Operative Management of Boutonnière Deformity: Soft Tissue Reconstruction to Salvage Arthroplasty
Key Takeaway
The surgical correction of boutonnière deformity requires meticulous restoration of the extensor mechanism. For moderate deformities, treatment focuses on central slip reconstruction and lateral band mobilization to restore proximal interphalangeal (PIP) joint extension. Severe, fixed deformities often necessitate PIP joint arthrodesis or resection arthroplasty. This guide details the biomechanical principles, step-by-step surgical techniques, and postoperative rehabilitation protocols essential for optimizing functional outcomes in complex digital deformities.
INTRODUCTION AND PATHOANATOMY
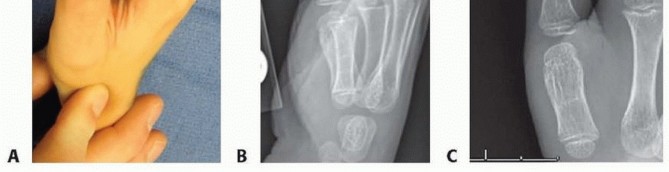
The boutonnière (buttonhole) deformity represents one of the most challenging biomechanical disruptions in hand surgery. Characterized by flexion of the proximal interphalangeal (PIP) joint and hyperextension of the distal interphalangeal (DIP) joint, the deformity arises from a primary disruption or attenuation of the central slip of the extensor mechanism at its insertion on the base of the middle phalanx.
As the central slip fails, the head of the proximal phalanx herniates dorsally through the defect in the extensor hood—the metaphorical "buttonhole." Subsequently, the triangular ligament attenuates, allowing the lateral bands to subluxate volarly to the axis of rotation of the PIP joint. Once volarly displaced, the lateral bands transition from being PIP joint extensors to PIP joint flexors. The transverse retinacular ligaments contract, tethering the lateral bands in this abnormal volar position, while the concentrated extensor pull is transmitted entirely to the terminal tendon, resulting in the characteristic DIP joint hyperextension.
Clinical Pearl: The key to successful surgical correction lies in understanding that the boutonnière deformity is a progressive, multi-structural failure. Surgical intervention must address not only the central slip defect but also the contracted transverse retinacular ligaments and the volarly displaced lateral bands.
PREOPERATIVE EVALUATION AND STAGING
Surgical decision-making is dictated by the flexibility of the PIP and DIP joints, the integrity of the articular cartilage, and the chronicity of the deformity.
- Mild Deformity: Passively correctable PIP flexion contracture (usually <30 degrees) with mild DIP hyperextension. Often amenable to conservative management via dynamic splinting (e.g., Capener splint).
- Moderate Deformity: Fixed or partially fixed PIP flexion contracture (30 to 60 degrees) with preserved articular cartilage. Requires soft tissue reconstruction, central slip shortening, and lateral band mobilization.
- Severe Deformity: Fixed PIP flexion contracture (>60 degrees) with joint destruction, severe arthrosis, or volar plate contracture. Necessitates salvage procedures such as PIP joint arthrodesis or resection arthroplasty.
CORRECTION OF MODERATE BUTTONHOLE DEFORMITY
When conservative measures fail or the deformity presents at a moderate, partially fixed stage with preserved joint surfaces, a comprehensive soft tissue reconstruction is indicated. The primary goals are to restore the central slip tension, relocate the lateral bands dorsal to the PIP joint axis of rotation, and release the hyperextension contracture at the DIP joint.
Patient Positioning and Anesthesia
- Anesthesia: Regional block (axillary or supraclavicular brachial plexus block) or wide-awake local anesthesia no tourniquet (WALANT). WALANT is highly advantageous as it allows for intraoperative active movement to assess tendon balance.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A pneumatic arm tourniquet is applied and inflated to 250 mm Hg (if WALANT is not utilized).
Surgical Approach and Exposure
- Make a generous, curved, dorsal longitudinal incision over the PIP joint.
- Extend the incision distally to the level of the DIP joint to ensure adequate exposure of the entire distal extensor mechanism.
- Elevate full-thickness skin flaps, preserving the dorsal sensory nerve branches and the delicate venous drainage network to prevent postoperative skin necrosis.
Surgical Warning: Avoid straight dorsal longitudinal incisions directly over the PIP joint, as these are prone to hypertrophic scarring and secondary flexion contractures. A curvilinear or lazy-S incision provides superior exposure and mitigates scar contracture.
Step-by-Step Soft Tissue Reconstruction
1. Mobilization of the Lateral Bands
* Identify the volarly subluxated lateral bands.
* Incise the transverse retinacular ligament longitudinally on both the radial and ulnar aspects.
* Carefully dissect underneath the displaced lateral slips to free them from the underlying capsule and collateral ligaments. This release is critical to allow the lateral bands to be transposed dorsally.
2. Synovectomy
* Perform a thorough PIP joint synovectomy after mobilizing the lateral bands.
* In rheumatoid patients or those with post-traumatic synovitis, hypertrophic synovium stretches the extensor mechanism and contributes to the deformity. Excision of this tissue decompresses the joint and facilitates reduction.
3. Terminal Slip Tenotomy (Fowler Release)
* Address the DIP joint hyperextension by performing a tenotomy of the terminal slips of the two lateral tendons.
* Execute this tenotomy just proximal to the DIP joint.
* This release eliminates the deforming hyperextension force at the DIP joint and allows the lateral bands to shift proximally and dorsally, aiding in PIP joint extension.
4. Central Tendon Shortening and Repair
* Assess the central tendon. In moderate deformities, it is typically attenuated, stretched, or scarred into a lengthened state.
* Perform a tenotomy of the central slip if it is severely scarred, or isolate the stretched segment.
* Shorten the central tendon by overlapping and suturing it (plication) using non-absorbable 4-0 or 3-0 braided sutures.
* Crucial Step: When shortening the central slip, take extreme care not to over-tighten it. Over-plication will create an iatrogenic PIP joint extension contracture, which is often more functionally debilitating than the original boutonnière deformity.
5. Realignment of the Lateral Bands
* Bring the mobilized lateral bands dorsally.
* Align and suture the lateral bands to the central slip at the base of the middle phalanx.
* Reconstruct the triangular ligament using 4-0 absorbable sutures to prevent recurrent volar subluxation of the lateral bands.
Intraoperative Assessment and Fixation
Surgical Pitfall: Tendon balance is the most critical and unforgiving aspect of this operation. Failure to verify passive flexion intraoperatively will inevitably lead to a stiff, non-functional digit.
- Passive Range of Motion Check: Before final fixation, passively flex the PIP joint. You must be certain that 80 degrees of PIP joint passive flexion is achievable. If the joint cannot flex to 80 degrees, the central slip repair is too tight and must be revised immediately to prevent a permanent extension contracture.
- Kirschner Wire Fixation: Once tendon balance is confirmed, reduce the PIP joint to full extension (0 degrees).
- Pass a small-caliber (0.045-inch or 0.035-inch) transfixing Kirschner wire (K-wire) obliquely across the PIP joint to hold it rigidly in extension. This protects the delicate central slip repair and lateral band realignment during the initial healing phase.
CORRECTION OF SEVERE BUTTONHOLE DEFORMITY
In severe, chronic boutonnière deformities, the PIP joint often develops a fixed, unyielding flexion contracture accompanied by severe articular cartilage destruction, volar plate scarring, and collateral ligament contracture. In these scenarios, soft tissue reconstruction is doomed to fail. Salvage procedures—namely PIP joint arthrodesis or resection arthroplasty—are indicated.
Proximal Interphalangeal Joint Arthrodesis
Arthrodesis provides a stable, painless, and durable digit, albeit at the cost of PIP joint motion. It is the gold standard for severe deformities in the index and middle fingers, where lateral pinch stability is paramount.
Surgical Technique:
* Approach: Utilize a dorsal approach, excising the scarred extensor mechanism over the PIP joint.
* Joint Preparation: Resect the articular surfaces of the proximal phalanx head and the middle phalanx base. Create flat, congruent cancellous bone surfaces.
* Positioning: The angle of fusion depends on the digit involved to optimize the cascade of the hand:
* Index finger: 25 to 30 degrees of flexion.
* Middle finger: 30 to 35 degrees of flexion.
* Ring finger: 35 to 40 degrees of flexion.
* Small finger: 40 to 45 degrees of flexion.
* Fixation: Utilize crossed K-wires, intraosseous wiring, or a dorsal tension band construct.
* DIP Joint Release: Because the lateral bands are chronically contracted, fusing the PIP joint will exacerbate DIP hyperextension. Therefore, release the DIP joint by performing an oblique tenotomy of the lateral tendons just proximal to the DIP joint. This allows the DIP joint to drop into a neutral, functional position.
Interphalangeal Joint Arthroplasty
Resection arthroplasty utilizing a silicone implant (e.g., Swanson implant) is a viable option for severe deformities, provided the flexion contracture is not so extreme that it requires excessive bone shortening to accommodate the implant.
Indications and Patient Selection:
* Arthroplasty is generally reserved for older, lower-demand patients, particularly those with rheumatoid arthritis.
* Prerequisite: The patient must have near-normal, reasonably well-preserved metacarpophalangeal (MCP) joints. If the MCP joints are destroyed, PIP arthroplasty will fail due to poor proximal biomechanical support.
* Digit Selection: Many surgeons consider the central two digits (middle and ring fingers) more suitable for PIP arthroplasty. These digits benefit from the lateral stability provided by the adjacent border digits (index and small fingers) during grasp and pinch activities.
Surgical Technique (Swanson Implant):
* Resection: Perform a generous resection of the proximal phalanx head. Minimal resection of the middle phalanx base is performed to preserve the collateral ligament insertions.
* Canal Preparation: Broach the medullary canals of the proximal and middle phalanges to accommodate the stems of the silicone spacer.
* Implant Insertion: Insert the Swanson silicone implant using a no-touch technique to minimize infection risk.
* Extensor Reconstruction: The central slip must be reattached to the base of the middle phalanx (often via drill holes) to provide active extension over the new implant.
Clinical Pearl: If the preoperative PIP flexion contracture exceeds 60 degrees, extensive bone resection is required to fit the implant without buckling. Excessive bone resection compromises collateral ligament origins, leading to catastrophic lateral instability of the arthroplasty. In such cases, arthrodesis is strongly preferred.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of boutonnière deformity correction relies as much on meticulous postoperative hand therapy as it does on surgical execution.
Protocol for Soft Tissue Reconstruction (Moderate Deformity)
- Weeks 0 to 3-4: The PIP joint remains immobilized in full extension via the transarticular K-wire. The DIP joint is left free. The patient is encouraged to perform active DIP joint flexion exercises immediately. This active DIP flexion pulls the lateral bands distally, preventing them from scarring to the dorsal PIP capsule.
- Weeks 3 to 4: The transarticular K-wire is removed in the clinic.
- Splinting: The joint is immediately placed in a dynamic extension splint (e.g., Capener or reverse knuckle bender splint) if indicated by a slight extensor lag.
- Motion: Active PIP joint motion is initiated promptly. The goal is to maintain active joint flexion while protecting the extensor repair. Passive PIP flexion is strictly avoided for the first 6 weeks to prevent stretching the central slip repair.
- Weeks 6 to 8: Wean from the extension splint during the day. Continue night splinting if an extensor lag persists. Begin gentle strengthening.
Protocol for Arthrodesis and Arthroplasty (Severe Deformity)
- Arthrodesis: The digit is immobilized in a protective splint for 6 to 8 weeks until radiographic evidence of bony union is observed. DIP joint motion is encouraged.
- Arthroplasty: A dynamic extension splint is applied within the first week. Controlled active range of motion is initiated early to promote the formation of a functional pseudocapsule around the silicone implant. Lateral stress is avoided for 6 weeks to prevent implant subluxation.
COMPLICATIONS AND MANAGEMENT
- Extension Contracture: The most common complication following soft tissue reconstruction, resulting from over-plication of the central slip or failure to achieve 80 degrees of intraoperative passive flexion. Management requires aggressive hand therapy; surgical tenolysis is rarely successful and often leads to recurrent boutonnière deformity.
- Recurrent Deformity: Caused by failure of the central slip repair, inadequate release of the transverse retinacular ligaments, or premature removal of the K-wire. May require revision surgery or salvage arthrodesis.
- Infection: Particularly devastating in the presence of a silicone implant or K-wires. Requires immediate hardware removal, aggressive debridement, and intravenous antibiotics.
- Skin Necrosis: Dorsal PIP skin is thin and poorly vascularized. Excessive undermining or straight incisions can lead to wound breakdown, exposing the tendon repair. Meticulous soft tissue handling is mandatory.
You Might Also Like