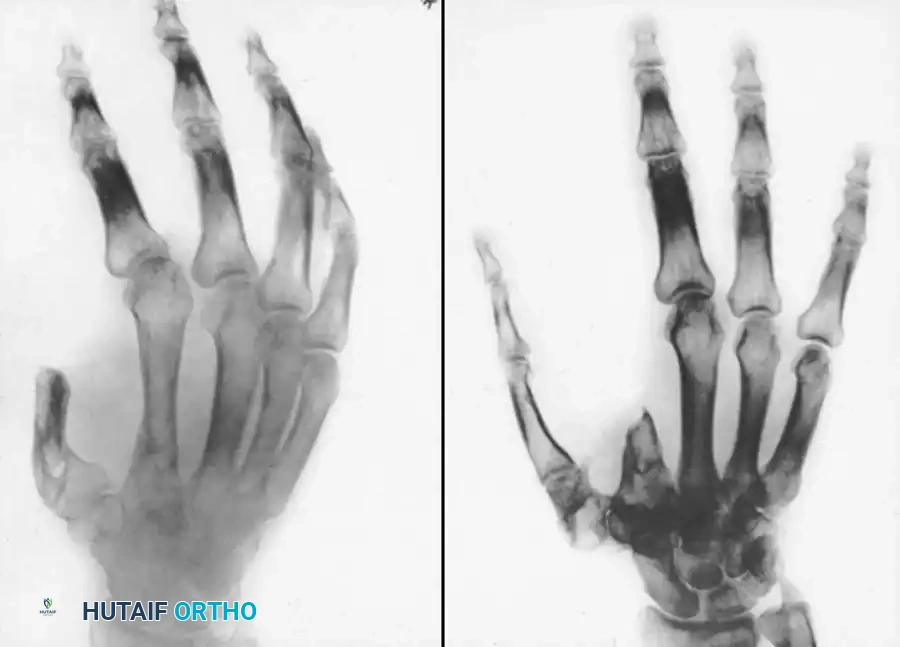
Associated Surgical & Radiographic Imaging


You Might Also Like

