Operative Management of Talar Fractures: A Comprehensive Surgical Guide

Key Takeaway
Talar fractures present complex challenges due to the tenuous retrograde blood supply of the talus, predisposing patients to osteonecrosis and post-traumatic arthritis. Successful management requires precise anatomical reduction, rigid internal fixation, and careful handling of soft tissues. This guide details the biomechanics, surgical indications, step-by-step operative approaches, and postoperative protocols for talar neck, body, and osteochondral fractures, ensuring optimal outcomes in both pediatric and adult populations.
INTRODUCTION TO TALAR FRACTURES
Fractures of the talus represent a formidable challenge in orthopedic traumatology. As the primary mechanical link between the leg and the foot, the talus is responsible for transmitting the entire weight of the body across the ankle and subtalar joints. Approximately 60% of the talar surface is covered by articular cartilage, leaving a limited vascular footprint. The absence of muscular or tendinous attachments means the talus relies entirely on a tenuous, retrograde extraosseous blood supply—primarily from the artery of the tarsal canal, the artery of the sinus tarsi, and superior neck vessels. Disruption of this vascular network during high-energy trauma frequently leads to osteonecrosis (avascular necrosis), malunion, and debilitating post-traumatic arthritis.
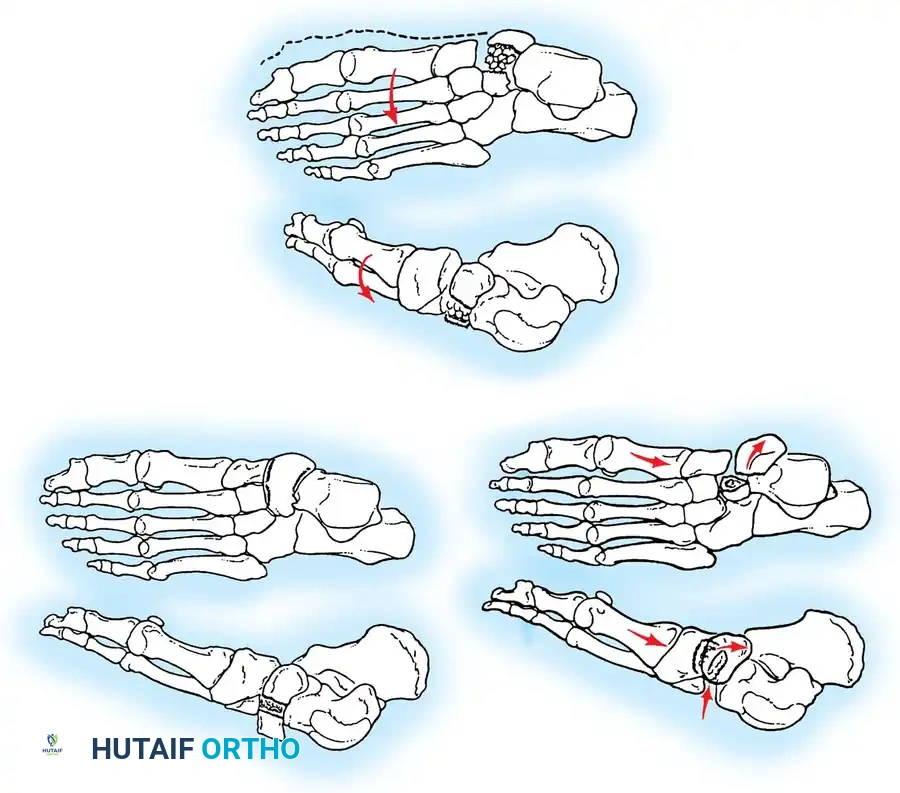
Talar fractures are broadly categorized into three basic anatomical types: (1) fractures of the neck, (2) fractures of the body and dome, and (3) fractures of the lateral, medial, or posterior processes.
TALAR NECK FRACTURES
Talar neck fractures are the most common type of talar fracture, typically resulting from high-energy hyperdorsiflexion injuries (the classic "aviator's astragalus"). The talar neck is driven against the anterior lip of the tibial plafond, leading to fracture and subsequent displacement of the talar body.
Radiographic Evaluation and Positioning
Accurate radiographic evaluation is paramount. Standard anteroposterior (AP), lateral, and mortise views of the ankle are required, but the Canale view is essential for evaluating the talar neck.
To obtain the Canale view, the foot is placed directly under the x-ray tube, and the ankle is placed in maximal equinus—the usual position after the reduction of a talar neck fracture. This position can be maintained more easily by maximal flexion of the hip and knee. The foot is pronated 15 degrees, and the x-ray tube is directed cephalad at a 75-degree angle from the horizontal tabletop. This specialized technique enables the surgeon to detect any subtle offset, comminution, or varus deformity of the head and neck of the talus.
Osteonecrosis and the Hawkins Sign
The most feared complication of talar neck fractures is osteonecrosis of the talar body. The risk correlates directly with the degree of displacement and dislocation (Hawkins Classification).
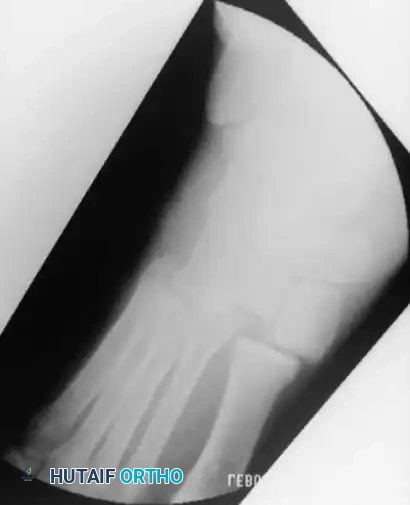
A critical prognostic indicator is the Hawkins sign—a subchondral radiolucency present in the talar dome 8 to 12 weeks after injury. This lucency represents subchondral osteopenia secondary to active hyperemia, indicating that the talar body remains vascularized.
Clinical Pearl: A positive Hawkins sign (subchondral lucency) at 12 weeks is a highly reliable indicator that osteonecrosis will not occur. Conversely, the lack of a subchondral lucency at 3 months strongly indicates that osteonecrosis has occurred.
Fig. 33-200 Hawkins line is not visible in sclerotic (latent osteonecrosis) talar dome 3 months after injury.
If standard radiographs are equivocal, bone scanning or Magnetic Resonance Imaging (MRI) may be utilized. Decreased uptake on a bone scan or altered signal intensity on MRI confirms the avascular state.
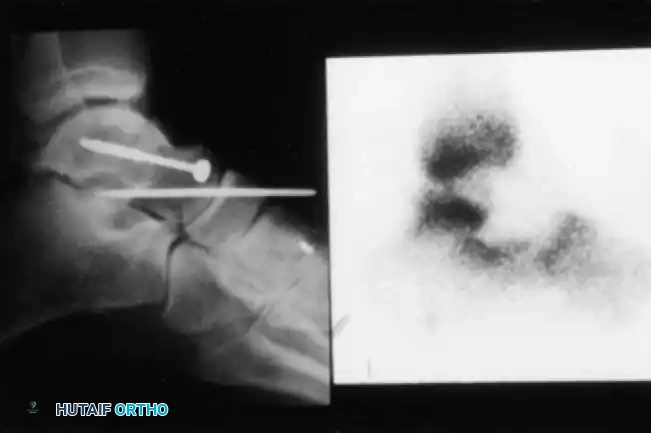
Fig. 33-201 Bone scan 8 days after open reduction of type IV talar neck fracture with talonavicular dislocation shows decreased uptake indicating area of osteonecrosis.
Pediatric Considerations in Talar Neck Fractures
Talar neck fractures in children behave differently than in adults. While osteonecrosis can still occur, the pediatric talus demonstrates a remarkable capacity for revascularization and remodeling. In our institutional evaluation of pediatric patients, those who developed osteonecrosis presented with a sclerotic lesion in the dome and body of the talus that subsequently became a cystic lesion on radiographs. Over a 2- to 3-year period, the area resolved, and the vast majority remained asymptomatic at long-term follow-up.
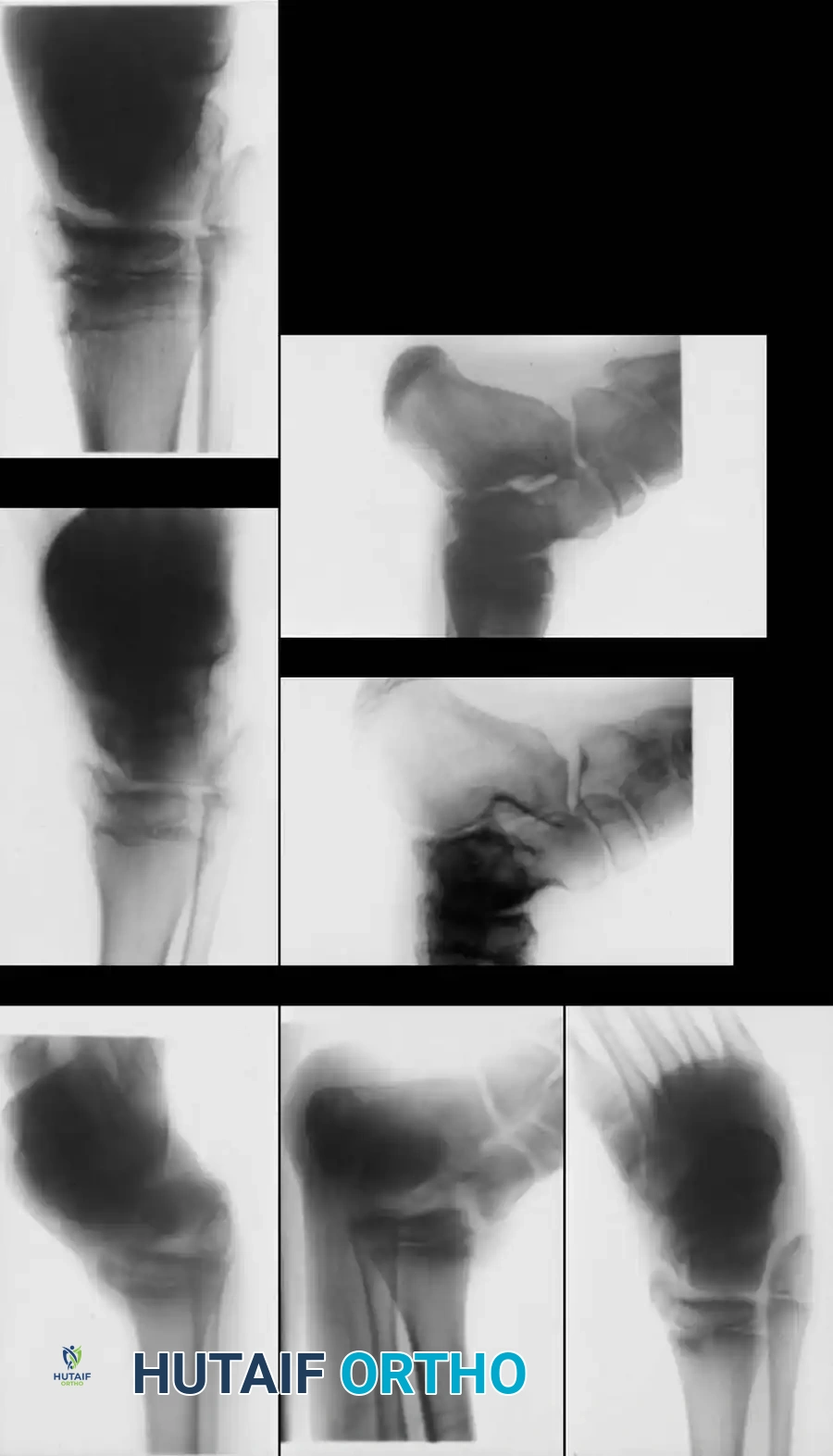
Fig. 33-202 A and B, Type III talar neck fracture with posteromedial displacement in 9-year-old child. C, After closed reduction and cast immobilization. D and E, At 9 months after injury, there is evidence of healing, but osteonecrosis of talus with sclerotic and cystic changes is evident. F and G, At 6 years after injury, physes are still open, and some healing of osteonecrosis of talus has occurred; patient has no symptoms.
Most children with osteonecrosis do not require surgery. A prolonged period of non–weight bearing or the use of a patellar tendon–bearing, weight-relieving brace should be strictly trialed before any surgical intervention is considered.

Pediatric talar healing progression demonstrating gradual resolution of cystic changes over time with conservative bracing.
Surgical Approaches and Fixation
For displaced talar neck fractures, open reduction and internal fixation (ORIF) is mandatory to restore articular congruity and prevent varus malunion.
Anteromedial Approach:
An anteromedial approach is frequently utilized. The incision is made medial to the tibialis anterior tendon, carefully retracting the neurovascular bundle laterally. This exposes the medial talar neck. Fixation is usually achieved with a cancellous lag screw directed from a medial to a lateral direction.
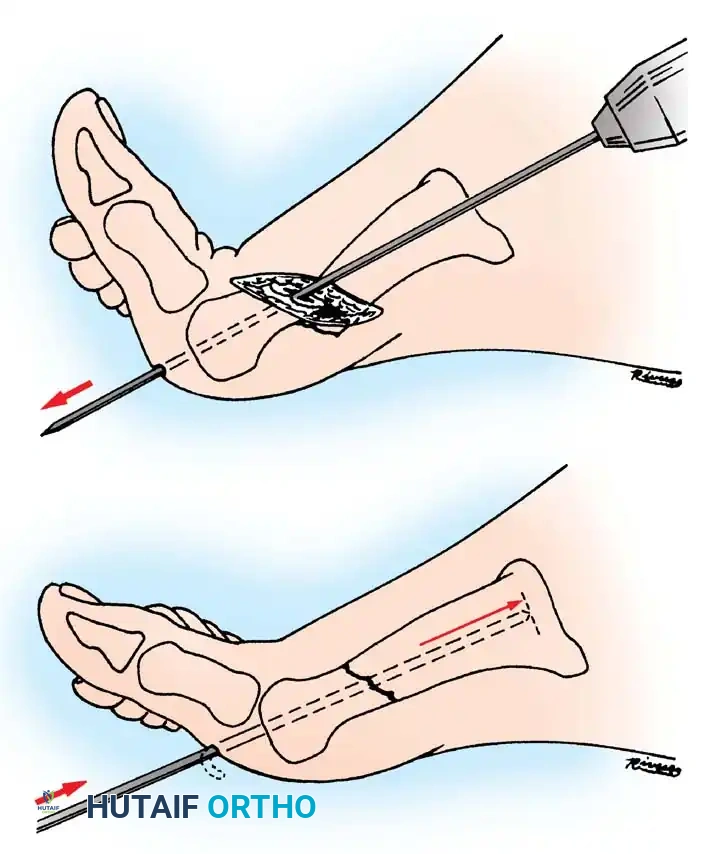
Posterior to Anterior Fixation:
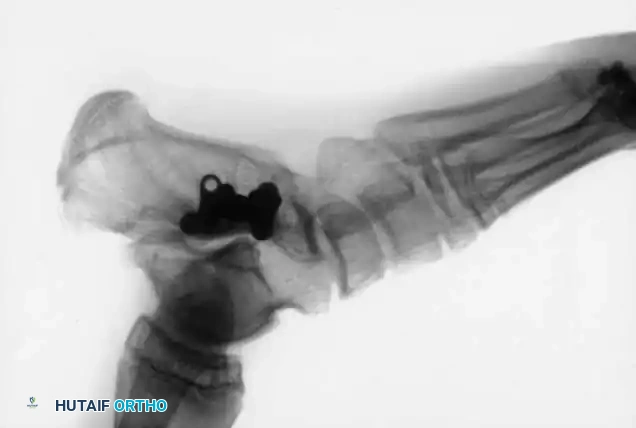
As a biomechanically superior alternative, a cancellous lag screw can be inserted percutaneously from posterior to anterior. This requires a posterolateral approach, taking extreme care to protect the sural nerve and the flexor hallucis longus (FHL) tendon. Posterior-to-anterior screws cross the fracture site perpendicular to the primary fracture plane, offering enhanced compression.

Radiographic example of robust internal fixation utilizing multiple cancellous screws to achieve rigid stability.
Complications: Malunion and Infection
Malunions of talar fractures are frequent in adults treated nonoperatively or with inadequate fixation. Malunion usually occurs with the distal fragment dorsiflexed or in a varus position, causing the fibula to rotate more anteriorly than normal. This forces the patient to bear an excessive amount of weight on the lateral side of the foot, rapidly leading to traumatic arthritis in the ankle and subtalar joints.
Infection is another devastating complication, particularly following open fractures. Because the talus is composed almost entirely of cancellous bone, and because a fracture through the neck seriously disrupts the blood supply, established osteomyelitis of the talus is highly resistant to treatment.
Surgical Warning: Repeated sequestrectomy or attempted excision and drainage of a sinus tract are generally contraindicated in established osteomyelitis of the talus. The results of talectomy without fusion have been historically poor.
The preferred treatment for fractures of the talus complicated by intractable infection is excision of the affected bone followed by arthrodesis (e.g., tibiocalcaneal fusion), even in children. Salvage operations for severe osteonecrosis, malunion, or infection include triple arthrodesis, ankle fusion, Blair fusion, and talocalcaneal fusion.
Salvage arthrodesis utilizing rigid internal fixation following failed talar fracture management and subsequent avascular collapse.
FRACTURES OF THE DOME AND LATERAL PROCESS
Fractures of the dome and body of the talus are rare in children but do occur in severe shearing injuries, such as those caused by lawn mowers, bicycle spokes, and "degloving" trauma. Severe, open shearing injuries require meticulous irrigation, aggressive débridement, and often excision of devitalized portions of the talus. The wound should be left open for delayed primary closure or skin grafting. The primary goal is to salvage as much length and function of the foot and ankle as possible.
Lateral Process Fractures ("Snowboarder's Fracture")
Fractures of the lateral process of the talus have seen a dramatic increase in incidence, particularly among snowboarders. The mechanism typically involves axial loading combined with dorsiflexion and eversion.
Because these fractures are notoriously difficult to visualize on standard plain radiographs, a high index of suspicion is required when a patient presents with persistent lateral subtalar pain mimicking a severe ankle sprain. A CT scan is often necessary to make a definitive diagnosis and assess articular comminution.
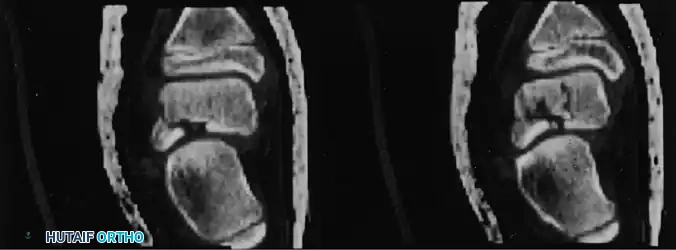
Fig. 33-203 Coronal CT reconstruction highlighting intraarticular nature of talar lateral process fracture. (From Leibner ED, Simanovsky N, Abu-Sneinah K, et al: Fractures of the lateral process of the talus in children. J Pediatr Orthop 10B:68, 2001.)
Management:
- Nondisplaced fragments: Can be treated successfully with closed cast immobilization.
- Large displaced fragments: Require open reduction and internal fixation to restore the subtalar joint surface.
- Small, comminuted displaced fragments: Should be excised primarily to prevent the development of painful subtalar arthritis.

Advanced CT imaging demonstrating the complex, multi-planar nature of talar body and process fractures requiring precise preoperative planning.
OSTEOCHONDRAL FRACTURES OF THE TALUS (OLT)
Osteochondral lesions of the talus (OLT), historically termed osteochondritis dissecans, present as localized lesions of articular cartilage and underlying subchondral bone. Symptoms frequently begin in the second decade of life, suggesting a lesion of adolescence progressing into early adulthood.
Classification and Morphology
The widely accepted classification system by Berndt and Harty categorizes these lesions into four stages based on radiographic appearance:
- Stage I: A small area of subchondral compression ("blister").
- Stage II: A partially detached osteochondral fragment.
- Stage III: A completely detached fragment remaining within the crater.
- Stage IV: A displaced fragment loose within the joint.
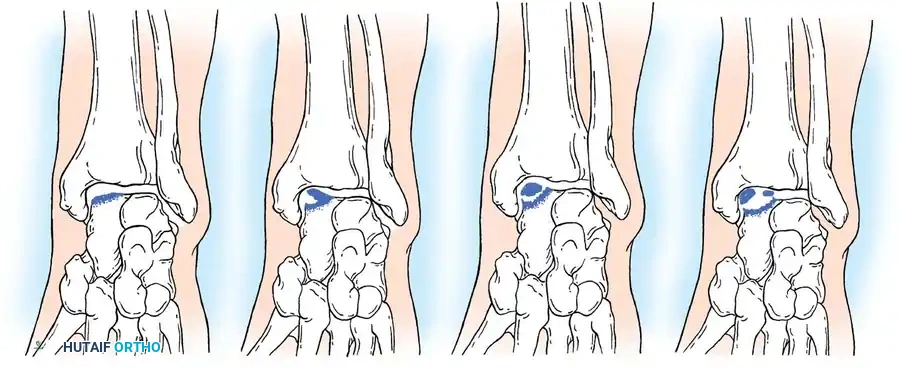
Fig. 33-204 Four types or stages of osteochondral fractures (osteochondritis dissecans of talus). Stage I, “blister”; stage II, elevated fragment but attached; stage III, fragment detached but still in crater; stage IV, displaced fragment.
Morphologically and etiologically, medial and lateral lesions differ significantly:
- Lateral Lesions: Almost exclusively caused by trauma. They are typically thin, wafer-shaped, and resemble acute osteochondral shear fractures. They are more prone to persistent symptoms and degenerative changes.
- Medial Lesions: While many are traumatic, a significant portion have no history of trauma (suggesting true osteochondritis dissecans or ischemic etiology). Medial lesions are typically deep and cup-shaped.
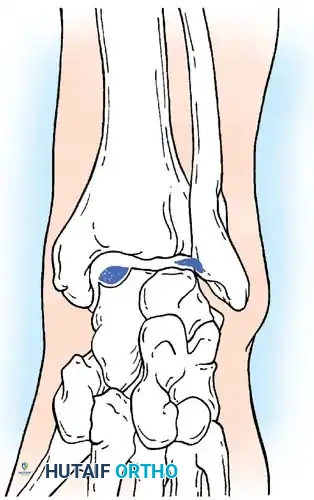
Fig. 33-205 Morphology of medial and lateral lesions. Lateral lesions are typically shallow and wafer-shaped, while medial lesions are deeper and cup-shaped.
Diagnostic Imaging and The "Inverted Fragment"
Standard radiographs often fail to accurately locate the lesion's anterior-to-posterior position. Computed Tomography (CT) in the coronal and axial planes is the gold standard for defining the exact location, size, and depth of the crater, which is critical for planning the surgical approach.
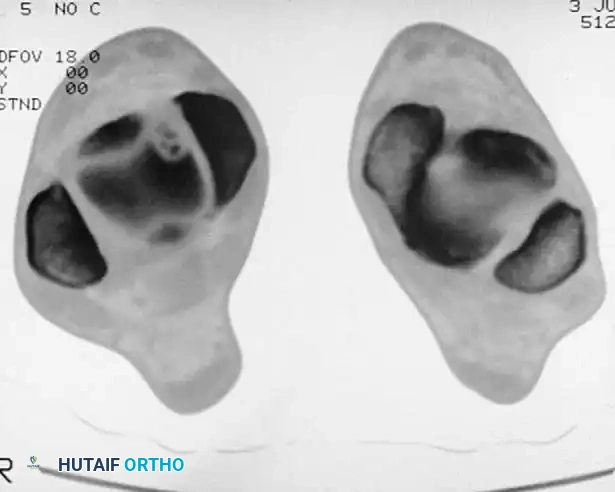
Fig. 33-207A Osteochondral lesion in anteromedial dome of talus. CT scan in axial plane shows crater and fragments.

Fig. 33-207B Coronal CT scan locates lesion whether anterior, middle, or posterior, which often is difficult to determine on radiograph.
High-resolution coronal CT demonstrating a deep medial osteochondral defect requiring surgical intervention.
Clinical Pearl - The "Floating" Fragment: If an osteochondral fragment appears on radiographs to be floating in its crater and riding high, with a flake of bone proximally that appears to be in the joint, the fragment is likely inverted in the crater. This means the subchondral bone is facing the joint space, and the cartilage is facing the bony crater. In this position, healing is impossible, and surgical excision is absolutely indicated.
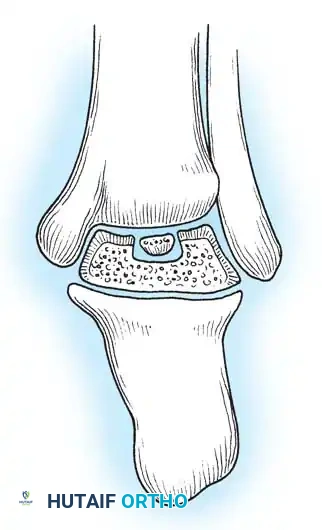
Fig. 33-206 “Floating” fragment in reality is loose fragment turned upside down in crater.
Treatment Protocols
Conservative Management:
Stage I and II lesions, as well as Stage III medial lesions (especially in children and adolescents), are initially treated nonoperatively. Immobilization in a cast for approximately 12 weeks, followed by patellar tendon–bearing braces or ankle corsets, yields favorable results.
Operative Management:
Surgery is recommended for Stage III lateral lesions (which have poor healing rates conservatively) and
Associated Surgical & Radiographic Imaging


You Might Also Like