Congenital Upper Extremity Anomalies: Embryology and Transverse Deficiencies
Key Takeaway
The upper extremity develops between days 26 and 56 of gestation, governed by complex signaling centers including the apical ectodermal ridge and zone of polarizing activity. Disruptions in this embryological sequence can result in transverse deficiencies. Management requires a multidisciplinary approach, prioritizing early prosthetic fitting to match developmental milestones. Surgical interventions, such as the Krukenberg reconstruction, are reserved for specific functional indications, particularly in bilateral amputees with visual impairments.
Embryology of the Upper Extremity
The morphogenesis of the upper extremity is a highly orchestrated, spatiotemporally regulated process that begins early in the embryonic period. The arm arises as a small bud of mesenchymal tissue on the lateral body wall beginning on day 26 of gestation. Notably, this precedes the formation of the lower extremity (leg bud) by approximately 24 hours, establishing a cranial-to-caudal developmental gradient.
Growth and differentiation proceed in a strict proximal-to-distal fashion, governed by three primary signaling centers that dictate the three-dimensional spatial orientation of the limb:
- The Apical Ectodermal Ridge (AER): Located at the distal tip of the limb bud, the AER is responsible for proximal-to-distal growth. It secretes Fibroblast Growth Factors (FGFs) that maintain the underlying mesoderm in a highly proliferative state known as the progress zone.
- The Zone of Polarizing Activity (ZPA): Situated in the posterior (postaxial) margin of the limb bud mesoderm, the ZPA controls radioulnar (anterior-posterior) differentiation. The primary morphogen secreted by the ZPA is the Sonic Hedgehog (SHH) protein. Disruptions in SHH signaling explain the clinical phenomenon where ulnar-deficient limbs frequently present with associated preaxial (radial) hand deficiencies.
- The Wingless-Type (WNT) Signaling Center: Located within the dorsal ectoderm, this center secretes WNT-7a, which induces the expression of LMX1B in the underlying mesoderm, thereby determining the dorsal differentiation of the limb.
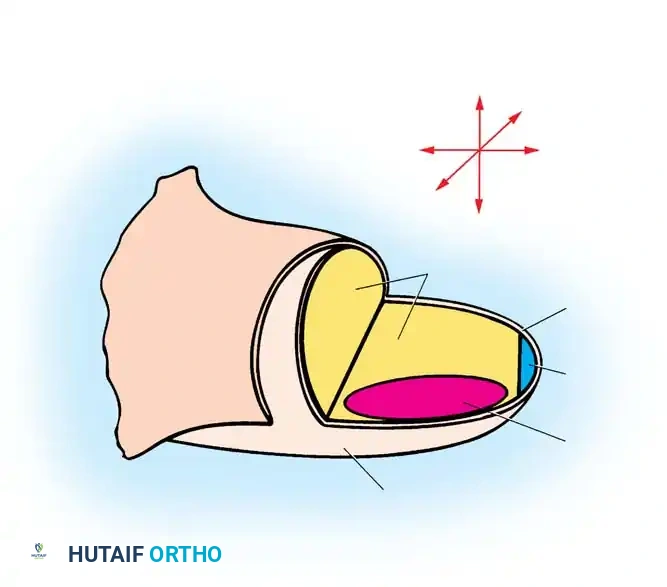
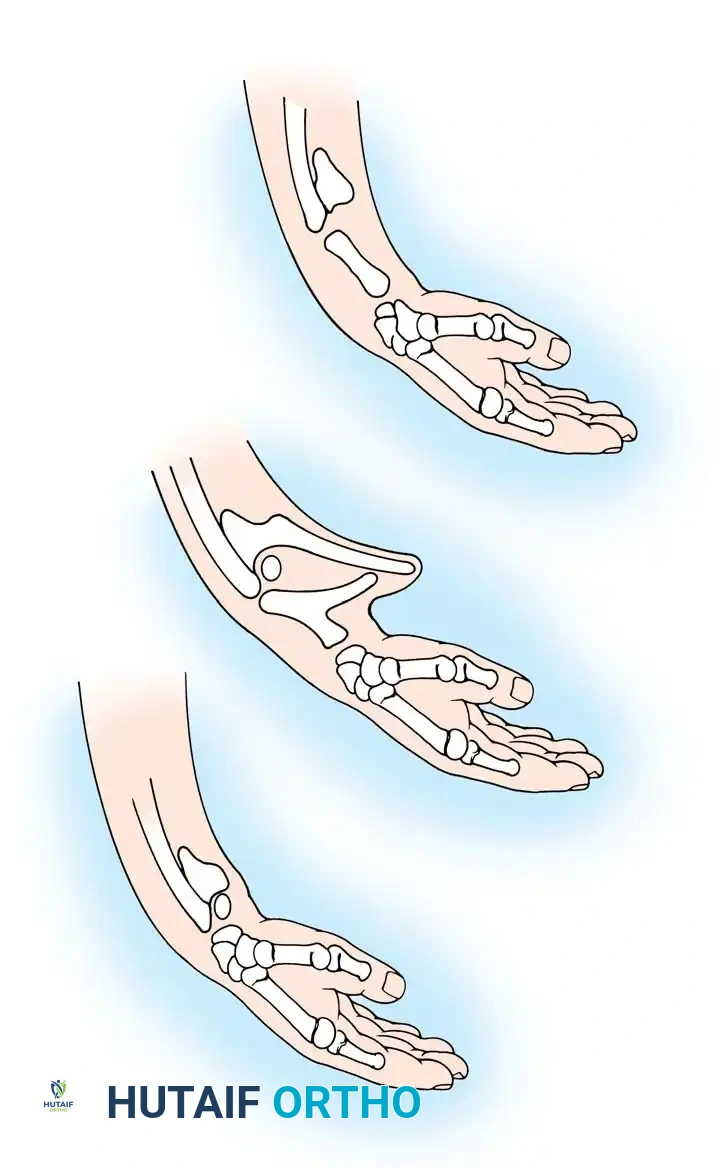
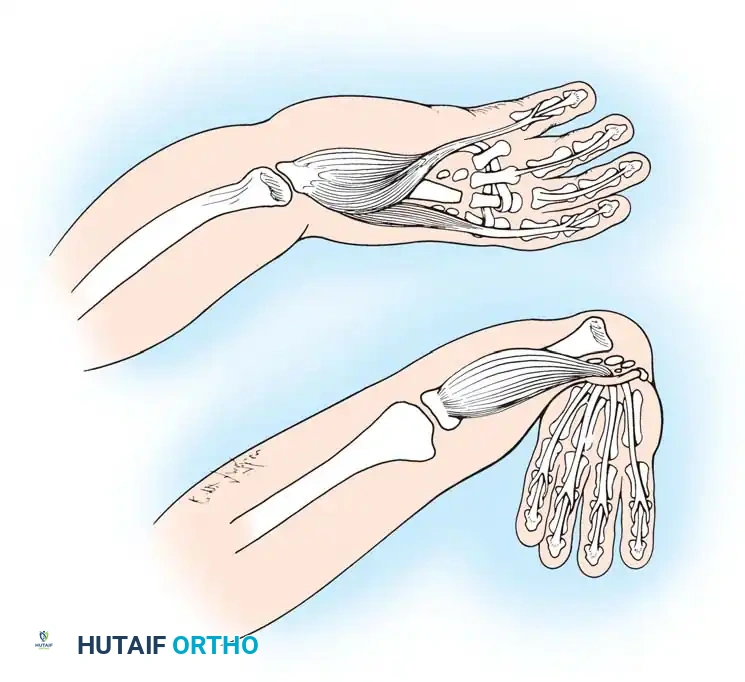
Fig. 76-1 Limb bud. The apical ectodermal ridge extends from anterior to posterior along the dorsal/ventral boundary of the growing limb bud. Proximal to the AER is the progress zone. Within the posterior mesoderm is the zone of polarizing activity. These centers are highly interconnected; limb patterning and growth depend entirely on their coordinated function.
By day 31 of gestation, the hand paddle becomes morphologically distinct. Through a genetically programmed process of cellular apoptosis (programmed cell death), the fissuring of the hand paddle is completed by day 36. The central rays form first, followed rapidly by the preaxial and postaxial digits. The formation of chondral elements, endochondral ossification, and the subsequent development of joints, musculature, and vascular networks follow in rapid succession. The entire embryological formation of the upper extremity is completed by the end of the 8th week of gestation.
Failure of Formation: Transverse Deficiencies
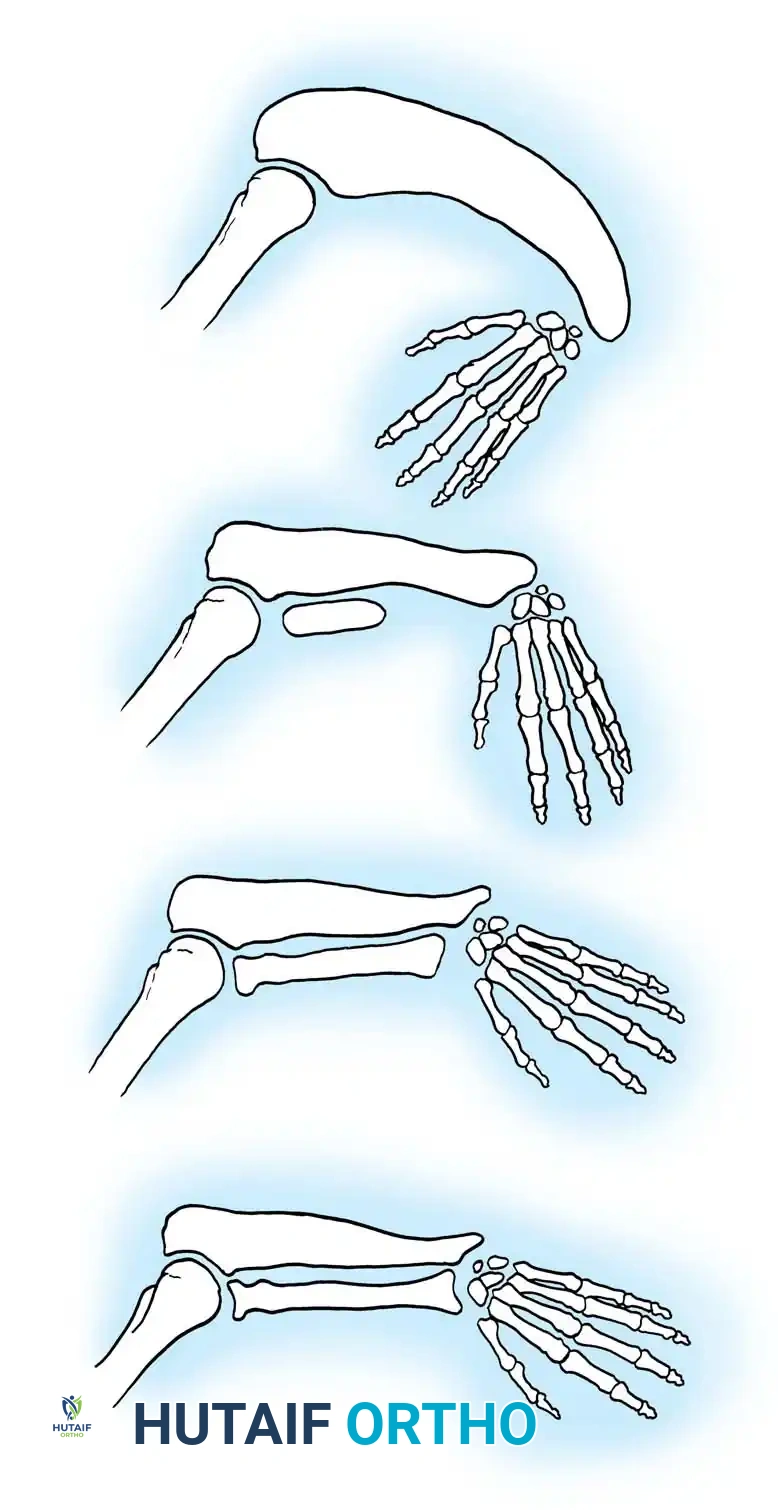
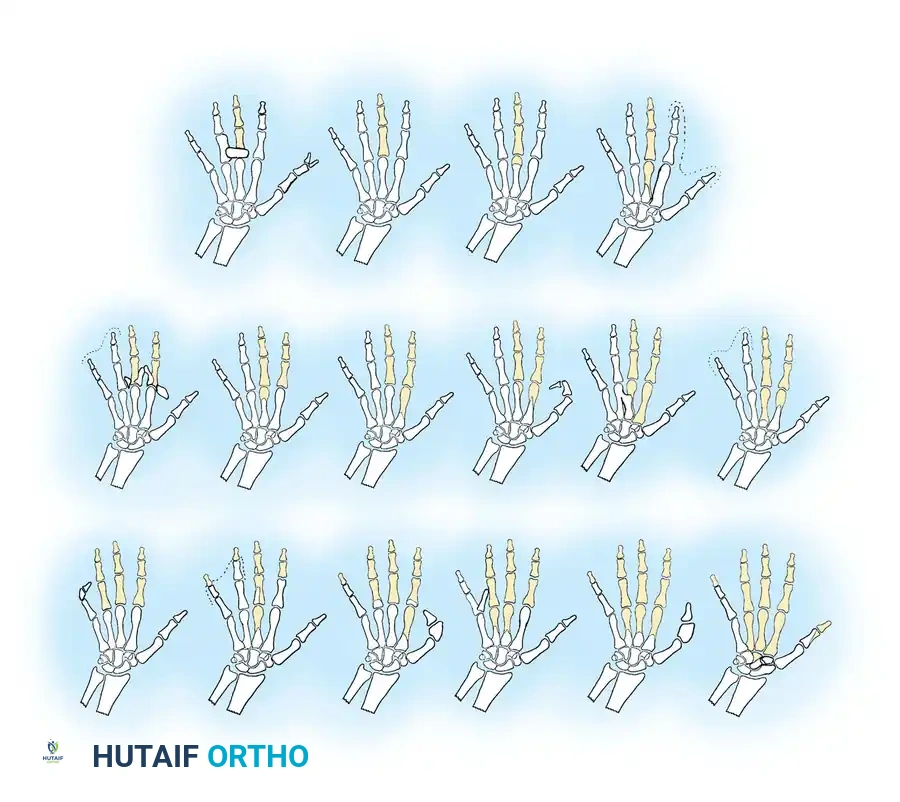
Transverse deficiencies represent a failure of formation (arrest of development) characterized by the complete absence of parts distal to a specific point on the upper extremity. This produces an amputation-like stump. Classification is strictly anatomical, naming the level at which the remaining stump terminates (e.g., proximal third forearm deficiency).
Epidemiology and Etiology
Wynne-Davies and Lamb reported the incidence of transverse deficiencies to be approximately 6.8 per 10,000 live births. The vast majority (98%) are unilateral, with the most common anatomical level being the upper third of the forearm. There is no established sex predilection.
The primary etiology is believed to be a failure or premature involution of the apical ectodermal ridge, likely secondary to an intrauterine vascular infarct. Environmental and pharmacological factors have also been implicated; for instance, the use of misoprostol (a prostaglandin E1 analogue) to induce abortion has been definitively shown to cause vascular disruption in utero, leading to transverse deficiencies in surviving infants.
Clinical Pearl: In the standard unilateral transverse deficiency, there is no underlying genetic basis. However, rare bilateral or multiple transverse deficiencies may be inherited as an autosomal recessive trait. Genetic counseling should be tailored accordingly.
While transverse deficiencies typically occur as isolated anomalies, they have been reported in association with several malformation syndromes and conditions, including:
* Hydrocephalus
* Spina bifida and myelomeningocele
* Congenital talipes equinovarus (Clubfoot)
* Radial head dislocation
* Radioulnar synostosis
Clinical Presentation
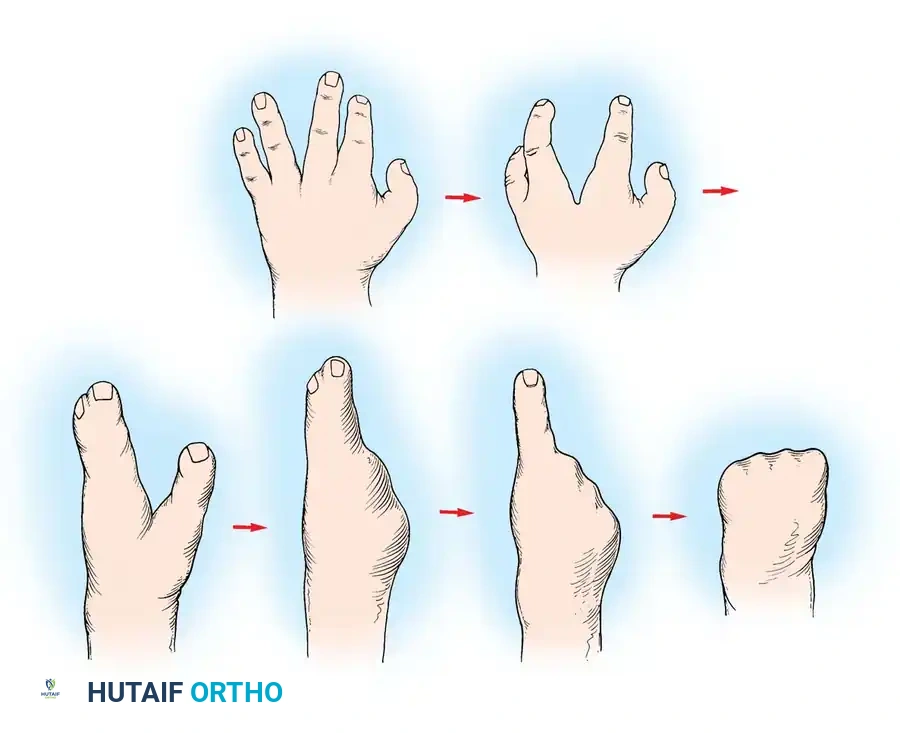
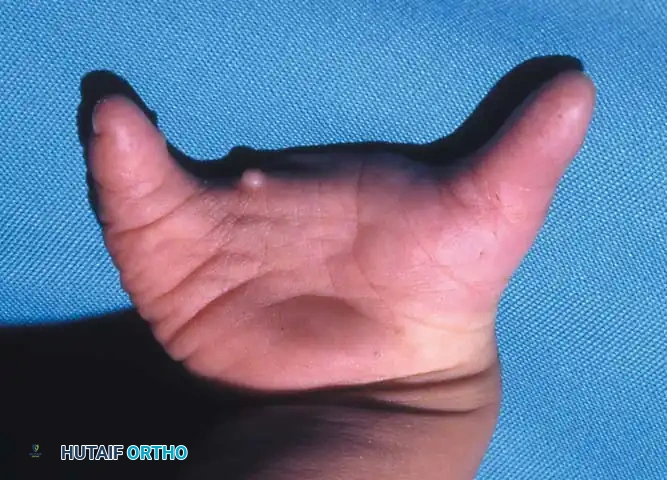
A newborn presenting with a transverse deficiency typically exhibits a slightly bulbous, well-padded stump. In more distal deficiencies, rudimentary, vestigial digital "nubbins" are frequently observed.

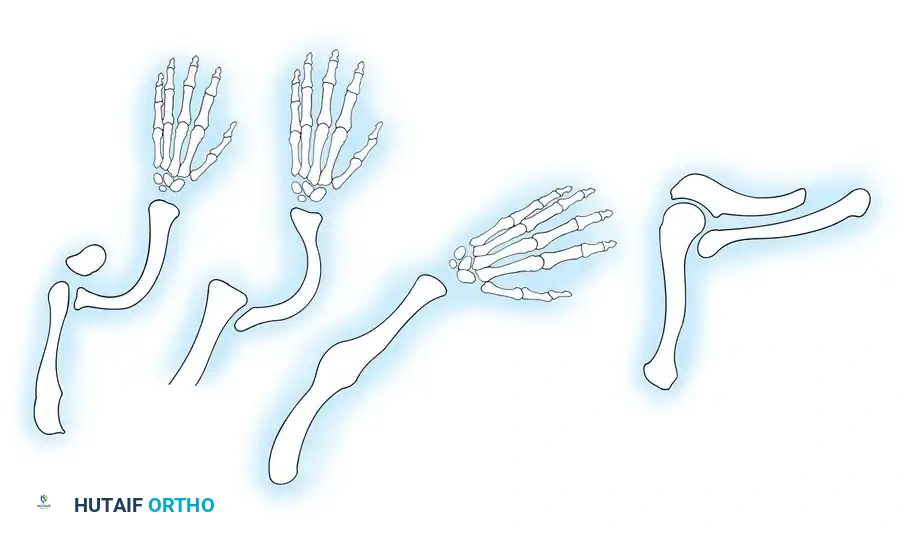
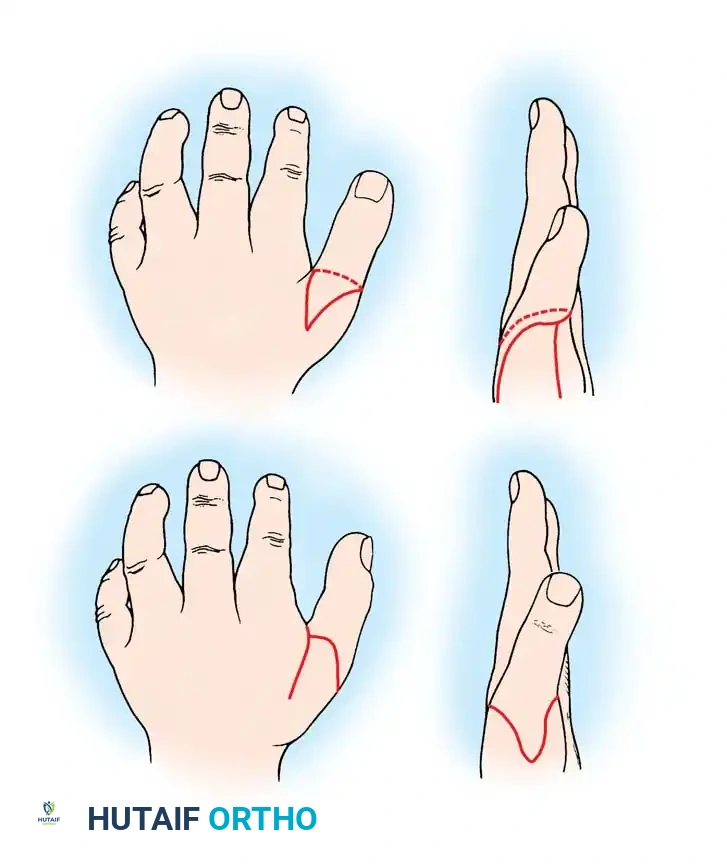
Fig. 76-2 Failure of formation (digital nubbins). The presence of functional wrist motion allows the limb to be used effectively as an assisting hand.
Hypoplasia of the more proximal musculature is a key clinical finding that helps differentiate true transverse deficiencies from amputations caused by congenital constriction band syndrome (amniotic band sequence). In the most common presentation—the upper forearm amputation—the forearm is usually no more than 7 cm long at birth and will reach a maximum length of approximately 10 cm by skeletal maturity.
In midcarpal amputations (the second most frequent level), the rudimentary digital remnants are almost always nonfunctional. However, because the radiocarpal joint is preserved, pronation and supination are usually possible, providing a highly functional assisting limb. Cognitive development and intelligence in these children are generally normal.
Prosthetic Management and Rehabilitation
For the vast majority of patients with transverse deficiencies, surgical intervention is unnecessary. The cornerstone of management is early prosthetic fitting, coordinated with the child's natural neurodevelopmental milestones.
Developmental Milestones and Prosthetic Staging
A child’s manual and bimanual skills develop in a predictable, orderly sequence. Prosthetic fitting must complement this timeline:
* Birth to 9 Months: Prehension is achieved primarily via bilateral palmar grasp.
* 12 to 18 Months: Single-hand grasp develops, followed by thumb-to-finger pinch. The cognitive ability to grasp precedes the voluntary ability to release.
* 24 Months: The child develops coordinated shoulder positioning, grasp, and release.

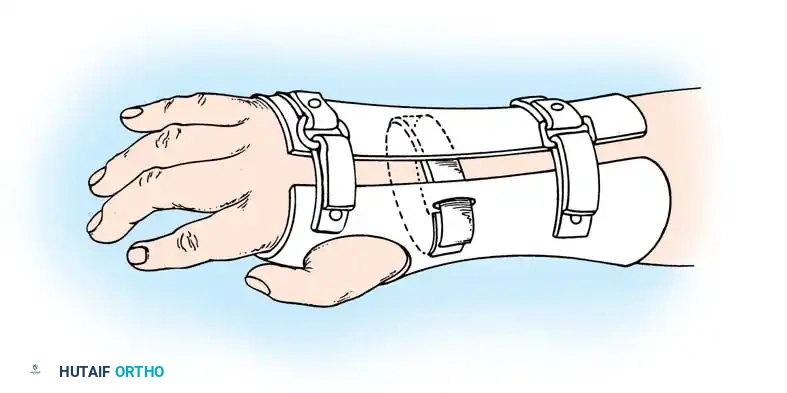
Fig. 76-3 A and B. Early fitting of a passive prosthesis in a child with a congenital forearm amputation is critical to encourage incorporation of the prosthesis into the child's body image.
Prosthetic Protocol by Age:
1. 3 to 6 Months (Sit to Fit): A passive plastic mitten prosthesis is introduced once the child achieves independent sitting balance. This provides stability during sitting and assists in pulling to a stand.
2. 12 to 18 Months: The passive mitten is exchanged for an actively opened, plastisol-covered split hook. A Child Amputee Prosthetic Program (CAPP) terminal device may be substituted. Training with the functional device begins immediately.
3. 2 to 4 Years: A myoelectrical prosthesis may be considered. Studies have shown these to be highly useful and appropriate for preschool-aged children, offering superior cosmesis and intuitive grip control.
4. 3 Years and Older: For above-elbow amputations, dual-terminal devices and articulated elbow controls (friction elbows) are introduced.
Surgical Warning: Prosthetic management for midcarpal amputations remains controversial. The long, below-elbow stump is exceptionally useful for stabilizing objects and bimanual function because it retains native sensibility. Sacrificing terminal sensibility for a cosmetic artificial hand must be carefully weighed against the functional loss.
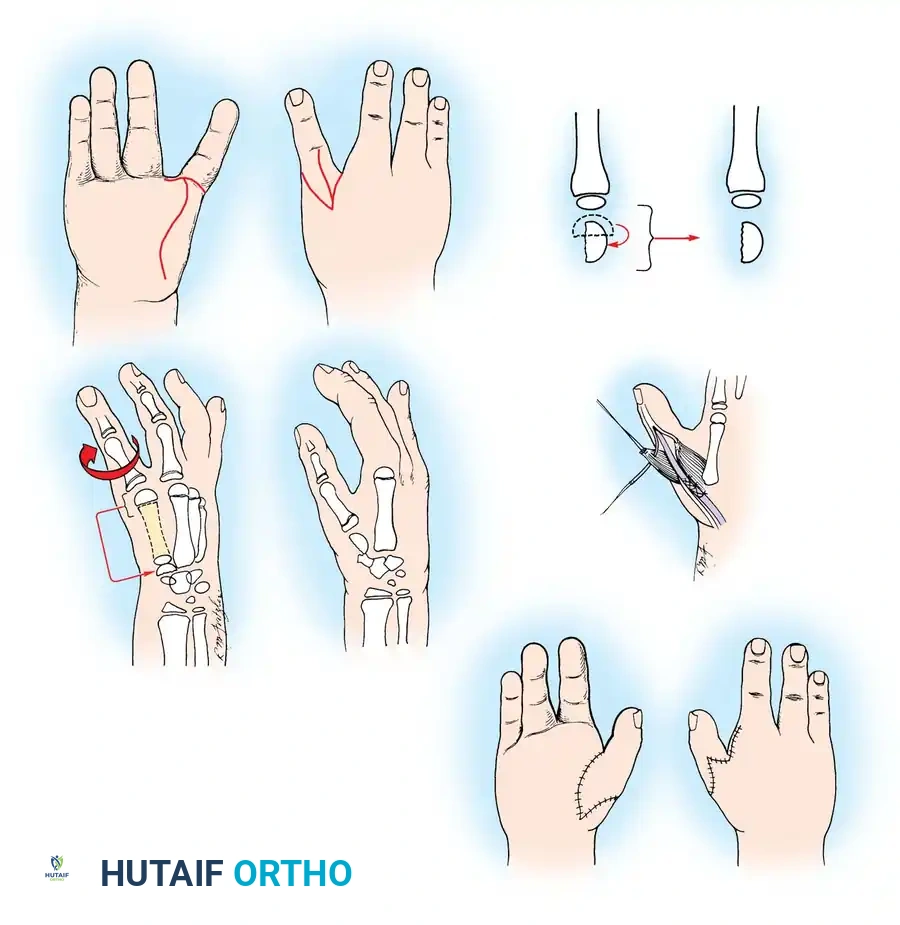
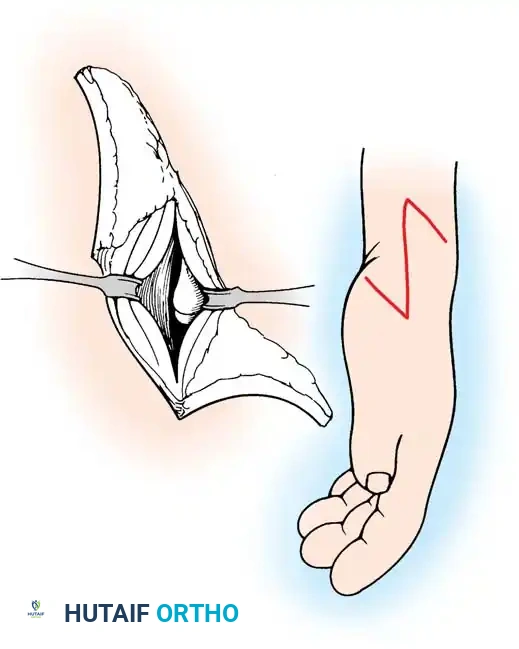
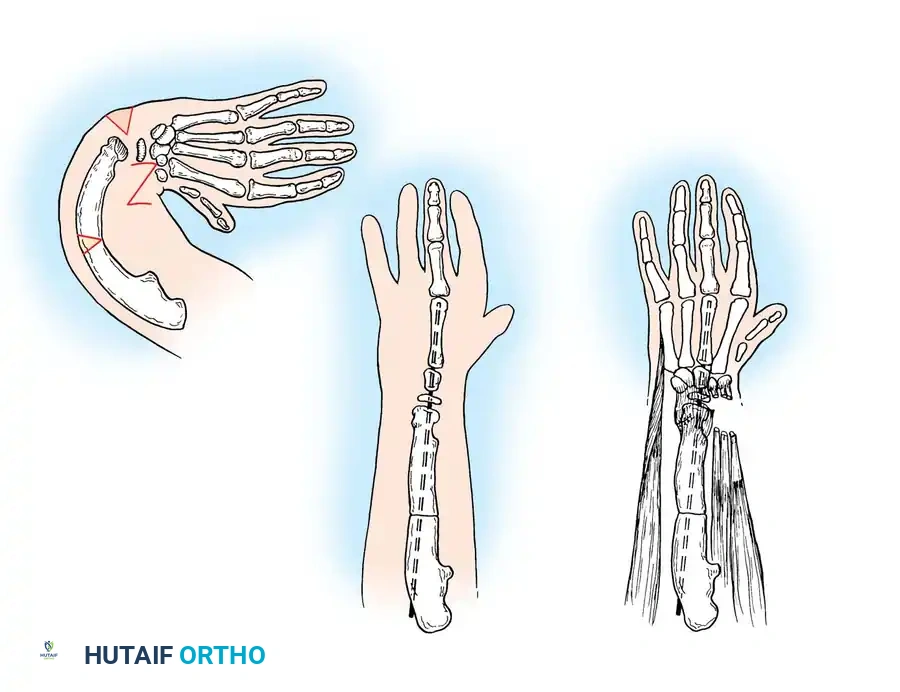
Surgical Interventions in Transverse Deficiencies
Surgical indications for transverse deficiencies are exceedingly rare. Epps, Burkhalter, and McCollough reported that out of 1,077 children
Associated Surgical & Radiographic Imaging














You Might Also Like


