

Orthopedic MCQS online Anatomy 017
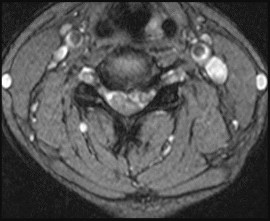
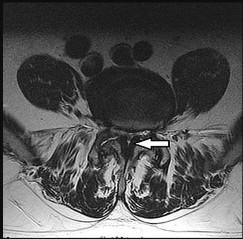
Figures 1a and 1b are the MR images of a 69-year-old woman with bilateral leg pain that is worse with ambulation. She feels better when she is sitting down or leaning on a grocery cart. Which condition or structure is indicated by the arrows?

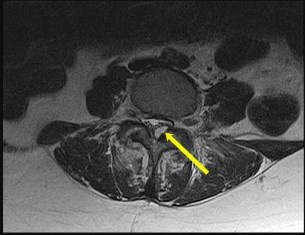
A disk herniation is not bright on T2. An arachnoid cyst is a sac filled with cerebrospinal fluid. Spinal arachnoid cysts are relatively uncommon, and typically are intradural, but they also can be extradural. Epidural lipomatosis is a condition caused by excessive accumulation of fat within the epidural space. It is not well circumscribed as seen with this lesion.
RECOMMENDED READINGS
1. [Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012;3(Suppl 3):S157-66. doi: 10.4103/2152-7806.98576. Epub 2012 Jul 17. PubMed PMID: 22905322. ](http://www.ncbi.nlm.nih.gov/pubmed/22905322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22905322)
2. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20173680)
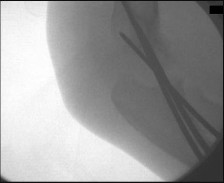
Figures 2a and 2b are the clinical photographs taken at the time of cubital tunnel surgery. The ulnar nerve is indicated by the red arrow. What is the name of the structure at the tip of the blue arrow?


RECOMMENDED READINGS
3. [Masear VR, Meyer RD, Pichora DR. Surgical anatomy of the medial antebrachial cutaneous nerve. J Hand Surg Am. 1989 Mar;14(2 Pt 1):267-71. PubMed PMID: 2703673. ](http://www.ncbi.nlm.nih.gov/pubmed/2703673)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2703673)
4. [Masear VR, Hill JJ Jr, Cohen SM. Ulnar compression neuropathy secondary to the anconeus epitrochlearis muscle. J Hand Surg Am. 1988 Sep;13(5):720-4. PubMed PMID: 3241044. ](http://www.ncbi.nlm.nih.gov/pubmed/3241044)[View](http://www.ncbi.nlm.nih.gov/pubmed/3241044)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3241044)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3241044)
Which nerve is at greatest risk in the setting of an anterior shoulder dislocation?



RECOMMENDED READINGS
5. [de Laat EA, Visser CP, Coene LN, Pahlplatz PV, Tavy DL. Nerve lesions in primary shoulder dislocations and humeral neck fractures. A prospective clinical and EMG study. J Bone Joint Surg Br. 1994 May;76(3):381-3. PubMed PMID: 8175837. ](http://www.ncbi.nlm.nih.gov/pubmed/8175837)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8175837)
6. [Lynch JR, Clinton JM, Dewing CB, Warme WJ, Matsen FA 3rd. Treatment of osseous defects associated with anterior shoulder instability. J Shoulder Elbow Surg. 2009 Mar-Apr;18(2):317-28. doi: 10.1016/j.jse.2008.10.013. Review. PubMed PMID: 19218054. ](http://www.ncbi.nlm.nih.gov/pubmed/19218054)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19218054)
7. [Pavlov H, Warren RF, Weiss CB Jr, Dines DM. The roentgenographic evaluation of anterior shoulder instability. Clin Orthop Relat Res. 1985 Apr;(194):153-8. PubMed PMID: 3978907. ](http://www.ncbi.nlm.nih.gov/pubmed/3978907)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/3978907)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3978907)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3978907)
CLINICAL SITUATION FOR QUESTIONS 4 THROUGH 7
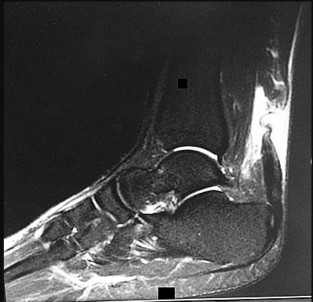
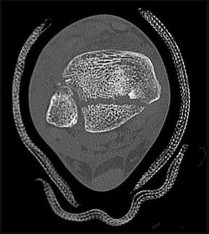
An 18-year-old woman was skateboarding when she fell and sustained the injury seen in Figures 4a through 4c.
What is the most serious outcome associated with this injury?
Risk for osteonecrosis associated with this injury is most related to
Which surgical approach will provide the most exposure and pose the lowest risk?
If all levels of injury severity are taken into account, what is the likelihood of osteonecrosis among all patients with this injury?
infrequency. However, the largest study on these injuries revealed that time from injury to surgery had little bearing on risk for complications. The energy imparted at the time of injury (comminution and open fracture) was much more relevant. The safest approach to this injury that provides the widest exposure is a 2-incision lateral and medial approach with a medial malleolar osteotomy, if needed. Some of the blood supply to the talus proceeds through the deltoid ligament, so it is not to be violated. A 2015 meta-analysis noted that the rate of osteonecrosis, if all injury severities were taken into account, was 31%. That same meta-analysis noted a mean rate of subtalar arthritis of 49%. This rate increased to 81% in studies with more than 2 years of follow-up.
RECOMMENDED READINGS
8. [Dodd A, Lefaivre KA. Outcomes of Talar Neck Fractures: A Systematic Review and Meta-analysis. J Orthop Trauma. 2015 May;29(5):210-5. doi: 10.1097/BOT.0000000000000297. Review. PubMed PMID: 25635362.](http://www.ncbi.nlm.nih.gov/pubmed/25635362)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25635362)
9. [Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004 Aug;86-A(8):1616-24. ](http://www.ncbi.nlm.nih.gov/pubmed/15292407)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15292407)
10. [Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004 Oct;86-A(10):2229-34. PubMed PMID: 15466732. ](http://www.ncbi.nlm.nih.gov/pubmed/15466732)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15466732)
11. [Ohl X, Harisboure A, Hemery X, Dehoux E. Long-term follow-up after surgical treatment of talar fractures: Twenty cases with an average follow-up of 7.5 years. Int Orthop. 2011 Jan;35(1):93-9. doi: 10.1007/s00264-009-0930-y. Epub 2009 Dec 22. ](http://www.ncbi.nlm.nih.gov/pubmed/20033158)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20033158)
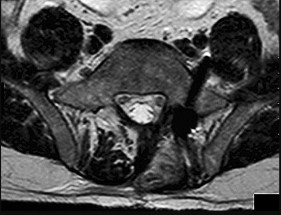
Figure 8 is the axial MR image through C5-6 of a 55-year-old right-handed man who is experiencing excruciating neck pain and left arm weakness. What is the most likely finding upon examination?
RECOMMENDED READINGS
12. Rhee JM, Yoon T, Riew KD. Cervical radiculopathy. J Am Acad Orthop Surg. 2007 Aug;15(8):486-
[94/. Review. PubMed PMID: 17664368. ](http://www.ncbi.nlm.nih.gov/pubmed/17664368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17664368)
13. [Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. Instr Course Lect. 2008;57:447-69. Review. PubMed PMID: 18399602. ](http://www.ncbi.nlm.nih.gov/pubmed/18399602)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18399602)
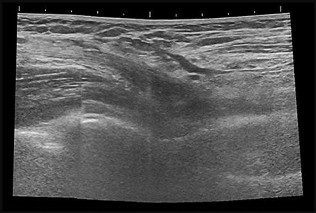
An examination of a newborn infant reveals a positive Ortolani test result on the right side and a negative result on the left. What is the preferred hip imaging method?
The imaging screening method of choice for newborns with suspected developmental hip dysplasia is ultrasound. Plain radiographs are of limited use because the femoral head ossific nucleus cannot be visualized. Ultrasound is easily performed without sedation or accompanying radiation exposure and is relatively inexpensive. The alpha angle is typically measured during the ultrasound and is defined as the angle measured between a vertical line drawn along the edge of the acetabulum (Perkin line) and a second line drawn along the acetabular roof. The alpha angle should measure more than 60 degrees.
Initial treatment for newborns is accomplished with a Pavlik harness. Risk factors for developmental dysplasia are multifactorial and include a family history in either a parent or a sibling, a primiparous mother, a breech presentation of any kind at the time of birth regardless of delivery method, and female sex.
RECOMMENDED READINGS
14. Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. _Orthopaedic Knowledge Update: Pediatrics 4_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
15. [Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11730331)
16. [Weinstein SL, Mubarak SJ, Wenger DR. Fundamental concepts of developmental dysplasia of the hip. Instr Course Lect. 2014;63:299-305. PubMed PMID: 24720315. ](http://www.ncbi.nlm.nih.gov/pubmed/24720315)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24720315)
Figures 10a through 10c are the radiographs and MR image of a 65-year-old woman with rheumatoid arthritis who has posterior headaches, hand and gait clumsiness, and dizziness. What is the most likely diagnosis?



Basilar invagination symptoms can include posterior headaches, cervical myelopathy, dizziness, and sudden death from compression of the medulla oblongata. In this scenario, there is no subaxial or atlantoaxial subluxation or rheumatoid plaque.
RECOMMENDED READINGS
17. [Fujiwara K, Owaki H, Fujimoto M, Yonenobu K, Ochi T. A long-term follow-up study of cervical lesions in rheumatoid arthritis. J Spinal Disord. 2000 Dec;13(6):519-26. PubMed PMID: 11132984. ](http://www.ncbi.nlm.nih.gov/pubmed/11132984)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11132984)
18. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A longterm analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993 Sep;75(9):1282-
[97/. PubMed PMID: 8408150. ](http://www.ncbi.nlm.nih.gov/pubmed/8408150)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8408150)
19. [Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001 Feb;83-A(2):194-200. PubMed PMID: 11216680. ](http://www.ncbi.nlm.nih.gov/pubmed/11216680)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216680)
Which procedure(s) would most directly correct the principal deformity shown in Figure 11?

TAL addresses the equinus deformity that is ever present with acquired flatfoot deformity. A medializing calcaneal osteotomy addresses hindfoot valgus. To address PTT dysfunction, the degenerative PTT is debrided and the FDL is often transferred into its position. A first tarsometatarsal fusion helps to stabilize the medial column. None of these procedures would correct the forefoot abduction seen in the above radiograph.
RECOMMENDED READINGS
20. [Chan JY, Greenfield ST, Soukup DS, Do HT, Deland JT, Ellis SJ. Contribution of Lateral Column Lengthening to Correction of Forefoot Abduction in Stage IIb Adult Acquired Flatfoot Deformity Reconstruction. Foot Ankle Int. 2015 Dec;36(12):1400-11. doi: 10.1177/1071100715596607. Epub 2015 Jul 27. PubMed PMID: 26216884. ](http://www.ncbi.nlm.nih.gov/pubmed/26216884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26216884)
21. [Deland JT. Adult-acquired flatfoot deformity. J Am Acad Orthop Surg. 2008 Jul;16(7):399-406. Review. PubMed PMID: 18611997. ](http://www.ncbi.nlm.nih.gov/pubmed/18611997)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18611997)
22. [Williams BR, Ellis SJ, Deyer TW, Pavlov H, Deland JT. Reconstruction of the spring ligament using a peroneus longus autograft tendon transfer. Foot Ankle Int. 2010 Jul;31(7):567-77. doi: 10.3113/FAI.2010.0567. PubMed PMID: 20663422. ](http://www.ncbi.nlm.nih.gov/pubmed/20663422)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20663422)
RESPONSES FOR QUESTIONS 12 THROUGH 15
1. T-type fracture
2. Anterior column fracture
3. Anterior wall fracture
4. Posterior wall fracture
5. Posterior column and posterior wall fracture
6. Transverse with posterior wall fracture
For each image set below, please select the correct diagnosis listed above
Figures 12a through 12c



Figures 13a through 13c



Figures 14a through 14c



Figures 15a through 15d


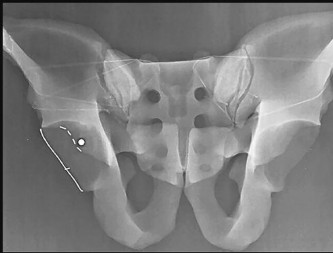
Judet and Letournel have a classification system for acetabular fractures. The system consists of 5 elementary fracture patterns: anterior wall, anterior column, posterior wall, and posterior column fractures of the acetabulum and a transverse pattern. There are also 5 associated fracture patterns: posterior column/posterior wall, transverse/posterior wall, T-type, anterior column with hemitransverse fracture of the posterior column, and both-column fractures.
Figure 12b shows a fracture of the posterior column on the Iliac oblique, and Figure 12c shows a fracture of the posterior wall in the obturator oblique.
In Question 13, the figures only reveal a fracture of the posterior wall, and this is best appreciated in Figure 13c, the obturator oblique view.
The T-type fracture is a transverse fracture with a secondary fracture line extending inferiorly. This causes the anterior and posterior columns to be separated. The iliac oblique view, Figure 14b, shows a fracture extending through the posterior column. In the obturator oblique view (Figure 14c), the yellow arrow shows a fracture extending through the anterior column, and the red arrow shows a fracture extending inferiorly through the ischium.
Fractures extending through the anterior and posterior columns are seen, which represent a transverse fracture, but there is no extension inferiorly, which eliminates T-type as a possible correct response. The anterior column fracture is best seen on the inlet view (Figure 15b), but it also can be seen in Figure 15d, the obturator oblique view. Figure 15c shows the fracture through the posterior column. For this patient, a small fracture of the posterior wall is visualized on the AP view (Figure 15a).
RECOMMENDED READINGS
1. Dickson KF, Dowling RM. Treatment of pelvic and acetabular fractures in elderly patients. Orthopaedic Knowledge Online Journal. Volume 11, Number 8 August 2013.
2. [Tornetta P 3rd. Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28. Review. PubMed PMID: 11174160. ](http://www.ncbi.nlm.nih.gov/pubmed/11174160)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/11174160)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11174160)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11174160)
3. [Moed BR, Kregor PJ, Reilly MC, Stover MD, Vrahas MS. Current management of posterior wall fractures of the acetabulum. Instr Course Lect. 2015;64:139-59. Review. PubMed PMID: 25745901. ](http://www.ncbi.nlm.nih.gov/pubmed/25745901)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25745901)
During the deep dissection for a direct anterior hip arthroplasty, a vascular bundle is encountered in the interval between the rectus femoris muscle and the gluteus medius muscle. Which artery is contained in this vascular bundle?
RECOMMENDED READINGS
4. McGann MA. Surgical approaches. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:683-733.
5. Baumgaertner MR, Higgins TF. Femoral neck fractures. In: Heckman JD, Kasser JR, Bucholz RW, Beaty JH, eds. _Rockwood and Green’s Fractures in Adults_. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:1579-1634.
If growth arrest is suspected after the fracture shown in the radiographs in Figures 17a through 17c, what is the most appropriate imaging modality to verify the presence of a physeal bar?



A physeal bar is difficult to rule in or out on radiographs because of natural undulations in the physis or a residual angular deformity after fracture that causes the physis to be less clearly visible. Often, the best clue that indicates physeal arrest after distal radius fracture is clinical prominence of the ulna head or increasing ulna-positive variance. The posteroanterior view of the wrist should be taken with the shoulder abducted to 90 degrees and elbow flexed to 90 degrees. This places the forearm in neutral rotation, and changes in ulnar variance can more accurately be detected. Comparison views of the other side may be warranted.
If a growth arrest is suspected, CT scan and MRI are both effective modalities for imaging the size and location of the bar. The bar is most easily detected on the T1-weighted MR images. Early, unossified cartilaginous bars also may be detected on some MRI sequences. MRI with 3D mapping functions is now used to map the size and location into an easy-to-visualize format, but the computer programs are not yet mainstream. A CT scan can demonstrate the bar but is not as acceptable because of the high dose of radiation (compared to MRI).
The physis has 3 main zones. The zone that is most important and susceptible to injury is the resting zone, where pluripotent chondrocytes reside. This layer is immediately adjacent to the epiphysis. If this layer is disrupted or ischemic, there is permanent growth arrest of that physis section. The central layer is the proliferative zone. The hypertrophic zone is the layer adjacent to the metaphysis and is subdivided into 3 layers: maturation, degeneration, and provisional calcification. The weakest link is the junction between the provisional calcification layer and the metaphysis. Most physeal fractures occur through this layer. Thus, growth arrest after fracture is rare because the level of injury typically is as far as possible from the delicate resting zone.
If growth arrest occurs after distal radius fracture, surgical intervention is tailored to the situation. If the child is young, an attempt at bar resection and interposition of fat or bone wax is appropriate. If a teenage child is asymptomatic and ulna variance is a few millimeters positive, simple ulna epiphysiodesis is appropriate. If there is deformity of the distal radius, corrective osteotomy may be best.
RECOMMENDED READINGS
6. [Abzug JM, Little K, Kozin SH. Physeal arrest of the distal radius. J Am Acad Orthop Surg. 2014 Jun;22(6):381-9. doi: 10.5435/JAAOS-22-06-381. Review. PubMed PMID: 24860134. ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24860134)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24860134)
7. [Craig JG, Cramer KE, Cody DD, Hearshen DO, Ceulemans RY, van Holsbeeck MT, Eyler WR. Premature partial closure and other deformities of the growth plate: MR imaging and three-dimensional modeling. Radiology. 1999 Mar;210(3):835-43. PubMed PMID: 10207489. ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/10207489)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10207489)
8. [Ecklund K, Jaramillo D. Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol. 2002 Apr;178(4):967-72. PubMed PMID: 11906884. ](http://www.ncbi.nlm.nih.gov/pubmed/11906884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11906884)
Where are the origin and insertion of the knee posterior cruciate ligament (PCL)?
RECOMMENDED READINGS
9. [Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178. ](http://www.ncbi.nlm.nih.gov/pubmed/16228178)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16228178)
10. [Moorman CT 3rd, Murphy Zane MS, Bansai S, Cina SJ, Wickiewicz TL, Warren RF, Kaseta MK. Tibial insertion of the posterior cruciate ligament: a sagittal plane analysis using gross, histologic, and radiographic methods. Arthroscopy. 2008 Mar;24(3):269-75. doi: 10.1016/j.arthro.2007.08.032. Epub 2007 Nov 5. PubMed PMID: 18308177. ](http://www.ncbi.nlm.nih.gov/pubmed/18308177)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18308177)
During an anterior approach to correct thoracolumbar scoliosis, there is a sudden decrease in somatosensory-evoked potential (SSEP) and motor-evoked potential (MEP) signals. Correction maneuvers have not been attempted when signals go down. All neuromonitoring and anesthesia concerns have been addressed, and the measured abnormalities persist. What is the likely reason behind the neuromonitoring abnormalities?
The artery of Adamkiewicz originates in more than 90% of patients between T8 and L1. It has been postulated that the artery of Adamkiewicz is the primary blood supply to the thoracic spinal cord. Standard anterior retroperitoneal- and thoracotomy-based approaches typically necessitate sacrifice of segmental vessels that can disrupt blood supply to the anterior thoracic cord.
It is unlikely at this point in the surgery that neurapraxia caused this change because no correction maneuvers have been attempted and no instrumentation has been placed; however, these interventions can indeed trigger neuromonitoring issues during a procedure.
RECOMMENDED READINGS
11. [Fanous AA, Lipinski LJ, Krishna C, Roger EP, Siddiqui AH, Levy EI, Leonardo J, Pollina J. The Impact of Preoperative Angiographic Identification of the Artery of Adamkiewicz on Surgical Decision Making in Patients Undergoing Thoracolumbar Corpectomy. Spine (Phila Pa 1976). 2015 Aug 1;40(15):1194-9. PubMed PMID: 25816140.](http://www.ncbi.nlm.nih.gov/pubmed/25816140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25816140)
12. [Gonzalez AA, Jeyanandarajan D, Hansen C, Zada G, Hsieh PC. Intraoperative neurophysiological monitoring during spine surgery: a review. Neurosurg Focus. 2009 Oct;27(4):E6. doi: 10.3171/2009.8.FOCUS09150. Review. PubMed PMID: 19795955. ](http://www.ncbi.nlm.nih.gov/pubmed/19795955)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19795955)
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figure 20 is the MR image of a 27-year-old man who was playing basketball when he sustained the injury shown.
Treatment for this injury can be surgical or nonsurgical. Which outcome is more likely with surgical treatment?
Which 2 things generally need to be present for this injury to occur?
Which aspect of rehabilitation from this injury is necessary, regardless of how it is treated?
How long does it generally take for patients to return to preinjury levels of activity after sustaining this injury?
RECOMMENDED READINGS
13. [Vosseller JT, Ellis SJ, Levine DS, Kennedy JG, Elliott AJ, Deland JT, Roberts MM, O'Malley MJ. Achilles tendon rupture in women. Foot Ankle Int. 2013 Jan;34(1):49-53. doi: 10.1177/1071100712460223. PubMed PMID: 23386761. ](http://www.ncbi.nlm.nih.gov/pubmed/23386761)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386761)
14. [Tallon C, Maffulli N, Ewen SW. Ruptured Achilles tendons are significantly more degenerated than tendinopathic tendons. Med Sci Sports Exerc. 2001 Dec;33(12):1983-90. PubMed PMID: 11740288. ](http://www.ncbi.nlm.nih.gov/pubmed/11740288)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11740288)
15. [Willits K, Amendola A, Bryant D, Mohtadi NG, Giffin JR, Fowler P, Kean CO, Kirkley A. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am. 2010 Dec 1;92(17):2767-75. doi: 10.2106/JBJS.I.01401. Epub 2010 Oct 29. PubMed PMID: 21037028. ](http://www.ncbi.nlm.nih.gov/pubmed/21037028)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21037028)
What is the incidence of malignant transformation for the lesion shown in Figures 24a and 24b?







RECOMMENDED READINGS
16. [T Scharschmidt, J Mayerson. Chrondrosarcoma. Orthopaedic Knowledge Online Journal. November 2010. ](http://www.aaos.org/OKOJ/vol8/issue10/ONC021/)http://www.aaos.org/OKOJ/vol8/issue10/ONC021/ Accessed May 2, 2016.
17. [Marco RA, Gitelis S, Brebach GT, Healey JH. Cartilage tumors: evaluation and treatment. J Am Acad Orthop Surg. 2000 Sep-Oct;8(5):292-304. Review. PubMed PMID: 11029557. ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11029557)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11029557)
Figures 25a through 25d are the presurgical anteroposterior (AP), presurgical lateral, postsurgical AP, and postsurgical lateral radiographs of a 65-year-old woman who undergoes a multilevel lumbar laminectomy and fusion through a combined left lateral and posterior approach. After surgery, she awakens with excruciating left anterior thigh numbness and pain. Furthermore, she cannot bear weight on her left leg because her leg keeps buckling. What is the most likely cause of this neurological deficit?




any degree of lower extremity weakness was found in 34% of patients. Fortunately, only 5% of those patients sustained persistent weakness at 1 year.
Although neurapraxia can occur because of deformity correction, the problem likely is not attributable to isolated left leg quadriceps weakness. Patient positioning on the table also is an unlikely cause because no corrective maneuvers took place. Postsurgical radiographs show that screws are within the pedicles on the lateral views and are appropriately going from lateral to medial on the AP view, so hardware malpositioning is unlikely.
RECOMMENDED READINGS
18. Phillips FM, Isaacs RE, Rodgers WB, Khajavi K, Tohmeh AG, Deviren V, Peterson MD, Hyde J, Kurd
[M. Adult degenerative scoliosis treated with XLIF: clinical and radiographical results of a prospective multicenter study with 24-month follow-up. Spine (Phila Pa 1976). 2013 Oct 1;38(21):1853-61. doi: 10.1097/BRS.0b013e3182a43f0b. PubMed PMID: 23873244.](http://www.ncbi.nlm.nih.gov/pubmed/23873244)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23873244)
19. Park DK, Lee MJ, Lin EL, Singh K, An HS, Phillips FM. The relationship of intrapsoas nerves during a transpsoas approach to the lumbar spine: anatomic study. J Spinal Disord Tech. 2010 Jun;23(4):223-
[8/. doi: 10.1097/BSD.0b013e3181a9d540. PubMed PMID: 20084033. ](http://www.ncbi.nlm.nih.gov/pubmed/20084033)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20084033)
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
A 13-year-old boy has left anterior knee pain that is localized to the tibial tubercle. The pain is worse with jumping and has been getting worse during his current basketball season. Ice provides temporary symptom relief. His knee never bothered him before, and his other knee does not hurt.
What is the most likely diagnosis?
Which pathology is associated with this condition?
The patient returns 4 years later; now he is a 17-year-old boy who has anterior knee pain with jumping and kneeling (Figure 28). The pain is located at the tibial tubercle. There is soft-tissue swelling and tenderness to palpation over the tubercle. He is able to do a straight-leg raise and there is no effusion, but the pain prevents him from playing basketball. Initial treatment should include

The patient fails nonsurgical treatment for this condition. What is the best next step?
RECOMMENDED READINGS
1. [Vergara-Amador E, Davalos Herrera D, Moreno LÁ. Radiographic features of the development of the anterior tibial tuberosity. Radiologia. 2016 Feb 22. pii: S0033-8338(16)00019-9. doi: 10.1016/j.rx.2016.01.005. [Epub ahead of print] English, Spanish. PubMed PMID: 26917430. ](http://www.ncbi.nlm.nih.gov/pubmed/26917430)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26917430)
2. [Frank JB, Jarit GJ, Bravman JT, Rosen JE. Lower extremity injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2007 Jun;15(6):356-66. Review. PubMed PMID: 17548885. ](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17548885)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17548885)
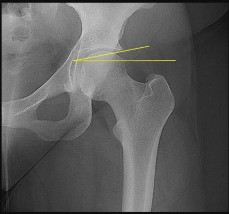
Which structure does the dashed line represent in Figure 30?
RECOMMENDED READINGS
3. Vrahas M, Tile M. Fractures of the acetabulum. In: Bucholz R, Heckman J. _Rockwood and Green’s Fractures in Adults_. 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002:1513-1545.
4. Armfield DR, Towers JD. Radiographic evaluation of the hip. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:349-391.
A surgeon is performing a revision total hip arthroplasty. Multiple screws are used to stabilize the acetabulum, including screws placed in the anterior superior and posterior superior quadrants. In the postanesthesia care unit, the patient develops a progressive decline in blood pressure. Intraoperative injury to which anatomical structure has most likely occurred?
The femoral artery is more anterior and distal and less likely to be damaged by screw placement. The superior and inferior gluteal arteries may be injured but are less likely to be affected by screw placement anteriorly and are more likely to be noted immediately.
RECOMMENDED READINGS
5. Wasielewski RC, Cooperstein LA, Kruger MP, Rubash HE. Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am. 1990 Apr;72(4):501-
[8/. PubMed PMID: 2324135. ](http://www.ncbi.nlm.nih.gov/pubmed/2324135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2324135)
6. [Wasielewski RC, Crossett LS, Rubash HE. Neural and vascular injury in total hip arthroplasty. Orthop Clin North Am. 1992 Apr;23(2):219-35. Review. PubMed PMID: 1315014. ](http://www.ncbi.nlm.nih.gov/pubmed/1315014)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/1315014)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1315014)
Figures 32a and 32b are the CT and MR image of a man who undergoes fusion for his degenerative spondylolisthesis. He wakes up with a foot drop. Which structure has most likely been injured?

The iliac vein and artery lie more ventral than the L5 nerve root, which is draped closely to the sacral ala. The S1 nerve root exits inferior to the S1 sacral ala and is seen medial to the S1 pedicle on the MR axial image provided. On the CT scan the pedicle screw is aiming medial to lateral and is penetrating several millimeters outside the bone. Although an injury to the peroneal division of the sciatic nerve could result in a foot drop, this is not the most likely cause in this scenario and it lies more peripherally.
RECOMMENDED READINGS
7. [Mirkovic S, Abitbol JJ, Steinman J, Edwards CC, Schaffler M, Massie J, Garfin SR. Anatomic consideration for sacral screw placement. Spine (Phila Pa 1976). 1991 Jun;16(6 Suppl):S289-94. PubMed PMID: 1862427. ](http://www.ncbi.nlm.nih.gov/pubmed/1862427)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1862427)
8. [Santos ER, Rosner MK, Perra JH, Polly DW Jr. Spinopelvic fixation in deformity: a review. Neurosurg Clin N Am. 2007 Apr;18(2):373-84. Review. PubMed PMID: 17556140. ](http://www.ncbi.nlm.nih.gov/pubmed/17556140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17556140)
Figures 33a through 33c are the radiographs of a total knee arthroplasty (TKA). What is the cause of the radiographic abnormality?



RECOMMENDED READINGS
9. [Malo M, Vince KG. The unstable patella after total knee arthroplasty: etiology, prevention, and management. J Am Acad Orthop Surg. 2003 Sep-Oct;11(5):364-71. Review. PubMed PMID: 14565758.](http://www.ncbi.nlm.nih.gov/pubmed/14565758)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14565758)
10. Rhoads DD, Noble PC, Reuben JD, Mahoney OM, Tullos HS. The effect of femoral component position on patellar tracking after total knee arthroplasty. Clin Orthop Relat Res. 1990 Nov;(260):43-
[51/. PubMed PMID: 2225641. ](http://www.ncbi.nlm.nih.gov/pubmed/2225641)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2225641)
Figures 34a through 34c are the radiographs and MR image of a 15-year-old, right-hand-dominant boy who was playing ice hockey and was checked into the boards. He had immediate anterior right shoulder pain and was unable to return to play. He was seen in the emergency department, and radiograph findings reportedly were normal. A sling is placed and he is seen in the office 3 days later. An examination reveals forward flexion of 90 degrees, abduction of 50 degrees, and external rotation of 0 degrees; all are painful. Belly-press test findings also are painful and abnormal. What is the most likely diagnosis?



RECOMMENDED READINGS
11. [Sugalski MT, Hyman JE, Ahmad CS. Avulsion fracture of the lesser tuberosity in an adolescent baseball pitcher: a case report. Am J Sports Med. 2004 Apr-May;32(3):793-6. PubMed PMID: 15090399. ](http://www.ncbi.nlm.nih.gov/pubmed/15090399)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15090399)
12. [Harper DK, Craig JG, van Holsbeeck MT. Apophyseal injuries of the lesser tuberosity in adolescents: a series of five cases. Emerg Radiol. 2013 Jan;20(1):33-7. doi: 10.1007/s10140-012-1064-x. Epub 2012 Aug 16. PubMed PMID: 22895662. ](http://www.ncbi.nlm.nih.gov/pubmed/22895662)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22895662)
RESPONSES FOR QUESTIONS 35 THROUGH 38
1. Open reduction and internal fixation (ORIF)
2. Walking boot and weight bearing as tolerated until pain subsides
3. Nonweight-bearing cast for 6 weeks
4. Physical therapy
5. Closed reduction and weight bearing as tolerated
6. Closed reduction and percutaneous fixation
A 23-year-old man sustains an inversion ankle injury. For each figure(s) shown below, select the most appropriate treatment listed above.
Figure 35

Figure 36

Figure 37

Figures 38a and 38b


RECOMMENDED READINGS
1. [View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23959223)
2. [Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. ](http://www.ncbi.nlm.nih.gov/pubmed/22465516)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22465516)
3. [Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22956165)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22956165)
4. [Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. ](http://www.ncbi.nlm.nih.gov/pubmed/16330511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16330511)
What is the most likely cause of the deformity shown in Figures 39a through 39c?



Clinically, the finger has a short distal phalangeal segment with a dorsally curved fingernail. Patients tend to seek an evaluation for this progressive deformity during adolescence. The deformity ceases to increase once a patient reaches skeletal maturity and the physis closes. This condition is frequently diagnosed as a partial growth arrest, but there is always a mysterious lack of a trauma history. Infection and inflammation are other possible causes, but laboratory studies and MRI do not show enhancement.
This deformity is largely cosmetic, although pain is occasionally reported. If patients find the deformity unacceptable, treatment is a palmarly based opening-wedge osteotomy. While this is an exceedingly rare condition, it is relevant for general orthopaedic surgeons to recognize the condition to avoid the consternation associated with misdiagnosis.
Vitamin D deficiency does not cause skeletal deformity in the hand. Frostbite typically is associated with wide, short phalanges with early growth arrest. Posttraumatic growth arrest occurs occasionally with a Seymour fracture but is most often a central or asymmetric arrest.
RECOMMENDED READINGS
5. [Dykes RG. Kirner's deformity of the little finger. J Bone Joint Surg Br. 1978 Feb;60(1):58-60. PubMed PMID: 627580.](http://www.ncbi.nlm.nih.gov/pubmed/627580)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/627580)
6. Khalid S, Khalid M, Zaheer S, Ahmad I, Ullah E. Kirner's Deformity Misdiagnosed as Fracture: A Case Report. Oman Med J. 2012 May;27(3):237-8. doi: 10.5001/omj.2012.53. PubMed PMID: 22811775.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22811775)
7. Lee J, Ahn JK, Choi SH, Koh EM, Cha HS. MRI findings in Kirner deformity: normal insertion of the flexor digitorum profundus tendon without soft-tissue enhancement. Pediatr Radiol. 2010 Sep;40(9):1572-5. doi: 10.1007/s00247-010-1628-4. Epub 2010 Mar 25. PubMed PMID: 20336287.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20336287)
While performing the modified Stoppa approach for fixation of an acetabular fracture, a vascular anastomosis, the “corona mortis,” will be encountered. Which 2 blood vessels contribute to this anastomosis?
RECOMMENDED READINGS
8. [Ponsen KJ, Joosse P, Schigt A, Goslings JC, Luitse JS. Internal fracture fixation using the Stoppa approach in pelvic ring and acetabular fractures: technical aspects and operative results. J Trauma. 2006 Sep;61(3):662-7. Erratum in: J Trauma. 2007 Jun;62(6):1490. Goslings, Carel J [corrected to Goslings, J Carel]. PubMed PMID: 16967004.](http://www.ncbi.nlm.nih.gov/pubmed/16967004)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16967004)
9. [Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. ](http://www.ncbi.nlm.nih.gov/pubmed/21368098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21368098)
RESPONSES FOR QUESTIONS 41 THROUGH 44
1. Tibial and/or fibular osteotomy with open reduction and internal fixation (ORIF)
2. Ankle distraction arthroplasty
3. Ankle fusion
4. Total ankle arthroplasty (TAA)
For each scenario described below, select the most appropriate treatment listed above.
A 27-year-old man who underwent ankle ORIF 5 years ago is experiencing continuous ankle pain that has worsened over time (Figures 41a and 41b).


A 71-year-old man with long-standing ankle arthrosis who has previously had a subtalar fusion (Figure 42).
A 52-year-old woman who is an avid hiker. Her ankle pain has begun to substantially limit her activity (Figure 43).

A 46-year-old woman had an ankle fracture and ORIF 6 years ago. She had subsequent removal of some of the hardware, but her pain has persisted (Figures 44a and 44b).


One of the strongest indications for ankle arthroplasty is a preexisting hindfoot fusion with a goal to retain some ankle/hindfoot motion. Ankle fusion is perhaps the most predictable surgical treatment for a relatively young, active patient with ankle arthritis. Moreover, there are concerns regarding implant loosening when performing TAA in active patients.
Outcome after syndesmosis ORIF has been linked to the quality of the reduction at the index procedure. Syndesmotic malreduction that is severe necessitates osteotomy and revision ORIF.
RECOMMENDED READINGS
1. [Sagi HC, Shah AR, Sanders RW. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J Orthop Trauma. 2012 Jul;26(7):439-43. doi: 10.1097/BOT.0b013e31822a526a. PubMed PMID: 22357084. ](http://www.ncbi.nlm.nih.gov/pubmed/22357084)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22357084)
2. [Smith NC, Beaman D, Rozbruch SR, Glazebrook MA. Evidence-based indications for distraction ankle arthroplasty. Foot Ankle Int. 2012 Aug;33(8):632-6. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/22995229)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22995229)
3. [Kim BS, Knupp M, Zwicky L, Lee JW, Hintermann B. Total ankle replacement in association with hindfoot fusion: Outcome and complications. J Bone Joint Surg Br. 2010 Nov;92(11):1540-7. doi: 10.1302/0301-620X.92B11.24452. PubMed PMID: 21037349. ](http://www.ncbi.nlm.nih.gov/pubmed/21037349)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21037349)
4. [Daniels TR, Younger AS, Penner M, Wing K, Dryden PJ, Wong H, Glazebrook M. Intermediate-term results of total ankle replacement and ankle arthrodesis: a COFAS multicenter study. J Bone Joint Surg Am. 2014 Jan 15;96(2):135-42. doi: 10.2106/JBJS.L.01597. ](http://www.ncbi.nlm.nih.gov/pubmed/24430413)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24430413)
Figures 45a through 45e are the radiographs and clinical photographs of a 10-year-old boy who sustained a direct blow to the elbow yesterday while playing football. He has focal tenderness over the lateral side of the elbow without significant swelling and 10 to 140 degrees of flexion with full pronosupination. What is the most likely explanation for the appearance on radiographs?





Reading pediatric elbow radiographs can be daunting because there are 6 different ossification centers about the elbow (4 in the distal humerus [capitellum and lateral epicondyle laterally and trochlea and medial epicondyle medially]) and in the radial head and olecranon. Girls tend to be about 2 years ahead of boys in terms of skeletal maturity.
The capitellum is the first to ossify and usually is visible by the first year. This ossification center helps to assess alignment with the shaft of the radius in Monteggia fractures and the anterior humeral line in supracondylar fractures. Fractures of the lateral condyle tend to be at least partially through the capitellar physis. Spontaneous osteonecrosis of the capitellar ossification center is called Panner disease.
The radial head typically begins to ossify at age 4 to 5. Although occurrence is rare, children without a visible radial head ossification center may sustain a fracture through the physis and the epiphysis may displace. The only radiographic signs may be large fat pad signs, but significant injury should be clearly seen during an examination.
The medial epicondyle appears at age 4 to 5. Fracture through the physis is fairly common after repetitive trauma (throwing) or elbow dislocation because of pull of the flexor-pronator mass. It may become entrapped in the joint after elbow dislocation. A high index of suspicion must be maintained for skeletally immature patients with elbow dislocation.
The trochlear ossification center in the distal humerus appears at age 8 to 9. The appearance is often perceived as abnormal after trauma because the trochlea begins to ossify in a fragmented manner.
The tip of the olecranon ossification center appears at age 8 to 9. Although the olecranon ossification center looks oblique like the tip of the olecranon, the first part to appear is in the most proximal part of the epiphysis, adjacent to the physis. It is rare to fracture through this physis or epiphysis.
The lateral epicondylar ossification center is the last to appear at around age 10. It is a small ossification center seen on the lateral margin of the distal humerus proximal to the capitellum. This vertically oriented and pointed center frequently is mistaken for an avulsion fracture. It is virtually impossible to avulse this fragment.
RECOMMENDED READINGS
5. [Skaggs DL. Elbow Fractures in Children: Diagnosis and Management. J Am Acad Orthop Surg. 1997 Nov;5(6):303-312. PubMed PMID: 10797226.](http://www.ncbi.nlm.nih.gov/pubmed/10797226)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10797226)
6. [Cheng JC, Wing-Man K, Shen WY, Yurianto H, Xia G, Lau JT, Cheung AY. A new look at the sequential development of elbow-ossification centers in children. J Pediatr Orthop. 1998 Mar-Apr;18(2):161-7. PubMed PMID: 9531396. ](http://www.ncbi.nlm.nih.gov/pubmed/9531396)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9531396)
Figure 46 is the CT scan of a 50-year-old man who is brought to the emergency department after a fall. He has a complete C5 neurological injury. What is the root cause of his fracture?
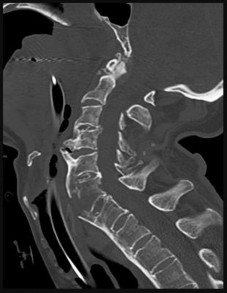
This patient also has degenerative changes found at C3-4, C4-5, but the ankylosing of the spine is the main reason for the higher fracture risk. DISH (Forestier disease) is a noninflammatory
spondyloarthropathy characterized by flowing ossifications and bone proliferations at sites of tendinous and ligamentous insertion.
RECOMMENDED READINGS
7. [El Tecle NE, Abode-Iyamah KO, Hitchon PW, Dahdaleh NS. Management of spinal fractures in patients with ankylosing spondylitis. Clin Neurol Neurosurg. 2015 Dec;139:177-82. doi: 10.1016/j.clineuro.2015.10.014. Epub 2015 Oct 23. Review. PubMed PMID: 26513429. ](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[ ](http://www.ncbi.nlm.nih.gov/pubmed/26513429)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26513429)
8. [Lukasiewicz AM, Bohl DD, Varthi AG, Basques BA, Webb ML, Samuel AM, Grauer JN. Spinal Fracture in Patients With Ankylosing Spondylitis: Cohort Definition, Distribution of Injuries, and Hospital Outcomes. Spine (Phila Pa 1976). 2016 Feb;41(3):191-6. doi: 10.1097/BRS.0000000000001190. PubMed PMID: 26579959. ](http://www.ncbi.nlm.nih.gov/pubmed/26579959)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26579959)
Figures 47a and 47b are the radiograph and ultrasound of a 62-year-old, right-hand-dominant manual laborer who has experienced 3 days of right elbow pain and antecubital swelling and ecchymosis. He was changing a truck tire when he felt a pop in his elbow. A hook test result is abnormal; he has pain with resisted supination and weakness with resisted elbow flexion. Which outcome can be expected if this patient chooses nonsurgical treatment?


RECOMMENDED READINGS
9. [Sutton KM, Dodds SD, Ahmad CS, Sethi PM. Surgical treatment of distal biceps rupture. J Am Acad Orthop Surg. 2010 Mar;18(3):139-48. Review. PubMed PMID: 20190104. ](http://www.ncbi.nlm.nih.gov/pubmed/20190104)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20190104)
10. [O'Driscoll SW, Goncalves LB, Dietz P. The hook test for distal biceps tendon avulsion. Am J Sports Med. 2007 Nov;35(11):1865-9. Epub 2007 Aug 8. PubMed PMID: 17687121. ](http://www.ncbi.nlm.nih.gov/pubmed/17687121)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17687121)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17687121)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17687121)
CLINICAL SITUATION FOR QUESTIONS 48 AND 49
Six hours ago, a 31-year-old healthy man sustained the injury shown in Figure 48. His skin is intact posteriorly.
**Question 48 of 100**
After splinting, what is the best next step?
1. Open reduction and internal fixation (ORIF)
2. Splinting in plantar flexion
3. Discharge home for outpatient follow-up
4. Admission to the hospital and pain control
_PREFERRED RESPONSE: 1- Open reduction and internal fixation (ORIF)_
Optimal biomechanical fixation for the injury should include
RECOMMENDED READINGS
11. Banerjee R, Chao JC, Taylor R, Siddiqui A. Management of calcaneal tuberosity fractures. J Am Acad Orthop Surg. 2012 Apr;20(4):253-8. doi: 10.5435/JAAOS-20-04-253. Review. PubMed PMID:
[22474095/. ](http://www.ncbi.nlm.nih.gov/pubmed/22474095)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22474095)
12. [Gitajn IL, Abousayed M, Toussaint RJ, Vrahas M, Kwon JY. Calcaneal avulsion fractures: a case series of 33 patients describing prognostic factors and outcomes. Foot Ankle Spec. 2015 Feb;8(1):10-7. doi: 10.1177/1938640014548323. Epub 2014 Sep 8. PubMed PMID: 25205682. ](http://www.ncbi.nlm.nih.gov/pubmed/25205682)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/25205682)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25205682)
13. [Attinger CE, Evans KK, Bulan E, Blume P, Cooper P. Angiosomes of the foot and ankle and clinical implications for limb salvage: reconstruction, incisions, and revascularization. Plast Reconstr Surg. 2006 Jun;117(7 Suppl):261S-293S. Review. PubMed PMID: 16799395.](http://www.ncbi.nlm.nih.gov/pubmed/16799395)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16799395)
Figure 50 is the radiograph of a 19-year-old woman who injured her left knee while playing soccer 4 days ago. She was cutting to her right, was tackled on the inside of her left knee, and felt a pop. She has no history of prior injury to her knee. Which structure attaches at the site of the avulsion fracture?








The iliotibial band inserts on Gerdy’s tubercle. A portion of the ALL may insert on the lateral meniscus; however, a lateral meniscus tear is not directly associated with avulsion fractures. The fibular collateral ligament inserts on the fibular head.
RECOMMENDED READINGS
14. Macchi V, Porzionato A, Morra A, Stecco C, Tortorella C, Menegolo M, Grignon B, De Caro R. The anterolateral ligament of the knee: a radiologic and histotopographic study. Surg Radiol Anat. 2015 Oct
[17/. [Epub ahead of print] PubMed PMID: 26476833.](http://www.ncbi.nlm.nih.gov/pubmed/26476833)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26476833)
15. Kennedy MI, Claes S, Fuso FA, Williams BT, Goldsmith MT, Turnbull TL, Wijdicks CA, LaPrade RF. The Anterolateral Ligament: An Anatomic, Radiographic, and Biomechanical Analysis. Am J Sports Med. 2015 Jul;43(7):1606-15. doi: 10.1177/0363546515578253. Epub 2015 Apr 17. PubMed
[PMID: 25888590. ](http://www.ncbi.nlm.nih.gov/pubmed/25888590)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25888590)
RESPONSES FOR QUESTIONS 51 THROUGH 57
Figure 51 a- h
a b c
h
d
e
f
g
Hip dysplasia is indicated if the measurement exceeds 10 degrees
Indicates the anterior center edge angle
Indicates the lateral center edge angle
The femoral head overlaps the ilioischial spine medially
The floor of the acetabular fossa touches the ilioischial line
Allows for visualization of the anterior column
Provides visualization of the ilioischial line
Coxa profunda is indicated when the medial line of the acetabulum is medial to the ilioischial line on a plain AP view of the hip. Protrusio acetabuli refers to the femoral head being medial to the ilioischial line.
The iliac oblique and obturator oblique (Judet) views are used along with the AP of the hip to evaluate patients who have sustained acetabular fractures. The iliac oblique view shows the anterior wall and the posterior column of the acetabulum (as seen by the ilioischial line), and the obturator oblique view shows the posterior wall and the anterior column (as seen by the iliopectineal line).
RECOMMENDED READINGS
1. [Bloomfield MR, Erickson JA, McCarthy JC, Mont MA, Mulkey P, Peters CL, Pivec R, Austin MS. Hip pain in the young, active patient: surgical strategies. Instr Course Lect. 2014;63:159-76. PubMed PMID: 24720303.](http://www.ncbi.nlm.nih.gov/pubmed/24720303)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24720303)
2. Sassoon A, Haidukewyech GJ. Hip and pelvic reconstruction and arthroplasty. In: Cannada LK, ed. _Orthopaedic Knowledge Update 11_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:489-507.
3. Nepple JJ, Prather H, Trousdale RT, Clohisy JC, Beaulé PE, Glyn-Jones S, Rakhra K, Kim YJ. Diagnostic imaging of femoroacetabular impingement. J Am Acad Orthop Surg. 2013;21 Suppl 1:S20-
[6/. doi: 10.5435/JAAOS-21-07-S20. PubMed PMID: 23818187.](http://www.ncbi.nlm.nih.gov/pubmed/23818187)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23818187)
4. [Tornetta P 3rd. Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28. Review. PubMed PMID: 11174160. ](http://www.ncbi.nlm.nih.gov/pubmed/11174160)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/11174160)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11174160)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11174160)
Figure 58 is the CT scan of a 50-year-old man who has fallen from a height of 12 feet. He has a reported incomplete spinal cord injury. He is intubated and sedated prior to an examination. What are the likely neurological examination findings?

RECOMMENDED READINGS
5. [Ko HY, Ditunno JF Jr, Graziani V, Little JW. The pattern of reflex recovery during spinal shock. Spinal Cord. 1999 Jun;37(6):402-9. PubMed PMID: 10432259.](http://www.ncbi.nlm.nih.gov/pubmed/10432259)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432259)
6. [Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, Jones L, Krassioukov A, Mulcahey MJ, Schmidt-Read M, Waring W. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011 Nov;34(6):535-46. doi: 10.1179/204577211X13207446293695. PubMed PMID: 22330108. ](http://www.ncbi.nlm.nih.gov/pubmed/22330108)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22330108)
7. American Spinal Injury Association Standards for neurological classification of spinal injured patients. Chicago, IL: ASIA; 1982.
Which structures are often encountered and may need to be mobilized in the surgical treatment of the injury shown in Figure 59?
The CT scan shows a large posterior malleolar fracture that necessitates open reduction and internal fixation. The best approach to this fragment is posterolateral to the ankle, which necessitates an incision over the posterolateral ankle roughly halfway between the fibula and the Achilles tendon. In that interval, the sural nerve runs with the lesser saphenous vein, both of which often need to be mobilized.
The greater saphenous vein and the saphenous nerve run along the medial aspect of the ankle. The superficial peroneal nerve is anterolateral at this level.
RECOMMENDED READINGS
8. [Jowett AJ, Sheikh FT, Carare RO, Goodwin MI. Location of the sural nerve during posterolateral approach to the ankle. Foot Ankle Int. 2010 Oct;31(10):880-3. doi: 10.3113/FAI.2010.0880. PubMed PMID: 20964966.](http://www.ncbi.nlm.nih.gov/pubmed/20964966)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20964966)
9. Franzone JM, Vosseller JT. Posterolateral approach for open reduction and internal fixation of a posterior malleolus fracture--hinging on an intact PITFL to disimpact the tibial plafond: a technical note. Foot Ankle Int. 2013 Aug;34(8):1177-81. doi: 10.1177/1071100713481455. Epub 2013 Mar 12.
[PubMed PMID: 23481092. ](http://www.ncbi.nlm.nih.gov/pubmed/23481092)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23481092)
The direct anterior approach is used to perform a total hip arthroplasty (THA). When the surgeon makes postsurgical rounds, it is noted that the patient cannot extend her knee flat into the bed. What is the most likely explanation for this finding?
This will result in abductor weakness. Obturator nerve injury is rare, and its clinical consequences are not usually noticed, nor are they usually clinically tested for. Injury to the femoral nerve is becoming more common with the increased use of the direct anterior approach.
RECOMMENDED READINGS
10. Hoppenfeld S, deBoer P. The hip. In: _Surgical Exposures in Orthopaedics: The Anatomic Approach_. Philadelphia, PA: JB Lippincott; 1984:301-356.
11. Hanssen AD. Anatomy and surgical approaches. In: Morrey BF, An KN, Cofield RH, Lewallen DG, Cooney WP III, Kitaoka HB, Pagnano MW, eds. _Joint Replacement Arthroplasty_. 3rd ed. Philadelphia, PA: Churchill-Livingstone; 2003:566-593.
**RESPONSES FOR QUESTIONS 61 THROUGH 66**
1. Osteonecrosis
2. Chondrosarcoma
3. Hip dysplasia
4. Transient osteoporosis of the hip
5. Femoral neck fracture
6. Labral tear
For each image below, identify the correct diagnosis from the list above.
Figure 61
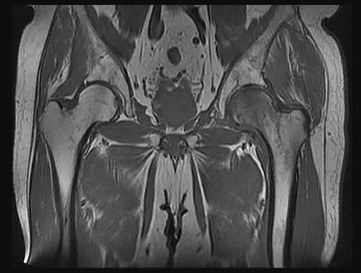
Figure 62
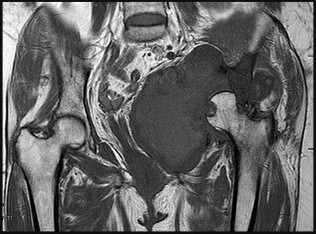
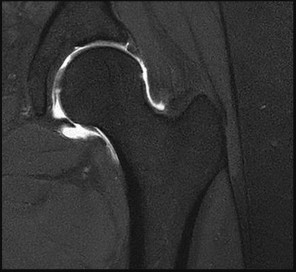
Figure 63
Figure 64

**Question 65 of 100**
1. Osteonecrosis
2. Chondrosarcoma
3. Hip dysplasia
4. Transient osteoporosis of the hip
5. Femoral neck fracture
6. Labral tear
Figure 65
_PREFERRED RESPONSE: 3- Hip dysplasia_
Figure 66
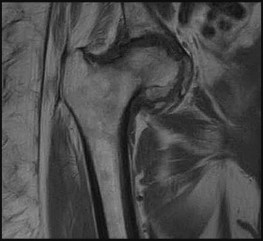
image would show high-intensity signal in a similar distribution. These changes signify an increase in bone marrow edema. On occasion, a subchondral insufficiency fracture is seen, but collapse of the femoral head should not occur with transient osteoporosis of the hip. It is seen most commonly in healthy middle-age men and in women during the third trimester of pregnancy. Hip pain is the most common symptom, and this typically lasts 6 to 8 months. Complete resolution of symptoms without long-term sequelae is the rule with few exceptions.
Figure 62 shows chondrosarcoma of the pelvis. This is a T1-weighted image that reveals a large soft-tissue mass of low-signal intensity, signifying destruction of the left acetabulum with medial protrusion of the left femoral head into the pelvis. These tumors occur typically in adults and are usually located in the proximal femur, ilium, or the periacetabular regions.
Figure 63 shows a superior acetabular labral tear. This is a T2-weighted image of the left hip after administration of intra-articular contrast. The distension of the joint with contrast shows the separation of the superior labrum from the bony acetabular rim.
Figure 64 shows end-stage osteonecrosis of the left femoral head. This is a T1-weighted image of the left hip with low-intensity signal, signifying bone marrow edema and femoral head collapse. There is a bandlike low signal intensity line that is characteristically seen on T1-weighted images. This represents the zone of demarcation between the viable and necrotic bone. The most common risk factors for osteonecrosis are heavy alcohol intake and chronic glucocorticoid use.
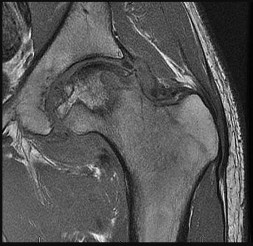
Figure 65 shows a T1-weighted image of a dysplastic right hip. A shallow acetabulum is present with approximately 40% uncoverage of the right femoral head. A shallow fovea on the femoral head and a hyperplastic superior labrum also are seen.
Figure 66 shows a T1-weighted image of a nondisplaced right femoral neck fracture. The fracture line is seen in the subcapital region of the femoral neck, and there is low-signal intensity signifying surrounding bone edema. Plain radiographs are negative in 8% of femoral neck fractures, and MRI has been shown to be 99% sensitive.
RECOMMENDED READINGS
1. [Korompilias AV, Karantanas AH, Lykissas MG, Beris AE. Transient osteoporosis. J Am Acad Orthop Surg. 2008 Aug;16(8):480-9. Review. PubMed PMID: 18664637. ](http://www.ncbi.nlm.nih.gov/pubmed/18664637)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18664637)
2. [Hartley KG, Damon BM, Patterson GT, Long JH, Holt GE. MRI techniques: a review and update for the orthopaedic surgeon. J Am Acad Orthop Surg. 2012 Dec;20(12):775-87. doi: 10.5435/JAAOS-20-12-775. Review. PubMed PMID: 23203937. ](http://www.ncbi.nlm.nih.gov/pubmed/23203937)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23203937)
3. Potter HG, Sou IT. Magnetic resonance imaging. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:409-422.
Figures 67a and 67b are the radiographs of a 58-year-old man who has a painful left shoulder. Three months ago he underwent an anatomic total shoulder arthroplasty (TSA) for glenohumeral osteoarthritis. He was doing some yardwork when he felt a pop in his shoulder. What is the most likely diagnosis?


RECOMMENDED READINGS
4. Aldinger PR, Raiss P, Rickert M, Loew M. Complications in shoulder arthroplasty: an analysis of 485 cases. Int Orthop. 2010 Apr;34(4):517-24. doi: 10.1007/s00264-009-0780-7. Epub 2009 Apr 28.
[PubMed PMID: 19396634.](http://www.ncbi.nlm.nih.gov/pubmed/19396634)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19396634)
5. [Miller BS, Joseph TA, Noonan TJ, Horan MP, Hawkins RJ. Rupture of the subscapularis tendon after shoulder arthroplasty: diagnosis, treatment, and outcome. J Shoulder Elbow Surg. 2005 Sep-Oct;14(5):492-6. PubMed PMID: 16194740. ](http://www.ncbi.nlm.nih.gov/pubmed/16194740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16194740)
Figure 68 is the MR image of an 85-year-old patient who cannot ambulate unless leaning over things. While sitting, the patient has minimal pain. Which structure is the arrow pointing to?



RECOMMENDED READINGS
6. Lurie JD, Tosteson TD, Tosteson A, Abdu WA, Zhao W, Morgan TS, Weinstein JN. Long-term outcomes of lumbar spinal stenosis: eight-year results of the Spine Patient Outcomes Research Trial (SPORT). Spine (Phila Pa 1976). 2015 Jan 15;40(2):63-76. doi: 10.1097/BRS.0000000000000731.
[PubMed PMID: 25569524.](http://www.ncbi.nlm.nih.gov/pubmed/25569524)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25569524)
7. [Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. doi: 10.2106/JBJS.H.00913. PubMed PMID: 19487505. ](http://www.ncbi.nlm.nih.gov/pubmed/19487505)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487505)
**Question 69 of 100**
For the injury shown in Figure 69, open reduction and internal fixation (ORIF) results in which outcome relative to primary arthrodesis (PA)?
1. Better radiographic outcome
2. Better physical function on SF-36
3. Higher rate of hardware removal
4. Higher patient satisfaction
_PREFERRED RESPONSE: 3- Higher rate of hardware removal_
**DISCUSSION**
In a prospective randomized study, Henning and associates showed that the only difference between PA and ORIF was in the rate of planned and unplanned secondary surgeries, which was much higher for patients who underwent ORIF, almost exclusively because a large percentage of those patients had their hardware removed. Ly and Coetzee had previously shown, also in a prospective randomized study, that patients had better functional outcomes with PA, although these procedures primarily were performed for ligamentous Lisfranc injuries, and that study used a nonvalidated outcome measure.
RECOMMENDED READINGS
8. [Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583.](http://www.ncbi.nlm.nih.gov/pubmed/19796583)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/19796583)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19796583)
9. [Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816.](http://www.ncbi.nlm.nih.gov/pubmed/16510816)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16510816)
CLINICAL SITUATION FOR QUESTIONS 70 THROUGH 73
Figures 70a through 70c are the radiographs of a 5-year-old boy who sustained a closed injury when he fell from a trampoline bed.
Where does the blood supply enter the fracture fragment?
What is the most likely complication after surgical treatment of this injury?
What is the average time to radiographic union of this fracture?
Surveillance for growth arrest resulting from this injury should continue for how long after injury?
The blood supply to the lateral condyle fragment enters posterolaterally. Disruption of the blood supply may lead to osteonecrosis of the capitellum, so great care should be taken during open approaches to the elbow in skeletally immature patients, especially during lateral condyle open reduction and internal fixation.
Treatment of lateral condyle fractures in skeletally immature patients may be fraught with danger. The most common complication is persistent stiffness.
Growth arrest is a surprisingly rare complication, considering the fracture usually involves the capitellar physis, and reduction of the physis is often radiographically imperfect even with open reduction. However, this may be an underrecognized complication because arrest of the capitellar physis may not be evident until 1 to 3 years postinjury—beyond the time at which some surgeons or patients believe follow-up is necessary. Growth arrest has been reported with smooth wire fixation and lag screw fixation. The average time to radiographic union of a lateral condyle fracture is 6 weeks.
RECOMMENDED READINGS
10. [Cardona JI, Riddle E, Kumar SJ. Displaced fractures of the lateral humeral condyle: criteria for implant removal. J Pediatr Orthop. 2002 Mar-Apr;22(2):194-7. PubMed PMID: 11856929. ](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11856929)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11856929)
11. [Stein BE, Ramji AF, Hassanzadeh H, Wohlgemut JM, Ain MC, Sponseller PD. Cannulated Lag Screw Fixation of Displaced Lateral Humeral Condyle Fractures Is Associated With Lower Rates of Open Reduction and Infection Than Pin Fixation. J Pediatr Orthop. 2015 Jul 17. [Epub ahead of print] PubMed PMID: 26192878. ](http://www.ncbi.nlm.nih.gov/pubmed/26192878)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26192878)
12. [Das De S, Bae DS, Waters PM. Displaced humeral lateral condyle fractures in children: should we bury the pins? J Pediatr Orthop. 2012 Sep;32(6):573-8. doi: 10.1097/BPO.0b013e318263a25f. PubMed PMID: 22892618. ](http://www.ncbi.nlm.nih.gov/pubmed/22892618)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22892618)
13. [Cates RA, Mehlman CT. Growth arrest of the capitellar physis after displaced lateral condyle fractures in children. J Pediatr Orthop. 2012 Dec;32(8):e57-62. doi: 10.1097/BPO.0b013e31826bb0d5. PubMed PMID: 23147632. ](http://www.ncbi.nlm.nih.gov/pubmed/23147632)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23147632)
Figures 74a and 74b are the MR images of a 36-year-old man with a 3-month history of excruciating left leg pain. Which finding upon examination would be most consistent with the MR images?


RECOMMENDED READINGS
14. [Rhee JM, Schaufele M, Abdu WA. Radiculopathy and the herniated lumbar disk: controversies regarding pathophysiology and management. Instr Course Lect.2007;56:287-99. Review. PubMed PMID: 17472314. ](http://www.ncbi.nlm.nih.gov/pubmed/17472314)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17472314)
15. Mixter WJ, Barr JS. Rupture of the intervertebral disk with involvement of the spinal canal. N Engl J Med. 1934: 211: 210-5.
During a transpsoas approach, which lumbar level is at highest risk for a neurological motor deficit?
RECOMMENDED READINGS
16. [Moro T, Kikuchi S, Konno S, Yaginuma H. An anatomic study of the lumbar plexus with respect to retroperitoneal endoscopic surgery. Spine (Phila Pa 1976). 2003 Mar 1;28(5):423-8; discussion 427-8. PubMed PMID: 12616150.](http://www.ncbi.nlm.nih.gov/pubmed/12616150)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12616150)
17. Park DK, Lee MJ, Lin EL, Singh K, An HS, Phillips FM. The relationship of intrapsoas nerves during a transpsoas approach to the lumbar spine: anatomic study. J Spinal Disord Tech. 2010 Jun;23(4):223-
[8/. doi: 10.1097/BSD.0b013e3181a9d540. PubMed PMID: 20084033. ](http://www.ncbi.nlm.nih.gov/pubmed/20084033)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20084033)
18. Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J Neurosurg Spine. 2009 Feb;10(2):139-
[44/. doi: 10.3171/2008.10.SPI08479. PubMed PMID: 19278328. ](http://www.ncbi.nlm.nih.gov/pubmed/19278328)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19278328)
In a neutrally aligned leg, which percentage of force is transmitted through the medial compartment during weight-bearing activities?
Anatomic and mechanical alignment of the leg are different. The anatomic axis has approximately 6 degrees of valgus, while mechanical alignment is typically neutral (range, 0-2 degrees of varus). It has been reported that in a neutrally aligned limb, 60% to 70% of the force across the knee is transmitted through the medial compartment.
RECOMMENDED READINGS
19. [Hunter DJ, Sharma L, Skaife T. Alignment and osteoarthritis of the knee. J Bone Joint Surg Am. 2009 Feb;91 Suppl 1:85-9. doi: 10.2106/JBJS.H.01409. PubMed PMID: 19182031. ](http://www.ncbi.nlm.nih.gov/pubmed/19182031)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/19182031)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19182031)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19182031)
20. [Andriacchi TP. Dynamics of knee malalignment. Orthop Clin North Am. 1994 Jul;25(3):395-403. Review. PubMed PMID: 8028883. ](http://www.ncbi.nlm.nih.gov/pubmed/8028883)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8028883)
21. [Cooke TD, Sled EA, Scudamore RA. Frontal plane knee alignment: a call for standardized measurement. J Rheumatol. 2007 Sep;34(9):1796-801. PubMed PMID: 17787049. ](http://www.ncbi.nlm.nih.gov/pubmed/17787049)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/17787049)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17787049)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17787049)
Figure 77 shows the CT scan of a 65-year-old Asian man who has been experiencing increasing difficulty using his hands. His handwriting has changed and he feels off balance. What is the most likely cause of his symptoms?

A herniated disk may be difficult to see on a CT scan and is not typically calcified This patient has degenerative spondylosis and likely some ligamentum hypertrophy, but the OPLL is fairly prominent and thick in the upper cervical spine. The ligamentum flavum is located dorsal to the dural sac, and the ossification is ventral to the dural sac.
RECOMMENDED READINGS
22. [An HS, Al-Shihabi L, Kurd M. Surgical treatment for ossification of the posterior longitudinal ligament in the cervical spine. J Am Acad Orthop Surg. 2014 Jul;22(7):420-9. doi: 10.5435/JAAOS-22-07-420. Review. PubMed PMID: 24966248.](http://www.ncbi.nlm.nih.gov/pubmed/24966248)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24966248)
23. [Mizuno J, Nakagawa H. Ossified posterior longitudinal ligament: management strategies and outcomes. Spine J. 2006 Nov-Dec;6(6 Suppl):282S-288S. Review. PubMed PMID: 17097548. ](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[View](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17097548)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17097548)
Figure 78 is the radiograph of a 20-year-old male college basketball player who sustained the injury shown. Which treatment most likely will allow quickest return to play?

RECOMMENDED READINGS
24. [Portland G, Kelikian A, Kodros S. Acute surgical management of Jones' fractures. Foot Ankle Int. 2003 Nov;24(11):829-33. PubMed PMID: 14655886.](http://www.ncbi.nlm.nih.gov/pubmed/14655886)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14655886)
25. [Fernández Fairen M, Guillen J, Busto JM, Roura J. Fractures of the fifth metatarsal in basketball players. Knee Surg Sports Traumatol Arthrosc. 1999;7(6):373-7. ](http://www.ncbi.nlm.nih.gov/pubmed/10639656)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10639656)
Which level has the smallest pedicle diameter?
From proximal to distal, pedicle sizes decrease from T1 to roughly the T4-T6 level, and then pedicle size increases in diameter. L1 is typically smaller than T12. The diameter, however, continues to increase in the lumbar spine and the sacrum.
RECOMMENDED READINGS
26. [Scoles PV, Linton AE, Latimer B, Levy ME, Digiovanni BF. Vertebral body and posterior element morphology: the normal spine in middle life. Spine (Phila Pa 1976). 1988 Oct;13(10):1082-6. PubMed PMID: 3206263. ](http://www.ncbi.nlm.nih.gov/pubmed/3206263)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3206263)
27. [Ofiram E, Polly DW, Gilbert TJ Jr, Choma TJ. Is it safer to place pedicle screws in the lower thoracic spine than in the upper lumbar spine? Spine (Phila Pa 1976). 2007 Jan 1;32(1):49-54. PubMed PMID: 17202892. ](http://www.ncbi.nlm.nih.gov/pubmed/17202892)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17202892)
28. [Christodoulou AG, Apostolou T, Ploumis A, Terzidis I, Hantzokos I, Pournaras J. Pedicle dimensions of the thoracic and lumbar vertebrae in the Greek population. Clin Anat. 2005 Sep;18(6):404-8. PubMed PMID: 16015613. ](http://www.ncbi.nlm.nih.gov/pubmed/16015613)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16015613)
RESPONSES FOR QUESTIONS 80 THROUGH 86
1. Well-fixed cemented stem
2. Well-fixed uncemented stem
3. Well-fixed uncemented stem with femoral osteolysis
4. Well-fixed uncemented stem with stress shielding
5. Loose cemented stem
6. Loose uncemented stem
For each image below, select the above response that best describes the femoral component.
Figure 80a
Figure 81
Figure 82


Figure 84

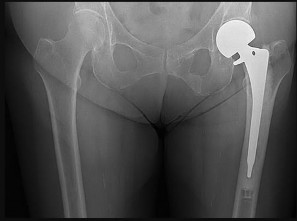
Figure 85


Figures 81, 83, and 84 reveal well-fixed uncemented stems and osseointegration around the porous portions of the stems without subsidence or pedestal formation. In Figure 83, there is osteolysis in the medial calcar, bony trabeculae about the lateral portion of the stem, and spot welds. Figure 84 shows proximal stress shielding around a well-fixed uncemented implant. Stress shielding is disuse
osteopenia that occurs in bone as a result of a metal prosthesis preventing bone from deformity or bending. This is an example of Wolff’s law, which states that bone will adapt to the load under which it is placed. This can be seen in the proximal femur, typically from a femoral stem that is larger in diameter; made of a stiffer material, such as cobalt and chromium; and/or is extensively porous coated. Stress shielding does not result in loosening of the implant because the osseointegration is still present.
Figures 82 and 86 show loose uncemented stems. Both figures reveal radiolucent lines around the entire implants, stem subsidence, and pedestal formation.
Figures 80a and 85 are stems with cemented fixation. Figure 85 is well fixed and has an adequate cement mantle around the entire prosthesis with interdigitation into the cancellous bone and no radiolucent lines. Figure 80b shows a fractured cement mantle and radiolucency at the bone-cement interface with poor cancellous bone integration of cement.
RECOMMENDED READINGS
1. White RE, Archibeck MJ. Evaluation of the painful total hip replacement. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:1343-1351.
2. MacDowell AD, Howie DW. Fixation by methyl methacrylate. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:184-194.
3. Jasty M, Kienapfel H, Griss P. Fixation by ingrowth. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. _The Adult Hip_. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:195-206.
4. [Duffy P, Masri BA, Garbuz D, Duncan CP. Evaluation of patients with pain following total hip replacement. Instr Course Lect. 2006;55:223-32. Review.](http://www.ncbi.nlm.nih.gov/pubmed/16958458)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16958458)
Which abnormality most likely is associated with the clinical photograph and radiograph findings in Figures 87a and 87b?


Apert syndrome has associated hand and craniofacial anomalies. The congenital hand difference in Apert syndrome is complex-complete syndactyly with multiple nail and underlying distal phalangeal synostoses (acrosyndactyly).
Many congenital hand differences involve associated cardiac defects because the heart and limbs develop simultaneously. A common example is radial dysplasia (formerly known as radial club hand) and associated cardiac defects.
The congenital upper extremity difference known to be a harbinger for intra-abdominal malignancy is hemihyperplasia (formerly known as hemihypertrophy). Hemihyperplasia may be isolated or associated with syndromes such as Beckwith-Wiedemann syndrome. Consultation with a medical geneticist and abdominal screening ultrasounds are recommended.
RECOMMENDED READINGS
5. [Catena N, Divizia MT, Calevo MG, Baban A, Torre M, Ravazzolo R, Lerone M, Sénès FM. Hand and upper limb anomalies in Poland syndrome: a new proposal of classification. J Pediatr Orthop. 2012 Oct-Nov;32(7):727-31. doi: 10.1097/BPO.0b013e318269c898. ](http://www.ncbi.nlm.nih.gov/pubmed/22955538)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22955538)
6. [Wilson MR, Louis DS, Stevenson TR. Poland's syndrome: variable expression and associated anomalies. J Hand Surg Am. 1988 Nov;13(6):880-2. ](http://www.ncbi.nlm.nih.gov/pubmed/2852197)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2852197)
7. [Online Mendielian Inheritance in Man. ](http://www.omim.org/entry/173800?search=poland%20&highlight=poland)[http://www.omim.org/entry/173800?search=poland](http://www.omim.org/entry/173800?search=poland%20&highlight=poland)[ ](http://www.omim.org/entry/173800?search=poland%20&highlight=poland)[&highlight=poland](http://www.omim.org/entry/173800?search=poland%20&highlight=poland)
A 75-year-old woman falls from standing height. She is found a few hours later by her family and is taken to the emergency department. She has more profound weakness in her upper extremities than lower. She can elevate her shoulders bilaterally but cannot grasp. Her sensation is slightly diminished in both upper extremities. What is the likely scenario?
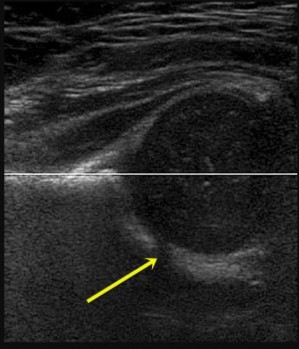

Anterior cord syndrome typically is a result of injury to the anterior spinal artery. Patients develop paralysis and loss of pain and temperature sensation below the level of the lesion, sparing the touch, vibration, and proprioceptions. Brown-Séquard syndrome causes ipsilateral paralysis, and ipsilateral loss of vibration and position sense below the level of the lesion. Patients experience impaired pain and temperature sensation contralateral to the side of the lesion. Cauda equina syndrome is the result of compression of the lower lumbosacral nerve roots. This is characterized by polyradiculopathy, motor weakness, and sphincter disturbances.
RECOMMENDED READINGS
8. [Guest J, Eleraky MA, Apostolides PJ, Dickman CA, Sonntag VK. Traumatic central cord syndrome: results of surgical management. J Neurosurg. 2002 Jul;97(1 Suppl):25-32. PubMed PMID: 12120648. ](http://www.ncbi.nlm.nih.gov/pubmed/12120648)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12120648)
9. Kepler CK, Kong C, Schroeder GD, Hjelm N, Sayadipour A, Vaccaro AR, Anderson DG. Early outcome and predictors of early outcome in patients treated surgically for central cord syndrome. J Neurosurg Spine. 2015 Oct;23(4):490-4. doi: 10.3171/2015.1.SPINE141013. Epub 2015 Jul 10.
[PubMed PMID: 26161520. ](http://www.ncbi.nlm.nih.gov/pubmed/26161520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26161520)
CLINICAL SITUATION FOR QUESTIONS 89 THROUGH 93
Figures 89a and 89b are the ultrasound and CT scan of a 20-month-old girl who has a dislocated, irreducible right hip attributable to developmental dysplasia. She has failed all nonsurgical treatment and is scheduled for open surgical reduction of her right hip.
Which approach will allow for the best visualization of all structures that may be impeding reduction through the interval between the pectineus and the femoral neurovascular bundle?
Numbness in the proximal lateral thigh is attributable to structure damage indicated by Figure 89b through which surgical approach?
Which surgical approach is less useful for children who have reached walking age because it does not allow for capsulorrhaphy?
During a medial approach to the hip, which anatomic structure identified in the figures can help surgeons locate the true acetabulum?
A 30-month-old boy underwent open reduction of his right hip to address developmental hip dysplasia. The reduction was performed through an anterior approach, and a shortening femoral osteotomy was not performed. Four months after surgery, hip radiographs reveal absence of ossification of the femoral epiphysis and fragmentation of the ossific nucleus. What is the likely cause of this complication?
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
1. Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. _Orthopaedic Knowledge Update: Pediatrics 4_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
2. [Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11730331)
3. Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
[24/. PubMed PMID: 759421. ](http://www.ncbi.nlm.nih.gov/pubmed/759421)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/759421)
4. Olszewski DC, Karol LA. The medial Ludloff open reduction in developmental dysplasia of the hip before the age of walking. Operative Techniques in Orthopaedics. 2013;23:109-114.
Figure 94 is the radiograph of a 60-year-old patient who has a drop-head deformity. What is the most likely cause?

There are no indications of muscular dystrophy in this scenario. Rheumatoid arthritis typically results in basilar invagination, subaxial subluxation, and/or atlantoaxial instability (none of which is an issue in this scenario). Down syndrome can cause atlantoaxial instability in approximately 15% of patients.
RECOMMENDED READINGS
5. Kaptain GJ, Simmons NE, Replogle RE, Pobereskin L. Incidence and outcome of kyphotic deformity following laminectomy for cervical spondylotic myelopathy. J Neurosurg. 2000 Oct;93(2 Suppl):199-
[204/. PubMed PMID: 11012049.](http://www.ncbi.nlm.nih.gov/pubmed/11012049)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11012049)
6. [Park DK, An HS. Problems related to cervical fusion: malalignment and nonunion. Instr Course Lect. 2009;58:737-45. PubMed PMID: 19385582. ](http://www.ncbi.nlm.nih.gov/pubmed/19385582)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19385582)
Excessive leg lengthening has been implicated as a risk factor for sciatic nerve palsy during total hip arthroplasty (THA). As a percentage of femur length, what is the maximum amount the sciatic nerve can safely be lengthened?
RECOMMENDED READINGS
7. [DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):101-11. Review. PubMed PMID: 10217818. ](http://www.ncbi.nlm.nih.gov/pubmed/10217818)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10217818)
8. [Nercessian OA, Piccoluga F, Eftekhar NS. Postoperative sciatic and femoral nerve palsy with reference to leg lengthening and medialization/lateralization of the hip joint following total hip arthroplasty. Clin Orthop Relat Res. 1994 Jul;(304):165-71. PubMed PMID: 8020209. ](http://www.ncbi.nlm.nih.gov/pubmed/8020209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8020209)
RESPONSES FOR QUESTIONS 96 THROUGH 99
1. Proximal phalangeal osteotomy alone
2. Proximal metatarsal osteotomy with a modified McBride procedure
3. Distal metatarsal osteotomy with a modified McBride procedure
4. First tarsometatarsal fusion with a modified McBride procedure
5. First metatarsophalangeal fusion
Please choose the most appropriate surgical treatment listed above to address each clinical scenario seen in the radiographs below.
The patient in Figure 96 has medial pain at the first metatarsophalangeal (MTP) joint and no other pain.

The patient in Figure 97 has medial pain at the first MTP joint and pain under the second metatarsal head, or transfer metatarsalgia, with a loose first tarsometatarsal joint.

The patient in Figure 98 has pain medially at the first MTP joint and no other pain.

The patient in Figure 99 has pain at the first MTP joint.

deformities. A lapidus procedure, or tarsometatarsal fusion, provides the highest potential to correct deformity plus the advantage of stabilizing the first tarsometatarsal joint and limiting or eliminating transfer metatarsalgia. A first MTP fusion is most appropriate for patients with severe first MTP arthrosis.
RECOMMENDED READINGS
1. [Easley ME, Trnka HJ. Current concepts review: hallux valgus part II: operative treatment. Foot Ankle Int. 2007 Jun;28(6):748-58. Review. PubMed PMID: 17592710.](http://www.ncbi.nlm.nih.gov/pubmed/17592710)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17592710)
2. [Coughlin MJ, Shurnas PS. Hallux rigidus. Grading and long-term results of operative treatment. J Bone Joint Surg Am. 2003 Nov;85-A(11):2072-88. PubMed PMID: 14630834. ](http://www.ncbi.nlm.nih.gov/pubmed/14630834)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14630834)
A 65-year-old woman with an unstable C2 fracture undergoes posterior fixation with a C1 lateral mass and C2 pars screw technique. Pulsatile bleeding is encountered while placing the C1 screw, which was placed across both cortices. Which artery is most likely injured?
RECOMMENDED READINGS
3. [Simsek S, Yigitkanli K, Turba UC, Comert A, Seçkin H, Tekdemir I, Elhan A.Safe zone for C1 lateral mass screws: anatomic and radiological study.Neurosurgery. 2009 Dec;65(6):1154-60; discussion 1160. doi:10.1227/01.NEU.0000351779.58845.62. ](http://www.ncbi.nlm.nih.gov/pubmed/19934975)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19934975)
4. [Murakami S, Mizutani J, Fukuoka M, Kato K, Sekiya I, Okamoto H, Abumi K, Otsuka T. Relationship between screw trajectory of C1 lateral mass screw and internal carotid artery. Spine (Phila Pa 1976). 2008 Nov 15;33(24):2581-5. doi:10.1097/BRS.0b013e318186b2fd. ](http://www.ncbi.nlm.nih.gov/pubmed/19011539)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19011539)
_**This is the last question of the exam.**_
_**GOOD LUCK**_
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-mcqs-online-anatomy-017
Orthopedic Anatomy Review | Dr Hutaif Basic Science Rev -...
ONLINE ORTHOPEDIC MCQS ANATOMY08 1 . During a retroperitoneal approach to the L4-5 disk, what structure must be l…
Orthopedic With Answer An Review | Dr Hutaif General Or -...
ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02 1 . A patient has right shoulder pain. Figure 1a shows a gadoliniu…
Orthopedic With Answer Anatomy Review | Dr Hutaif Basic -...
ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05 1 . A 65-year-old man with ankylosing spondylitis sustains an extension …
Orthopedic Anatomy Review | Dr Hutaif Basic Science Rev -...
ORTHOPEDIC MCQS O11 ANATOMY IMAGING Online 2011 Anatomy-Imaging Self-Assessment Examination by Dr.Dhahirortho 1 Q 1 1…
Orthopedic Anatomy Imag Review | Dr Hutaif Basic Scienc -...
ORTHOPEDIC MCQS ONLINE 014 ANATOMY IMAGING Anatomy Imaging Self-Assessment Examination AHMED ALTAEI RESPONSES FOR QUEST…