Centralization and Tendon Transfer Techniques for Radial Clubhand
Key Takeaway
Centralization with flexor carpi ulnaris (FCU) transfer is a cornerstone surgical intervention for radial clubhand (radial longitudinal deficiency). This procedure realigns the carpus over the distal ulna, utilizing precise soft tissue releases, K-wire fixation, and dynamic tendon transfers to restore wrist biomechanics. Achieving perfect carpal reduction and balancing deforming forces are critical to preventing recurrence and optimizing long-term upper extremity function in pediatric patients.
Introduction to Radial Longitudinal Deficiency
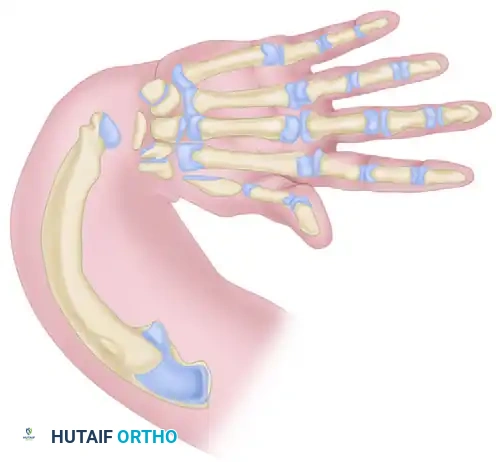
Radial longitudinal deficiency (RLD), commonly referred to as radial clubhand, represents a complex spectrum of congenital upper extremity anomalies characterized by hypoplasia or aplasia of the radius and its associated preaxial soft tissue structures. The absence of radial skeletal support, combined with the unopposed pull of the radial-sided musculature, results in a severe radial deviation and volar subluxation of the carpus.
The primary surgical goals in the management of RLD are to correct the severe radial deviation, balance the deforming muscular forces, stabilize the wrist, and maximize the functional length of the upper extremity while preserving the growth potential of the distal ulnar physis. The Bayne and Klug Centralization combined with the transfer of the flexor carpi ulnaris (FCU) remains a foundational operative strategy. By repositioning the carpus centrally over the distal ulna and dynamically balancing the wrist through tendon transfers, surgeons can significantly improve both the cosmetic appearance and the biomechanical function of the limb.
Clinical Pearl: Centralization is strictly contraindicated in patients with a stiff elbow in extension. In such cases, the severe radial deviation of the wrist is the only mechanism allowing the patient's hand to reach their mouth for feeding and facial hygiene. Correcting the wrist deformity in the presence of a stiff elbow will result in a catastrophic loss of independence.
Biomechanics and Pathoanatomy
Understanding the pathoanatomy of RLD is critical for successful surgical reconstruction. The deformity is not merely a skeletal absence; it is a profound soft-tissue imbalance.
* Skeletal Deficit: The distal radius is absent, removing the primary platform for carpal articulation. The ulna is typically thickened, shortened (approximately 60% of normal length at birth), and bowed with a concavity directed radially and volarly.
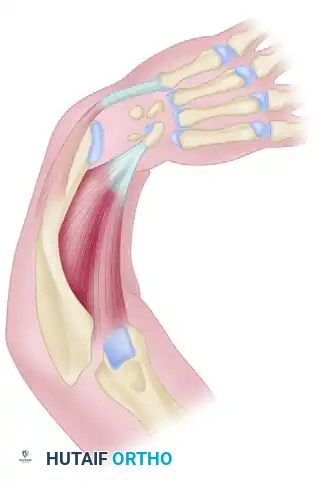
* Muscular Tethering: The flexor carpi radialis (FCR), brachioradialis, and tight radial capsular structures act as a dense, fibrotic tether, pulling the unsupported carpus into severe radial deviation.
* Neurovascular Anomalies: The radial artery and radial nerve are frequently absent or severely hypoplastic. The hand is typically perfused by the ulnar artery and a persistent median artery. Crucially, the median nerve often exhibits an anomalous superficial branch that runs directly in the radial fold, making it highly susceptible to iatrogenic injury during radial releases.
Preoperative Planning and Preparation
Surgical intervention is typically performed when the child is between 6 and 12 months of age. This timing allows the child to be large enough to tolerate the procedure and the anatomical structures to be of sufficient size for meticulous dissection, while intervening before the deforming forces cause irreversible adaptive changes to the carpus and distal ulna.
Prior to surgery, a rigorous regimen of serial casting or splinting is mandatory to stretch the tight radial soft tissues. If the radial contracture cannot be passively corrected to a neutral position preoperatively, preliminary soft-tissue distraction using a uniplanar or multiplanar external fixator may be required to avoid excessive tension on the neurovascular structures during acute centralization.
Surgical Technique: Bayne and Klug Centralization
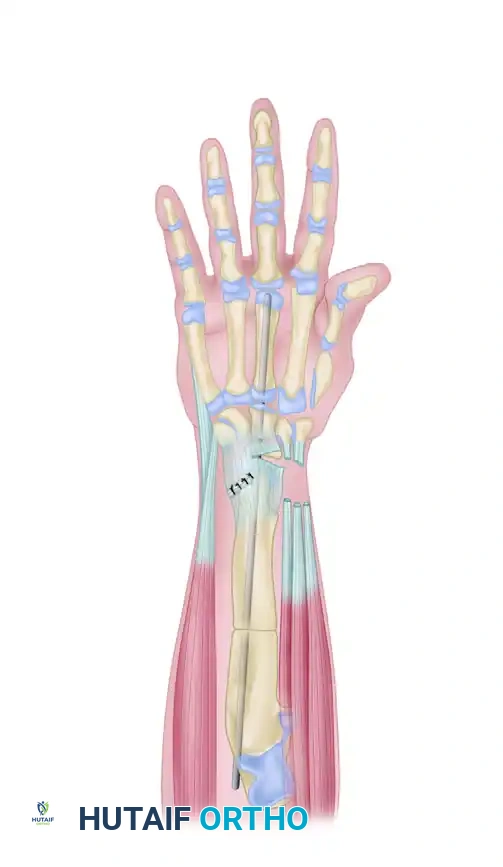
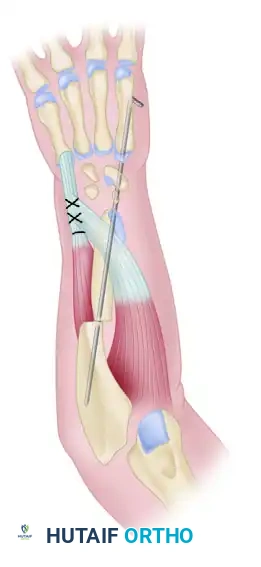
The Bayne and Klug technique involves a comprehensive soft-tissue release, reduction of the carpus onto the distal ulna, skeletal stabilization with a Kirschner wire (K-wire), and dynamic rebalancing via tendon transfers.
Incision and Soft Tissue Dissection
- Ulnar Incision: Make a transverse wedge incision over the distal end of the ulna to excise the redundant skin and fibrofatty tissue that accumulates on the convex ulnar side of the deformity.
- Radial Z-Plasty: A Z-plasty incision is frequently necessary on the radial surface of the distal forearm and wrist. This serves a dual purpose: it provides extra length to the contracted skin on the radial side and allows direct access to the tight wrist flexors and capsular attachments. Note: If preoperative serial casting or distraction has fully corrected the radial contracture, the Z-plasty may be omitted.
- Nerve Identification: Through the ulnar incision, meticulously identify and protect the dorsal sensory branch of the ulnar nerve. Locate the extensor carpi ulnaris (ECU) and the flexor carpi ulnaris (FCU) tendons, which will be utilized later for dynamic balancing.
- Anomalous Median Nerve: Elevate the radial skin flaps with extreme caution. Identify and protect the anomalous superficial branch of the median nerve, which frequently lies directly beneath the dermis in the radial fold.
Ulnar Preparation and Carpal Reduction
- Distal Ulna Exposure: Expose the distal ulna, taking absolute care to avoid any damage to the epiphyseal blood supply or the perichondrial ring. Iatrogenic injury to the distal ulnar physis will arrest longitudinal growth, severely exacerbating the limb length discrepancy.
- Ulnocarpal Flap: Develop a distally based ulnocarpal flap. Locate the interval between the carpus and the radial aspect of the ulna.
- Capsular Release: Using sharp dissection, free the capsular attachments to the carpal structures. Flex the elbow to relax the neurovascular bundle, and attempt to reduce the carpus directly over the end of the ulna. If reduction is impeded, utilize the radial incision to perform further releases.
- Release of Tethering Muscles: The flexor carpi radialis (FCR) and the brachioradialis are frequently attached directly to the radial carpal bones, producing a massive tethering force. Release these tendinous insertions completely to mobilize the carpus.
- Articular Preparation: If reduction remains difficult despite aggressive soft-tissue release, lightly shave the cartilage of the distal ulna to flatten its surface, creating a more stable platform for the carpus.
Surgical Warning: Do not expose the epiphyseal bone of the distal ulna. Bayne and Klug strongly advise against carpal bone excision (carpectomy) or excessive shaving of the ulnar cartilage, as this frequently leads to spontaneous intercarpal fusion, premature physeal arrest, and a rigidly stiff wrist. If reduction cannot be obtained, an ulnar shortening osteotomy is the preferred alternative.
Skeletal Fixation
- Pilot Channel: Select a K-wire slightly smaller than the one intended for final fixation. Use it to drill a pilot channel from distal to proximal directly through the center of the distal ulnar epiphysis and into the medullary canal.
- Carpal and Metacarpal Pinning: Introduce the larger, definitive K-wire distally into the carpal bones (typically through the capitate) and advance it down the shaft of the third metacarpal, crossing the metacarpophalangeal (MCP) joint.
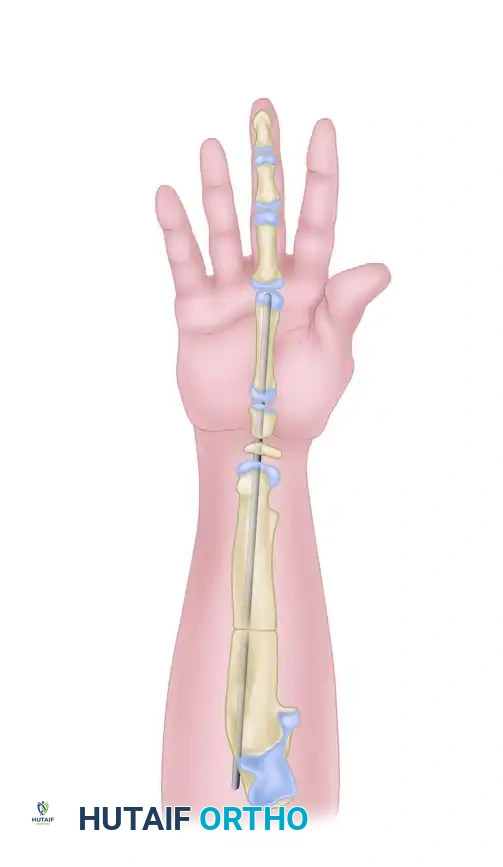
- Retrograde Ulnar Fixation: Place the proximal end of the K-wire into the previously drilled pilot hole in the central portion of the distal ulna. Drive the wire retrograde proximally through the ulnar shaft to secure the centralization.
- MCP Joint Clearance: Withdraw the pin slightly distally so that the tip clears the third MCP joint, ensuring it does not block digital motion during the postoperative period.
- Radiographic Confirmation: Obtain intraoperative fluoroscopic radiographs to ensure the carpus is perfectly centralized on the distal ulna.
Pitfall: Failure to achieve perfect, dead-center reduction of the carpus on the distal ulna is the most common technical cause of subsequent loss of centralization and recurrent radial deviation. Accept nothing less than perfect alignment.
Tendon Transfers and Soft Tissue Balancing
Once skeletal fixation is secure, the soft tissues must be dynamically balanced to prevent recurrence.
- Flap Advancement: Advance the distally based ulnocarpal flap proximally and suture it securely in place to reinforce the ulnar capsule.
- ECU Advancement: Isolate the extensor carpi ulnaris (ECU) tendon and advance its insertion as far distally as possible onto the base of the fifth metacarpal to maximize its mechanical advantage as an ulnar deviator.
- FCU Transfer: Suture the flexor carpi ulnaris (FCU) tendon directly into the ECU tendon as far distally and dorsally as possible. This transfer redirects the volar-ulnar force of the FCU into a dorsal-ulnar vector, counteracting the palmar and radial deforming structures and dynamically balancing the hand on the end of the ulna.
Surgical Technique 79-7: Sublimis Tendon Transfer Augmentation
In cases of severe imbalance, additional dynamic support can be achieved by transferring the flexor digitorum superficialis (sublimis) tendons to the dorsum of the hand.
- Tendon Harvest: Divide the sublimis tendon of the middle finger at the level of the middle phalanx, carefully dividing the chiasm of the decussating fibers. Perform an identical harvest on the ring finger sublimis tendon.
- Volar Routing: Make a short transverse incision on the volar aspect of the forearm and pull the two harvested tendons proximally into the wound.
- Subcutaneous Transfer: Reenter the wrist at the site of the previous dorsal incision. Route the sublimis tendons subcutaneously around the ulnar border of the ulna to the dorsum of the hand.
- Metacarpal Looping: Loop the tendon from the long finger around the shaft of the index finger metacarpal. Loop the tendon from the ring finger around the shaft of the long finger metacarpal.
- Tensioning and Suture: Transpose the tendons extraperiosteally. Suture them back onto themselves with the wrist held in 15 degrees of dorsiflexion and maximal ulnar deviation.
- Hypothenar Advancement: Transfer the origin of the hypothenar muscles proximally along the ulnar shaft to further enhance the ulnar-deviating vector.
Surgical Technique 79-8: Buck-Gramcko Radialization
As an alternative to true centralization, Buck-Gramcko introduced the concept of "radialization." Rather than placing the carpus directly over the ulna, radialization involves overcorrecting the deformity by placing the distal ulna under the radial carpal bones (the scaphoid or trapezium equivalent). This creates a mechanical block to radial deviation.
- Incision: Utilize an S-shaped incision over the dorsal-ulnar aspect of the wrist to provide wide exposure.
- Skeletal Alignment: Mobilize the carpus and translate it ulnarward until the radial-most carpal bones rest directly on the distal ulna.
- Pin Fixation: Secure the overcorrected position with a robust K-wire driven retrograde through the radial carpus and down the ulnar shaft.
- Tendon Transfers: The key to radialization is the aggressive transfer of the radial wrist extensors (ECR) and flexors (FCR) to the ulnar side of the hand (typically the ECU insertion) to convert all radial-deviating forces into ulnar-deviating forces.
Addressing Ulnar Bowing: The Closing Wedge Osteotomy
The ulna in RLD is invariably bowed, with the concavity facing radially. Mild bowing may remodel after centralization, but severe bowing mechanically disadvantages the tendon transfers and predisposes the wrist to recurrent radial deviation.
- Indication: If the ulna is severely bowed (angulation greater than 30 degrees), a concurrent ulnar osteotomy is mandatory.
- Technique: Perform a closing wedge osteotomy at the apex of the ulnar angulation. The K-wire used for centralization is driven proximally across the osteotomy site to provide intramedullary fixation.
Closure and Postoperative Care
Immediate Postoperative Management
- Closure: Deflate the tourniquet prior to final closure to ensure meticulous hemostasis and to evaluate the vascularity of the hand, particularly the radial digits, which may be compromised by the acute correction of the deformity.
- Immobilization: Close the incisions without tension. Place the hand in a neutral position and apply a bulky, non-compressive dressing followed by a long-arm plaster splint or cast.
Rehabilitation Protocol
The postoperative rehabilitation timeline is extensive and requires strict adherence to prevent recurrence.
* 0 to 2 Weeks: The initial dressing is left intact. At 2 weeks, the dressing is changed, sutures are removed, and a definitive long-arm plaster cast is applied. Mobilization of the fingers is strongly encouraged to prevent tendon adhesions.
* 6 to 8 Weeks: The long-arm cast and the intramedullary K-wire are removed in the clinic or under brief sedation.
* 8 Weeks to 6 Years of Age: A custom-molded short-arm Orthoplast splint is fabricated. The splint must hold the wrist in neutral to slight ulnar deviation. The fingers and elbow are left free to encourage functional use. This splint is worn full-time (23 hours a day) until the child reaches 6 years of age.
* 6 Years to Skeletal Maturity: After age 6, the splinting regimen is transitioned to nighttime use only. Night splinting must be maintained rigorously until the child reaches complete skeletal maturity, as the risk of recurrent radial deviation persists throughout the entire growth period.
Clinical Pearl: Careful, long-term follow-up is paramount. Recurrence of the radial deviation deformity is the most common complication of centralization. It is usually insidious and results from a combination of inadequate initial soft-tissue release, failure to achieve perfect skeletal centralization, loss of dynamic tendon balance, or poor compliance with the postoperative splinting regimen. Early detection of recurrence may allow for soft-tissue revision before skeletal changes become fixed.
You Might Also Like
