Operative Management of Sesamoid Pathology: Bone Grafting and Reconstruction
Key Takeaway
Sesamoid nonunion often results from chronic repetitive microtrauma or acute fracture with compromised vascularity. When conservative measures fail, surgical intervention is indicated. If the articular surface remains intact, extraarticular autogenous bone grafting—utilizing local graft from the first metatarsal—is the gold standard. This technique preserves the sesamoid apparatus, maintaining first ray biomechanics while avoiding the complications associated with sesamoidectomy, such as iatrogenic hallux valgus or varus deformities.
INTRODUCTION TO HALLUCAL SESAMOID PATHOLOGY
The hallucal sesamoids play an indispensable biomechanical role in the function of the first ray. Embedded within the tendinous insertions of the flexor hallucis brevis (FHB) muscle, the tibial (medial) and fibular (lateral) sesamoids absorb weight-bearing forces, reduce friction, and protect the flexor hallucis longus (FHL) tendon. Furthermore, they act as a fulcrum, increasing the mechanical advantage of the intrinsic musculature of the first metatarsophalangeal (MTP) joint.
Because the tibial sesamoid bears a significantly higher proportion of the load during the terminal stance phase of gait, it is disproportionately susceptible to acute fractures, chronic stress fractures, and subsequent nonunion. The vascular anatomy of the sesamoids—often characterized by a tenuous blood supply entering from the proximal and distal poles—creates a central watershed zone. This anatomic vulnerability predisposes the sesamoids to delayed union, nonunion, and osteochondritis (avascular necrosis).
When conservative management of a sesamoid nonunion fails, surgical intervention is warranted. While sesamoidectomy has historically been utilized, it carries significant risks of iatrogenic deformity (hallux valgus if the medial sesamoid is excised; hallux varus if the lateral is excised) and decreased push-off strength. Therefore, in cases where the articular cartilage remains viable, autogenous bone grafting of the sesamoid nonunion is the preferred, joint-preserving alternative.
BONE GRAFTING OF SESAMOID NONUNION
The decision to proceed with bone grafting versus excision hinges entirely on the integrity of the sesamoid-metatarsal articulation. The technique popularized by Anderson and McBryde provides a systematic approach to evaluating the joint and performing an extraarticular bone graft, thereby preserving the critical gliding mechanism of the first MTP joint.
Indications and Preoperative Evaluation
Surgical intervention is indicated for patients with symptomatic sesamoid nonunion who have failed a minimum of 3 to 6 months of rigorous conservative management (e.g., offloading orthotics, dancer’s pads, rigid carbon fiber plates, and immobilization).
Preoperative imaging must include:
* Weight-bearing radiographs: Anteroposterior, lateral, and axial sesamoid views to assess alignment and joint space.
* Computed Tomography (CT): The gold standard for evaluating the extent of the nonunion, cystic changes, and sclerosis.
* Magnetic Resonance Imaging (MRI): Useful for assessing the viability of the bone (avascular necrosis) and the integrity of the surrounding soft tissues, including the plantar plate and FHB tendon.
Clinical Pearl: Differentiating a bipartite sesamoid from a true nonunion is critical. A bipartite sesamoid typically features smooth, well-corticated margins, and the combined size of the fragments is larger than a normal sesamoid. A nonunion or fracture will exhibit irregular, jagged edges, and the fragments will fit together to form a normal-sized sesamoid.
🔪 Surgical Technique: The Anderson and McBryde Approach
1. Patient Positioning and Anesthesia
The patient is placed in the supine position on the operating table. A regional ankle block or general anesthesia may be utilized, depending on patient and surgeon preference. A calf or thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for the meticulous identification of neurovascular structures.
2. Surgical Incision and Superficial Dissection
- Make a 5-cm longitudinal skin incision along the medial plantar aspect of the first ray. The incision should be perfectly centered over the first MTP joint.
- Carefully deepen the incision through the subcutaneous tissues.
- Identify the medial capsule of the first MTP joint and the abductor hallucis tendon.
- Divide the deep fascia in line with the skin incision.
3. Joint Inspection and Decision Matrix
- Enter the first MTP joint via a capsulotomy placed dorsal to the tibial hallucal sesamoid.
- Use a small Ragnell or Senn retractor to expose the articular surface of the sesamoid and the corresponding plantar facet of the first metatarsal head.
- Decision Point: Inspect the chondral surfaces meticulously.
- If severe cartilaginous destruction, advanced osteoarthritis, or gross fragmentation is present: Bone grafting is contraindicated. Proceed with a partial or complete sesamoidectomy, ensuring meticulous repair of the FHB defect to prevent hallux valgus.
- If the articular surface is intact (as is usually the case in isolated nonunions): Proceed with joint-preserving bone grafting via an extraarticular approach.
4. Extraarticular Exposure of the Nonunion
- Returning to the primary incision, direct the dissection plantar to the abductor hallucis tendon to achieve extraarticular exposure of the plantar aspect of the tibial sesamoid.
Surgical Warning: The medial plantar digital nerve courses in close proximity to the plantar-medial aspect of the tibial sesamoid. Meticulous blunt dissection and gentle retraction are mandatory to avoid iatrogenic neurapraxia or the formation of a painful postoperative neuroma.
- Perform sharp periosteal elevation over the plantar surface of the sesamoid.
- Identify the nonunion site, which is typically located within the midportion (transverse watershed zone) of the sesamoid. Gross motion or fibrous instability at the nonunion site is often visually apparent upon probing.
5. Preparation of the Nonunion Site
- Using a small dental curet or a 2.0-mm burr, meticulously debride all interposed fibrous tissue, sclerotic bone, and necrotic debris from the nonunion interface.
- Crucial Step: The curettage must be strictly confined to the extraarticular portion of the bone. Do not penetrate the dorsal cortex of the sesamoid, as this will disrupt the intact articular cartilage and precipitate postoperative osteoarthritis.
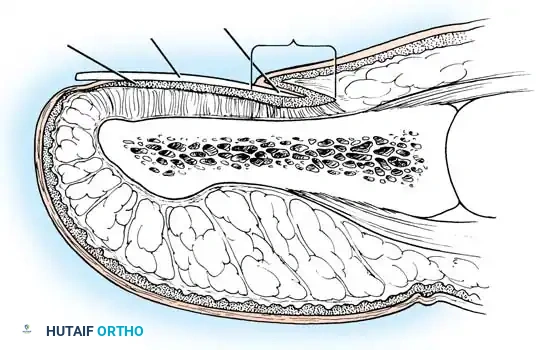
- Continue debridement until healthy, bleeding cancellous bone is encountered on both the proximal and distal fragments (the "paprika sign").
6. Bone Graft Harvesting and Placement
- Autogenous cancellous bone graft is required to stimulate osteogenesis. This can be conveniently harvested locally from the first metatarsal.
- Create a small cortical window in the medial eminence of the first metatarsal head (proximal to the articular cartilage).
- Use a small curet to harvest highly osteogenic cancellous bone.
- Firmly pack the harvested autogenous bone graft into the prepared defect of the sesamoid nonunion.
- Note on Fixation: Internal fixation (e.g., micro-screws) is rarely required and often technically prohibitive due to the small size of the fragments. The robust tendinous expansion of the FHB that envelops the sesamoid acts as a dynamic tension band, keeping the proximal and distal fragments in excellent apposition once the defect is grafted.
7. Closure
- Approximate the periosteal layers and the capsule using a 2-0 or 3-0 absorbable suture (e.g., Vicryl).
- Close the subcutaneous tissue and skin in a standard layered fashion.
- Apply a sterile, compressive dressing.
Postoperative Rehabilitation Protocol
Successful union relies as much on strict postoperative compliance as it does on surgical execution. The FHB complex must be protected from tensile loads while the graft incorporates.
- Phase 1 (Weeks 0 to 3-4): The patient is placed immediately into a short-leg plaster splint or a rigid cast, rendering the entire hallux completely immobile. The patient must remain strictly non-weight-bearing (NWB).
- Phase 2 (Weeks 4 to 8): The patient is transitioned to a short-leg walking cast or a rigid controlled ankle motion (CAM) boot. The hallux remains immobilized to prevent dorsiflexion, but progressive weight-bearing is permitted as tolerated.
- Phase 3 (Week 8 and Beyond): The cast/boot is removed. Clinical and radiographic evaluation is performed to confirm graft incorporation.
- Orthotic Management: A soft medial longitudinal arch support, combined with a dancer's pad to offload the first ray, is prescribed. The patient must use a firm-soled shoe or a shoe with a Morton's extension to limit MTP joint dorsiflexion.
- Physical Therapy: Active range of motion (ROM) exercises are initiated. Gentle passive ROM is introduced gradually, strictly guided by patient tolerance and the absence of inflammatory symptoms.
OSTEOCHONDRITIS OF THE SESAMOID
Osteochondritis of the sesamoid (often referred to as avascular necrosis, or Renander's disease when occurring in adolescents) is a distinct pathologic entity characterized by ischemic necrosis, structural collapse, and fragmentation of the sesamoid bone.
Pathogenesis and Diagnosis
While the exact etiology remains idiopathic in many cases, chronic repetitive microtrauma is widely considered the primary precipitating factor. The tenuous vascular supply to the sesamoid is compromised by repetitive loading, leading to microfractures, ischemia, and eventual osteonecrosis.
Clinically, patients present with insidious onset of localized pain beneath the first MTP joint, exacerbated by weight-bearing and terminal toe-off.
Radiographic evaluation is paramount:
* Axial Radiographs: May reveal a deformed, flattened sesamoid with irregular areas of increased sclerosis (bone density) intermixed with radiolucent cystic changes, modeling a fragmented appearance.
* CT Scan: Provides superior resolution of the trabecular architecture, confirming fragmentation and subchondral collapse.
* MRI: Highly sensitive in the early stages. T1-weighted images will show decreased signal intensity (edema/necrosis), while T2-weighted images may show bone marrow edema before radiographic changes become apparent.
Management Strategy
As with all sesamoid disorders, a highly conservative approach is mandatory before considering surgical extirpation.
- Conservative Treatment: The primary goal is mechanical offloading. This is achieved using a dancer’s pad (a U-shaped pad that floats the first metatarsal head) combined with a full-length rigid carbon fiber plate inserted into the shoe. This construct prevents dorsiflexion of the MTP joint and eliminates the windlass mechanism's compressive forces on the sesamoids. NSAIDs and localized icing are used adjunctively.
- Surgical Treatment: If 6 months of aggressive conservative management fails, and the patient experiences intractable pain, a partial or complete sesamoidectomy is recommended. Because osteochondritis destroys the structural integrity and articular surface of the bone, bone grafting is generally not a viable option for this specific pathology.
OTHER CONDITIONS OF THE SESAMOID
The differential diagnosis for plantar first MTP joint pain is broad. Several other conditions can afflict the sesamoid apparatus, requiring careful clinical differentiation.
Sesamoiditis
"Sesamoiditis" is a poorly understood and fairly vague diagnosis, often used as a catch-all term for perisesamoid inflammation without radiographic evidence of fracture, nonunion, or osteonecrosis. It is essentially a localized tendinosis or periostitis of the FHB complex.
* Treatment: Surgical treatment should be strictly delayed until all conservative measures (activity modification, taping, orthotics, NSAIDs, and potentially a single corticosteroid injection) have been completely exhausted. Surgery is rarely indicated for pure sesamoiditis.
Sesamoid Osteoarthritis
Primary or post-traumatic arthritis can affect the sesamoid-metatarsal articulation. Patients present with grinding, crepitus, and pain during MTP dorsiflexion. If conservative offloading fails, surgical excision of the arthritic sesamoid is the definitive treatment.
Intractable Plantar Keratoses (IPK)
A hypertrophic, plantarflexed first metatarsal or an enlarged sesamoid can create a focal pressure point, leading to a painful, intractable plantar keratosis (callus) directly beneath the sesamoid.
* Treatment: Initial management involves routine paring of the callus and offloading orthotics. If recalcitrant, surgical intervention may involve a plantar condylectomy (shaving the prominent plantar half of the sesamoid) rather than a complete excision, thereby preserving the FHB insertion and joint mechanics.
Nerve Impingement
The medial plantar digital nerve is intimately associated with the tibial sesamoid. Perineural fibrosis, often secondary to prior trauma, sesamoid fracture, or chronic inflammation, can lead to nerve impingement. Patients will present with radiating neuropathic pain, tingling, or numbness along the medial aspect of the hallux. Diagnostic injections can help isolate the nerve as the pain generator. Surgical neurolysis or neurectomy is reserved for refractory cases.
Summary: The hallucal sesamoids are small but biomechanically critical structures. A deep understanding of their anatomy, vascularity, and function is required to manage their pathologies. When surgery is indicated for nonunion, the Anderson and McBryde extraarticular bone grafting technique offers a highly effective, joint-preserving solution that restores function while mitigating the risks of complex first ray deformities.
📚 Medical References
- sesamoid nonunions, Foot Ankle Int 18:293, 1997.
- Aper RL, Saltzman CL, Brown TD: The effect of hallux sesamoid resection on the effective moment of the fl exor hallucis brevis, Foot Ankle 15:462, 1994.
- Aper RL, Saltzman CL, Brown TD: The effect of hallux sesamoid excision on the fl exor hallucis longus moment arm, Clin Orthop Relat Res 325:209, 1996.
- Brown TIS: Avulsion fractures of the fi bular sesamoid in association with dorsal dislocation of the metatarsophalangeal joint of the hallux: report of a case and review of the literature, Clin Orthop Relat Res 149:229, 1980.
- Burman MS, Lapidus PW: The functional disturbances caused by the inconstant bones and sesamoids of the foot, Arch Surg 22:936, 1931.
- Chisin R, Peyser A, Milgrom C: Bone scintigraphy in the assessment of the hallucal sesamoids, Foot Ankle Int 16:291, 1995.
- deBritto SR: The fi rst metatarso-sesamoid joint, Int Orthop 6:61, 1982.
- Fleischli J, Cheleuitte E: Avascular necrosis of the hallucal sesamoids, J Foot Ankle Surg 34:358, 1995.
- Glass B: Fractured fi bular sesamoid: a case report, J Foot Surg 19:19, 1980.
- Helal B: Surgery of the forefoot, Br J Med 1:276, 1977.
- Helal B: The great toe sesamoid bones: the lux or lost souls of Ushia, Clin Orthop Relat Res 157:82, 1981.
- Hussain A: Dislocation of the fi rst metatarsophalangeal joint with fracture of fi bular sesamoid, Clin Orthop Relat Res 359:209, 1999.
- Inge GAL, Ferguson AB: Surgery of the sesamoid bones of the great toe: an anatomical and clinical study with a report of 41 cases, Arch Surg 27:466, 1933.
- Irwin AS, Maffulli N, Wardlaw D: Traumatic dislocation of the lateral sesamoid of the great toe: nonoperative management, J Orthop Trauma 180:2, 1995.
- Jahss MH: The sesamoids of the hallux, Clin Orthop Relat Res 157:88, 1981.
- Kaiman ME, Piccona R: Tibial sesamoidectomy: a review of the literature and retrospective study, J Foot Surg 22:286, 1983.
- Morris JM: Biomechanics of the foot and ankle, Clin Orthop Relat Res 122:10, 1977.
- Nuber GW, Anderson PR: Acute osteomyelitis of the metatarsal sesamoid, Clin Orthop Relat Res 167:212, 1982.
- Richardson EG: Hallucal sesamoid pain: causes and surgical treatment, J Am Acad Orthop Surg 7:270, 1999.
- Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals, Foot Ankle Int 24:415, 2003.
- Van Hal ME, Keene JS, Lange TA, et al: Stress fractures of the great toe sesamoids, Am J Sports Med 10:122, 1982.
- Weiss JS: Fracture of the medial sesamoid bone of the great toe: controversies in therapy, Orthopedics 14:1003, 1991.
- Zinman H, Keret D, Reis ND: Fracture of the medial sesamoid bone of the hallux, J Trauma 21:581, 1981.
- Vol. I: pages 1-1060; Vol. II: pages 1061-2350; Vol. III: pages 2351-3632; Vol. IV: pages 3633-4900
You Might Also Like