Open Finger Syndactyly Release and Dorsal Flap Reconstruction
Key Takeaway
Syndactyly release is a foundational pediatric hand surgery procedure aimed at restoring independent digital function and preventing angular deformities. This guide details two primary approaches: the open finger technique by Withey et al., which utilizes secondary intention healing to avoid skin grafts, and the classic dorsal rectangular flap technique by Bauer et al., which relies on interdigitating flaps and full-thickness skin grafting to reconstruct the commissure and digital borders.
Introduction to Syndactyly and Web Space Reconstruction
Syndactyly is one of the most common congenital hand anomalies, occurring in approximately 1 in 2,000 to 3,000 live births. It results from a failure of apoptosis (programmed cell death) within the interdigital necrotic zone during the sixth to eighth weeks of embryonic development. The condition can manifest as an isolated anomaly or as part of a broader syndromic presentation (e.g., Apert syndrome, Poland syndrome).
The primary goal of syndactyly release is to establish independent digital motion, optimize prehension, and prevent progressive angular deformities that occur when adjacent digits of unequal length are tethered together. Reconstructing a functional and aesthetically acceptable web space is a technically demanding endeavor that requires a profound understanding of local flap geometry, digital vascular arborization, and the biomechanics of the normal commissure.
This comprehensive guide details two highly effective, evidence-based surgical approaches for syndactyly release: the Open Finger Syndactyly Release (as described by Withey et al.) and the Syndactyly Release with Dorsal Flap (as described by Bauer et al.).
Preoperative Assessment and Surgical Timing
Clinical and Radiographic Evaluation
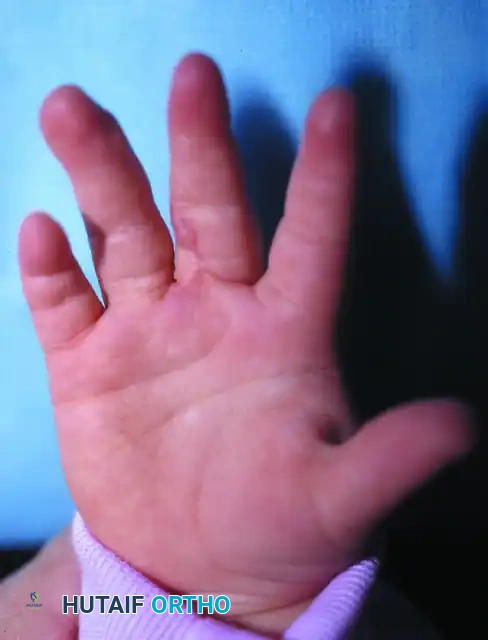
A meticulous preoperative clinical examination is mandatory. The surgeon must assess the extent of the webbing (complete vs. incomplete) and the involvement of underlying osseous structures (simple vs. complex).
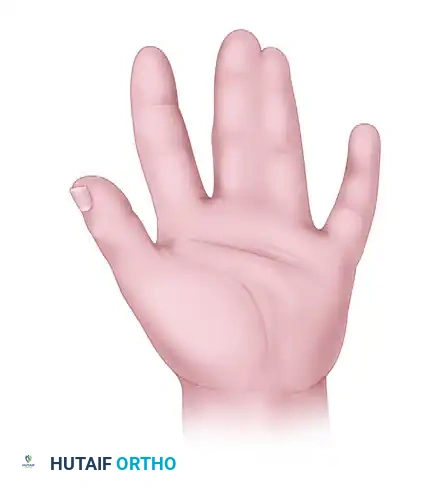
Clinical photograph demonstrating a complete simple syndactyly prior to surgical intervention. Note the tight tethering extending to the distal phalanges.
Standard posteroanterior and lateral radiographs of the hand are required to identify bony fusions, delta phalanges, or symphalangism. In complex or syndromic cases, preoperative Doppler ultrasonography or magnetic resonance angiography (MRA) may be indicated to map the digital vascular anatomy, as anomalous bifurcations of the common digital arteries are frequent.
Timing of Surgical Intervention
The timing of syndactyly release is dictated by the specific digits involved:
* Border Digits (Thumb-Index and Ring-Small): Release is typically performed early, between 6 to 12 months of age. The significant length discrepancy between these digits causes rapid angular deformity and joint contracture if left tethered.
* Central Digits (Index-Long and Long-Ring): Release is generally deferred until 12 to 18 months of age. Delaying the procedure allows for increased digital size, which facilitates easier flap dissection and reduces the anesthetic risk, without compromising functional outcomes.
💡 Surgical Warning: The Bilateral Release Rule
Never release both sides of a single digit during the same surgical setting. Simultaneous bilateral release severely compromises the vascular supply to the digit, carrying an unacceptably high risk of catastrophic digital ischemia and necrosis. If a patient has multiple adjacent syndactylies (e.g., index-long-ring), the releases must be staged at least 3 to 6 months apart.
Surgical Anatomy and Biomechanics of the Web Space
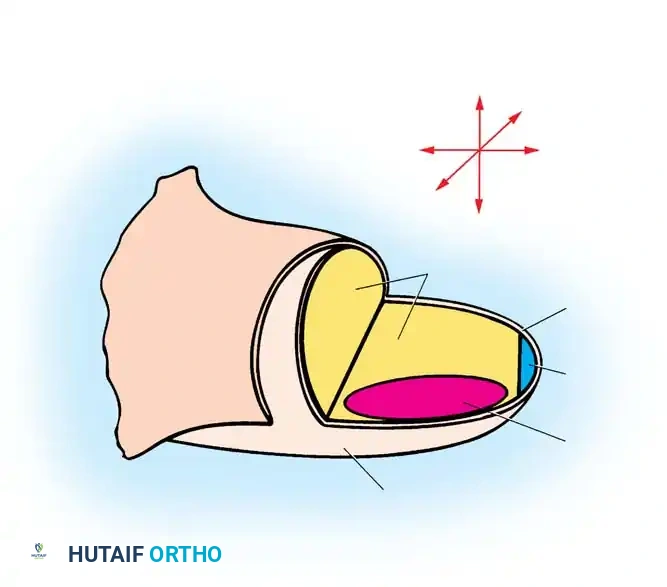
A normal digital web space is not a simple V-shaped cleft; it is a complex, three-dimensional structure. It slopes proximally from dorsal to palmar, creating a dorsal skin fold that extends further distally than the palmar skin crease. The normal web space is composed of supple, hairless skin that allows for wide digital abduction and independent flexion.
When separating webbed fingers, the total surface area of the newly separated digits is significantly greater than the surface area of the conjoined digits. Historically, this absolute skin deficiency necessitated the use of skin grafts in almost all cases. The surgical techniques detailed below represent two distinct philosophies in managing this skin deficit: secondary intention healing (Withey) and full-thickness skin grafting (Bauer).
Technique 1: Open Finger Syndactyly Release (Withey et al.)
Withey et al. introduced a paradigm-shifting "open" technique that challenges the traditional reliance on skin grafting. By comparing patients treated with the open technique against those treated with standard closed grafting, they demonstrated that the open technique yielded significantly better scar quality and reduced rates of web contracture.
The core principle of this technique is the use of numerous, narrow, non-defatted flaps that are allowed to heal partially by secondary intention, thereby eliminating the donor site morbidity associated with skin grafting.
Step-by-Step Surgical Execution
- Flap Design and Marking:
- Begin by designing a proximally based rectangular dorsal flap to re-create the web space commissure.
- Design seven or eight narrow, interdigitating triangular flaps along the palmar and dorsal aspects of the conjoined digits. The sheer number of flaps ensures that each flap has a narrow base, which is critical for the open technique's success.
- Incision and Flap Elevation:
- Incise the skin markings sharply.
- Raise each triangular flap to the midaxial line of the respective digit.
- Preservation of Subcutaneous Fat:
- Crucial Step: Do not defat the digital flaps. Unlike traditional techniques where defatting is standard to create a deep web, retaining the subcutaneous fat in the open technique is vital to preserving the delicate subdermal vascular plexus, thereby preventing flap tip necrosis.
- Flap Inset and Suturing:
- Tack the flaps into their respective recipient beds using a single apical stitch (typically a fine absorbable suture such as 5-0 or 6-0 chromic gut or Vicryl Rapide).
- Deliberately leave the raw, uncovered areas between the flaps to heal by secondary intention. The narrow design of the flaps ensures that these raw areas are small and linear.
- Commissure Resurfacing (If Required):
- While the goal is to avoid grafting, if the defect at the base of the commissure is excessively large and cannot be adequately covered by the dorsal rectangular flap, a small split-thickness skin graft (STSG) may be utilized strictly at the web base.
- Dressing Application:
- Apply a non-adherent dressing (e.g., Xeroform) over the open areas, followed by a bulky, soft, absorptive dressing to protect the digits and absorb exudate during the secondary healing phase.
🔪 Clinical Pearl: Secondary Intention Healing
The success of the Withey open technique relies on the biological principle that small, narrow, longitudinally oriented defects on the digits will epithelialize rapidly with minimal contractile scarring, provided the surrounding flaps are well-vascularized and not under tension.
Technique 2: Syndactyly Release with Dorsal Flap (Bauer et al.)
The Bauer technique remains the gold standard and workhorse procedure for syndactyly release worldwide. It utilizes a robust, proximally based dorsal rectangular flap to reconstruct the web space slope, combined with palmar and dorsal interdigitating zig-zag flaps to break up the linear scar and prevent flexion contractures. Because this technique aims for primary closure of the web, it inherently requires full-thickness skin grafting to cover the remaining lateral digital defects.
Step-by-Step Surgical Execution
1. Preoperative Marking
Meticulous planning is the most critical step of the Bauer technique. All incisions must be outlined carefully with a fine skin-marking pen before inflation of the tourniquet.
Dorsal skin incisions. The rectangular dorsal flap (A) is designed to reconstruct the web space. Alternating triangular flaps (C, D, and E) are arranged to interdigitate with the corresponding volar flaps.
- Dorsal Flap Design: Draw a dotted line along the central axis of each involved digit. Design the dorsal rectangular flap ("A") so that its base begins at the level of the metacarpal heads. The flap should extend distally for approximately two-thirds of the length of the proximal phalanx.
- Palmar Flap Design: Design the proximal palmar flap ("B") so that its proximal limb sits just proximal to the adjacent normal commissures.
Palmar skin incisions. The rectangular flap (B) is arranged to cover the radial side of the ring finger. The remaining triangular flaps (C', D', and E') are designed to interdigitate seamlessly with the dorsal flaps.
2. Incision and Dissection
- Exsanguinate the limb and inflate the pneumatic tourniquet.
- Incise the dorsal flaps first. Elevate the dorsal rectangular flap ("A") from distal to proximal.
- Defatting: Carefully defat the proximal dorsal flap. This is essential to create a deep, natural-appearing web space. During defatting, meticulously identify and protect the dorsal sensory branches and the underlying neurovascular bundles.
- Incise the palmar flaps. Proceed with the midline dissection to separate the digits.
- Neurovascular Management: Dissect the common digital nerve and artery. The bifurcation of the common digital nerve can usually be teased apart proximally using blunt dissection. If the common digital artery bifurcates too distally (distal to the planned web space), the surgeon must ligate one of the proper digital arteries to allow the web space to drop to its normal anatomical level. Always verify the presence of an intact proper digital artery on the opposite side of the digit before ligation.
3. Flap Inset and Commissure Reconstruction
- Remove excess dorsal and palmar fat from the newly created web space to prevent a bulky, unnatural commissure.
- Suturing the Web: Suture the dorsal rectangular flap ("A") into the palmar defect first. This flap forms the floor of the new commissure and provides the critical dorsal-to-palmar slope.
- Suture the proximal palmar flap ("B") to resurface the proximal border of the adjacent digit.
- Interdigitating the Flaps: Suture the remaining triangular flaps (C to C', D to D', E to E') to resurface as much of the lateral intersurfaces of the digits as possible. The zig-zag nature of these flaps prevents longitudinal scar contracture.
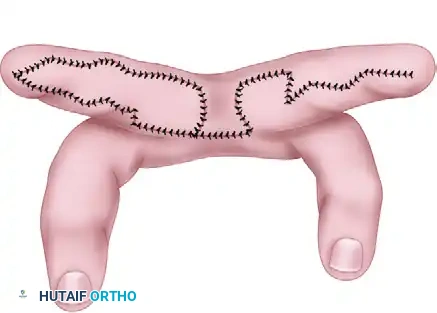
Separation is completed. The flaps have been sutured into place, covering the radial side of the ring finger and the web space. A full-thickness skin graft will be required for the remaining defect on the ulnar side of the long finger.
4. Tourniquet Release and Perfusion Check
- Deflate the tourniquet before applying skin grafts.
- Apply warm saline sponges to the hand and observe for reactive hyperemia.
- Ensure that perfusion to the tips of all triangular flaps is robust. If any flap appears ischemic or congested, remove the sutures, allow the tissue to rest, and resuture under less tension. Ischemic flap tips should be debrided to prevent delayed necrosis and infection.
5. Full-Thickness Skin Grafting (FTSG)
- Measure the remaining lateral digital defects.
- Harvest a full-thickness skin graft. The preferred donor sites in pediatric patients are the groin crease (lower abdomen, lateral to the femoral vessels) or the antecubital fossa (elbow crease). The groin is highly preferred as it provides hairless skin and the donor site scar is easily concealed by undergarments.
- Defat the graft meticulously until the white, shiny dermis is exposed.
- Suture the FTSG into the lateral digital defects using fine absorbable sutures.
💡 Management of Confluent Fingernails
In cases of complex complete syndactyly where the fingernails are confluent (synonychia), the nails must be sharply separated. It is imperative to excise the germinal and sterile matrix at the adjacent margins. The full-thickness skin grafts must then be brought around the lateral aspect of the distal phalanx to reconstruct the paronychial fold, preventing postoperative nail spikes and deformities.
Postoperative Protocol and Rehabilitation
The success of a syndactyly release is heavily dependent on meticulous postoperative care and immobilization. Pediatric patients are highly active, and graft shear or flap dehiscence are significant risks if the hand is not properly secured.
- Immediate Postoperative Dressing:
- Place a single layer of non-adherent gauze (e.g., Xeroform) over the suture lines and skin grafts.
- Carefully insert a wet contour dressing (such as saline-soaked fluffed gauze or cotton) between the newly separated fingers. Begin packing at the web space and work distally. This packing is critical to hold the fingers in wide abduction and full extension, preventing hematoma formation and graft shear.
- Apply a dry, bulky outer dressing.
- Immobilization:
- Apply a well-padded long-arm plaster splint or cast. The elbow should be flexed to 90 degrees, and the wrist placed in neutral to slight extension. A long-arm cast is mandatory in young children to prevent the dressing from slipping off.
- Elevation and Follow-up:
- The hand must be strictly elevated for the first 1 to 2 weeks to minimize edema.
- The initial dressing is typically left undisturbed for 1 to 2 weeks.
- At the 2-week postoperative mark, the cast and dressings are removed in the clinic (or under mild sedation if necessary). By this time, the flaps should be fully viable, the skin grafts should have achieved primary "take," and the incisions should be largely healed.

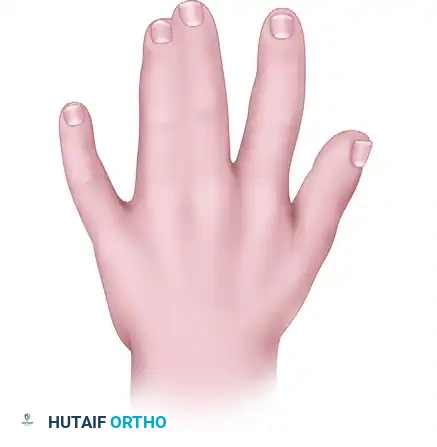
Postoperative clinical photograph demonstrating a successful syndactyly release. Note the well-healed commissure, the absence of web creep, and the independent alignment of the digits.
Complications and Pitfalls
Despite meticulous surgical technique, complications can occur following syndactyly release. Surgeons must be prepared to identify and manage these issues promptly.
- Web Creep: This is the most common long-term complication, characterized by the distal migration of the web space over time. It is usually caused by linear scar contracture, inadequate proximal reach of the dorsal rectangular flap, or partial loss of the skin graft at the base of the commissure. Severe web creep requires revision surgery, often utilizing a Z-plasty or a local advancement flap.
- Flap Necrosis and Graft Failure: Usually secondary to excessive tension, inadequate defatting of the FTSG, or postoperative hematoma. Minor tip necrosis can often be managed conservatively with local wound care, allowing it to heal by secondary intention. Major graft loss may require delayed regrafting.
- Neurovascular Injury: Accidental transection of the proper digital nerve or artery is a devastating complication. Meticulous loupe magnification and blunt longitudinal dissection are essential to prevent this. If an artery is inadvertently injured, microvascular repair should be attempted if feasible.
- Angular Deformity: Can persist if the syndactyly release is performed too late, particularly in border digits, or if underlying bony abnormalities (e.g., delta phalanx) are not addressed concurrently.
Conclusion
Syndactyly release requires a delicate balance of anatomical knowledge, precise flap geometry, and meticulous tissue handling. Whether utilizing the graft-sparing open technique of Withey et al. or the classic dorsal flap and FTSG technique of Bauer et al., the ultimate objective remains the same: to provide the pediatric patient with a functional, independent, and aesthetically pleasing hand that will grow and develop without restriction. Strict adherence to the principles of flap design, vascular preservation, and rigorous postoperative immobilization will ensure optimal outcomes in these challenging cases.
You Might Also Like