Interdigital Neuroma Excision: The Dorsal Approach

Key Takeaway
The dorsal approach for interdigital neuroma excision provides excellent visualization of the deep transverse metatarsal ligament and common digital nerve while avoiding a painful plantar scar. Success depends on complete ligament release, meticulous proximal nerve dissection, and burying the transected nerve stump in the non-weight-bearing interosseous musculature to prevent recurrent stump neuromas. This guide details the step-by-step surgical technique, anatomical considerations, and postoperative protocols for optimal patient outcomes.
INTRODUCTION AND PATHOPHYSIOLOGY
Interdigital neuroma, commonly referred to as Morton’s neuroma, is a mechanically induced compressive neuropathy of the common plantar digital nerve. Despite the nomenclature, it is not a true neoplastic neuroma but rather a localized perineural fibrosis, endoneurial edema, and axonal degeneration caused by repetitive microtrauma and entrapment beneath the deep transverse metatarsal ligament (DTML).
The condition predominantly affects the third intermetatarsal space, followed by the second. The anatomical predisposition of the third web space is multifactorial. It is the site where the medial and lateral plantar nerves frequently anastomose, resulting in a comparatively thicker common digital nerve. Furthermore, the third web space represents the biomechanical transition zone between the hypermobile fourth and fifth metatarsals and the relatively rigid first, second, and third metatarsals. During the terminal stance phase of gait, the common digital nerve is subjected to severe shearing forces and compression against the unyielding DTML.
Surgical excision is indicated for patients who have failed exhaustive conservative management, including footwear modifications (wide toe box, rigid sole), metatarsal offloading pads, nonsteroidal anti-inflammatory drugs (NSAIDs), and targeted corticosteroid or alcohol sclerosing injections. The dorsal approach is the gold standard for primary excision, as it provides excellent exposure of the neurovascular bundle and the DTML while entirely avoiding the creation of a potentially debilitating, painful plantar scar on the weight-bearing surface of the forefoot.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of forefoot anatomy is mandatory to execute a safe and definitive excision while minimizing the risk of recurrence or iatrogenic injury.
- Deep Transverse Metatarsal Ligament (DTML): A strong, inelastic fibrous band connecting the plantar plates of adjacent metatarsophalangeal (MTP) joints. It serves as the primary tethering structure over the neurovascular bundle.
- Common Plantar Digital Nerve: Courses longitudinally in the intermetatarsal space, strictly plantar to the DTML. Just distal to the ligament, it bifurcates into the proper digital nerves supplying the adjacent aspects of the toes.
- Vascular Supply: The common digital artery typically courses proximal-medial to distal-lateral, lying dorsal to the nerve. It frequently emerges from beneath the medial metatarsal neck.
- Lumbrical Muscles: The lumbrical tendon passes plantar to the DTML and medial to the base of the proximal phalanx. It must be carefully protected during ligamentous release.
Clinical Pearl: The most common cause of failed interdigital neuroma surgery is incomplete release of the deep transverse metatarsal ligament and inadequate proximal resection of the nerve, leading to a symptomatic stump neuroma tethered in the weight-bearing zone.
PREOPERATIVE PREPARATION AND POSITIONING
Patient Positioning
- The patient is placed in the supine position on the operating table.
- A small bump or sandbag is placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a neutral, directly vertical position.
- A well-padded calf or ankle tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the delicate proper digital branches and the common digital artery.
- Surgical loupe magnification (2.5x to 3.5x) is highly recommended to aid in the meticulous dissection of the neurovascular bundle and to differentiate the nerve from adjacent vascular and tendinous structures.
Anesthesia
The procedure is typically performed under Monitored Anesthesia Care (MAC) combined with a regional ankle block or a localized Mayo block. General anesthesia is rarely required unless dictated by patient comorbidities or severe anxiety.
SURGICAL TECHNIQUE: STEP-BY-STEP DORSAL APPROACH
1. Incision and Superficial Dissection
Make a dorsal longitudinal incision approximately 3 to 4 cm in length. The incision should begin proximally in the intermetatarsal space and extend distally, terminating just proximal to the web space commissure.
Surgical Warning: Do not blindly follow the course of the extensor tendons. The extensor tendons deviate laterally as they approach the digits. A properly placed incision must be slightly oblique and medial in relation to the extensor tendons to remain centered over the intermetatarsal space.
Deepen the dissection through the subcutaneous tissue. Carefully identify and retract the dorsal sensory nerve branches (branches of the superficial peroneal or sural nerves, depending on the web space) to the side of least resistance using delicate skin hooks or a Senn retractor.
2. Deep Dissection and Web Space Exposure
Proximally, identify the dorsal interosseous fascia. Incise this fascia longitudinally and follow the dorsal interosseous muscle distally, leading directly to the intermetatarsal bursa that overlies the DTML.
Open the bursa to expose the underlying intermetatarsal ligament. Bluntly dissect proximally between the adjacent metatarsals (e.g., the third and fourth metatarsals for a third web space neuroma). Retract the corresponding dorsal interosseous muscle medially to open the web space and enhance proximal visualization.
To achieve optimal exposure, insert a small (6 ½-inch) lamina spreader between the metatarsal necks. Gently open the spreader to distract the metatarsals.
FIGURE 86-10: Interdigital neuroma (dorsal approach) visualized after distraction of the metatarsal necks with a lamina spreader. Note the clear exposure of the intermetatarsal space.
Retract the web space fat pad distally using the deep blade of a Senn or Ragnell retractor. At this stage, a large, bulbous interdigital neuroma may be immediately visible bulging just distal to the DTML.
Pitfall: Do not apply upward pressure on the plantar aspect of the foot to extrude the neuroma dorsally. While this makes the neuroma easier to see, it artificially distorts the anatomy, providing a false sense of proximal exposure. This maneuver is a primary reason for incomplete proximal resection and subsequent recurrence.
3. Release of the Deep Transverse Metatarsal Ligament
The complete division of the DTML is the most critical step in decompressing the web space.
1. Identify the distal margin of the intermetatarsal ligament.
2. Using a No. 15 blade or tenotomy scissors, carefully divide the ligament along its entire longitudinal length from distal to proximal.
3. Maintain strict control of the cutting instrument to protect the underlying structures, specifically the lumbrical tendon and the neurovascular bundle located immediately plantar to the ligament.
4. Once released, use digital manipulation or a blunt probe to sweep proximally and confirm that no residual bands of the ligament remain intact. A complete release is non-negotiable for surgical success.
4. Isolation of the Neurovascular Bundle
With the DTML completely transected, the neurovascular bundle is unroofed. Use tenotomy scissors to gently spread and free the bundle from the surrounding adventitial tissue, working from distal to proximal.
Differentiate the common digital nerve from the common digital artery. The artery typically crosses from proximal-medial to distal-lateral and lies dorsal to the nerve. If the artery is identified, meticulously dissect it away from the nerve and preserve it to maintain optimal digital perfusion.
Clinical Pearl: Structures commonly mistaken for the nerve include the lumbrical tendon (which passes medially to the base of the proximal phalanx) and the digital artery. The nerve will have a distinct pale, fascicular appearance compared to the muscular tendon or the pulsatile, tubular artery.
5. Neuroma Resection and Specimen Analysis
Trace the common digital nerve distally to identify its bifurcation into the two proper digital branches. The neuroma is typically located at this bifurcation, just distal to the DTML.
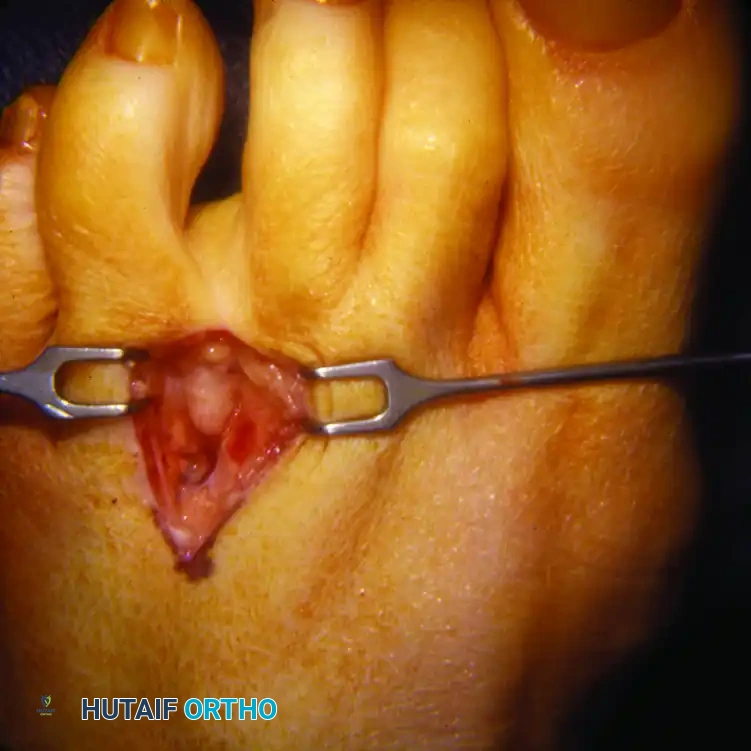
FIGURE 86-11: Excised common digital nerve demonstrating the classic bulbous neuroma at the junction of the two proper digital branches.
- Extend the dissection to the distal aspect of the neuroma. Transect the two proper digital branches distal to the fibrotic enlargement.
- Grasp the distal stump of the neuroma with a hemostat and apply gentle distal traction.
- Dissect the common digital nerve circumferentially, tracing it 3.0 to 3.5 cm proximally into the deep plantar arch.
- If the dissection reaches the adductor hallucis muscle, partially divide the muscle or retract it dorsally with a small right-angle retractor to maintain visualization.
- Identify and divide any small, plantar-directed articular or cutaneous branches tethering the nerve to the forefoot pad. This ensures the nerve can be mobilized and traced adequately proximal.
6. Proximal Stump Management
The management of the proximal nerve stump dictates the long-term success of the procedure. The goal is to allow the transected nerve end to retract into the deep, non-weight-bearing intrinsic musculature of the foot.
- Determine the exact point of transection. This must be 1 to 2 cm proximal to the weight-bearing pad of the forefoot.
- Verify this location by placing a blunt instrument at the proposed transection site and palpating it from the plantar aspect of the foot. If the instrument is palpable within the weight-bearing zone, the dissection must be carried further proximally.
- Once the non-weight-bearing zone is reached, sharply divide the nerve at its proximal resting place.
- Remove the excised specimen (the circumferentially dissected nerve and the neuroma) and send it to the pathology department for histological confirmation.
- Cauterize the proximal nerve stump using bipolar electrocautery to seal the epineurium and minimize axonal regeneration.
- Using a small hemostat, actively bury the cauterized stump well proximally and dorsally into the belly of the interosseous muscles. This prevents the stump from migrating plantarly and forming a painful recurrent neuroma in the weight-bearing area.
7. Hemostasis and Closure
- With the lamina spreader still in place, deflate the tourniquet.
- Observe the surgical field for 5 to 10 minutes during the period of reactive hyperemia. Identify and meticulously coagulate any transected arteries or larger vessels to prevent postoperative hematoma formation.
- Alternatively, the wound may be closed under tourniquet control, with the tourniquet released only after a compressive sterile dressing has been applied.
- Remove the lamina spreader.
- Irrigate the wound copiously with sterile saline.
- Close the skin loosely to accommodate postoperative swelling. Use a 4-0 non-absorbable monofilament suture (e.g., Nylon or Prolene) in a horizontal mattress fashion to gently evert the skin edges. Deep subcutaneous closure is generally unnecessary and may increase the risk of deep space infection or foreign body reaction.
POSTOPERATIVE REHABILITATION PROTOCOL
Optimal postoperative care is designed to minimize edema, prevent hematoma formation, and promote primary wound healing.
Phase 1: Immediate Postoperative (Weeks 0-2)
- Weight-Bearing: The patient is placed in a rigid, flat-bottomed postoperative shoe or a controlled ankle motion (CAM) boot. Heel-weight-bearing only is permitted. Strict avoidance of forefoot loading or toe-off mechanics is mandatory.
- Elevation: Strict elevation of the operative extremity above heart level is required for the first 48 to 72 hours to mitigate edema and throbbing pain.
- Wound Care: The bulky compressive dressing applied in the operating room remains intact and undisturbed until the first postoperative clinic visit.
Phase 2: Suture Removal and Transition (Weeks 2-4)
- Clinical Evaluation: Sutures are typically removed between 14 and 21 days postoperatively, contingent upon complete epithelialization of the incision.
- Footwear: Patients may transition to a wide, stiff-soled athletic shoe. A metatarsal pad may be utilized to splay the metatarsals and reduce pressure on the healing web space.
- Activity: Weight-bearing to tolerance is initiated. Patients are instructed to perform active and passive range of motion exercises of the MTP and interphalangeal joints to prevent capsular contracture and tendon adhesions.
Phase 3: Return to Full Activity (Weeks 4-8)
- Activity Progression: Gradual return to low-impact activities (e.g., stationary cycling, swimming). High-impact activities (running, jumping) are generally restricted until 6 to 8 weeks postoperatively.
- Expectation Management: Patients must be counseled that mild residual swelling and localized web space numbness (due to the resection of the proper digital nerves) are expected and permanent, though the numbness rarely causes functional impairment.
COMPLICATIONS AND PITFALLS
While dorsal excision of an interdigital neuroma is highly successful (with satisfaction rates exceeding 80-85%), complications can occur and must be managed aggressively.
1. Recurrent (Stump) Neuroma
The most dreaded complication is the formation of a symptomatic stump neuroma. This occurs when the nerve is transected too distally, allowing the regenerating nerve end to become tethered in the weight-bearing plantar fat pad or the residual stump of the DTML.
* Prevention: Meticulous proximal dissection (3.5 cm), complete release of the DTML, and burying the cauterized stump deep within the interosseous musculature.
* Treatment: Revision surgery via a plantar approach is often required to excise the stump neuroma and bury the nerve further proximally into the intrinsic foot musculature or even into the medullary canal of the metatarsal.
2. Hematoma Formation
The highly vascular nature of the intermetatarsal space predisposes the area to hematoma formation, which can lead to delayed wound healing, infection, or excessive fibrosis.
* Prevention: Meticulous hemostasis after tourniquet deflation, avoidance of dead space, and application of a robust compressive dressing.
3. Digital Ischemia
Simultaneous excision of adjacent neuromas (e.g., 2nd and 3rd web spaces) through a single or adjacent incisions carries a severe risk of compromising the vascular supply to the intervening digit, potentially leading to gangrene.
* Prevention: Never perform simultaneous adjacent web space neuroma excisions. If bilateral or adjacent neuromas are suspected, stage the procedures or utilize conservative measures for the less symptomatic web space.
4. Complex Regional Pain Syndrome (CRPS)
A rare but devastating complication characterized by disproportionate pain, allodynia, and autonomic dysfunction.
* Prevention: Gentle tissue handling, avoidance of excessive traction on the nerve during resection, and early postoperative mobilization.
* Treatment: Immediate referral to a pain management specialist for sympathetic blocks, gabapentinoids, and aggressive physical therapy.
CONCLUSION
The dorsal approach for interdigital neuroma excision remains the definitive surgical intervention for recalcitrant Morton's neuroma. By adhering to strict anatomical principles—specifically the complete release of the deep transverse metatarsal ligament and the meticulous proximal relocation of the nerve stump—the orthopedic surgeon can reliably eradicate the compressive neuropathy, restore forefoot mechanics, and achieve excellent long-term functional outcomes for the patient.
You Might Also Like


