Congenital Ring Syndrome: Surgical Management & Z-Plasty

Key Takeaway
Congenital ring syndrome, or amniotic band sequence, presents with deep circumferential cutaneous creases that compromise lymphatic and venous drainage. Surgical management requires a staged approach, typically utilizing multiple Z-plasties to excise the constricting bands without jeopardizing distal perfusion. Associated anomalies, such as acrosyndactyly and congenital amputations, necessitate early, coordinated reconstructive interventions to optimize hand function and prevent irreversible ischemic or neuropathic complications.
CONGENITAL RING SYNDROME: COMPREHENSIVE SURGICAL MANAGEMENT
Congenital ring syndrome—also widely recognized in the orthopedic and plastic surgery literature as congenital constriction band syndrome, amniotic band sequence, Streeter dysplasia, or annular grooves—is a complex congenital anomaly characterized by deep cutaneous creases that encircle a limb or digit. The clinical presentation mimics a scenario in which a string has been tightly tied around the developing extremity, leading to a cascade of mechanical, vascular, and neurological complications.
Because this condition is frequently associated with congenital amputations and acrosyndactyly, it is formally designated as a syndrome. The management of congenital ring syndrome demands a profound understanding of pediatric microvascular anatomy, the biomechanics of local tissue rearrangement, and the precise timing of staged surgical interventions to optimize functional outcomes and prevent irreversible ischemic damage.
Epidemiology and Etiology
The incidence of congenital ring syndrome is generally reported as approximately 1 in 15,000 live births, as established by Patterson's foundational epidemiological studies. In comprehensive reviews of congenital hand anomalies, such as Flatt’s extensive series, constriction bands represent roughly 2% of all upper extremity malformations. The condition exhibits a predilection for the distal aspects of the extremities, with the central digits of the hand being the most frequently involved.
There is currently no robust genetic evidence to suggest that congenital ring syndrome is an inherited condition; it is overwhelmingly considered a sporadic event. However, the exact pathogenesis has been a subject of historical and modern debate, broadly divided into extrinsic and intrinsic theories:
- The Extrinsic Theory (Kino & Torpin): Kino suggested that the primary etiology is an external mechanical effect caused by amniotic adhesions. Following a spontaneous rupture of the amnion (without rupture of the chorion) early in gestation, mesodermic bands emanate from the chorionic face of the amnion. These fibrous bands entangle the developing limbs, leading to mechanical constriction, secondary hemorrhages in the distal rays, and subsequent auto-amputation or syndactyly.
- The Intrinsic Theory (Patterson & Streeter): Streeter originally theorized that the bands were the result of a localized failure of germ plasm. Patterson expanded on this, suggesting that the rings represent a failure of the normal development of subcutaneous tissue, occurring in the exact same manner that normal skin creases are formed, but in a pathological, circumferential pattern.
Modern consensus heavily favors the extrinsic amniotic band theory, though there is general agreement that regardless of the exact mechanism, these malformations occur relatively later in embryogenesis (post-limb bud formation), which explains why the proximal anatomy is typically normal while the distal anatomy is mechanically disrupted.
CLINICAL PRESENTATION AND PATHOPHYSIOLOGY
The clinical manifestation of congenital ring syndrome exists on a spectrum of severity, ranging from superficial cosmetic grooves to deep, bone-deep constrictions that threaten the viability of the limb.
The primary pathophysiological insult is mechanical. A deep circumferential band acts as an unyielding tourniquet. Initially, this compromises the low-pressure lymphatic and venous systems, leading to profound distal lymphedema and cyanosis.

If the constriction is severe enough, arterial inflow is subsequently compromised, leading to ischemia, necrosis, and intrauterine auto-amputation.
Associated Anomalies
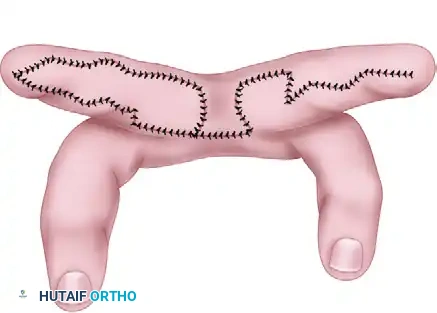
1. Acrosyndactyly:
Acrosyndactyly is a hallmark of congenital ring syndrome. Unlike simple syndactyly, where digits fail to separate during embryogenesis, acrosyndactyly occurs when normally formed digits are bound together by amniotic bands, leading to secondary fusion of the distal parts (usually the fingertips). A classic diagnostic feature of acrosyndactyly is the presence of proximal epithelialized clefts or sinuses between the fused digits, indicating that proximal separation had initially occurred.

2. Congenital Amputations:
Intrauterine amputations are common and represent the end-stage of severe vascular compromise. Fortunately, amputations in this syndrome usually possess adequate or even abundant soft-tissue coverage over the bony stumps and rarely require acute surgical reconstruction for coverage alone.

3. Neurological Deficits:
Deep bands can cause severe compression neuropathies. Jones et al. described their clinical experience with ulnar nerve palsy associated with congenital ring syndrome in children. A critical finding from their research is that simple, early surgical release of the band did not result in the return of ulnar nerve function at a mean follow-up of 7 years. The chronic intrauterine compression often leads to irreversible intraneural fibrosis. Consequently, they suggested that excision of the involved, fibrotic segment of the nerve followed by early nerve grafting may offer a superior chance for nerve recovery compared to simple neurolysis.
Clinical Pearl: Always perform a meticulous preoperative neurological examination in infants with deep constriction bands. Do not assume that releasing the band will spontaneously resolve a distal motor or sensory deficit. Be prepared for complex nerve reconstruction if a dense palsy is present.
SURGICAL INDICATIONS AND TIMING
The timing of surgical intervention is dictated by the severity of the vascular and lymphatic compromise:
- Emergent Intervention: Required in the neonatal period if a deep band is causing acute arterial insufficiency or rapidly progressive, severe lymphedema that threatens the viability of the distal part.
- Elective Staged Intervention: For stable bands, surgery is typically delayed until the infant is 3 to 6 months old to decrease anesthetic risks and allow for growth of the anatomical structures, making surgical dissection safer.
- Acrosyndactyly Timing: Because the fingertips are frequently bound together in a disorganized mass, permanent skeletal deformity and joint contractures will result unless early reconstruction is performed. Release of the border digits (thumb and small finger) should be prioritized and performed within the first 6 months of life to allow for independent grasp and pinch. Release of the central digits is typically staged when the child is approximately 18 months old.
BIOMECHANICS OF THE Z-PLASTY IN RING SYNDROME
Simple excision of a congenital groove with a direct, everting closure is universally condemned in modern operative orthopedics. A linear, circumferential incision will inevitably heal with a circumferential scar. As this scar matures and contracts, it will recreate the exact tourniquet effect the surgery was intended to cure.
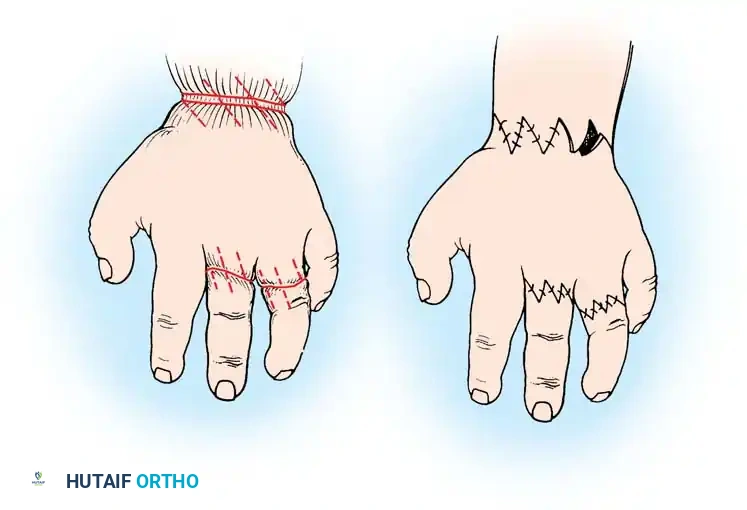
The multiple Z-plasty technique is the gold standard. A Z-plasty serves two critical biomechanical functions:
1. Elongation: By transposing two triangular flaps, the central limb of the Z is elongated. A classic 60-degree Z-plasty increases the length of the tissue in the direction of the central limb by approximately 73%.
2. Redirection of Scar Tension: The Z-plasty breaks up the linear scar, redirecting the forces of scar contracture by 90 degrees, thereby completely eliminating the risk of a recurrent circumferential stricture.
Surgical Warning: Never attempt to excise a deep congenital ring 360 degrees around a limb or digit in a single operative setting. The subdermal plexus and superficial venous drainage are already compromised by the band. A complete circumferential excision disrupts the remaining superficial venous and lymphatic return, risking catastrophic venous congestion, flap necrosis, and loss of the digit. Always stage the release, addressing only 50% of the circumference at a time.
SURGICAL TECHNIQUE: MULTIPLE Z-PLASTY RELEASE (TECHNIQUE 76-50)
The following technique details the staged excision and multiple Z-plasty reconstruction for a deep congenital constriction band.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia is required. Ensure the pediatric anesthesiologist is comfortable with the infant's age and weight.
- Positioning: Supine with the affected extremity extended on a radiolucent hand table.
- Tourniquet: A pediatric pneumatic tourniquet is applied proximally. Crucial step: Do not inflate the tourniquet until all surgical markings are complete, as exsanguination will distort the normal resting tension of the skin and the exact depth of the band.
Step-by-Step Surgical Approach
-
Surgical Planning and Marking:
- Examine the depth of the ring. Ascertain that you will only address one-half (180 degrees) of the circumference (e.g., the volar half or the dorsal half) during this initial procedure.
- Using a fine surgical marker, outline the multiple Z-plasty sites along the constricting ring. The central limb of each Z-plasty should lie directly within the deepest part of the groove.
- Design the triangular flaps with angles of approximately 60 degrees to maximize lengthening while preserving robust flap vascularity.
-
Exsanguination and Tourniquet Inflation:
- Elevate the limb and exsanguinate using an Esmarch bandage or gravity elevation, depending on the fragility of the distal tissues.
- Inflate the tourniquet to the appropriate pediatric pressure (typically 50-75 mmHg above systolic blood pressure).
-
Excision of the Constricting Band:
- Sharply incise along the marked central limbs within the groove.
- Critical Maneuver: The constricting band is not merely a skin crease; it consists of dense, fibrotic, avascular tissue that extends deep into the subcutaneous fat, often down to the deep investing fascia of the muscle or tendon sheaths.
- Meticulously excise this entire fibrotic band. You must visualize healthy, unscarred fat and normal deep fascia before proceeding. Failure to excise the deep fibrotic tether will result in persistent lymphedema and incomplete resolution of the contour deformity.
- Take extreme care to protect underlying neurovascular bundles, which may be displaced or compressed immediately deep to the band.
-
Flap Elevation and Transposition:
- Sharply incise the limbs of the Z-plasties to create the triangular flaps.
- Elevate the flaps at the level of the deep subcutaneous tissue, ensuring a robust subdermal plexus is maintained to prevent tip necrosis.
- Transpose the flaps in an interdigitating fashion. This maneuver will immediately release the constriction and visibly lengthen the segment.
-
Closure and Hemostasis:
- Deflate the tourniquet before final closure to ensure meticulous hemostasis. Bipolar electrocautery should be used sparingly to avoid thermal injury to the delicate pediatric skin edges.
- Suture the flaps using fine, absorbable sutures (e.g., 5-0 or 6-0 chromic gut or fast-absorbing plain gut) to avoid the need for suture removal in an awake infant. Place deep dermal interrupted sutures to take tension off the epidermal closure.
-
Dressing and Splinting:
- Apply a non-adherent dressing (e.g., Xeroform or Adaptic) over the incisions.
- Apply a bulky, soft compressive dressing.
- Immobilize the extremity in a well-padded short-arm or long-arm plaster splint, depending on the level of the band, to protect the surgical site from shear forces during the healing phase.
ADVANCED RECONSTRUCTIVE CONSIDERATIONS
Management of Acrosyndactyly
Because the fingertips in acrosyndactyly are bound together by scar tissue rather than a failure of embryologic separation, the surgical approach differs slightly from simple syndactyly. The distal fusion mass must be carefully dissected to separate the terminal phalanges and nail beds.
Finger stiffness, particularly at the proximal interphalangeal (PIP) joints, is a very common postoperative complication following syndactyly release in these patients. This stiffness is multifactorial, stemming from both the initial intrauterine tethering and the subsequent surgical scarring. Aggressive postoperative occupational therapy is mandatory once the incisions have healed.
Management of the Shortened Digit and Thumb
Congenital amputations or severe growth arrests can leave the child with profoundly shortened digits that impair pinch and grasp mechanics.
* Distraction Osteogenesis: Short digits may require lengthening by osteotomy and the application of a miniature external fixator for gradual distraction osteogenesis. This is typically delayed until the child is older and the phalangeal bones have sufficient stock to hold the pins.
* Thumb Reconstruction: A shortened, inadequate thumb severely limits hand function. Reconstruction may involve deepening of the first web space (using a four-flap Z-plasty or dorsal rotational flap) to increase the relative length of the thumb.
* The Søiland Method: In cases of extreme thumb hypoplasia combined with a shortened, non-functional index finger, the method of Søiland may be employed. This complex procedure involves transposing the remnant of the shortened index finger onto the top of the thumb stump, effectively creating a longer, stable post to oppose the remaining ulnar digits.
POSTOPERATIVE PROTOCOL AND AFTERTREATMENT
The immediate postoperative focus is on protecting the transposed flaps and monitoring distal perfusion.
- Immobilization: The bulky dressing and splint are maintained continuously for 2 to 3 weeks. In infants, an above-elbow splint is often necessary even for distal procedures to prevent the child from pulling the splint off.
- Wound Care: If non-absorbable sutures were utilized, they are removed in the clinic under mild sedation or distraction after 10 to 14 days. If absorbable sutures were used, the wounds are simply inspected at the 2-week mark.
- Resolution of Symptoms: Parents should be counseled that the lymphedema and cyanosis distal to the band will not disappear instantly. The lymphatic channels require time to recanalize and remodel. Improvement is usually gradual over several weeks to months following the release.
- Staging the Second Procedure: The remaining unoperated half of the constricting ring is scheduled for identical Z-plasty reconstruction approximately 2 to 3 months after the index procedure. This interval allows the initial surgical site to heal completely, ensuring that the newly established superficial venous and lymphatic drainage pathways are robust enough to support the distal extremity during the second surgery.
By adhering to these strict biomechanical principles and staged surgical timelines, the orthopedic surgeon can safely eliminate the constricting bands, restore normal limb contour, and maximize the functional potential of the child's extremity.
You Might Also Like