Orthopaedic Hand Surgery Instruments & Tourniquet Protocols

Key Takeaway
Precision in hand surgery demands specialized instruments and meticulous hemostasis. This guide details the biomechanics and selection of soft tissue, osseous, and microvascular tools. It further provides evidence-based protocols for tourniquet application, exsanguination, and ischemia management, ensuring optimal surgical exposure while minimizing neurovascular complications and metabolic disturbances during prolonged operative procedures.
OPTIMIZING THE SURGICAL FIELD: INSTRUMENTATION AND HEMOSTASIS
The margin between functional restoration and iatrogenic morbidity in hand and upper extremity surgery is exceptionally narrow. The intricate anatomy of the hand—comprising densely packed neurovascular bundles, delicate flexor tendon pulleys, and complex articular geometries—demands absolute precision. Achieving this precision relies on two foundational pillars: the selection of appropriate, highly specialized surgical instruments and the meticulous management of a bloodless surgical field via pneumatic tourniquets.
This comprehensive guide details the biomechanics, indications, and handling of essential hand surgery instruments, alongside evidence-based protocols for tourniquet application, exsanguination, and the physiological management of limb ischemia.
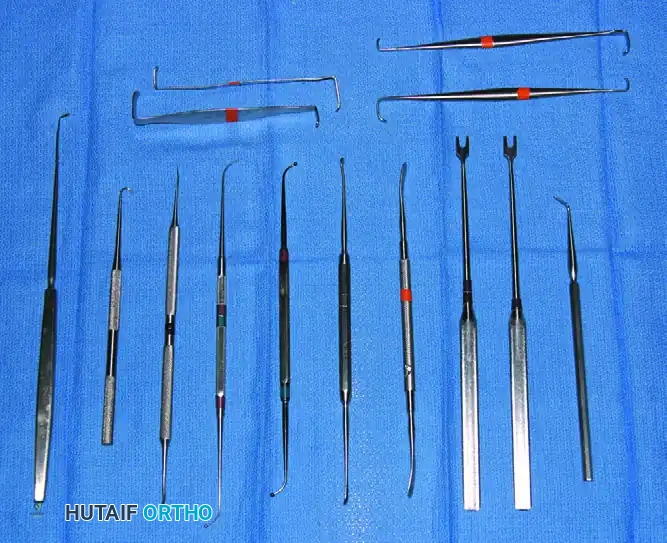
ERGONOMICS AND BASIC SOFT TISSUE INSTRUMENTS
For the accurate work required in hand surgery, instruments must feature fine, atraumatic points. However, the handles must be disproportionately large relative to the tips. This ergonomic design is critical; a larger handle allows the surgeon to maintain a firm, secure "pencil grip" or "palmar grip" without over-recruiting the intrinsic muscles of the hand, thereby minimizing fatigue and physiological tremor during prolonged micro-dissection.
The four basic instruments in the hand surgeon's armamentarium are the scalpel (knife), small forceps, dissecting scissors, and the mosquito hemostat.
The Scalpel and Principles of Dissection
The knife blade must be firmly attached to the handle and changed frequently to maintain a flawless cutting edge. In hand surgery, the scalpel should be utilized for the vast majority of dissection.
Surgical Pearl: Avoid the temptation to tear through tissues with blunt instruments. Blunt dissection in the hand disrupts the delicate paratenon, epineurium, and fine fascial planes, leading to excessive postoperative scarring, tendon tethering, and compromised functional outcomes. Sharp dissection respects tissue planes and minimizes the inflammatory cascade.
Forceps and Tissue Handling
Forceps must be carefully inspected prior to surgery to ensure absolute cleanliness and precision of closure. Debris trapped in the teeth or misaligned jaws will crush delicate tissues rather than securely grasping them. For skin and robust fascia, fine-toothed forceps (e.g., Adson or Brown-Adson) are preferred as they puncture rather than crush. For nerves and vessels, smooth, non-toothed jeweler's forceps are mandatory.
Dissecting Scissors
Scissors utilized in the hand should feature sharp, double points and are preferably curved (e.g., Stevens tenotomy scissors). The curvature serves a dual biomechanical purpose: it improves the surgeon's line of sight into deep, narrow wounds, and it allows the tips to point away from critical structures when dissecting along the longitudinal axis of neurovascular bundles.
Hemostats and Electrocautery
A mosquito hemostat or a specialized micro-forceps is the instrument of choice for clamping vessels, as their fine tips cause minimal collateral tissue damage.
Surgical Warning: Vessels must be clamped precisely as they are visualized, even when a tourniquet is inflated. Blind clamping in a bloodless field risks incorporating adjacent digital nerves into the hemostat, leading to devastating iatrogenic neuromas.
While monopolar electrocautery is standard in general orthopaedics, an electric cautery of the bipolar type is strongly recommended in hand surgery. Bipolar cautery ensures that the electrical current passes only between the two tips of the forceps, preventing the current from channeling down a vessel and causing thermal necrosis to an adjacent digital nerve.
RETRACTORS AND SURGICAL EXPOSURE
Optimal exposure without tissue ischemia is the goal of retraction. Retractors in hand surgery should generally be of the small single-hook or double-hook variety (e.g., Senn or skin hooks).
A critical design feature of hand retractors is the handle length. Handles must be long enough to keep the surgical assistant’s hands entirely out of the primary surgeon’s working area and line of sight. Small self-retaining retractors (such as miniature Weitlaner or Gelpi retractors) are highly useful in specific situations, such as maintaining exposure during a carpal tunnel release or palmar fasciectomy, provided they are not opened under excessive tension which could cause skin edge necrosis.
OSSEOUS INSTRUMENTS AND POWER EQUIPMENT
Surgical intervention on the phalanges, metacarpals, and carpal bones requires miniaturized osseous instruments that provide high precision without compromising the structural integrity of these small bones.

Drills and Kirschner Wires
For drilling holes in bone, the small steel twist drill points provided in most modular surgical drill sets are highly satisfactory. Small, sharp-pointed Kirschner wires (K-wires) are frequently required for provisional or definitive fracture fixation.
Air-powered or battery-powered modular drills allow for the precise placement of drill holes and wires. When utilizing power equipment on small bones, the surgeon must be acutely aware of thermal necrosis. Bone temperatures exceeding 47°C for more than one minute result in irreversible osteocyte death and subsequent pin-tract loosening or infection. Copious chilled saline irrigation must be applied directly to the drill bit-bone interface during all power drilling.
MICROVASCULAR AND NERVE REPAIR INSTRUMENTS
The advent of microsurgery has necessitated a specialized subset of instruments designed for the repair of vessels and nerves measuring less than 2 mm in diameter.

Needle holders used for microvascular anastomoses or epineurial repairs must feature narrow noses and perfectly smooth jaws. Textured jaws, common in macro-surgery, will fray and compromise the tensile strength of fine monofilament sutures (e.g., 8-0 to 10-0 nylon). Castroviejo-style needle holders with a spring-loaded locking mechanism allow for fluid, rotational wrist movements without the jarring "click" of traditional ratcheted holders.
Numerous varieties of braided and nonbraided sutures are available to meet specific procedural requirements. Most sutures utilized in hand surgery are swaged onto straight or curved atraumatic needles to minimize the tissue drag associated with eyed needles.
Optical Magnification
Fine surgery on soft tissues, particularly digital nerve repairs and arterial anastomoses, cannot be performed safely with the naked eye.
Surgical loupes are mandatory. It is possible to achieve a magnification of up to 6× with magnification lenses mounted directly onto a glasses frame. However, if more than 6× magnification is required (such as for distal digital artery replantation), the magnification lenses become too heavy and ergonomically prohibitive for frame mounting. In these instances, a free-standing operating microscope is required.
TOURNIQUET PROTOCOLS AND ISCHEMIA MANAGEMENT
A completely bloodless field is an absolute prerequisite for the safe identification of the intricate neurovascular anatomy of the upper extremity. This is achieved through the disciplined use of pneumatic tourniquets.
Exsanguination Techniques
Prior to tourniquet inflation, the limb must be thoroughly exsanguinated. This can be achieved via two primary methods:
1. Gravity Elevation: The limb is elevated at 60 degrees for 2 to 5 minutes. This allows for adequate venous drainage and is the preferred method for patients with active infections in the limb or in whom malignant tumors are suspected, as it prevents the proximal mechanical seeding of pathogens or tumor cells.
2. Elastic Compression: Wrapping the limb with a Martin elastic bandage (approximately 10 cm wide), beginning tightly at the fingertips and proceeding proximally to just distal to the tourniquet edge.
Pitfall: Wrapping of the limb with an elastic bandage is strictly contraindicated in patients with purulent infections, suspected malignancies, or known deep vein thrombosis (DVT) in the affected extremity. In these cases, rely solely on gravity elevation for 5 to 10 minutes prior to inflation.
Tourniquet Application and Positioning
The standard procedure for tourniquet application involves wrapping several layers of cast padding (e.g., Webril) smoothly around the middle of the upper arm, near the axilla.
The tourniquet should be applied by the operating surgeon, an experienced surgical assistant, or the anesthesiologist. Wrinkles in the padding must be strictly avoided. The presence of wrinkles creates focal areas of high pressure that can cause severe friction blisters, pinching of the skin, and full-thickness dermal necrosis.
Wider tourniquet cuffs are generally preferred as they distribute pressure over a larger surface area, thereby minimizing focal compression and mechanical shearing of the underlying peripheral nerves (e.g., the radial nerve at the spiral groove). However, appropriately sized smaller cuffs are required for pediatric patients to ensure a proper fit.
Forearm vs. Upper Arm Tourniquets
While the tourniquet is traditionally applied to the proximal upper arm, extensive clinical reports have indicated that forearm tourniquets are highly safe, reliable, and offer distinct advantages for specific procedures.
Forearm tourniquets are indicated for procedures lasting 25 minutes or less, or for surgeries located strictly distal to the wrist joint, particularly when performed under regional block anesthesia.
The advantages of a forearm tourniquet include:
* Decreased Anesthetic Requirement: The dosage of local anesthetic required for a regional block can be decreased to almost half of that required to tolerate an upper arm tourniquet.
* Reduced Tourniquet Pain: The frequency and severity of ischemic tourniquet pain are significantly less with a forearm placement.
* Prolonged Analgesia: Both a longer duration of intraoperative sensory block and prolonged postoperative analgesia have been described when utilizing a forearm tourniquet.
For minor procedures performed under local infiltration or a simple wrist block, an elastic wrap tourniquet (Esmarch) can be utilized. The bandage is wrapped tightly beginning distally at the hand and proceeding up to the mid-forearm. The overlapped layers in the mid-forearm are left in place to act as the tourniquet until the operation is finished. Alternatively, a pneumatic tourniquet can be applied just below the elbow and left inflated for up to 30 minutes without causing the patient extreme discomfort.
Inflation Pressures and Automatic Systems
With modern automatic tourniquets, inflation is rapid enough to instantly occlude arterial inflow, avoiding the trapping of excessive venous blood in the arm during the inflation phase.
Evidence-Based Guideline: The tourniquet inflation pressure should generally not exceed 100 mm Hg above the patient's systolic blood pressure for both adults and children. Excessive pressures do not improve hemostasis but exponentially increase the risk of neurapraxia and crush injury to the underlying musculature.
Improvements in biomedical design have resulted in "automatic" pneumatic tourniquets that allow for the precise setting of pressures within a safe range and for specific, monitored periods of time. These systems feature integrated alarms that notify the surgeon and anesthesiologist when safe time thresholds are approaching.
The Metabolic Consequences of Tourniquet Ischemia
The maximum safe duration for continuous tourniquet ischemia in the upper extremity is generally accepted to be 2 hours. Prolonged ischemia leads to profound local metabolic derangements, cellular hypoxia, and subsequent reperfusion injury.
Wilgis (1971) extensively documented the metabolic effects of tourniquet ischemia on the venous blood of the occluded limb. As demonstrated in the data below, prolonged ischemia results in severe local acidosis, hypoxia, and hypercapnia.
Metabolic Changes During Tourniquet Ischemia (Adapted from Wilgis, J Bone Joint Surg 1971)
* Pre-inflation: pH 7.40 | pO2 45 mm Hg | pCO2 38 mm Hg
* 0.5 Hours: pH 7.31 | pO2 24 mm Hg | pCO2 50 mm Hg
* 1.0 Hour: pH 7.19 | pO2 20 mm Hg | pCO2 62 mm Hg
* 1.5 Hours: pH 7.04 | pO2 10 mm Hg | pCO2 85 mm Hg
* 2.0 Hours: pH 6.90 | pO2 4 mm Hg | pCO2 104 mm Hg
At 2 hours, the local environment is profoundly acidotic (pH 6.9) and nearly anoxic (pO2 4 mm Hg). If the surgical procedure requires more than 2 hours, the tourniquet must be deflated to allow for a period of reperfusion (typically 15 to 20 minutes) before re-exsanguination and re-inflation.
Postoperative Tourniquet Management
When the surgical procedure is complete and the tourniquet has been released, the cuff and the underlying cotton wrapping must be removed immediately. Leaving a deflated cuff and tight padding on the extremity acts as a venous tourniquet, impeding venous return, causing severe venous congestion, and increasing the risk of postoperative hematoma formation and compartment syndrome.
Meticulous attention to these instrumentation and tourniquet protocols ensures that the orthopaedic surgeon maintains an optimal, safe surgical environment, thereby maximizing the potential for excellent functional recovery in hand and upper extremity surgery.
You Might Also Like


