Surgical Management and Excision of the Tibial Sesamoid

Key Takeaway
The initial management of sesamoid pathology relies on conservative measures, including offloading orthoses and immobilization. When nonoperative treatment fails after a six-month trial, surgical excision of the involved sesamoid is indicated. This procedure requires meticulous dissection to protect the proper digital nerve and preserve the flexor hallucis brevis tendon, ensuring the mechanical integrity of the first ray while alleviating chronic pain and intractable plantar keratoses.
BIOMECHANICS AND PATHOANATOMY OF THE SESAMOID COMPLEX
The hallucal sesamoids are integral to the biomechanical function and structural integrity of the first metatarsophalangeal (MTP) joint. Embedded within the medial and lateral slips of the flexor hallucis brevis (FHB) tendon, the tibial (medial) and fibular (lateral) sesamoids articulate with the plantar facets of the first metatarsal head. They are separated by the crista, a longitudinal bony ridge that stabilizes their tracking during the gait cycle.
The primary functions of the sesamoids include absorbing weight-bearing forces, reducing friction, protecting the flexor hallucis longus (FHL) tendon as it glides between them, and increasing the mechanical advantage of the FHB by acting as a fulcrum. During the terminal stance phase of gait, the sesamoids transmit up to 300% of body weight, making them highly susceptible to acute trauma, repetitive microtrauma, and degenerative conditions.
Pathologic conditions affecting the sesamoids present a complex diagnostic and therapeutic challenge. Diagnoses encompass a wide spectrum of disorders, including:
* Sesamoiditis: A diagnosis of exclusion characterized by localized tenderness over the sesamoid without distinct radiographic abnormalities.
* Osteochondritis (Avascular Necrosis): Often affecting the tibial sesamoid, leading to fragmentation and collapse.
* Acute Calcific Tendinitis: Typically involving the lateral head of the FHB.
* Chronic Tendinitis: Often associated with traction osteophytes at the insertion into the sesamoid.
* Fractures: Acute traumatic or stress fractures, most commonly involving the tibial sesamoid due to its primary weight-bearing role.
* Intractable Plantar Keratoses (IPK) and Bursitis: Resulting from prominent plantar exostoses or structural malalignment.
CLINICAL AND RADIOGRAPHIC EVALUATION
A meticulous clinical examination is paramount. Palpation must precisely differentiate sesamoid tenderness from first metatarsal head pathology or FHL tendinitis. Pain exacerbated by passive dorsiflexion of the hallux against resistance often indicates a disruption of the sesamoid-FHB complex.
Standard weight-bearing anteroposterior (AP) and lateral radiographs of the foot are required, but the axial sesamoid view is the most critical imaging modality for evaluating the articular surface, the crista, and the presence of fractures or fragmentation.
FIGURE 81-106: Axial sesamoid view demonstrating a distinct fracture of the tibial sesamoid. Note the sharp, irregular radiolucent line differentiating it from a bipartite sesamoid, which typically features smooth, sclerotic margins.
Advanced imaging, such as magnetic resonance imaging (MRI) or technetium-99m bone scintigraphy, may be indicated to differentiate acute stress fractures from symptomatic bipartite sesamoids or to diagnose early osteochondritis before radiographic collapse occurs.
NONOPERATIVE MANAGEMENT
The initial treatment of sesamoid pathology is strictly nonoperative and depends on the severity of the clinical and radiographic findings. A comprehensive conservative protocol should be maintained for a minimum of 6 months before considering surgical intervention.
Modalities of Conservative Treatment
- Pharmacotherapy: Nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce acute capsular and bursal inflammation.
- Activity Modification: Immediate cessation of high-impact sports, jumping, or activities requiring extreme hallux dorsiflexion.
- Orthotic Management: Full-length rigid or semi-rigid shoe orthoses are the cornerstone of treatment. These must incorporate a metatarsal pad placed proximal to the metatarsal heads and a specific "dancer's pad" or U-shaped relief cutout directly beneath the first metatarsal head to offload the sesamoids.
- Shoe Modifications: A metatarsal bar applied to the outer sole of the shoe shifts the weight-bearing axis proximally, reducing pressure on the sesamoid complex during toe-off.
- Immobilization: In cases of acute fractures, severe osteochondritis, or recalcitrant sesamoiditis, a short-leg walking cast or a rigid controlled ankle motion (CAM) boot for 4 to 6 weeks may be required to achieve complete mechanical rest.
💡 Clinical Pearl: Orthotic Compliance
Shoe modifications and custom orthoses should be initiated preoperatively. If the patient is disturbed by their continual use or finds them intolerable, they must be adjusted until the patient is symptom-free or until nonoperative management is officially deemed a failure.
INDICATIONS FOR OPERATIVE INTERVENTION
If a lengthy (6-month) trial of nonoperative treatment fails to provide relief, surgical excision of the involved sesamoid (sesamoidectomy) is indicated. Surgery is most frequently performed in athletically active patients who wish to return to their sports more rapidly; however, patients must be counseled that surgical complications or prolonged rehabilitation can delay their return to activity.
Specific indications for sesamoidectomy include:
1. Recalcitrant sesamoiditis or osteochondritis.
2. Nonunion of a sesamoid fracture with persistent pain.
3. Symptomatic exostoses causing chronic ulceration.
4. Persistent bursitis and painful intractable plantar keratoses (IPK).
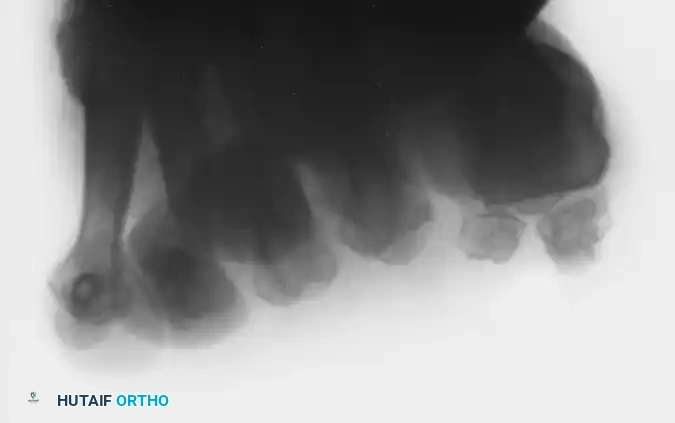
FIGURE 81-107A: Lateral radiograph demonstrating a prominent exostosis on the plantar surface of the tibial sesamoid.

FIGURE 81-107B: Clinical presentation of the same patient, revealing a severe keratotic lesion with intermittent ulceration directly underlying the exostosis. Excision of the sesamoid is definitively indicated.
Intractable Plantar Keratoses (IPK)
Hypertrophic sesamoids or plantar exostoses frequently lead to localized pressure points, resulting in painful keratoses and adventitial bursae. These lesions are highly resistant to superficial debridement and require removal of the underlying bony prominence.

FIGURE 81-108A: Persistent keratotic lesion beneath the tibial sesamoid.

FIGURE 81-108B: Intraoperative view of the bursa and keratotic lesion prior to excision.

FIGURE 81-108C: The excised tibial sesamoid and the overlying hypertrophic bursa. In this case, preoperative radiographs, including the axial sesamoid view, were normal, highlighting that soft tissue pathology alone can necessitate excision.

FIGURE 81-109: A diffuse, broad-based keratosis that persisted over a protracted period, completely unresponsive to aggressive nonoperative management and offloading.
SURGICAL TECHNIQUE: EXCISION OF THE TIBIAL SESAMOID
The excision of the tibial sesamoid requires meticulous anatomical knowledge to prevent iatrogenic complications, specifically injury to the proper digital nerve and postoperative hallux valgus deformity resulting from FHB incompetence.
🚨 Surgical Warning: Iatrogenic Deformity
Excision of the tibial sesamoid removes the medial stabilizing force of the first MTP joint. If the medial capsule and the remaining slips of the FHB are not meticulously repaired, the unopposed pull of the adductor hallucis and the lateral head of the FHB will rapidly induce an iatrogenic hallux valgus deformity.
Step 1: Patient Positioning and Anesthesia
The patient is placed supine on the operating table. A regional ankle block or a popliteal sciatic nerve block is administered, supplemented by intravenous sedation or general anesthesia. A calf or thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying fine neurovascular structures.
Step 2: Surgical Approach and Incision
Two primary approaches may be utilized: the medial approach and the plantar approach.
The Medial Approach (Preferred):
Make a 3-cm longitudinal incision along the medial aspect of the first MTP joint. This incision is placed in the internervous plane between the dorsal and plantar medial cutaneous nerves. This approach is highly preferred as it avoids a plantar scar, which can become a source of chronic pain.
The Plantar Approach (Alternative):
Alternatively, an incision can be made directly in the plantar midline if the capsule is to be opened and turned plantarward, allowing the sesamoid to be removed from the inside out. While this approach requires less capsular disruption, it places the proper digital branch of the medial plantar nerve at significant risk.
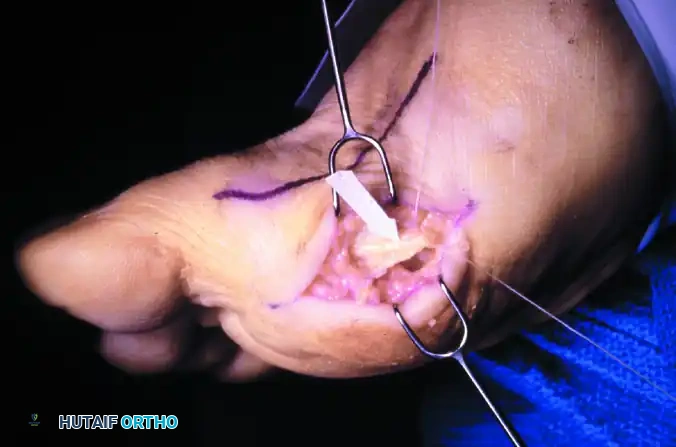
FIGURE 81-110A: Optional plantar-medial incision for the removal of the tibial sesamoid.
Step 3: Deep Dissection and Nerve Protection
Careful blunt dissection is carried out through the subcutaneous tissues. The proper digital branch of the medial plantar nerve, which supplies the medial side of the pulp of the hallux, must be identified and protected.

FIGURE 81-110B: The arrow and suture delineate the proper digital nerve to the medial side of the hallux. The nerve intimately blends with the capsule and subcutaneous tissue, making it highly vulnerable by both position and appearance during a plantar approach.
Locate the tibial sesamoid by direct palpation to differentiate it clearly from the plantar aspect of the first metatarsal head.
Step 4: Enucleation of the Sesamoid
The goal is to "shell" the sesamoid out of the capsule and plantar plate with minimal disruption to the surrounding tendinous structures.
1. Incise across the plantar surface and the articular surface of the sesamoid.
2. Remain acutely aware of the flexor hallucis longus (FHL) tendon, which lies immediately lateral to the tibial sesamoid.
3. Once the FHL is definitively identified, keep the great toe flexed 20 to 30 degrees. This maneuver relaxes the FHL and the plantar structures, facilitating exposure.
4. Carefully incise the intersesamoid ligament.
5. Grasp the tibial sesamoid with a towel clip or strong toothed forceps and apply medial traction.
6. Complete the excision by sharply releasing the medial head of the flexor hallucis brevis and its distal continuation to the base of the proximal phalanx of the hallux.
🔪 Surgical Technique Pearl: Preserving the FHB
A careful, sharp enucleation of the sesamoid (staying directly on the bone) can leave intact small, thin slips of the FHB tendon. Preserving this continuity is vital to maintaining the flexion moment of the first MTP joint and preventing a postoperative cock-up deformity.

FIGURE 81-110C: The excised tibial sesamoid, the intact tendon of the flexor hallucis longus (FHL), and the exposed undersurface (tibial sesamoid facet) of the first metatarsal head.
Step 5: Closure and Soft Tissue Balancing
Meticulous closure is mandatory to restore the biomechanical balance of the first ray.
* Close the medial side of the capsule tightly using heavy absorbable sutures (e.g., 2-0 or 0 Vicryl). Do not close the plantar side of the capsule, as this can tether the FHL or create painful plantar scarring.
* Ensure that the medial capsulorrhaphy provides sufficient tension to counteract the lateral pull of the adductor hallucis.
* Close the skin with nonabsorbable sutures (e.g., 3-0 or 4-0 Nylon) using a horizontal mattress or simple interrupted technique.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is designed to protect the capsular repair while allowing early weight-bearing to prevent stiffness.
Phase 1: Immediate Postoperative Period (Days 0 to 16)
* A bulky, compressive forefoot dressing is applied in the operating room.
* The patient is fitted with a postoperative rigid-soled shoe.
* Weight-bearing to tolerance is permitted immediately on the operated foot, emphasizing heel-weighting to protect the forefoot.
* The use of crutches or a walker is optional, depending on patient comfort and baseline mobility.
* Alternative: Occasionally, a short-leg walking cast is applied if the patient is highly active or non-compliant and wishes to be more mobile during the first 2 to 3 weeks without risking the repair.
Phase 2: Suture Removal and Transition (Weeks 2 to 6)
* Sutures are removed between 12 and 16 days postoperatively.
* The patient is transitioned into a wide, deep-toe-box shoe of their choice.
* A metatarsal pad placed inside the shoe, or a metatarsal bar on the outside of the shoe, is highly recommended for several months. These modifications offload the healing surgical site and prevent transfer metatarsalgia.
Phase 3: Return to Activity (Months 2 to 6)
* Physical therapy is initiated to restore active and passive range of motion of the first MTP joint.
* Strengthening of the intrinsic foot musculature and the FHL is emphasized.
* Return to high-impact sports is permitted only when the patient is entirely symptom-free, exhibits full strength in hallux plantarflexion, and demonstrates no signs of dynamic hallux valgus.
COMPLICATIONS AND SALVAGE
While sesamoidectomy is highly effective for recalcitrant pathology, complications can significantly delay a patient's return to activity.
- Iatrogenic Hallux Valgus: The most common structural complication following tibial sesamoidectomy. It results from failure to adequately repair the medial capsule and FHB. Salvage may require a medial capsulorrhaphy, adductor release, or an MTP arthrodesis in severe cases.
- Nerve Injury: Neuroma formation or numbness along the medial aspect of the hallux due to transection or traction injury of the proper digital nerve.
- Transfer Metatarsalgia: Altered biomechanics can shift weight-bearing forces to the lesser metatarsal heads or the remaining fibular sesamoid, leading to new areas of intractable plantar keratosis.
- Cock-up Deformity: Complete loss of the FHB insertion can lead to unopposed extensor hallucis longus (EHL) action, resulting in a hyperextended MTP joint and a flexed interphalangeal joint.
Strict adherence to the internervous surgical approach, meticulous subperiosteal enucleation, and robust capsular repair are the hallmarks of a successful sesamoidectomy, ensuring optimal outcomes for both sedentary patients and elite athletes.
You Might Also Like

