Comprehensive Surgical Management of Bunionette (Tailor’s Bunion)

Key Takeaway
A bunionette, or Tailor’s bunion, is a painful bony prominence on the lateral aspect of the fifth metatarsal head. Often associated with splay foot or hallux valgus, it results from chronic pressure and mechanical overload. Conservative management includes shoe modifications and orthotics. When refractory, surgical intervention is indicated. Options range from partial lateral condylectomy for localized prominences to distal chevron or diaphyseal osteotomies for severe metatarsus quintus valgus, ensuring biomechanical restoration and symptom relief.
Pathoanatomy and Biomechanics of the Bunionette
The bony prominence on the lateral side of the fifth metatarsal head is classically referred to as a "tailor’s bunion." This nomenclature originates from the historical cross-legged sitting position of tailors, which forced the lateral border of the foot against the floor, leading to chronic mechanical overload and adventitial bursa formation.
In contemporary orthopedic practice, a bunionette is frequently observed as part of a broader forefoot pathology, most notably the splay foot deformity combined with hallux valgus. The etiology is multifactorial. The head of the fifth metatarsal may be congenitally or traumatically enlarged (Type I deformity). Alternatively, the diaphysis may be angulated laterally (Type II deformity), or there may be a widened fourth-fifth intermetatarsal angle (Type III deformity), making the fifth metatarsal head excessively prominent.
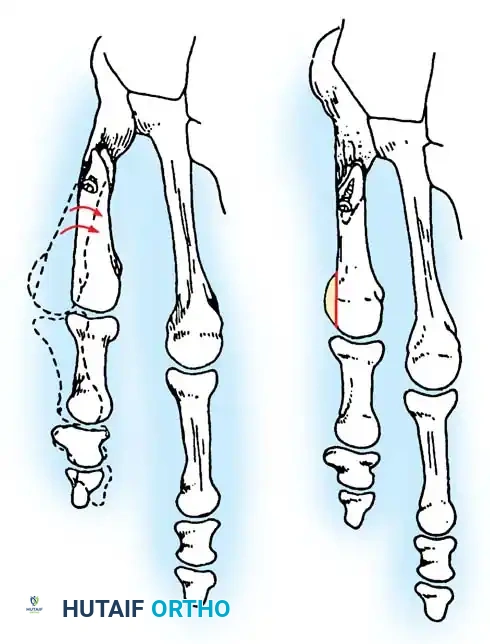
Fig. 80-30 A and B, Bunionette with metatarsus quintus valgus and fifth toe varus.

Fig. 80-31 Bunionette–hallux valgus–splay foot complex. Note lateral angulation of shaft of fifth metatarsal at distal third (arrows).
Constricting, narrow-toe-box footwear remains the primary extrinsic source of discomfort. Continuous pressure over this lateral bony prominence incites chronic irritation, leading to the development and subsequent hypertrophy of an adventitial bursa.

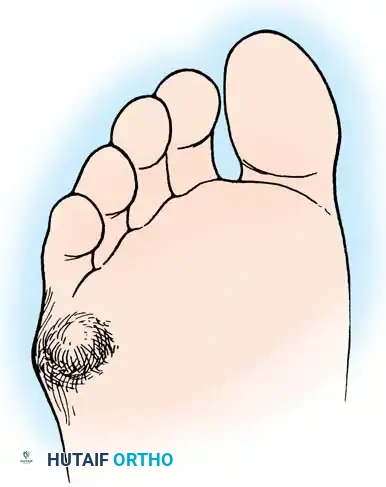
Fig. 80-32 Bunionette deformity with bursa formation.
If left untreated, ulceration may ensue. An intractable plantar keratosis (IPK) or lateral callus frequently develops over the prominent bunionette due to unyielding shoe pressure.
🚨 Clinical Warning: The Neuropathic Foot
In patients with diabetes mellitus, advanced Charcot-Marie-Tooth disease, or specific types of spinal dysraphism associated with poor sensibility, a neglected bunionette complication can be catastrophic. Ulceration and subsequent deep space infection can rapidly result in the loss of the entire fifth ray or even necessitate a major lower extremity amputation.
In addition to a symptomatic bursa over the lateral aspect of the prominent fifth metatarsal head, a diffuse callus or localized intractable keratosis can develop beneath the plantar aspect of the fifth metatarsal head, particularly if an extension deformity is present at the fifth metatarsophalangeal (MTP) joint.

General Surgical Diagram illustrating the lateral prominence and planned resection.
Conservative Management
Non-operative management is the first line of treatment and is highly effective in patients with flexible deformities or mild symptoms. Treatment modalities include:
* Footwear Modifications: Wide toe box shoes to eliminate lateral friction.
* Padding: Metatarsal pads or bars to offload the fifth ray.
* Orthotics: Semirigid shoe inserts featuring a relief (or “well”) beneath the plantar aspect of the condyle.
* Cushioning: Placement of 1/8- to 1/4-inch foam rubber between the bony prominence and the shoe.
Surgical Decision Making
If conservative treatment fails and surgical intervention becomes necessary, the procedure must be tailored to the specific pathoanatomy (Fallat and Buckholz classification). The primary surgical choices are:
1. Partial Resection: Excision of the lateral third of the fifth metatarsal head (Lateral Condylectomy).
2. Osteotomy: Distal, midshaft, or diaphyseal osteotomy of the fifth metatarsal to correct angular deformity.
3. Complete Resection: Resection of the fifth metatarsal head (salvage procedure, rarely indicated as a primary intervention).
Partial Resection of the Lateral Condyle of the Fifth Metatarsal Head
Partial resection of the lateral condyle of the fifth metatarsal head is historically the most commonly utilized procedure. It effectively relieves pressure symptoms and allows the patient a slightly greater variety of shoe wear. However, the cosmetic correction is not always pleasing, and patients must be counseled accordingly.
💡 Surgical Pearl: Managing Patient Expectations
The patient must be explicitly warned before surgery that only the painful bony prominence will be removed. The overall width of the forefoot will not be altered appreciably. If forefoot narrowing is the primary goal, an osteotomy is required.
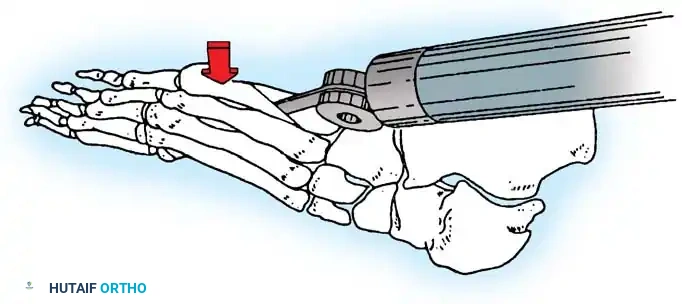
Causes of failure in lateral condylar resection include inadequate resection, MTP joint subluxation, and progressive forefoot splaying. Furthermore, if there is a painful callosity beneath the metatarsal head, the plantar aspect of the condyle must also be removed to prevent persistent plantar pain.
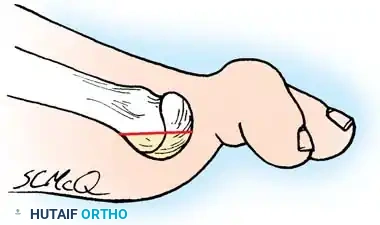
Fig. 80-35 Plantar aspect of fifth metatarsal head should be removed in addition to lateral flare if a plantar callus coexists.
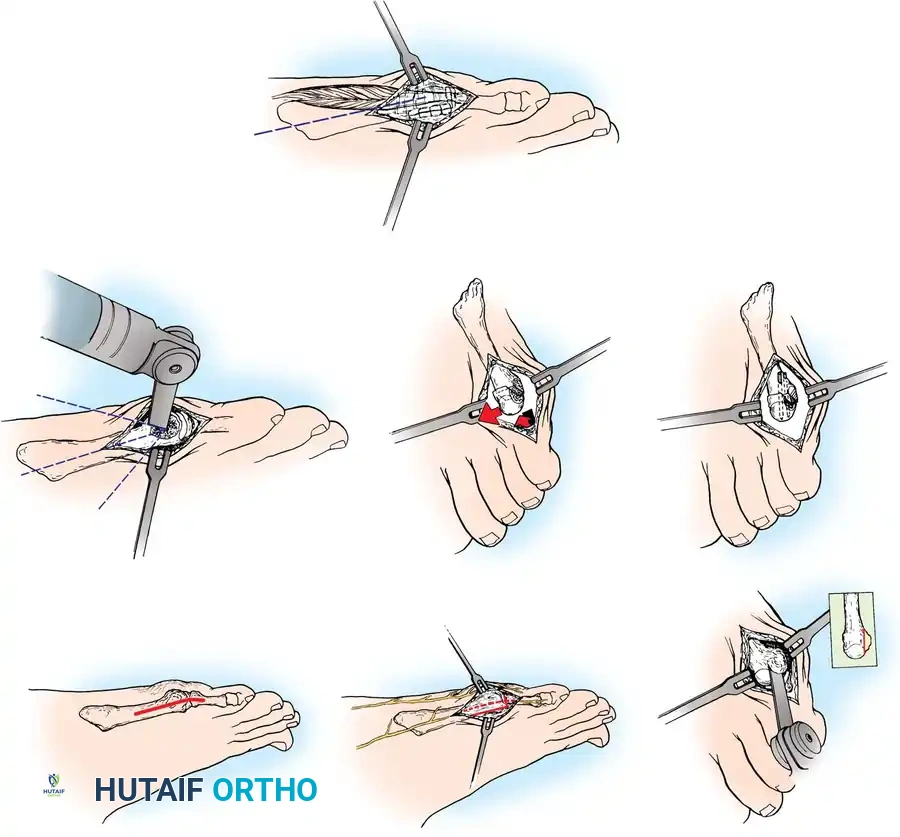
🔪 Surgical Technique 80-13: Bunionette Excision
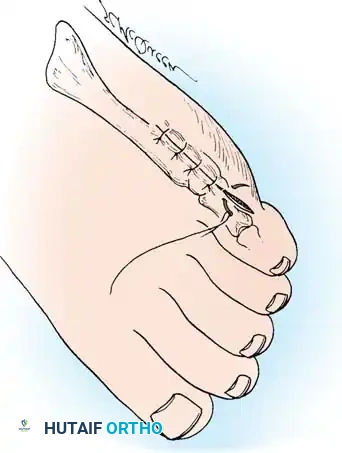
- Incision: Make a dorsolateral or straight lateral (preferred) incision extending from the junction of the middle and distal thirds of the fifth metatarsal shaft to the midshaft of the proximal phalanx. Incise only the skin initially.
- Nerve Protection: If the dorsolateral incision is used, meticulously identify and protect the dorsolateral cutaneous branch of the sural nerve. The straight lateral incision should pass safely between this nerve dorsally and the proper digital branch of the lateral plantar nerve to the fifth toe plantarward.

Fig. 80-36A Skin incision.
- Capsular Exposure: The tendon of insertion of the abductor digiti minimi passes just plantar to the midline of the lateral aspect of the fifth metatarsal head. Make the periosteal and capsular incision in a straight line 2 or 3 mm dorsal to the midline to preserve this tendon.
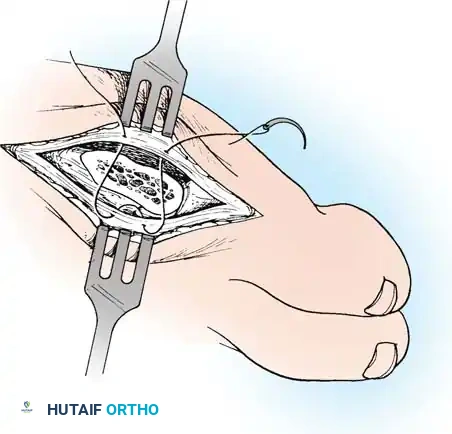
- Joint Delivery: By sharp dissection, elevate the capsule dorsally and plantarward until the fifth metatarsal head can be made visible by delivering it laterally as the phalanx is pushed medially.
⚠️ Surgical Pitfall: Over-resection
More metatarsal head can be removed than is intended if the medial edge of the articular cartilage is not adequately exposed. Approximately 35% to 40% of the metatarsal head is usually removed to excise the bony prominence. A thin osteotome or a small blade on a power saw is mandatory to prevent iatrogenic fracture or excessive bone loss.
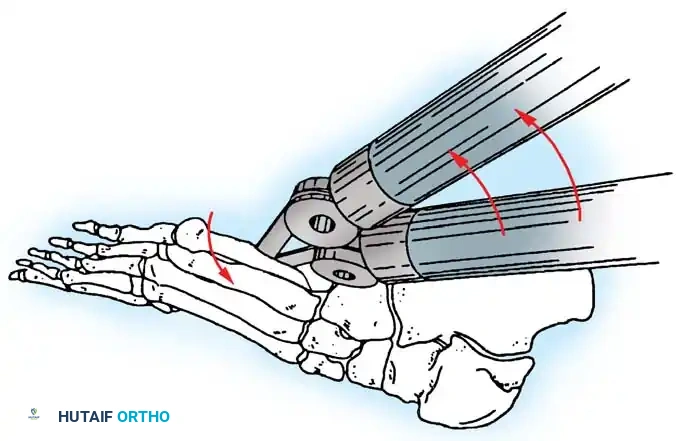
- Osteotomy Cut: Score the proximal margin of the proposed osteotomy, and direct the cut in a dorsal distal–to–plantar proximal direction.


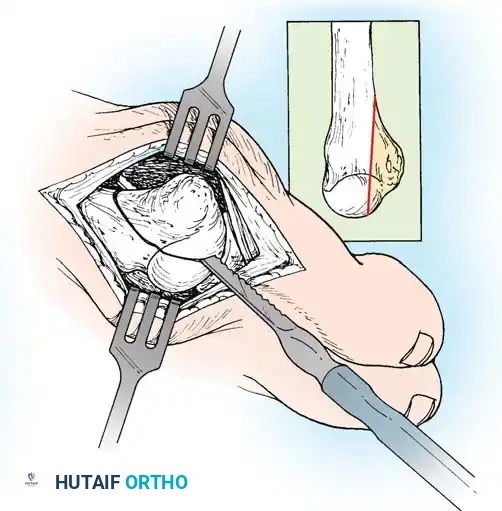
Fig. 80-36B Excision of lateral prominence of fifth metatarsal head to include 40% of articular surface.
- Phalangeal Contouring: Reduce the phalanx over the remaining part of the fifth metatarsal head, and palpate the lateral flare of the base of the phalanx. If this produces a projecting bony prominence that may cause symptoms, excise the prominence with a rongeur or bone-biter.
- Plantar Condylectomy: Before closing the capsule, round off the bone edges with a rasp. If a plantar callus coexists beneath the metatarsal head,
Associated Surgical & Radiographic Imaging




You Might Also Like

