Arthritis of the Foot: Inflammatory and Degenerative Management
Key Takeaway
Inflammatory and degenerative arthritis of the foot present with distinct biomechanical challenges. While early stages share clinical manifestations like activity-related pain, rheumatoid arthritis drives progressive joint destruction via synovial hyperplasia and capsular attenuation. This leads to profound intrinsic-extrinsic muscle imbalance, dorsal metatarsophalangeal subluxation, and severe claw toe deformities. Management requires a stepwise approach, utilizing targeted orthoses, advanced serological diagnostics, and precise surgical reconstruction to restore functional anatomy and alleviate intractable pain.
SIGNS AND SYMPTOMS OF FOOT ARTHRITIS
The early clinical manifestations of both inflammatory and degenerative arthritis of the foot and ankle share significant overlap, necessitating a high index of clinical suspicion and meticulous physical examination. Pain is the hallmark symptom; it is typically exacerbated by weight-bearing activities and initially relieved with rest. However, as joint destruction progresses, the threshold for pain decreases. Patients with advanced arthropathy frequently report pain at rest or intractable nocturnal pain that disrupts sleep architecture.
A comprehensive history will reveal specific mechanical triggers. A typical patient with midfoot or hindfoot arthritis will describe sharp, localized pain during stair climbing, at extremes of motion (such as deep squatting or terminal toe raises), and during rotational movements (e.g., the pivoting phase of a golf swing). Furthermore, environmental factors play a documented, albeit debated, role in symptomatology. Changes in barometric pressure associated with shifting weather patterns are frequently cited by patients as exacerbating their baseline pain levels.
It is critical to differentiate intra-articular pathology from extra-articular inflammatory processes. Disease and inflammation of the surrounding soft tissues—such as tenosynovitis, adventitial bursitis, or plantar fasciitis—often accompany true joint disease but can occur independently.
Clinical Pearl: Radiographic evidence of osteoarthritis or rheumatoid arthritis may be an incidental finding. Always correlate radiographic severity with the patient's focal point of maximal tenderness. Treating extra-articular generators of pain, such as localized synovitis or bursitis, may yield profound symptomatic relief while preserving the native joint space.
Diagnostic Injections
When the clinical picture is obfuscated by overlapping pain generators, particularly in the complex articulation of the midfoot, diagnostic injections are invaluable. Fluoroscopically or CT-guided intra-articular injections utilizing a short-acting local anesthetic (e.g., 1% lidocaine), with or without a corticosteroid preparation, can isolate the symptomatic joint.
Surgical Warning: Caution is necessary in patients whose pain is unrelieved—even for a brief period—following a confirmed, image-guided intra-articular injection. If the anesthetic fails to abolish the pain, it is highly unlikely that surgical arthrodesis or arthroplasty of that specific joint will significantly improve the patient's symptoms.
DIAGNOSTIC SEROLOGY IN INFLAMMATORY ARTHRITIS
Differentiating degenerative osteoarthritis from systemic inflammatory arthropathies, particularly Rheumatoid Arthritis (RA), requires targeted serological evaluation. The following laboratory studies are critical adjuncts in the diagnostic workup:
- Erythrocyte Sedimentation Rate (ESR): A non-specific marker of systemic inflammation.
- C-Reactive Protein (CRP): An acute-phase reactant indicating active inflammation; highly responsive to disease flares.
- Complete Blood Cell Count (CBC): Often reveals a normochromic, normocytic anemia characteristic of chronic disease.
- Rheumatoid Factor (RF) Assay: Positive in 60% to 80% of RA patients. However, it carries a false-positive rate of 25% in the general population and is positive in fewer than 40% of patients with early-stage RA. It is not exclusively specific to rheumatoid arthritis.
- Antinuclear Antibody (ANA) Assay: Present in 25% to 30% of patients with RA. It is highly non-specific (95% of ANA-positive patients have systemic lupus erythematosus rather than RA).
- Anticyclic Citrullinated Peptide (Anti-CCP) Assay: The gold standard for RA diagnosis, boasting a 98% specificity for rheumatoid arthritis.
- Anti-RA33 Antibody Assay: Demonstrates an 85% specificity for rheumatoid arthritis and is useful in seronegative clinical pictures.
NONOPERATIVE TREATMENT PROTOCOLS
The cornerstone of initial management for foot arthritis is nonoperative, focusing on biomechanical offloading and systemic medical management.
Activity Modification and Physical Therapy
Activity modification emphasizing low-impact, closed-kinetic-chain exercises (e.g., cycling, aquatic therapy) should be strongly encouraged. Complete cessation of activity is detrimental to overall cardiovascular health and joint mobility; therefore, a guided transition to joint-sparing exercises is preferred. For patients with an elevated Body Mass Index (BMI), aggressive dietary counseling and weight management are imperative, as the forces transmitted through the midfoot and forefoot during the terminal stance phase of gait can exceed three times body weight.
Orthoses and Shoe Modifications
Shoe modifications offer profound symptomatic relief, particularly for midfoot and forefoot arthritis. The prescription of a wide toe-box, rocker-bottom shoe alters the biomechanics of gait by facilitating rollover, thereby reducing the required excursion of the metatarsophalangeal (MTP) and midtarsal joints.
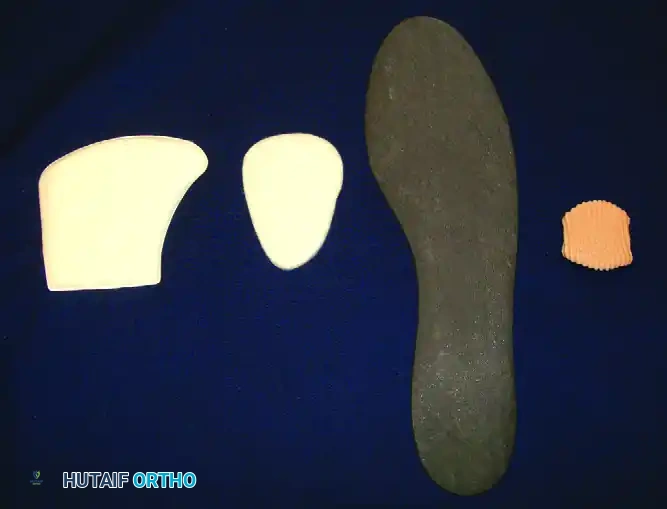
To further restrict painful articulation, a rigid carbon fiber plate insert or a built-in steel shank can be added to the sole. This stiffens the construct, effectively immobilizing the midfoot and forefoot during the propulsive phase of gait. Custom-molded ankle-foot orthoses (AFOs) or accommodative foot orthotics can significantly mitigate pain by redistributing plantar pressures away from prominent metatarsal heads.
Figure 1: Custom orthoses and rigid inserts designed to mitigate pain and improve function by limiting midfoot and forefoot excursion in patients with rheumatoid and degenerative deformities.
Pharmacotherapy
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first-line pharmacological intervention, provided there are no renal, gastrointestinal, or cardiovascular contraindications. In patients with confirmed rheumatoid arthritis, early referral to a rheumatologist for the initiation of Disease-Modifying Antirheumatic Drugs (DMARDs) and biologic agents is mandatory to halt progressive joint destruction.
FOREFOOT ARTHRITIS: HALLUX RIGIDUS
Hallux rigidus is the clinical term for degenerative arthritis of the first metatarsophalangeal joint. Historically described by Davies-Colley as a plantar-flexed proximal phalanx relative to the metatarsal head (coining the term hallux flexus), it was Cotterill in 1888 who accurately identified the limitation of motion in the first MTP joint as hallux rigidus.
While our understanding of the biomechanics has evolved, the exact etiology often remains elusive. Pathogenesis is generally attributed to:
1. Trauma: An acute osteochondral injury, often occurring in adolescence.
2. Repetitive Microtrauma: Chronic hyperextension of the first MTP joint during athletic activities (e.g., running, turf toe injuries).
3. Anatomic Predisposition: Conditions such as hallux valgus interphalangeus, metatarsus primus elevatus, or an abnormally long first metatarsal (index plus foot type).
A positive family history is frequently noted in patients presenting with bilateral hallux rigidus. Regardless of the inciting event, increased mechanical stress leads to focal cartilage degradation, secondary synovial hypertrophy, dorsal osteophyte formation, and progressive joint space narrowing.
ETIOLOGY OF JOINT DESTRUCTION IN RHEUMATOID ARTHRITIS
The pathophysiology of joint destruction in rheumatoid arthritis is fundamentally distinct from the mechanical wear-and-tear seen in primary osteoarthritis. RA is driven by an autoimmune cascade. Immune complexes deposit within the synovial membrane, triggering a profound inflammatory cellular response. This leads to synovial hyperplasia (pannus formation).
The hypertrophic synovium releases aggressive inflammatory cytokines (TNF-alpha, IL-1, IL-6) and matrix metalloproteinases (MMPs), which actively degrade articular cartilage and subchondral bone. Marginal articular erosions are the hallmark early radiographic finding, occurring at the "bare areas" of the joint where cartilage ends and the capsule attaches.
Crucially, this enzymatic degradation causes severe weakening and attenuation of the capsular ligaments and the plantar plate. This ligamentous failure is the primary catalyst for the profound structural deformities seen in the rheumatoid forefoot.
BIOMECHANICS OF RHEUMATOID FOREFOOT DEFORMITY
Hallux valgus is the predominant early clinical manifestation of rheumatoid arthritis in the foot, often preceding severe joint destruction. As the medial capsule of the first MTP joint attenuates due to synovitis, the hallux drifts into valgus, exacerbating the mechanical disadvantage of the lesser toes.
The deformity of the lesser toes follows a predictable and devastating biomechanical cascade:
1. Capsular Attenuation: Synovitis weakens the collateral ligaments and plantar plate of the lesser MTP joints.
2. Intrinsic Muscle Imbalance: Chronic dorsal subluxation of the MTP joints alters the vector of the intrinsic muscles (interossei and lumbricals). Normally plantar flexors of the MTP joint, these tendons are pulled dorsal to the joint's axis of rotation.
3. Vector Reversal: Once dorsal to the axis of rotation, the interossei and lumbricals are converted into weak extensors of the MTP joint, exacerbating the dorsal subluxation.
4. Extrinsic Overdrive: This intrinsic failure creates a massive imbalance with the extrinsic muscles (flexor digitorum longus and flexor hallucis longus). The loss of excursion of the extensor digitorum longus and brevis prevents extension of the middle and distal interphalangeal joints.
5. Claw Toe Formation: The result is a rigid claw toe deformity: severe hyperextension at the MTP joint and flexion at the proximal and distal interphalangeal (PIP and DIP) joints.
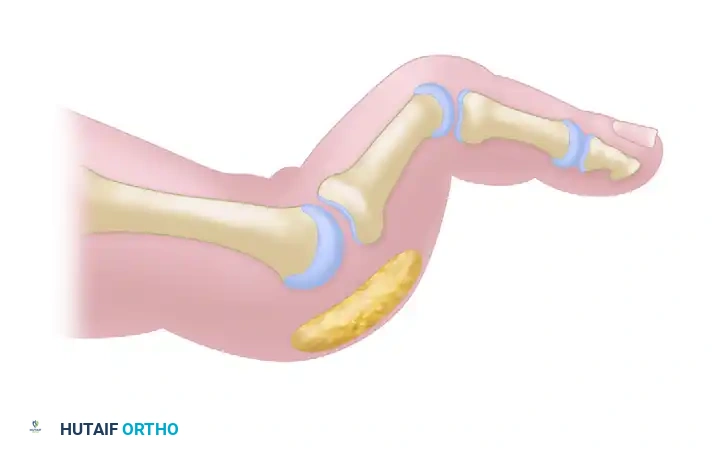
Figure 2: Normal alignment and balance of the metatarsophalangeal joints and toes, demonstrating the delicate equilibrium between intrinsic and extrinsic musculature.
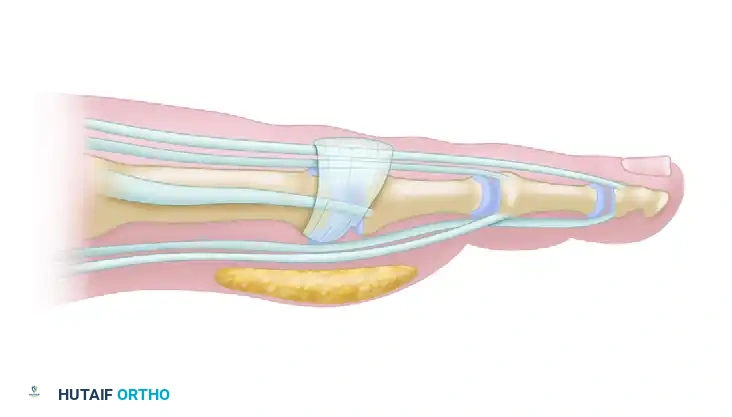
Figure 3: Normal sagittal anatomy of the lesser toe. Note the position of the intrinsic tendons plantar to the axis of rotation of the MTP joint, and the robust plantar fat pad protecting the metatarsal head.

Figure 4: Rheumatoid lesser toe contracture. As the MTP joint subluxates dorsally, the intrinsic tendons shift dorsal to the axis of rotation, exacerbating hyperextension. The plantar fat pad is dragged distally, leaving the metatarsal head prominent and unprotected.
Over time, the proximal phalanx dislocates completely, coming to rest on the dorsal aspect of the metatarsal neck. This dorsal dislocation forces the metatarsal heads plantarly. The protective plantar fat pad is dragged distally by the proximal phalanx, leaving the prominent metatarsal heads covered only by atrophic skin.

Figure 5: End-stage rheumatoid deformity. Complete dorsal dislocation of the metatarsophalangeal joint occurs, with the proximal phalanx ankylosing to the dorsal aspect of the metatarsal head.
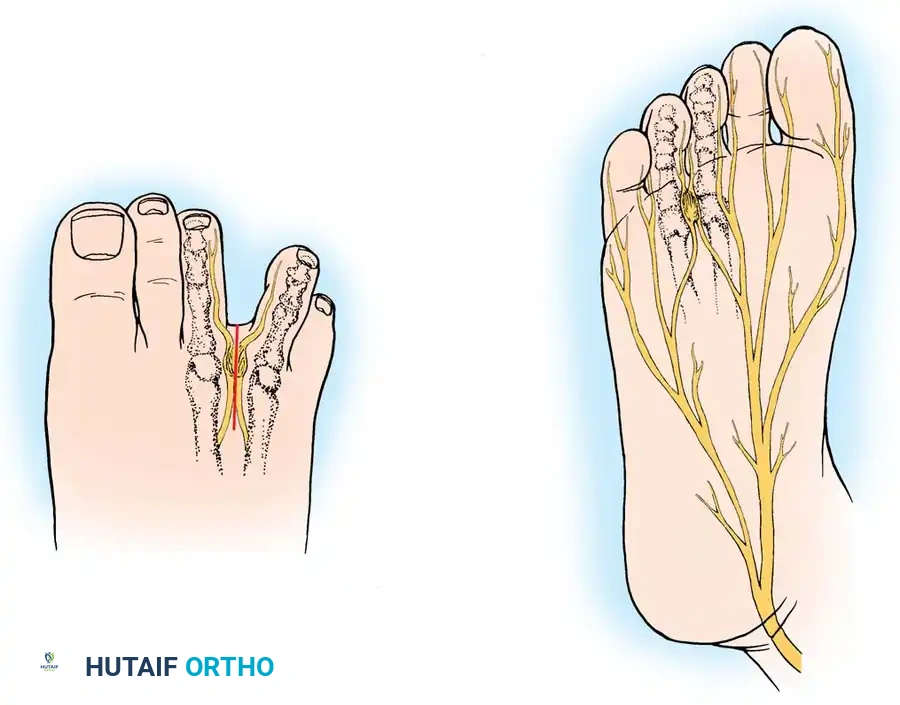
Clinical Consequences of Forefoot Deformity
This severe architectural collapse leads to several clinically significant and painful conditions:
* Intractable Plantar Keratoses (IPK): Painful callosities develop directly beneath the unprotected, prominent metatarsal heads.
* Skin Ulceration: High focal pressures over bony prominences can lead to full-thickness skin breakdown, posing a severe infection risk in immunocompromised RA patients.
* Dorsal Corns: Painful hyperkeratotic lesions form over the dorsum of the flexed PIP joints due to shoe friction.
* End Corns: Lesions develop at the nail-pulp junction of the distal phalanx due to abnormal weight-bearing on the tip of the clawed toe.
* Fifth Toe Varus: The fifth digit frequently collapses into a varus position, overriding or underriding the fourth digit.
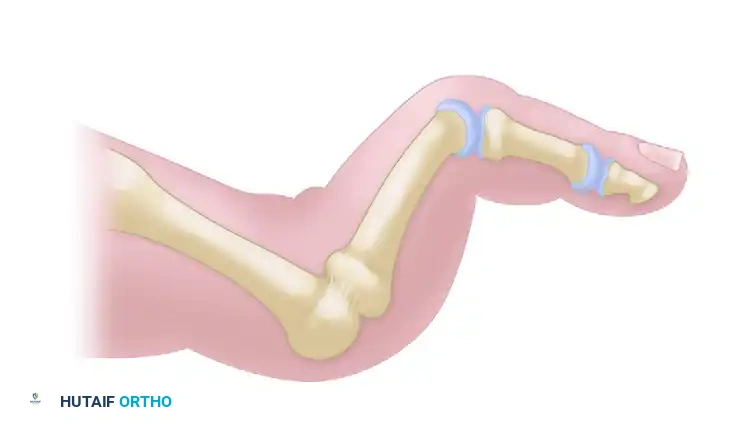
Figure 6: Severe claw toe deformity in the right foot of a patient with advanced rheumatoid arthritis. Note the profound hallux valgus, overriding lesser toes, and dorsal MTP dislocations. The left foot has undergone successful surgical reconstruction.
SURGICAL MANAGEMENT OF THE RHEUMATOID FOREFOOT
When nonoperative measures fail to control intractable pain or when severe deformity threatens skin integrity, surgical reconstruction is indicated. The gold standard for the severely deformed rheumatoid forefoot is Arthrodesis of the First Metatarsophalangeal Joint combined with Lesser Metatarsal Head Resection Arthroplasty (Hoffmann Procedure).
Preoperative Planning and Positioning
- Medical Optimization: Coordinate with the patient's rheumatologist regarding the perioperative management of DMARDs and biologics to balance infection risk with the risk of a systemic disease flare.
- Positioning: The patient is placed supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, bringing the foot pointing directly toward the ceiling.
- Tourniquet: A well-padded thigh or calf tourniquet is applied to ensure a bloodless surgical field.
Step-by-Step Surgical Approach
1. Arthrodesis of the First MTP Joint
Arthrodesis provides a stable, pain-free medial column, which is essential for the success of the lesser toe reconstruction.
* Incision: A dorsal longitudinal incision is made just medial to the extensor hallucis longus (EHL) tendon, extending from the mid-shaft of the first metatarsal to the interphalangeal joint.
* Joint Preparation: The capsule is incised, and the joint is exposed. Severe osteophytes and pannus are debrided. Using cup-and-cone reamers, the articular cartilage of the metatarsal head and the base of the proximal phalanx is removed down to bleeding subchondral bone.
* Positioning: The hallux is positioned in 10 to 15 degrees of valgus and 15 to 20 degrees of dorsiflexion relative to the first metatarsal shaft. Neutral rotation must be strictly maintained to prevent painful nail edge impingement.
* Fixation: Rigid internal fixation is achieved using a dorsal low-profile titanium plate and an interfragmentary compression screw.
2. Lesser Forefoot Arthroplasty (Metatarsal Head Resection)
- Incisions: Two dorsal longitudinal incisions are typically utilized: one centered in the second web space (accessing the 2nd and 3rd MTP joints) and one in the fourth web space (accessing the 4th and 5th MTP joints). Alternatively, a transverse plantar approach can be used if severe plantar callosities require excision.
- Resection: The extensor tendons are retracted or lengthened (Z-plasty). The dorsal capsule is incised, and the collateral ligaments are released to mobilize the dislocated proximal phalanx.
- Osteotomy: An oscillating saw is used to resect the metatarsal heads. The resection must be meticulously cascaded, with the second metatarsal left longest and the fifth metatarsal shortest, maintaining a smooth, parabolic curve to prevent transfer metatarsalgia.
- Soft Tissue Balancing: The plantar plate is mobilized and pulled dorsally over the resected metatarsal stump to provide a soft tissue interposition.
- Pinning: The lesser toes are reduced and stabilized with smooth 0.045-inch Kirschner wires (K-wires) driven antegrade through the toe and retrograde into the metatarsal shafts.
Postoperative Protocol
- 0-4 Weeks: The patient is placed in a bulky, compressive forefoot dressing and a rigid heel-weight-bearing shoe. Strict elevation is mandated to control edema.
- 4 Weeks: The K-wires in the lesser toes are removed in the clinic. The patient may begin progressive weight-bearing in a stiff-soled postoperative shoe.
- 6-8 Weeks: Radiographs are obtained to confirm consolidation of the first MTP arthrodesis. Once clinical and radiographic union is achieved, the patient is transitioned to a wide toe-box, supportive athletic shoe.
Surgical Warning: Failure to adequately shorten the lesser metatarsals during resection arthroplasty will result in recurrent dorsal dislocation of the proximal phalanges and persistent plantar ulcerations. The metatarsal parabola must be perfectly restored.
You Might Also Like