Interdigital Neuroma (Morton's Toe): Comprehensive Surgical Management
Key Takeaway
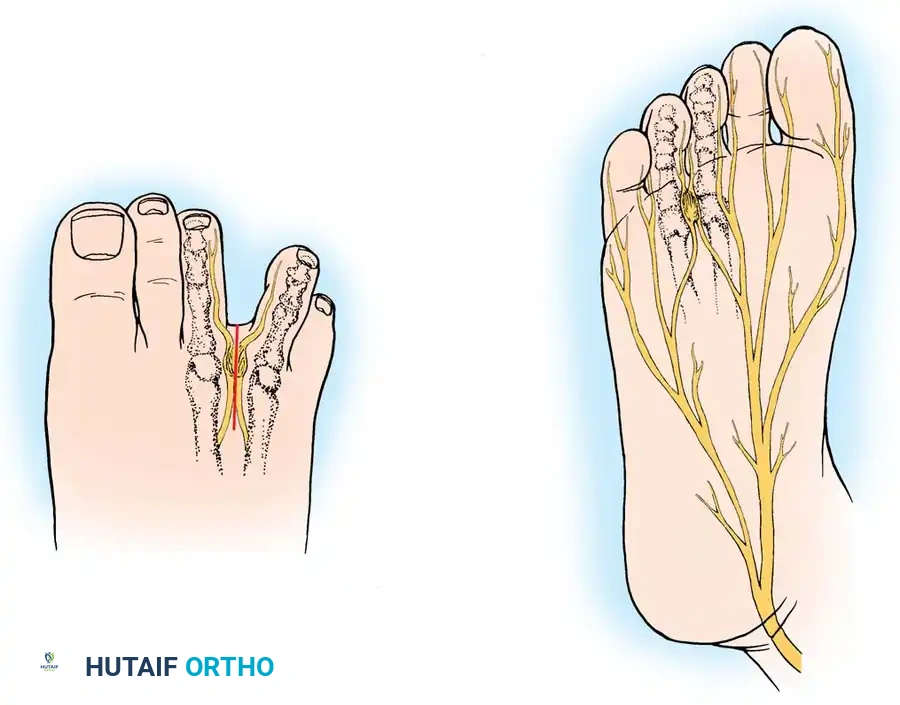
Interdigital neuroma, or Morton's toe, is a degenerative perineural fibrosis of the common digital nerve, most frequently affecting the third web space. Diagnosis is primarily clinical, characterized by forefoot pain and a positive Mulder's click. When conservative measures fail, surgical excision via a dorsal or plantar approach yields high satisfaction rates. This guide details the anatomical biomechanics, histological findings, and step-by-step operative techniques for successful neuroma resection.
Introduction and Historical Background
Interdigital neuroma, universally recognized by its eponym Morton's toe, is a common, painful affliction of the forefoot characterized by entrapment and subsequent degeneration of the common digital nerve. The condition was first described in 1845 by Durlacher, chiropodist to the Queen of England, who identified it as a "form of neuralgic affection" involving the plantar nerve between the third and fourth metatarsal bones. In 1876, Thomas G. Morton expanded upon this clinical description, postulating that the pathology resulted from the pinching of the common digital branch of the lateral plantar nerve between the mobile fourth and fifth metatarsal heads.
Historically, the exact etiology has been a subject of intense academic debate. Numerous theories have been advanced over the past century:
* Pollosson: Suggested laxity of the transverse metatarsal ligament, allowing a break in the anterior arch with plantar displacement of the central metatarsal heads.
* Guthrie & Woodruff: Proposed instability of the fourth metatarsophalangeal (MTP) joint.
* Jones & Tubby: Hypothesized a "pressure neuralgia" developing during weight-bearing.
* McElvenny: Theorized the presence of a tumor involving the lateralmost branch of the medial plantar nerve.
* Nissen: Suggested lumen occlusion in the common digital artery adjacent to the nerve.
In 1940, Betts introduced a compelling anatomical theory. He reasoned that the singular anatomy of the fourth digital branch of the medial plantar nerve was the primary culprit. This branch receives a communicating branch from the common digital branch of the lateral plantar nerve. Because of this anatomical convergence, the common digital nerve to the third web space is thicker and inherently more susceptible to compression against the unyielding deep transverse intermetatarsal ligament (DTML) located dorsal to it.
Clinical Pearl: While Betts' theory of the communicating branch is anatomically sound in many patients, an anatomical review by Levitsky et al. demonstrated that this communicating branch was absent in 73.2% of cadaveric feet. Neuromas were identified in almost equal distribution between the second and third web spaces, indicating that while nerve thickness plays a role, repetitive microtrauma against the DTML remains the primary mechanical driver.
Pathophysiology and Histological Findings
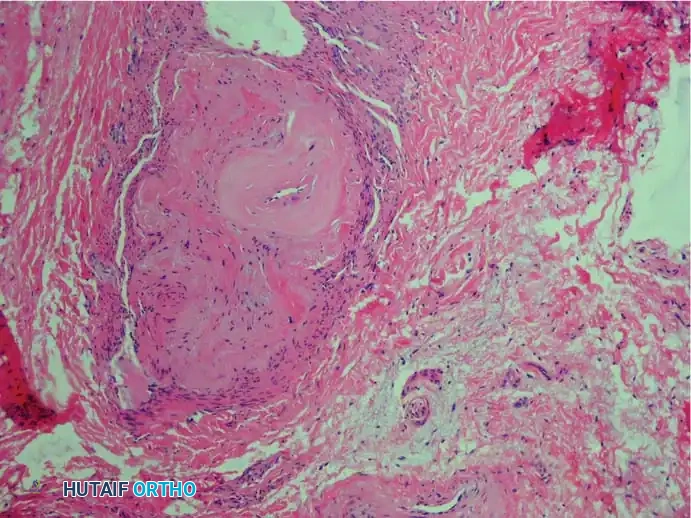
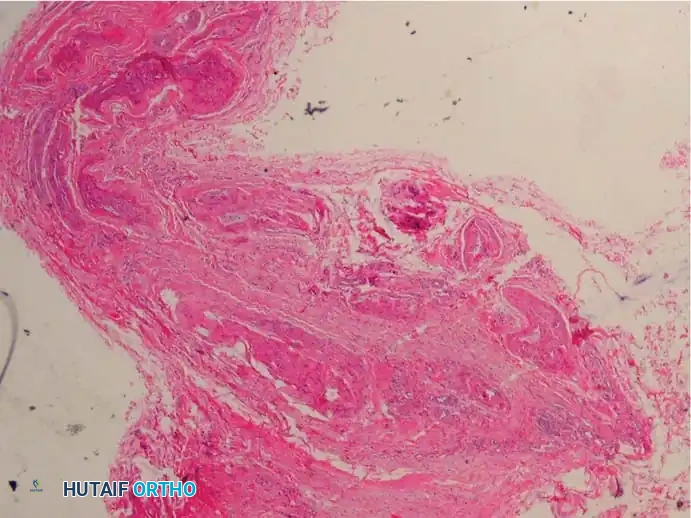
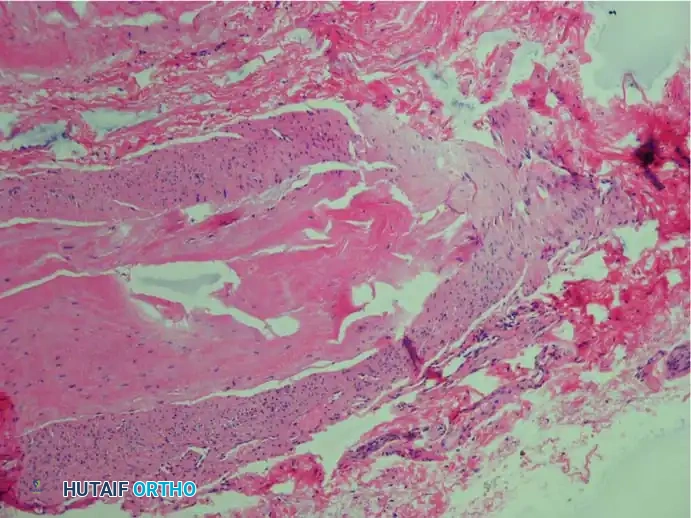
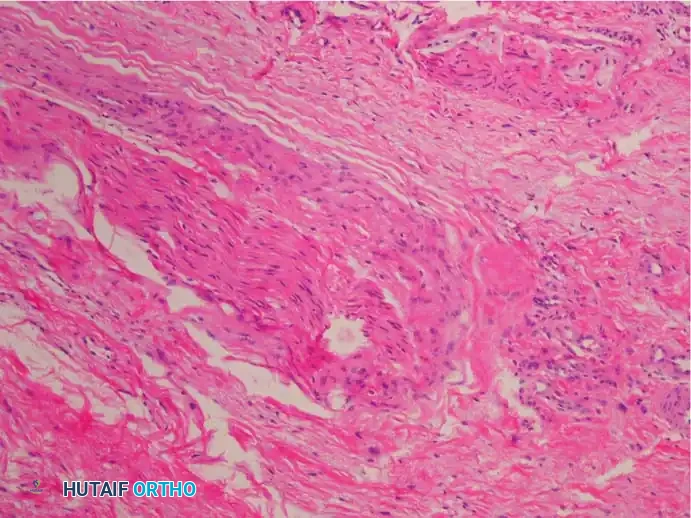
In a strict histopathological sense, the term neuroma is a misnomer. The haphazard proliferation of axons characteristic of a true traumatic neuroma is absent. Instead, the enlargement of the nerve is driven by the deposition of hyaline and collagenous material. The pathological process is fundamentally degenerative rather than proliferative. Consequently, Weinfeld and Myerson have advocated for the more accurate term, interdigital neuritis.
The pathogenesis is multifactorial, driven by repetitive microtrauma, perineural fibrosis, ischemia from vasa nervorum occlusion, and endoneural edema.
The essential histological findings, as described by Bickel, Dockerty, Lassmann, and others, include:
1. Perineural Fibrosis: Extensive thickening of the perineurium.
2. Vascular Changes: Increased number of intrafascicular arterioles exhibiting thickened and hyalinized walls due to multiple layers of basement membranes.
3. Axonal Degeneration: Demyelination and degeneration of nerve fibers with a marked decrease in the number of axis cylinders.
4. Endoneural Edema: Fluid accumulation within the endoneurium.
5. Absence of Inflammation: A distinct lack of acute inflammatory cells.
6. Bursal Tissue: Frequent presence of reactive intermetatarsal bursal tissue accompanying the nerve specimen.
Clinical Presentation and Diagnostic Evaluation
The diagnosis of an interdigital neuroma remains primarily clinical. Women are significantly more affected than men, and the condition is usually unilateral.
Signs and Symptoms
The hallmark symptom is severe, episodic pain located in the region of the metatarsal heads—most frequently the third and fourth. Patients often describe the pain as burning, aching, or cramping, occasionally radiating into the adjacent toes. A classic patient history includes pain that is exacerbated by weight-bearing, particularly in narrow, high-heeled shoes, and rapidly relieved by removing the shoe and massaging the forefoot. Subjective numbness of the toes of the involved interspace is common, though objective signs of decreased sensibility are rare.
Physical Examination
The most consistent physical finding is localized tenderness in the affected web space, just distal to the transverse intermetatarsal ligament.

Mulder's Sign: Described by Mulder, this is a pathognomonic clinical test. The examiner manually squeezes the metatarsal heads together with one hand, pushing the neuroma plantarward, while the thumb of the opposite hand rests on the plantar aspect of the suspected web space. A palpable, and sometimes audible, "click" occurs as the enlarged neuroma pops back and forth across the unyielding transverse ligament.

Diagnostic Pitfall: Palpating the web spaces with the patient standing is highly useful for differentiating a second web space neuroma from a plantar plate tear or instability at the second MTP joint. If tenderness is strictly in the web space and not on the plantar aspect of the proximal phalanx base or the MTP joint itself, a neuroma is the likely diagnosis.
Imaging Modalities
While plain weight-bearing radiographs of the foot should be obtained to rule out bony pathology (e.g., stress fractures, Freiberg's infraction, arthritis), they will be negative for a neuroma. Although MRI and ultrasonography are frequently utilized in modern practice to confirm the diagnosis or rule out associated bursitis, studies by Resch et al. have concluded that they are of limited value compared to a rigorous clinical examination. The diagnosis of Morton's toe remains a clinical one.
Nonoperative Management
Conservative treatment should always be the first line of management, as it can provide relief in a significant subset of patients.
* Footwear Modification: Transitioning to shoes with a wide toe box and a low heel reduces mechanical compression across the forefoot.
* Orthotics: Metatarsal pads or bars placed proximal to the metatarsal heads can help splay the rays and elevate the transverse arch, relieving pressure on the nerve.
* Injections: A local injection of a corticosteroid mixed with a local anesthetic into the affected web space (approached dorsally to avoid plantar fat pad atrophy) can provide both diagnostic confirmation and therapeutic relief.
Surgical Management
When nonoperative measures fail to provide durable relief, surgical intervention is indicated. The mainstay of operative treatment is the excision of the neuroma, a procedure independently popularized by Betts and McElvenny.
Surgical Warning: Preoperative patient counseling is paramount. While 80% to 95% of patients achieve complete pain relief, studies by Mann and Reynolds note that up to 65% of patients may experience mild residual local plantar tenderness, and 68% will note permanent numbness in the involved interspace. Patients must understand that the primary goal is the relief of neuralgic pain, not the restoration of normal sensation.
Technique 1: Dorsal Approach for Neuroma Excision
The dorsal approach is the most common primary surgical technique. It avoids a plantar scar, which can be a source of intractable postoperative pain, and allows excellent visualization of the deep transverse intermetatarsal ligament.
Step-by-Step Procedure:
1. Positioning and Anesthesia: The patient is placed supine. The procedure can be performed under a regional ankle block or general anesthesia with a calf or thigh tourniquet.
2. Incision: Make a 3 to 4 cm longitudinal incision centered over the dorsal aspect of the affected web space, beginning at the web and extending proximally between the metatarsal heads.
3. Dissection: Deepen the incision through the subcutaneous tissue. Carefully identify and retract any dorsal sensory nerve branches to avoid painful postoperative dorsal neuromas.
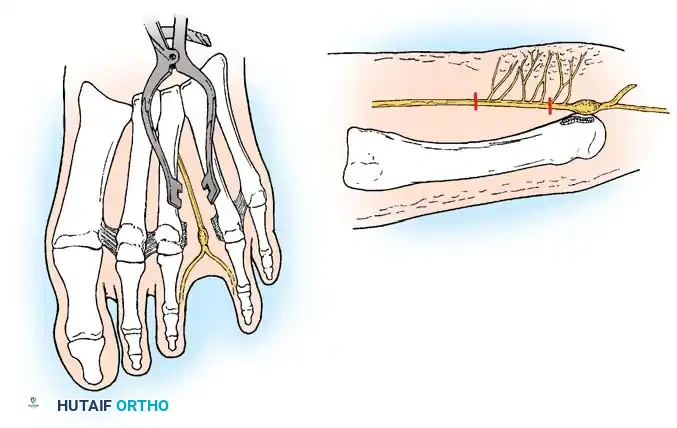
4. Exposure: Insert a self-retaining retractor (e.g., a Weitlaner) or a lamina spreader between the metatarsal heads. Gently spread the metatarsals to place the deep transverse intermetatarsal ligament under tension.
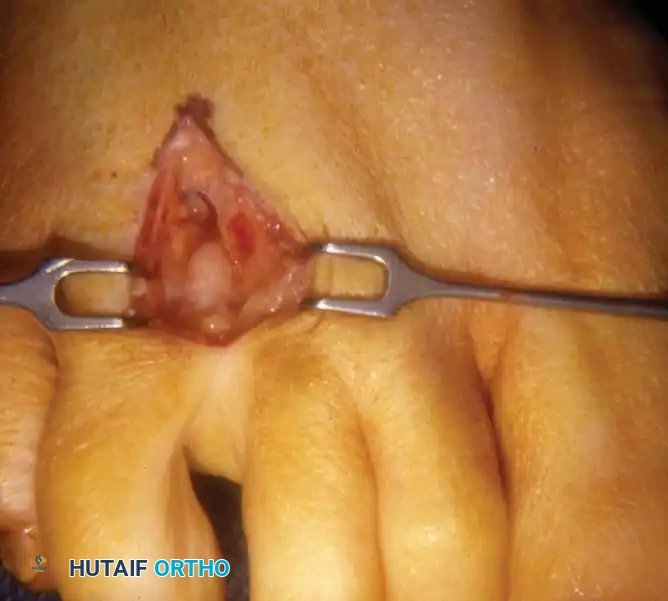
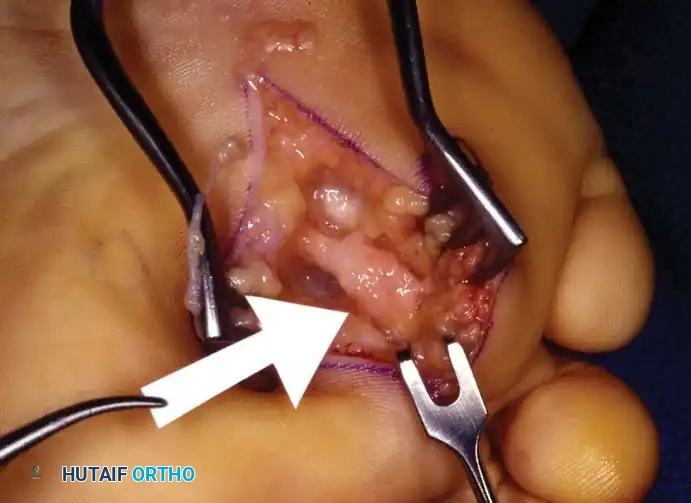
5. Ligament Release: Identify the distal edge of the DTML. Using a scalpel or dissecting scissors, carefully transect the ligament completely. Once the ligament is released, the underlying neuroma will frequently bulge dorsally into the operative field.
6. Nerve Resection: Isolate the common digital nerve. Dissect distally to identify the bifurcation into the proper digital nerves. Transect these branches just distal to the bifurcation.
7. Proximal Transection: Apply gentle distal traction to the nerve. Dissect proximally into the proximal intermetatarsal space. It is critical to transect the nerve 1 to 2 cm proximal to the weight-bearing pad of the metatarsal heads. Cut the nerve sharply under tension so that the proximal stump retracts deep into the intrinsic musculature (lumbricals), minimizing the risk of a symptomatic stump neuroma.
8. Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with non-absorbable sutures. The DTML is not repaired.

Technique 2: Plantar Approach for Neuroma Excision
The plantar approach is highly effective and is often the preferred approach for revision surgery (recurrent or stump neuromas) or for very proximally located lesions. It provides direct, unhindered anatomical access to the nerve proximal to the DTML without the need to divide the ligament.
Step-by-Step Procedure:
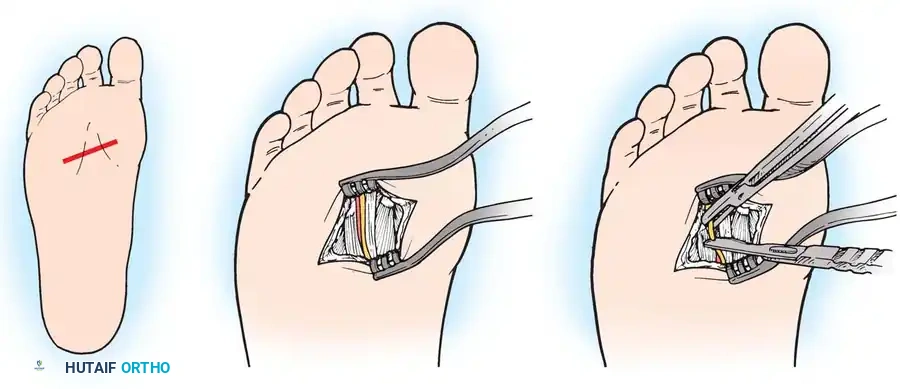
1. Incision: Make a longitudinal plantar incision centered over the affected interspace. Crucially, the incision must begin distal to the primary weight-bearing pad of the metatarsal heads and extend proximally, avoiding the peak pressure areas of the sole.
2. Dissection: Deepen the incision through the plantar fat pad and plantar aponeurosis.
3. Nerve Identification: The common digital nerve is identified directly beneath the plantar fascia, superficial to the lumbrical musculature.
4. Resection: Isolate the neuroma. Dissect distally to the bifurcation and proximally to healthy nerve tissue. Resect the nerve sharply, ensuring the proximal stump lies in a non-weight-bearing zone.
5. Closure: Close the plantar fascia if possible, followed by deep dermal and skin closure using vertical mattress sutures to ensure eversion of the thick plantar skin.

Alternative Technique: Epineural Neurolysis (Gauthier)
While excision is the gold standard, some surgeons advocate for nerve preservation. Gauthier reported on 206 patients treated with epineural neurolysis and DTML release.
* Technique: Using a dorsal approach, the DTML is released, allowing the common digital nerve to rise dorsally away from compressive forces. Under binocular loupes or a microscope, an epineural neurolysis is performed.
* Outcomes: Gauthier reported 83% of patients had relief of pain. However, critical evaluation shows that 12.5% had persistent pain, and 13.2% developed "mechanical pain" at the adjacent metatarsal heads due to the loss of the stabilizing DTML. Due to these unpredictable results, complete excision remains the preferred technique for most orthopedic surgeons.
Postoperative Protocol and Rehabilitation
Standardized postoperative care is essential to prevent wound complications, particularly with the plantar approach.
* Immediate Post-op: The foot is placed in a bulky, compressive soft dressing.
* Weight-Bearing: Patients are allowed heel-touch or flat-foot weight-bearing in a rigid, postoperative hard-soled shoe immediately after surgery. Forefoot loading and toe-off mechanics are strictly prohibited.
* Suture Removal: Sutures are typically removed at 14 to 21 days, depending on the incision site (plantar incisions may require up to 3 weeks for secure healing).
* Return to Activity: Patients can gradually transition to wide, supportive athletic shoes at 3 to 4 weeks. High-impact activities and the use of narrow or high-heeled shoes should be avoided for at least 6 to 8 weeks.
Complications
While generally highly successful, surgical excision of an interdigital neuroma carries specific risks:
1. Stump Neuroma (Recurrence): The most common cause of failed neuroma surgery. It occurs when the nerve is transected too distally, allowing the proximal stump to tether to the DTML or lie directly beneath the weight-bearing metatarsal head. Treatment requires a revision excision, typically via a plantar approach, to resect the nerve further proximally into the intrinsic muscles.
2. Incisional Pain/Keratosis: Particularly associated with the plantar approach if the incision crosses the weight-bearing pad.
3. Digital Deformity: Splaying of the toes can occasionally occur due to the release of the deep transverse intermetatarsal ligament, though this is rarely symptomatic.
4. Complex Regional Pain Syndrome (CRPS): A rare but severe complication requiring aggressive pain management and physical therapy.
You Might Also Like


