Management of Finger Metacarpophalangeal Dislocations and Radial Collateral Ligament Injuries
Key Takeaway
Metacarpophalangeal (MCP) joint dislocations, though less frequent than interphalangeal dislocations, present complex pathoanatomic challenges, particularly in the index finger. Kaplan’s lesion involves the dorsal displacement of the volar plate, which becomes incarcerated between the proximal phalanx and the metacarpal head, often necessitating open reduction. Concurrently, radial collateral ligament (RCL) injuries require precise diagnosis and management to prevent chronic instability during push-off activities. This guide details the biomechanics, reduction maneuvers, and operative interventions for these injuries.
INTRODUCTION TO METACARPOPHALANGEAL JOINT TRAUMA
Traumatic injuries to the metacarpophalangeal (MCP) joints encompass a spectrum of pathologies ranging from ligamentous sprains to complex, irreducible dislocations. The MCP joint is a diarthrodial condyloid joint, inherently stabilized by a robust capsuloligamentous complex comprising the proper and accessory collateral ligaments, the volar fibrocartilaginous plate, and the dynamic support of the extrinsic and intrinsic musculotendinous units.
While interphalangeal joint dislocations are ubiquitous in orthopedic trauma, MCP dislocations are comparatively rare. However, when they do occur, they present unique pathoanatomic challenges that demand a profound understanding of hand biomechanics. Mismanagement of these injuries—whether through inappropriate closed reduction techniques for complex dislocations or the neglect of radial collateral ligament (RCL) tears—can lead to devastating functional deficits, chronic pain, and debilitating instability.
This comprehensive guide delineates the precise pathoanatomy, clinical evaluation, and evidence-based surgical management of finger MCP dislocations and RCL injuries, providing a masterclass for the practicing orthopedic surgeon.
FINGER METACARPOPHALANGEAL DISLOCATIONS
Epidemiology and Mechanism of Injury
Metacarpophalangeal dislocations occur most frequently in the index finger, followed by the little finger. The central digits (long and ring fingers) are inherently protected by the deep transverse metacarpal ligaments on both their radial and ulnar aspects, making them less susceptible to isolated dislocation.
The classic mechanism of injury is a forceful hyperextension of the digit. This sudden, violent force overwhelms the primary volar stabilizers, leading to the avulsion of the volar plate from its weakest point: the membranous proximal attachment at the volar aspect of the metacarpal neck.
Pathoanatomy: The Kaplan Complex
Understanding the pathoanatomy of a complex (irreducible) MCP dislocation is paramount. Emanuel Kaplan’s original anatomical description remains the definitive framework for understanding why these joints become locked in a dislocated position.
When the volar fibrocartilaginous plate avulses from the metacarpal neck, the proximal phalanx translates dorsally. The volar plate is dragged dorsally over the metacarpal head, becoming wedged and incarcerated between the base of the proximal phalanx and the dorsal articular surface of the metacarpal head.
This displacement creates a constricting anatomical "noose" around the metacarpal neck, effectively trapping the metacarpal head in the palm. The boundaries of this noose are defined as follows:
* Volar (Palmar): The superficial transverse metacarpal ligament of the palmar fascia.
* Dorsal: The displaced volar plate and the natatory ligament.
* Ulnar: The flexor tendons (flexor digitorum superficialis and profundus) and the pretendinous band, which are violently displaced ulnarly.
* Radial: The lumbrical muscle, which is displaced radially.
Surgical Warning: The lateral collateral ligaments, which remain attached to the proximal phalanx and the metacarpal head, become abnormally tensioned across the joint. They act as secondary tethers, locking the proximal phalanx in its abnormal dorsal and hyperextended position, rendering simple longitudinal traction entirely ineffective.
Clinical Presentation and Radiographic Evaluation
Patients with a complex MCP dislocation present with a characteristic posture: the MCP joint is slightly hyperextended, and the interphalangeal joints are flexed.
Clinical Pearl: The pathognomonic sign of a complex, irreducible MCP dislocation is a prominent puckering or dimpling of the palmar skin at the level of the distal palmar crease. This dimple is caused by the superficial transverse metacarpal ligament being pulled dorsally by the trapped metacarpal head.
Standard posteroanterior (PA), lateral, and oblique radiographs are mandatory.
* PA View: Often demonstrates a widened MCP joint space. If a sesamoid bone is present (common in the index and little fingers), it may be seen widened or displaced into the joint space, which is a definitive radiographic sign of volar plate interposition.
* Lateral View: Confirms the dorsal displacement of the proximal phalanx relative to the metacarpal head.
Closed Reduction: Principles and Techniques
MCP dislocations are classified as either simple (subluxations or reducible dislocations without volar plate incarceration) or complex (irreducible due to soft tissue interposition).
Approximately 50% of MCP dislocations can be reduced by closed means if the dislocation is incomplete or if the volar plate has not become fully wedged.
Pitfall: NEVER apply longitudinal traction to a dislocated MCP joint. Traction tightens the anatomical noose (the flexor tendons, lumbrical, and ligaments) around the metacarpal neck and converts a simple dislocation into a complex, irreducible one by drawing the volar plate deeper into the joint space.
The Correct Closed Reduction Maneuver:
1. Wrist Flexion: Flex the wrist to relax the flexor tendons.
2. Hyperextension: Gently hyperextend the dislocated proximal phalanx to 90 degrees.
3. Distal Translation: Apply firm, distally directed pressure to the dorsal base of the proximal phalanx, sliding it distally along the dorsal surface of the metacarpal neck.
4. Flexion: Once the base of the phalanx clears the metacarpal head, acutely flex the MCP joint.
If this maneuver is successful, the joint will snap into place, and full, stable range of motion will be restored. If a single, well-executed attempt fails, the dislocation is deemed complex, and open reduction is indicated.
Operative Management: Open Reduction
When closed reduction fails, open reduction is required to extricate the incarcerated volar plate. Two primary surgical approaches are utilized: the Volar Approach and the Dorsal Approach.
1. The Volar Approach (Kaplan's Approach)
The volar approach provides direct visualization of the constricting pathoanatomy but carries a significant risk of iatrogenic neurovascular injury.
- Incision: A Brunner zigzag or an oblique incision is made over the volar aspect of the affected MCP joint, incorporating the palmar skin dimple.
- Neurovascular Identification:
> Surgical Warning: In an index finger MCP dislocation, the radial digital nerve is severely displaced and tented directly over the prominent metacarpal head, lying immediately beneath the skin. It is highly vulnerable to transection during the initial incision. The nerve must be identified and protected immediately. - Release of the Noose: The A1 pulley is identified. The superficial transverse metacarpal ligament is divided longitudinally. This releases the volar constriction.
- Reduction: The flexor tendons are retracted ulnarly, and the lumbrical is retracted radially. A blunt probe or Freer elevator is used to tease the incarcerated volar plate out from the joint space. Once the volar plate is freed, the joint is easily reduced by flexing the proximal phalanx.
- Closure: The skin is closed; the ligaments and volar plate generally do not require direct repair as they fall back into their anatomical positions.
2. The Dorsal Approach (Belsky's Approach)
Many contemporary hand surgeons prefer the dorsal approach due to its safety profile and excellent visualization of the volar plate.
- Incision: A longitudinal or slightly curved dorsal incision is made over the MCP joint.
- Extensor Mechanism: The extensor tendon is split longitudinally in the midline, or the sagittal band is incised to retract the extensor tendon laterally.
- Joint Arthrotomy: The dorsal capsule is incised, revealing the articular surface of the proximal phalanx and the incarcerated volar plate covering the metacarpal head.
- Volar Plate Release: A longitudinal incision is made directly through the center of the incarcerated volar plate. This splits the plate into two halves, instantly releasing the tension and allowing the two halves to slip volarly around the metacarpal head.
- Reduction: The joint is reduced with gentle flexion. The extensor mechanism is repaired with non-absorbable sutures.
Postoperative Protocol for MCP Dislocations
Following successful open or closed reduction, the joint is typically stable.
* Immobilization: A dorsal blocking splint is applied with the wrist in 30 degrees of extension and the MCP joints in 60 to 70 degrees of flexion. The interphalangeal joints are left free.
* Rehabilitation: Active range of motion within the constraints of the splint is initiated within 3 to 5 days to prevent stiffness. The splint is discontinued at 3 to 4 weeks, followed by buddy taping for an additional 2 to 3 weeks during athletic activities.
RADIAL COLLATERAL LIGAMENT (RCL) INJURIES
Biomechanics and Clinical Significance
While ulnar collateral ligament (UCL) injuries of the thumb (Skier's thumb) are widely recognized, radial collateral ligament (RCL) injuries of the thumb and finger MCP joints occur less frequently but are equally debilitating if mismanaged.
The RCL is the primary restraint to ulnar deviation of the digit. Biomechanically, the RCL is subjected to immense stress during "push-off" activities (e.g., pushing up from a chair) and during forceful pinch grips. Chronic insufficiency of the RCL leads to volar and ulnar subluxation of the proximal phalanx, resulting in a painful, unstable pinch and premature degenerative joint disease.
Pathoanatomy and Diagnosis
The mechanism of injury is typically a forced ulnar deviation of the digit with the MCP joint in flexion.
Clinical Pearl: Unlike the UCL of the thumb, where the adductor aponeurosis can interpose between the torn ligament and its insertion (the classic Stener lesion), no comparable anatomical structure exists on the radial side of the MCP joint. Therefore, a "Stener-equivalent" lesion does not occur in RCL injuries. This anatomical reality means that if proper protection is provided, adequate healing of an undisplaced RCL tear is highly probable.
Clinical Evaluation:
* Palpation: Tenderness and swelling are localized to the radial aspect of the MCP joint.
* Stress Testing: The MCP joint must be tested in 30 degrees of flexion to isolate the proper collateral ligament. Asymmetric joint opening of more than 15 to 20 degrees compared to the contralateral uninjured digit, or a lack of a firm endpoint, indicates a complete tear.
* Imaging: Radiographs should be obtained to rule out avulsion fractures. Stress radiographs can objectively quantify the degree of instability. MRI or high-resolution ultrasound can confirm the location and extent of the ligamentous disruption.
Non-Operative Management
Because there is no Stener lesion to prevent ligamentous apposition, non-operative management is highly successful for specific injury patterns.
* Indications: Incomplete tears (Grade I and II) and complete tears (Grade III) that are not associated with volar or rotational subluxation.
* Protocol: The affected digit is immobilized in a short-arm cast or a rigid thermoplastic splint. For the thumb, a thumb spica cast is used. The MCP joint is immobilized in slight flexion for 4 to 6 weeks. Following immobilization, progressive range of motion and strengthening are initiated.
Operative Management of Acute Complete Tears
Surgical intervention in the acute setting is reserved for severe injuries where conservative management is likely to fail.
* Indications: Complete tears demonstrating gross rotational instability, volar subluxation of the proximal phalanx, or failure to maintain reduction in a cast.
* Surgical Technique:
1. A lazy-S or mid-axial incision is made over the radial aspect of the MCP joint.
2. The sagittal band is incised, and the extensor mechanism is retracted to expose the joint capsule and the torn RCL.
3. The tear is most commonly an avulsion from the metacarpal origin.
4. The bony footprint is debrided to bleeding cancellous bone.
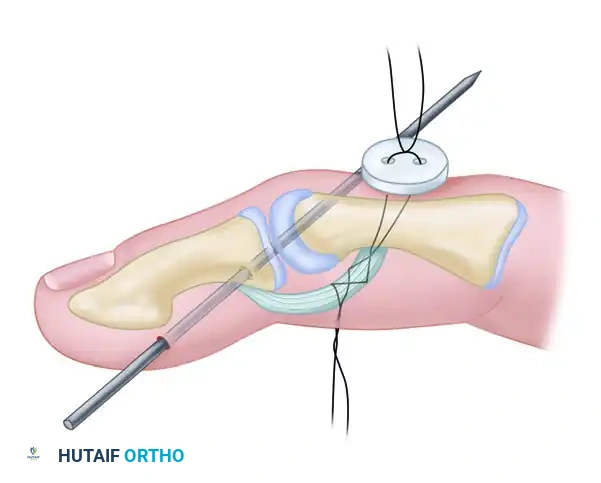
5. Direct repair is achieved using a micro-suture anchor (e.g., 1.3mm or 1.5mm) loaded with non-absorbable braided suture. The ligament is advanced and secured to its anatomical footprint.
6. The capsule and sagittal band are meticulously repaired.
Surgical Reconstruction for Chronic Instability
Improper initial treatment or missed diagnoses of RCL injuries inevitably lead to chronic, painful instability. In these scenarios, the native ligament is often attenuated, scarred, or completely resorbed, rendering direct repair impossible.
Surgical reconstruction is required to restore joint kinematics. Several techniques are utilized depending on the quality of the remaining tissue and the specific digit involved:
1. Radial Collateral Ligament Reefing
If the native ligament is intact but attenuated and lax, a reefing (imbrication) procedure can be performed. The ligament is incised, overlapped (pants-over-vest closure), and sutured with non-absorbable sutures to restore appropriate tension.
2. Tendon Graft Reconstruction (Palmaris Longus)
For severe chronic instability with deficient local tissue, an autologous tendon graft is the gold standard.
* Graft Harvest: The palmaris longus tendon is harvested.
* Bone Tunnels: Drill holes are created at the anatomical origins and insertions of the RCL on the metacarpal head and the base of the proximal phalanx.
* Graft Routing: The graft is passed through the bone tunnels in a figure-of-eight or box configuration to recreate both the proper and accessory collateral ligaments.
* Fixation: The graft is tensioned with the joint in 30 degrees of flexion and secured using interference screws or tying the graft over a bony bridge.
3. Advancement of the Abductor Pollicis Brevis (Thumb Specific)
For chronic RCL instability specifically involving the thumb MCP joint, dynamic stabilization can be achieved by advancing the insertion of the abductor pollicis brevis (APB).
* The tendinous insertion of the APB is identified, detached from its distal insertion, advanced dorsally and distally, and sutured tightly to the radial base of the proximal phalanx and the extensor mechanism. This provides a dynamic radial restraint to counteract ulnar deviating forces.
Postoperative Rehabilitation for RCL Procedures
Whether an acute repair or a chronic reconstruction is performed, the postoperative protocol is designed to protect the healing tissue while preventing joint contracture.
* Phase I (0-4 weeks): The joint is strictly immobilized in a cast or rigid splint.
* Phase II (4-6 weeks): The rigid splint is transitioned to a removable orthosis. Active range of motion exercises are initiated. Passive stretching and lateral stress are strictly avoided.
* Phase III (6-10 weeks): Progressive strengthening is introduced. Buddy taping (for fingers) or a soft functional brace (for the thumb) is utilized during activities.
* Phase IV (10-12+ weeks): Return to unrestricted heavy labor and sports, provided that pinch strength is restored and the joint is clinically stable.
CONCLUSION
Metacarpophalangeal joint dislocations and radial collateral ligament injuries require a high index of suspicion, a thorough understanding of hand pathoanatomy, and precise surgical execution. Recognizing the "noose" mechanism in complex MCP dislocations dictates the necessity of open reduction, with the dorsal approach offering a safe and effective means of extricating the volar plate. Similarly, while many RCL injuries heal with conservative management due to the absence of a Stener lesion, recognizing the indications for acute repair or chronic reconstruction is vital to preserving the critical push-off and pinch kinematics of the hand. Mastery of these principles ensures optimal functional outcomes and prevents the debilitating sequelae of chronic joint instability.
You Might Also Like