Orthopedic Trauma MCQs & Clinical Insights: Advanced Exam Preparation
14 Apr 2026
56 min read
136 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Trauma MCQs & Clinical Insights: A...
00:00
Start Quiz
Question 1High Yield
Which structure is indicated by the arrow in Figure 33?

Explanation
The posterior position of the sciatic nerve in relation to the acetabulum and the lateral peroneal division makes the peroneal division of the sciatic nerve the portion of the nerve that is most likely to be injured in a posterior traumatic hip dislocation, accounting for up to 10% of concomitant nerve injuries with posterior hip dislocation. The corona mortis is an anatomic variant that results in vascular anastomosis between the obturator and either the external iliac or inferior epigastric arteries. This variant occurs in approximately 80% of patients and varies in its position, being located 4 cm to 9 cm lateral to the symphysis pubis. The obturator vascular bundle is situated in the fat medial to the obturator internus muscle and must be mobilized to access the quadrilateral plate. Dissection may be carried out both above and below this vascular leash. The Kocher-Langenbeck approach is indicated for fractures involving the posterior wall and/or posterior column of the acetabulum and for both column fractures that require direct posterior visualization. This approach is not indicated for direct reduction of the anterior wall or column when direct visualization is required anteriorly. The L5 nerve root is located on the anterior sacrum and is indicated by the arrow.
The position of this neural structure must be considered whether the surgeon is stabilizing 31 the sacroiliac (SI) joint with percutaneous iliosacral screws or with anterior SI plating through the lateral window of the ilioinguinal approach.
RECOMMENDED READINGS
1. [Cornwall R, Radomisli TE. Nerve injury in traumatic dislocation of the hip. Clin Orthop Relat Res. 2000 Aug;(377):84-91. Review. PubMed PMID: 10943188. ](http://www.ncbi.nlm.nih.gov/pubmed/10943188)[View](http://www.ncbi.nlm.nih.gov/pubmed/10943188)[ ](http://www.ncbi.nlm.nih.gov/pubmed/10943188)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10943188)
2. [Darmanis S, Lewis A, Mansoor A, Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007 May;20(4):433-9. PubMed PMID: 16944498. ](http://www.ncbi.nlm.nih.gov/pubmed/16944498)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16944498)
3. [Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. ](http://www.ncbi.nlm.nih.gov/pubmed/21368098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21368098)
4. Rommens P. The Kocher-Langenbeck approach for the treatment of acetabular fractures. Operat Orthop Traumatol 2004; 16:59-74.
5. [Langford JR, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 2. Contemporary indications and techniques for definitive surgical management. J Am Acad Orthop Surg. 2013 Aug;21(8):458-68. doi: 10.5435/JAAOS-21-08-458. Review. PubMed PMID: 23908252.](http://www.ncbi.nlm.nih.gov/pubmed/23908252)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23908252)
The position of this neural structure must be considered whether the surgeon is stabilizing 31 the sacroiliac (SI) joint with percutaneous iliosacral screws or with anterior SI plating through the lateral window of the ilioinguinal approach.
RECOMMENDED READINGS
1. [Cornwall R, Radomisli TE. Nerve injury in traumatic dislocation of the hip. Clin Orthop Relat Res. 2000 Aug;(377):84-91. Review. PubMed PMID: 10943188. ](http://www.ncbi.nlm.nih.gov/pubmed/10943188)[View](http://www.ncbi.nlm.nih.gov/pubmed/10943188)[ ](http://www.ncbi.nlm.nih.gov/pubmed/10943188)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10943188)
2. [Darmanis S, Lewis A, Mansoor A, Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007 May;20(4):433-9. PubMed PMID: 16944498. ](http://www.ncbi.nlm.nih.gov/pubmed/16944498)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16944498)
3. [Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. ](http://www.ncbi.nlm.nih.gov/pubmed/21368098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21368098)
4. Rommens P. The Kocher-Langenbeck approach for the treatment of acetabular fractures. Operat Orthop Traumatol 2004; 16:59-74.
5. [Langford JR, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 2. Contemporary indications and techniques for definitive surgical management. J Am Acad Orthop Surg. 2013 Aug;21(8):458-68. doi: 10.5435/JAAOS-21-08-458. Review. PubMed PMID: 23908252.](http://www.ncbi.nlm.nih.gov/pubmed/23908252)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23908252)
Question 2High Yield
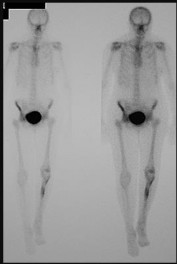
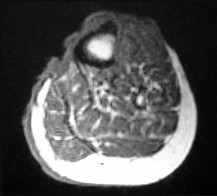
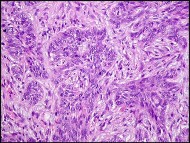
Figure 68a is the clinical photograph of a 59-year-old woman who has had a long-standing fungating ulcer on her left lower leg. She states that the ulcer began as a small reddened area and gradually enlarged during the last 4 years. Anteroposterior (AP) and lateral radiographs of her left leg are shown in Figures 68b and 68c. A whole-body bone scan is shown in Figure 68d. An axial T1-weighted MR image is shown in Figure 68e. A CT scan of the pelvis at the level of the groin is shown in Figure 68f. A histologic specimen is shown in Figure 68g. Based on the clinical, radiographic, and histologic information, the diagnosis is






Explanation
The clinical photograph reveals a large ulcerated lesion of the anterior leg. The AP and lateral radiographs reveal the soft-tissue abnormality, and the bone scan reveals increased metabolic activity of the underlying tibia. T1-weighted MR imaging reveals the lesion wrapping around the anterior tibia with loss of subcutaneous tissue. A CT scan of the pelvis reveals an inguinal lymph node. The histology reveals nests of polyhedral cells surrounded by reactive fibrosis. The diagnosis is poorly differentiated squamous cell carcinoma, and the patient has the characteristic findings of a long-standing squamous cell carcinoma with poor differentiation and likely regional lymph node metastasis. The history of a small reddened area does not suggest any of the other diagnoses. Although keratin pearls are not shown in this histologic field, nests of polyhedral cells indicate squamous cell carcinoma. A small subset of patients with squamous cell carcinoma will have advanced disease. Size and differentiation, as well as type of surgical procedure and margins of resection, are of prognostic significance. Sentinel node evaluation for patients at high risk has been suggested, including evaluations for lesions that are larger in size and with poor differentiation, perineural invasion, or compromised immunologic states. The nonpreferred responses are not associated with the clinical presentation of squamous cell carcinoma. Squamous cell carcinomas are keratin positive on immunohistochemistry.
RECOMMENDED READINGS
33. [Kwon S, Dong ZM, Wu PC. Sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma: clinical experience and review of literature. World J Surg Oncol. 2011 Jul 19;9:80. doi: 10.1186/1477-7819-9-80. Review. PubMed PMID: 21771334.](http://www.ncbi.nlm.nih.gov/pubmed/21771334)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21771334)
34. [North JH Jr, Spellman JE, Driscoll D, Velez A, Kraybill WG, Petrelli NJ. Advanced cutaneous squamous cell carcinoma of the trunk and extremity: analysis of prognostic factors. J Surg Oncol. 1997 Mar;64(3):212-7. PubMed PMID: 9121152.](http://www.ncbi.nlm.nih.gov/pubmed/9121152)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9121152)
CLINICAL SITUATION FOR QUESTIONS 69 AND 70
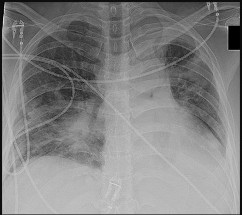
Figure 69a is the radiograph of a 39-year-old woman with metastatic lung cancer who underwent a prophylactic right intramedullary nail procedure. There were no intraoperative or immediate postsurgical problems. Ten hours after surgery, the patient became increasingly confused and agitated. An examination was notable for altered mentation, tachycardia, and new-onset hypoxemia. Chest radiographs were obtained before surgery (Figure 69b) and immediately after symptom onset (Figure 69c).
RECOMMENDED READINGS
33. [Kwon S, Dong ZM, Wu PC. Sentinel lymph node biopsy for high-risk cutaneous squamous cell carcinoma: clinical experience and review of literature. World J Surg Oncol. 2011 Jul 19;9:80. doi: 10.1186/1477-7819-9-80. Review. PubMed PMID: 21771334.](http://www.ncbi.nlm.nih.gov/pubmed/21771334)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21771334)
34. [North JH Jr, Spellman JE, Driscoll D, Velez A, Kraybill WG, Petrelli NJ. Advanced cutaneous squamous cell carcinoma of the trunk and extremity: analysis of prognostic factors. J Surg Oncol. 1997 Mar;64(3):212-7. PubMed PMID: 9121152.](http://www.ncbi.nlm.nih.gov/pubmed/9121152)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9121152)
CLINICAL SITUATION FOR QUESTIONS 69 AND 70
Figure 69a is the radiograph of a 39-year-old woman with metastatic lung cancer who underwent a prophylactic right intramedullary nail procedure. There were no intraoperative or immediate postsurgical problems. Ten hours after surgery, the patient became increasingly confused and agitated. An examination was notable for altered mentation, tachycardia, and new-onset hypoxemia. Chest radiographs were obtained before surgery (Figure 69b) and immediately after symptom onset (Figure 69c).
Question 3High Yield
--An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Explanation
No detailed explanation provided for this question.
Question 4High Yield
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include**
Explanation
The patient has a rupture of the long head of the biceps; however, patients older than age 45 years are at greater risk of having an associated rotator cuff tear. An MRI scan should be ordered to avoid missing concomitant rotator cuff pathology. While patients may report pain radiating down the arm at the time of the tendon rupture, an EMG is not indicated. The short head of the biceps is intact and needs no further work-up, even though the muscle descends in most cases. The anterior labrum can be injured but is not associated with this deformity.
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 5High Yield
Figures 1 and 2 are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?

Explanation
■
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
■
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
Question 6High Yield
If a patient develops posttraumatic osteonecrosis after undergoing head preservation treatment, which radiographic findings help to predict a lower likelihood of successful conversion to an anatomic shoulder arthroplasty?
Explanation
Fractures of the proximal humerus are now the third-most-common fracture in patients older than 60 years of age. This patient sustained a displaced, commonly described 3-part/4-part proximal humerus fracture. The number of fracture fragments and angulation, as initially described by Codman and then Neer, does not necessarily help to predict risk for subsequent AVN. Although the main blood supply to the humeral head historically was believed to be a branch from the anterior circumflex, adequate perfusion can remain through the posteromedial calcar following trauma. Hertel and associates reported that the most accurate predictor of ischemia was whether the length of the metaphyseal head extension for the calcar segment was shorter than 8 mm.
Locking plates have provided surgical alternatives to many unstable fracture patterns previously considered ominous. Although much enthusiasm remains for this use, a relatively high level of
complications has been reported with their use. A multicenter study reported a 14% incidence of intra-articular screw perforation as the most common complication.
When patients are deemed poor candidates for head preservation treatment, both hemiarthroplasty and rTSA can provide successful results when applied and performed appropriately. An increasing body of evidence appears to support consideration of a reverse prosthesis for older patients. A crucial aspect of hemiarthroplasty success is anatomic healing of the tuberosities around the implant. If the greater tuberosity displaces or reabsorbs, patients experience significant loss of active motion. The level of pain, however, is unpredictable. Although beneficial in a reverse prosthesis, anatomic tuberosity position does not appear to be as crucial. Depending on the definition of “complication,” some researchers have reported a higher complication rate for the reverse prosthesis.
If posttraumatic necrosis develops following head preservation treatment, conversion to an anatomic shoulder arthroplasty can provide good success in motion and function, particularly when the tuberosities heal in a relatively anatomic position. However, several researchers, most recently Moineau and associates, report suboptimal results when the greater tuberosity is positioned in a substantial amount of varus that necessitates osteotomy. In this scenario, rTSA should be considered.
RECOMMENDED READINGS
8. [Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. ](http://www.ncbi.nlm.nih.gov/pubmed/15220884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15220884)
9. [Südkamp N, Bayer J, Hepp P, Voigt C, Oestern H, Kääb M, Luo C, Plecko M, Wendt K, Köstler W, Konrad G. Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational study. J Bone Joint Surg Am. 2009 Jun;91(6):1320-8. PubMed PMID: 19487508. ](http://www.ncbi.nlm.nih.gov/pubmed/19487508)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487508)
10. [Anakwenze OA, Zoller S, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for acute proximal humerus fractures: a systematic review. J Shoulder Elbow Surg. 2014 Apr;23(4):e73-80. doi: 10.1016/j.jse.2013.09.012. Epub 2014 Jan 7. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24406120)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24406120)
11. [Jarrett CD, Brown BT, Schmidt CC. Reverse shoulder arthroplasty. Orthop Clin North Am. 2013 Jul;44(3):389-408, Epub 2013 Apr 29. Review. PubMed PMID: 23827841. ](http://www.ncbi.nlm.nih.gov/pubmed/23827841)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/23827841)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23827841)
12. Moineau G, McClelland WB Jr, Trojani C, Rumian A, Walch G, Boileau P. Prognostic factors and limitations of anatomic shoulder arthroplasty for the treatment of posttraumatic cephalic collapse or necrosis (type-1 proximal humeral fracture sequelae). J Bone Joint Surg Am. 2012 Dec 5;94(23):2186-
[94/. doi: 10.2106/JBJS.J.00412. PubMed PMID: 23224389. ](http://www.ncbi.nlm.nih.gov/pubmed/23224389)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23224389)
13. [Namdari S, Horneff JG, Baldwin K. Comparison of hemiarthroplasty and reverse arthroplasty for treatment of proximal humeral fractures: a systematic review. J Bone Joint Surg Am. 2013 Sep 18;95(18):1701-8.. PubMed PMID: 24048558. ](http://www.ncbi.nlm.nih.gov/pubmed/24048558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24048558)
Locking plates have provided surgical alternatives to many unstable fracture patterns previously considered ominous. Although much enthusiasm remains for this use, a relatively high level of
complications has been reported with their use. A multicenter study reported a 14% incidence of intra-articular screw perforation as the most common complication.
When patients are deemed poor candidates for head preservation treatment, both hemiarthroplasty and rTSA can provide successful results when applied and performed appropriately. An increasing body of evidence appears to support consideration of a reverse prosthesis for older patients. A crucial aspect of hemiarthroplasty success is anatomic healing of the tuberosities around the implant. If the greater tuberosity displaces or reabsorbs, patients experience significant loss of active motion. The level of pain, however, is unpredictable. Although beneficial in a reverse prosthesis, anatomic tuberosity position does not appear to be as crucial. Depending on the definition of “complication,” some researchers have reported a higher complication rate for the reverse prosthesis.
If posttraumatic necrosis develops following head preservation treatment, conversion to an anatomic shoulder arthroplasty can provide good success in motion and function, particularly when the tuberosities heal in a relatively anatomic position. However, several researchers, most recently Moineau and associates, report suboptimal results when the greater tuberosity is positioned in a substantial amount of varus that necessitates osteotomy. In this scenario, rTSA should be considered.
RECOMMENDED READINGS
8. [Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. ](http://www.ncbi.nlm.nih.gov/pubmed/15220884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15220884)
9. [Südkamp N, Bayer J, Hepp P, Voigt C, Oestern H, Kääb M, Luo C, Plecko M, Wendt K, Köstler W, Konrad G. Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational study. J Bone Joint Surg Am. 2009 Jun;91(6):1320-8. PubMed PMID: 19487508. ](http://www.ncbi.nlm.nih.gov/pubmed/19487508)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487508)
10. [Anakwenze OA, Zoller S, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for acute proximal humerus fractures: a systematic review. J Shoulder Elbow Surg. 2014 Apr;23(4):e73-80. doi: 10.1016/j.jse.2013.09.012. Epub 2014 Jan 7. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24406120)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24406120)
11. [Jarrett CD, Brown BT, Schmidt CC. Reverse shoulder arthroplasty. Orthop Clin North Am. 2013 Jul;44(3):389-408, Epub 2013 Apr 29. Review. PubMed PMID: 23827841. ](http://www.ncbi.nlm.nih.gov/pubmed/23827841)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/23827841)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23827841)
12. Moineau G, McClelland WB Jr, Trojani C, Rumian A, Walch G, Boileau P. Prognostic factors and limitations of anatomic shoulder arthroplasty for the treatment of posttraumatic cephalic collapse or necrosis (type-1 proximal humeral fracture sequelae). J Bone Joint Surg Am. 2012 Dec 5;94(23):2186-
[94/. doi: 10.2106/JBJS.J.00412. PubMed PMID: 23224389. ](http://www.ncbi.nlm.nih.gov/pubmed/23224389)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23224389)
13. [Namdari S, Horneff JG, Baldwin K. Comparison of hemiarthroplasty and reverse arthroplasty for treatment of proximal humeral fractures: a systematic review. J Bone Joint Surg Am. 2013 Sep 18;95(18):1701-8.. PubMed PMID: 24048558. ](http://www.ncbi.nlm.nih.gov/pubmed/24048558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24048558)
Question 7High Yield
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure?
---
---








Explanation
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette _of the shoulder and is a stabilizer of the humeral head._
Question 8High Yield
A 58-year-old African-American female who sustained an injury to her upper arm six months ago presents with persistent arm pain. She was initially treated with splinting, with conversion to fracture bracing. She is neurovascularly intact. An injury radiograph and a current radiograph are shown in Figures A and B respectively. What nutritional or metabolic disturbance is the most likely associated with this patient's diagnosis?


Explanation
This patient has sustained a humeral diaphyseal fracture that has gone on to an atrophic nonunion. Vitamin D deficiency is the most likely associated metabolic disturbance.
The incidence of nonunion with non-operative management of humeral shaft injuries ranges from 2-10%. Risk factors include vitamin D deficiency (most common), open fractures, segmental injuries, smoking and obesity. The optimal treatment is compression plating with bone grafting, which has been shown to be superior to intramedullary nailing with bone grafting or compression plating alone.
Ring et al. reviewed factors that contributed to humeral diaphyseal nonunion after fracture bracing. Fractures in the proximal to middle one-third of the shaft or fractures with a spiral/oblique pattern were more likely to go on to nonunion.
Brinker et al. reviewed 37 low-energy fractures that went onto nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having Vitamin D deficiency.
Figure A demonstrates a humeral shaft fracture. Figure B demonstrates an atrophic nonunion of the humeral shaft fracture.
Incorrect Answers:
Answers 1, 2, 3,5: Deficiencies of these options have not been associated with nonunion
The incidence of nonunion with non-operative management of humeral shaft injuries ranges from 2-10%. Risk factors include vitamin D deficiency (most common), open fractures, segmental injuries, smoking and obesity. The optimal treatment is compression plating with bone grafting, which has been shown to be superior to intramedullary nailing with bone grafting or compression plating alone.
Ring et al. reviewed factors that contributed to humeral diaphyseal nonunion after fracture bracing. Fractures in the proximal to middle one-third of the shaft or fractures with a spiral/oblique pattern were more likely to go on to nonunion.
Brinker et al. reviewed 37 low-energy fractures that went onto nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having Vitamin D deficiency.
Figure A demonstrates a humeral shaft fracture. Figure B demonstrates an atrophic nonunion of the humeral shaft fracture.
Incorrect Answers:
Answers 1, 2, 3,5: Deficiencies of these options have not been associated with nonunion
Question 9High Yield
A 78-year-old man is seen in the emergency room 3 hours after a fall from a standing position. The patient sustained a mild scalp laceration and the injury shown in Figure

Explanation
■
The patient has a hyperostotic condition of the cervical spine, most likely ankylosing spondylitis. Because of a rigid and osteoporotic spine, relatively minor falls can result in unstable spinal injuries with significant instability and a high risk for neurologic sequelae. The patient has an unstable injury at C6 with an incomplete spinal cord injury, necessitating urgent decompression and stabilization. Studies have shown that, in patients with ankylosing spondylitis, stand-alone anterior stabilization results in a high failure rate. Halothoracic vests carry a high risk of septic and pulmonary issues, especially in the elderly. Uninstrumented fusion will provide insufficient stability in such patients.
The patient has a hyperostotic condition of the cervical spine, most likely ankylosing spondylitis. Because of a rigid and osteoporotic spine, relatively minor falls can result in unstable spinal injuries with significant instability and a high risk for neurologic sequelae. The patient has an unstable injury at C6 with an incomplete spinal cord injury, necessitating urgent decompression and stabilization. Studies have shown that, in patients with ankylosing spondylitis, stand-alone anterior stabilization results in a high failure rate. Halothoracic vests carry a high risk of septic and pulmonary issues, especially in the elderly. Uninstrumented fusion will provide insufficient stability in such patients.
Question 10High Yield
-A 24-year-old man is involved in a motor vehicle accident at 60 mph. He sustains multiple injuries including an intra-abdominal injury requiring a splenectomy and a closed right femoral shaft fracture.Which variable will best indicate the patient’s resuscitation status when deciding whether to proceed with definitive care of the fracture at the conclusion of the laparotomy?
Explanation
No detailed explanation provided for this question.
Question 11High Yield
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
---
---
---
---







Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through _view, are useful for avoiding this complication._
Question 12High Yield
A 24-year-old white man presents to the emergency department. He was bitten on his fist while fighting with another man. You notice teeth marks on the dorsum of the metacarpophalangeal (MC P) joint of the right middle finger. The bite does not appear to be deep because the joint is not exposed, and you can see the extensor tendon, which seems intact. The patient has active extension at the MC P joint. The wound is red and swollen, but there is no tenderness or redness on the volar aspect of the MC P joint. The patient has some limitation in range of motion. He is afebrile. Radiographs reveal air in the joint but no joint
dislocation or fracture, and there is no neurovascular deficit. All of the following are appropriate steps in the management of this patient except:
dislocation or fracture, and there is no neurovascular deficit. All of the following are appropriate steps in the management of this patient except:
Explanation
Human bite wounds on the hand are typically found over the MP joint. The mechanism of injury is a clenched-fist blow to the mouth. Oral flora enters the wound, which often communicates with the joint. Eikenella corrodens is frequently cultured from human bite wounds, but the most common pathogen is staphylococcus aureus. Appropriate treatment includes the administration of tetanus toxoid, exploration if there is air in the joint or frank infection, observation, intravenous antibiotics, arm elevation, and splinting. All bites over joints should be assumed to penetrate and require formal incision and drainage.
Question 13High Yield
A 58-year-old woman underwent a left total knee arthroplasty 6 years ago. She initially did well after surgery but sustained a fall 2 months ago while at work. She now describes left knee pain and instability and an inability to straighten her knee since the fall. She has been using a hinged knee brace, which provides partial support. On examination, she has passive range of motion of 0° to 115° and active range of motion of 80° to -115°. Her radiographs are shown in Figures 1 through
Explanation
70
The patient has an extensor mechanism disruption with patellar tendon rupture. This injury is treated with extensor mechanism reconstruction in the setting of previous total knee arthroplasty. There is a reported high failure rate with attempted repair. Revision to hinge knee arthroplasty would provide implant stability but would not restore the extensor mechanism. The patient is relatively young and is working, so reconstruction would offer better long-term function than a drop lock brace, which can be better used in low-functioning patients with this type of injury. Extensor mechanism reconstruction historically has been accomplished with allograft material, but a novel technique using synthetic mesh also has proved successful in treating this difficult problem.
The patient has an extensor mechanism disruption with patellar tendon rupture. This injury is treated with extensor mechanism reconstruction in the setting of previous total knee arthroplasty. There is a reported high failure rate with attempted repair. Revision to hinge knee arthroplasty would provide implant stability but would not restore the extensor mechanism. The patient is relatively young and is working, so reconstruction would offer better long-term function than a drop lock brace, which can be better used in low-functioning patients with this type of injury. Extensor mechanism reconstruction historically has been accomplished with allograft material, but a novel technique using synthetic mesh also has proved successful in treating this difficult problem.
Question 14High Yield
What is the most common organism implicated in periprosthetic infection of the shoulder?
Explanation
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
54
54
Question 15High Yield
Which of the following best describes athletic pubalgia?
Explanation
Athletic pubalgia refers to a distinct syndrome of lower abdominal and adductor pain that is mostly commonly seen in high performance male athletes. This condition must be distinguished from others such as painful inflammation of the symphysis pubis, referred to as osteitis pubis. Symptoms attributable to the iliopsoas tendon are most commonly associated with snapping of the tendon. Stress fracture of the pubic ramus may cause symptoms in this area, but it is usually confirmed by imaging studies. Neurapraxia of the pudendal nerve is associated with pressure from the seat in cycling sports and also as a complication associated with traction during surgical procedures.
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 16High Yield
Placing the starting point for an antegrade femoral nail too anterior to the axis of the medullary canal can most commonly lead to what intraoperative complication?
Explanation
Usage of an anterior starting point that is too anterior leads to creation of significant hoop stresses in the proximal segment, potentially leading to iatrogenic fracture of the proximal segment. The referenced study by Johnson et al reviews the topic of femoral bursting and he notes that even shifting 6mm too far anteriorly can lead to proximal femoral fracture creation. He also reported that overreaming the canal by at least 0.5mm diameter is necessary to decrease hoop stresses throughout the femur, likely due to a mismatch in the radius of curvature of the femur and intramedullary nail.
Question 17High Yield
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
33
33
Explanation
The patient's radiographs demonstrate bone loss of the medial humeral head. He has risk factors for both septic arthritis/osteomyelitis, and metastatic cancer, and it is important to understand the extent of his pathology before moving forward with surgical intervention. An MRI scan would assist in the diagnosis and demonstrate the extent of disease/tissue involvement. Administration of IV antibiotics prior to obtaining appropriate cultures would decrease the success rate of treatment in the setting of infection, and mistreat the pathology in the setting of metastasis. Similarly, obtaining cultures from the draining sinus tract would fail to account for the possible tumor diagnosis and may result in inaccurate culture results.
Question 18High Yield
A 4-year-old girl has knee pain after a fall. Examination reveals tenderness about the proximal tibia with modest deformity. She has no neurovascular deficits. A radiograph is seen in Figure 24. What should her parents be told?
Explanation
The patient has a so-called Cozen fracture, and she is at significant risk for a posttraumatic genu valgum deformity. However, long-term studies have shown that when such a deformity occurs, it frequently resolves spontaneously and therefore surgical intervention to try and prevent the deformity is not advised.
REFERENCES: Jordan SE, Alonso JE, Cook FF: The etiology of valgus angulation after metaphyseal fractures of the tibia in children. J Pediatr Orthop 1987;7:450-457.
Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone
Joint Surg Am 1999;81:799-810.
REFERENCES: Jordan SE, Alonso JE, Cook FF: The etiology of valgus angulation after metaphyseal fractures of the tibia in children. J Pediatr Orthop 1987;7:450-457.
Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone
Joint Surg Am 1999;81:799-810.
Question 19High Yield
Which of the following statements best describes how unicompartmental knee arthroplasty (UKA) differs from total knee arthroplasty (TKA)?
Explanation
DISCUSSION: Because UKA does not require cruciate sacrifice, patellofemoral resurfacing, or rotational changes to the femur or tibia, it reliably recreates normal knee kinematics. UKAs have generally demonstrated higher reoperation rates than TKAs at intermediate and long-term follow-up, due in part to progression of arthritis in the nonresurfaced compartments. Mobile bearings have been clinically successful in both UKA and TKA.
REFERENCES: Patil S, Colwell CW Jr, Ezzet KA, et al: Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 2005;87:332-338.
Gioe TJ, Killeen KK, Hoeffel DP, et al: Analysis of unicompartmental knee arthroplasty in a community- based implant registry. Clin Orthop Relat Res 2003;416:111-119.
REFERENCES: Patil S, Colwell CW Jr, Ezzet KA, et al: Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 2005;87:332-338.
Gioe TJ, Killeen KK, Hoeffel DP, et al: Analysis of unicompartmental knee arthroplasty in a community- based implant registry. Clin Orthop Relat Res 2003;416:111-119.
Question 20High Yield
Which finger is most commonly involved in a flexor digitorum profundus (FDP) avulsion injury:
Explanation
An FDP avulsion is caused by forceful extension of the distal interphalangeal (DIP) joint, occurring at the same time as a maximum contraction of the FDP tendon. Jersey finger is often seen in athletes, especially football or rugby players, who commonly get their fingers caught in an opposing playerâs jersey, thus the name. In most cases, this injury affects the ring finger.
Question 21High Yield
Which of the following best describes the pathologic anatomy of cam impingement of the hip?
Explanation
DISCUSSION: Cam impingement creates shearing forces that result in an outside-in directed detachment of the labrum in the anterosuperior quadrant. Retroversion of the acetabulum is associated with pincer
impingement. The impingement is exhibited with hip flexion. Cam impingement involves a morphologic abnormality of the femoral head. Pincer lesions result from stresses of a normal femoral neck against an abnormal acetabular rim. Cam impingement is not associated with osteonecrosis.
REFERENCES: Jaberi FM, Parvizi J: Hip pain in young adults: Femoroacetabular impingement. J Arthroplasty 2007:22;37-42.
Byrd JW: The role of hip arthroscopy in the athletic hip. Clin Sports Med 2006:25;255-278.
Beck M, Kalhor M, Leunig M, et al: Hip morphology influences the pattern of damage to the acetabular
cartilage: Femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005:87; 1012-1018.
impingement. The impingement is exhibited with hip flexion. Cam impingement involves a morphologic abnormality of the femoral head. Pincer lesions result from stresses of a normal femoral neck against an abnormal acetabular rim. Cam impingement is not associated with osteonecrosis.
REFERENCES: Jaberi FM, Parvizi J: Hip pain in young adults: Femoroacetabular impingement. J Arthroplasty 2007:22;37-42.
Byrd JW: The role of hip arthroscopy in the athletic hip. Clin Sports Med 2006:25;255-278.
Beck M, Kalhor M, Leunig M, et al: Hip morphology influences the pattern of damage to the acetabular
cartilage: Femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005:87; 1012-1018.
Question 22High Yield
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of
Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is
not indicated.
REFERENCES: Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
not indicated.
REFERENCES: Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Question 23High Yield
A 23-year-old woman with a bilateral leg and foot deformity presents for evaluation. She has weakness in the foot and ankle, giving way of the ankle, and difficulty with exercise activities. She mentions that both her brother and uncle have similar problems and deformities with their limbs. On examination, she has a cavovarus foot deformity and muscle weakness. The most likely combination of muscle loss is:
Explanation
By history, this patient has hereditary sensorimotor neuropathy (C harcot-Marie-Tooth disorder). Historically referred to as peroneal muscular atrophy, this condition initially affects the peroneus brevis, followed by the intrinsic and anterior tibial muscles. Other patterns of deformity and muscle loss are occasionally present.
Question 24High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 25High Yield
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate.
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
Question 26High Yield
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
Congenital dislocation of the radial head is often confused with posttraumatic dislocation. The distinguishing feature here is the dome-shaped radial head. Some patients with congenital anomalies fail to recognize their limitations until an injury occurs. Soft-tissue contractures do not cause radial head dislocation nor do they usually cause this pattern of motion restriction (mainly flexion and rotation without significant loss of extension). There is no deformity of the ulna to suggest an old Monteggia lesion.
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Bell SN, Morrey BF, Bianco AJ Jr: Chronic posterior subluxation and dislocation of the radial head. J Bone Joint Surg Am 1991;73:392-396.
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Bell SN, Morrey BF, Bianco AJ Jr: Chronic posterior subluxation and dislocation of the radial head. J Bone Joint Surg Am 1991;73:392-396.
Question 27High Yield
When a patient has acute or chronic anterior shoulder instability, a bony or glenoid reconstructive procedure should be considered in which clinical setting?
Explanation
HAGL lesions may be initially treated without surgery. Recurrent instability in the setting of a HAGL lesion may be treated with a soft-tissue repair. A nonengaging or nontracking Hill-Sachs lesion may be treated with an anterior soft-tissue (Bankart) repair. A tracking or engaging lesion may be treated with a bony glenoid procedure or a soft-tissue procedure plus remplissage. An ALPSA lesion may be treated with a soft-tissue procedure unless it is associated with a glenoid bony defect exceeding 25%. A glenoid bony defect exceeding 25% is associated with substantially higher recurrence than defects smaller than 20%, and consideration for bony glenoid reconstruction is advised.
RECOMMENDED READINGS
73. [Beran MC, Donaldson CT, Bishop JY. Treatment of chronic glenoid defects in the setting of recurrent anterior shoulder instability: a systematic review. J Shoulder Elbow Surg. 2010 Jul;19(5):769-80. doi: 10.1016/j.jse.2010.01.011. Epub 2010 Apr 14. Review. PubMed PMID: 20392650. ](http://www.ncbi.nlm.nih.gov/pubmed/20392650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20392650)
74. [Boileau P, Villalba M, Héry JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006 Aug;88(8):1755-63. PubMed PMID: 16882898. ](http://www.ncbi.nlm.nih.gov/pubmed/16882898)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16882898)
RECOMMENDED READINGS
73. [Beran MC, Donaldson CT, Bishop JY. Treatment of chronic glenoid defects in the setting of recurrent anterior shoulder instability: a systematic review. J Shoulder Elbow Surg. 2010 Jul;19(5):769-80. doi: 10.1016/j.jse.2010.01.011. Epub 2010 Apr 14. Review. PubMed PMID: 20392650. ](http://www.ncbi.nlm.nih.gov/pubmed/20392650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20392650)
74. [Boileau P, Villalba M, Héry JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006 Aug;88(8):1755-63. PubMed PMID: 16882898. ](http://www.ncbi.nlm.nih.gov/pubmed/16882898)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16882898)
Question 28High Yield
A 26-year-old ballet dancer reports posterolateral ankle pain, especially with maximal plantar flexion. Examination reveals maximal tenderness just posterior to the lateral malleolus, and symptoms are heightened with forced passive plantar flexion. Radiographs are shown in Figures 42a and 42b. What is the most likely cause of the patient’s symptoms?
Explanation
The patient has a symptomatic os trigonum caused by impingement that occurs with maximal plantar flexion of the ankle in the demi-pointe or full-pointe position. Patients frequently report posterolateral pain localized behind the lateral malleolus that may be misinterpreted as a disorder of the peroneal tendon. Pain with passive plantar flexion (the plantar flexion sign) indicates posterior impingement, not a problem with the peroneal tendon. The symptoms are not characteristic of a stress fracture, nor do the radiographs show a stress fracture or an osteochondritis dissecans lesion. The os trigonum is modest in its dimensions. The incidence or magnitude of symptoms does not correlate with the size of the fragment. Large fragments may be asymptomatic, while small lesions may create significant symptoms.
REFERENCES: Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Hamilton WG: Foot and ankle injuries in dancers, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1241-1276.
REFERENCES: Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Hamilton WG: Foot and ankle injuries in dancers, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1241-1276.
Question 29High Yield
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
Explanation
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit.
Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon repair causes limited flexion of the injured finger.
RECOMMENDED READINGS
14. Malerich MM, Baird RA, McMaster W, Erickson JM. Permissible limits of flexor digitorum profundus tendon advancement--an anatomic study. J Hand Surg Am. 1987 Jan; 12(1):30-3. PubMed PMID: 3805640. View Abstract at PubMed
15. Schreuders TA. The quadriga phenomenon: a review and clinical relevance. J Hand Surg Eur Vol. 2012 Jul;37(6):513-22. doi: 10.1177/1753193411430810. Epub 2011 Dec 14. Review.
PubMed PMID: 22170246. View Abstract at PubMed
Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon repair causes limited flexion of the injured finger.
RECOMMENDED READINGS
14. Malerich MM, Baird RA, McMaster W, Erickson JM. Permissible limits of flexor digitorum profundus tendon advancement--an anatomic study. J Hand Surg Am. 1987 Jan; 12(1):30-3. PubMed PMID: 3805640. View Abstract at PubMed
15. Schreuders TA. The quadriga phenomenon: a review and clinical relevance. J Hand Surg Eur Vol. 2012 Jul;37(6):513-22. doi: 10.1177/1753193411430810. Epub 2011 Dec 14. Review.
PubMed PMID: 22170246. View Abstract at PubMed
Question 30High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve.
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
Question 31High Yield
A 68-year-old right-hand dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
Explanation
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
36
36
Question 32High Yield
Which of the following is the most cost-effective method of screening for idiopathic hypertrophic cardiomyopathy?
Explanation
DISCUSSION: Idiopathic hypertrophic cardiomyopathy is the leading cause of sudden cardiac death in athletes. The diagnosis is made with an echocardiogram; however, echocardiograms have not been shown to be a cost-effective screening tool for this condition. The most cost-effective method of screening for this condition includes obtaining a history of chest pain or syncope in the athlete, or a family history of early cardiac death. It has been estimated that it would cost over $500,000 to diagnose one case of hypertrophic cardiomyopathy if screening echocardiograms were used. Auscultation of the heart and heart sounds can be normal in an athlete at rest with this condition, and a stress test will not help diagnose idiopathic hypertrophic cardiomyopathy.
REFERENCES: Bader RS, Goldberg L, Sahn DJ: Risk of sudden death in young athletes: Which screening strategies are appropriate? Pediatr Clin North Am 2004;51:1421 -1441.
Maron BJ, Thompson PD, Ackerman MJ, et al: Recommendations and considerations related to prepar- ticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: A scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: Endorsed by the American College of Cardiology Foundation. Circulation 2007;115:1643-1655.
DISCUSSION: Idiopathic hypertrophic cardiomyopathy is the leading cause of sudden cardiac death in athletes. The diagnosis is made with an echocardiogram; however, echocardiograms have not been shown to be a cost-effective screening tool for this condition. The most cost-effective method of screening for this condition includes obtaining a history of chest pain or syncope in the athlete, or a family history of early cardiac death. It has been estimated that it would cost over $500,000 to diagnose one case of hypertrophic cardiomyopathy if screening echocardiograms were used. Auscultation of the heart and heart sounds can be normal in an athlete at rest with this condition, and a stress test will not help diagnose idiopathic hypertrophic cardiomyopathy.
REFERENCES: Bader RS, Goldberg L, Sahn DJ: Risk of sudden death in young athletes: Which screening strategies are appropriate? Pediatr Clin North Am 2004;51:1421 -1441.
Maron BJ, Thompson PD, Ackerman MJ, et al: Recommendations and considerations related to prepar- ticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: A scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: Endorsed by the American College of Cardiology Foundation. Circulation 2007;115:1643-1655.
Question 33High Yield
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic
symptomatic osteoarthritis, what outcome has been demonstrated?
symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
times between 1 week and 2 years after surgery.
Question 34High Yield
Figure 1 is the clinical photograph and Video 1 is the nonarthrographic sagittal plane MRI scan of a 23-year-old male active duty Marine who presents with 3 months of pain and weakness in his nondominant arm. He states that he had rapid onset of “severe” left shoulder pain, which has recently subsided followed closely by weakness in that arm. There was no antecedent trauma that he can recall. Upon further questioning, he states he had one episode of a brief cold sometime prior to the development of symptoms, but he is uncertain. On examination, he is weak in forward flexion and external rotation at 0° of abduction, but otherwise he is neurologically intact. The EMG result is abnormal. What is the best next step?
Explanation
The patient is exhibiting a motor mononeuropathy that does not follow a radicular pattern. In the absence of a space-filling lesion, e.g., a paralabral cyst at the suprascapular notch or, more commonly, at the spinoglenoid notch (which this patient does not have on MRI), at this time, the patient’s diagnosis is most consistent with neuralgic amyotrophy (NA) - i.e Parsonage-Turner syndrome. NA is reported to be quite rare, with a range of about 20 to 30 cases in 100,000 individuals. Although a hereditary form exists, it is much rarer (and severe), with most cases being idiopathic. Causes are unknown but generally it is thought to be autoimmune in nature and can be triggered by viral illness, as well as other noninfectious triggers..
69
Presentation is variable but most commonly affects males and nerves emanating from the upper trunk of the brachial plexus. Typically, the nerves affected are motor and usually, it is a unilateral presentation. The process is usually self-limiting within a 6-month period, but residual deficits can be seen as far out as 3 years from initial presentation. MRI is very sensitive to inflammation in the affected muscles and EMG is typically abnormal along the specific nerve affected. Typically, the best treatment in this time frame is benign neglect, with physical therapy helpful in maintaining range of motion of the affected joint (usually the shoulder) and treatment of the periscapular muscles that are usually being overused to establish function in the affected limb.
Physical examination and these supporting studies differentiate this condition from cervical radiculopathies. An arthroscopic or open decompression of the suprascapular notch may be indicated if no improvement is seen within 6 months of onset of symptoms
69
Presentation is variable but most commonly affects males and nerves emanating from the upper trunk of the brachial plexus. Typically, the nerves affected are motor and usually, it is a unilateral presentation. The process is usually self-limiting within a 6-month period, but residual deficits can be seen as far out as 3 years from initial presentation. MRI is very sensitive to inflammation in the affected muscles and EMG is typically abnormal along the specific nerve affected. Typically, the best treatment in this time frame is benign neglect, with physical therapy helpful in maintaining range of motion of the affected joint (usually the shoulder) and treatment of the periscapular muscles that are usually being overused to establish function in the affected limb.
Physical examination and these supporting studies differentiate this condition from cervical radiculopathies. An arthroscopic or open decompression of the suprascapular notch may be indicated if no improvement is seen within 6 months of onset of symptoms
Question 35High Yield
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
The development of arthritis in SLAC wrist follows a consistent pattern. Beginning at the radial styloid to the scaphoid articulation, it progresses through the entire radioscaphoid joint and the midcarpal joint. In all stages, the radiolunate joint is spared, which is the basis for a scaphoid excision and four-corner fusion performed as a motion-sparing procedure for treatment of this condition.
REFERENCES: Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281.
Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Watson HK, Ryu J: Evolution of arthritis of the wrist. Clin Orthop 1986;202:57-67.
REFERENCES: Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281.
Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Watson HK, Ryu J: Evolution of arthritis of the wrist. Clin Orthop 1986;202:57-67.
Question 36High Yield
The risk of malignant transformation in patients with multiple hereditary exostoses is:
Explanation
The rate of malignant transformation in patients with multiple hereditary exostoses is variable and is generally reported between
0.5% to 25%.
0.5% to 25%.
Question 37High Yield
Figures 91a through 91c are the radiographs of a 10-year-old boy who has a 6-month history of progressive heel pain. The patient is a year-round soccer player and now experiences pain with most every step. What is the most appropriate management?
Explanation
The patient has calcaneal apophysitis, an overuse syndrome common in children ages 9 to12 years. Symptoms are usually the result of excess tension and a tight heel cord. Management includes activity modification, as well as heel cord stretching, nonsteroidal anti-inflammatory drugs, icing, and other modalities. Radiographs are typically negative; MRI is unnecessary. Custom orthotics are not indicated. The condition is self-limiting, in that the symptoms fully resolve once the apophyses fuses,such that surgery is rarely indicated.
Question 38High Yield
Optimal treatment for a symptomatic ganglion is:
Explanation
Surgical excision of a symptomatic ganglion, with removal of the entire ganglion stalk and a portion of the joint capsule at its base, reliably relieves pain and has a low recurrence rate (approximately 5%). C losed rupture, while potentially effective, has a recurrence rate of approximately 50%. Ganglions are prone to recur after aspiration, although 3 serial aspirations of a ganglion have been shown to reduce the recurrence rate to about 15%. The addition of corticosteroids to aspiration treatment has not been shown to provide any additional benefit. While observation of painless ganglions is certainly acceptable treatment given their benign prognosis, it is not considered the optimal course for a symptomatic lesion.
Question 39High Yield
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
An immediate appointment for magnetic resonance imagine (MRI) and computed tomography (C T) scan are not available, and a genetic evaluation has been carried out previously. As you await the report from the geneticist office, you decide to get a skeletal radiograph series on the patient. The radiograph of the opposite forearm (Slide 1) and right leg are shown (Slide 2).
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 3). Your suspected diagnosis is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
An immediate appointment for magnetic resonance imagine (MRI) and computed tomography (C T) scan are not available, and a genetic evaluation has been carried out previously. As you await the report from the geneticist office, you decide to get a skeletal radiograph series on the patient. The radiograph of the opposite forearm (Slide 1) and right leg are shown (Slide 2).
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 3). Your suspected diagnosis is:
Explanation
Diaphyseal achalasia, also called multiple hereditary exostoses, classically presents in a young individual with multiple sites of involvement. The more involved the disease, the more likely hand involvement becomes. Forearm involvement is also common. The radius is bowed due to the shortened ulna. The risk of radial head dislocation is higher if the radius does not bow. While infection or traumatic injury could have produced early physeal arrest as seen in the first radiograph, presence of lesions elsewhere indicates multiple hereditary exostoses and should be investigated with skeletal surveys. Multiple epiphyseal dysplasia is not a possible diagnosis as only the ulna is involved in the first radiograph and radius alone in the left forearm. No enchondromas are present.
Question 40High Yield
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season.
REFERENCES: Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Cantu RC: Criteria for return to competition after closed head injury, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby, 1991.
REFERENCES: Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Cantu RC: Criteria for return to competition after closed head injury, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby, 1991.
Question 41High Yield
..Figure 33 is the radiograph of a 27-year-old bicyclist who crashes. He has an isolated and closed injury. He is neurovascularly intact in the upper extremity. The lateral fragment is displaced inferiorly by

Explanation
- gravity.
Question 42High Yield
A 10-year-old boy hit a tree with his sled and is seen in the emergency department with extreme left hip pain and inability to ambulate. He has no history of pain in the left groin, thigh, or knee. Radiographs are seen in Figures 29a and 29b. What is the most common complication resulting from this injury?
Explanation
DISCUSSION: The child has a type I hip fracture without associated dislocation. This is an acute hip fracture through the proximal femoral physis, and can occur with or without associated dislocation. He had no prodrome of hip or thigh pain and no femoral neck changes to indicate that this is an unstable slipped capital femoral epiphysis. Osteonecrosis in these transepiphyseal hip fractures is the most common and most devastating complication. The rate of osteonecrosis is most dependent on the initial displacement of the fracture. These fractures should be treated emergently, and decompression of the hip joint is recommended by many authors.
REFERENCES: Moon ES, Mehlman CT: Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta analysis of 360 cases. J Orthop Trauma 2006;20:323-329. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
**2010 Pediatric Orthopaedic Examination Answer Book • 29**
REFERENCES: Moon ES, Mehlman CT: Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta analysis of 360 cases. J Orthop Trauma 2006;20:323-329. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
**2010 Pediatric Orthopaedic Examination Answer Book • 29**
Question 43High Yield
A 4-year-old girl falls off a swing and injures her right elbow. The radiographs are shown in Figures 88a and 88b. What is the most likely diagnosis?
Explanation
DISCUSSION: To accurately diagnose skeletal injuries around the elbow in children, the practitioner must be knowledgeable about the progressive ossification centers. In this case, at age 4 years, a female will have a partially ossified capitellum, radial head, and medial epicondyle. The trochlea, olecranon, and lateral epicondyle ossification centers should remain fully cartilaginous at this stage of development. The irregularity in the area of the olecranon on the radiograph represents a displaced fracture requiring accurate reduction and fixation to ensure restoration of articular congruity and full elbow function. The presence of a posterior fat pad sign on the radiograph is indicative of a traumatic effusion, but there is an identifiable fracture in this patient. Olecranon fractures are commonly seen in children with osteogenesis imperfecta.
REFERENCES: Cheng JC, Wing-Man K, Shen WY, et al: A new look at the sequential development of elbow-ossification centers in children. J Pediatr Orthop 1998;18:161-167.
Parent S, Wedemeyer M, Mahar AT, et al: Displaced olecranon fractures in children: A biomechanical analysis of fixation methods. J Pediatr Orthop 2008;28:147-151.
Beaty JH, Kasser JR (eds): Rockwood and Green’s Fractures in Children, ed 6. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 591-660.
74 • American Academy of Orthopaedic Surgeons
REFERENCES: Cheng JC, Wing-Man K, Shen WY, et al: A new look at the sequential development of elbow-ossification centers in children. J Pediatr Orthop 1998;18:161-167.
Parent S, Wedemeyer M, Mahar AT, et al: Displaced olecranon fractures in children: A biomechanical analysis of fixation methods. J Pediatr Orthop 2008;28:147-151.
Beaty JH, Kasser JR (eds): Rockwood and Green’s Fractures in Children, ed 6. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 591-660.
74 • American Academy of Orthopaedic Surgeons
Question 44High Yield
A 2½-year-old boy has severe spastic diplegia and hips that are subluxating. His abduction is 20° on each side. The migration index is 35% on each side. Recommended treatment includes:
Explanation
If followed by postoperative bracing, lengthening of the adductors is usually successful in children younger than 4 to 6 years of age.
Traction would not be appropriate because the muscles are spastic. The surgical plan does not include the most important component â weakening the overactive adductors.
Trochanteric transfer is not advisable in patients younger than 8 years old. Trochanteric transfer would not help decrease the overpull of the adductors which is the cause of the subluxation.
Nighttime abduction splinting should be a component of the care after surgery. Bracing alone would not be an adequate treatment.
Physical therapy in the absence of surgery does not seem to be enough to overcome the pull of the adductors.
Traction would not be appropriate because the muscles are spastic. The surgical plan does not include the most important component â weakening the overactive adductors.
Trochanteric transfer is not advisable in patients younger than 8 years old. Trochanteric transfer would not help decrease the overpull of the adductors which is the cause of the subluxation.
Nighttime abduction splinting should be a component of the care after surgery. Bracing alone would not be an adequate treatment.
Physical therapy in the absence of surgery does not seem to be enough to overcome the pull of the adductors.
Question 45High Yield
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
The initial stages of posterior tibial tendon insufficiency, where the deformity remains supple, may be treated with bracing or an orthotic for pain relief. The Arizona brace was introduced in 1988, and assists in pain relief and deformity correction by minimizing hindfoot valgus alignment, lateral calcaneal displacement, and medial ankle collapse. It is particularly helpful in those patients with advanced disease that cannot tolerate an ankle-foot orthosis. All other choices are incorrect because of the addition of lateral posting, which is not advantageous in valgus deformities. The addition of medial posting to any of the above choices would render them correct alternatives. A heel lift is applicable in Achilles tendon disorders, not posterior tibial tendon disorders.
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 46High Yield
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion.
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 47High Yield
Figures 47a and 47b are the radiograph and axial CT section of a 73-year-old woman with metastatic lung cancer who has a painful left periacetabular lesion. She is a high-risk surgical candidate because of a prior pneumonectomy and progressive metastatic disease of her remaining lung. Palliative radiation is recommended. Two regimens are being considered: a single fraction of 8 Gy or 15 fractions of a 30-Gy cumulative dose over 3 weeks. Compared to the multifraction regimen, the 8-Gy single fraction is associated with

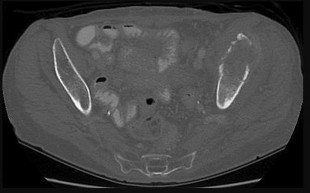
Explanation
Multiple prospective randomized controlled trials have evaluated single vs multifraction radiation regimens for the treatment of painful bone metastases. All studies have demonstrated equivalent pain relief. Retreatment rates are higher with single-fraction dosing, but it is unknown if this is
because of higher rates of recurrent pain with single fractions or reluctance of radiation oncologists to give additional radiation when multifraction regimens with higher cumulative doses have failed. Single-fraction radiation is less expensive and more convenient for patients. The American Board of Internal Medicine Foundation’s Choosing Wisely® campaign to encourage physician leadership in reducing harmful or inappropriate resource use selected “Don’t recommend more than a single fraction of palliative radiation for an uncomplicated painful bone metastasis” as 1 of the “5 things physicians and patients should question in hospice and palliative medicine.”
RECOMMENDED READINGS
31. [Fischberg D, Bull J, Casarett D, Hanson LC, Klein SM, Rotella J, Smith T, Storey CP Jr, Teno JM, Widera E; HPM Choosing Wisely Task Force. Five things physicians and patients should question in hospice and palliative medicine. J Pain Symptom Manage. 2013 Mar;45(3):595-605. doi: 10.1016/j.jpainsymman.2012.12.002. Epub 2013 Feb 22. ](http://www.ncbi.nlm.nih.gov/pubmed/23434175)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23434175)
32. [Dennis K, Makhani L, Zeng L, Lam H, Chow E. Single fraction conventional external beam radiation therapy for bone metastases: a systematic review of randomised controlled trials. Radiother Oncol. 2013 Jan;106(1):5-14. doi: 10.1016/j.radonc.2012.12.009. Epub 2013 Jan 13. Review. PubMed PMID: 23321492. ](http://www.ncbi.nlm.nih.gov/pubmed/23321492)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23321492)
33. [Hartsell WF, Konski AA, Lo SS, Hayman JA. Single fraction radiotherapy for bone metastases: clinically effective, time efficient, cost conscious and still underutilized in the United States? Clin Oncol (R Coll Radiol). 2009 Nov;21(9):652-4. doi: 10.1016/j.clon.2009.08.003. Epub 2009 Sep 9. PubMed PMID: 19744843. ](http://www.ncbi.nlm.nih.gov/pubmed/19744843)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19744843)
because of higher rates of recurrent pain with single fractions or reluctance of radiation oncologists to give additional radiation when multifraction regimens with higher cumulative doses have failed. Single-fraction radiation is less expensive and more convenient for patients. The American Board of Internal Medicine Foundation’s Choosing Wisely® campaign to encourage physician leadership in reducing harmful or inappropriate resource use selected “Don’t recommend more than a single fraction of palliative radiation for an uncomplicated painful bone metastasis” as 1 of the “5 things physicians and patients should question in hospice and palliative medicine.”
RECOMMENDED READINGS
31. [Fischberg D, Bull J, Casarett D, Hanson LC, Klein SM, Rotella J, Smith T, Storey CP Jr, Teno JM, Widera E; HPM Choosing Wisely Task Force. Five things physicians and patients should question in hospice and palliative medicine. J Pain Symptom Manage. 2013 Mar;45(3):595-605. doi: 10.1016/j.jpainsymman.2012.12.002. Epub 2013 Feb 22. ](http://www.ncbi.nlm.nih.gov/pubmed/23434175)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23434175)
32. [Dennis K, Makhani L, Zeng L, Lam H, Chow E. Single fraction conventional external beam radiation therapy for bone metastases: a systematic review of randomised controlled trials. Radiother Oncol. 2013 Jan;106(1):5-14. doi: 10.1016/j.radonc.2012.12.009. Epub 2013 Jan 13. Review. PubMed PMID: 23321492. ](http://www.ncbi.nlm.nih.gov/pubmed/23321492)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23321492)
33. [Hartsell WF, Konski AA, Lo SS, Hayman JA. Single fraction radiotherapy for bone metastases: clinically effective, time efficient, cost conscious and still underutilized in the United States? Clin Oncol (R Coll Radiol). 2009 Nov;21(9):652-4. doi: 10.1016/j.clon.2009.08.003. Epub 2009 Sep 9. PubMed PMID: 19744843. ](http://www.ncbi.nlm.nih.gov/pubmed/19744843)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19744843)
Question 48High Yield
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is
Explanation
Diabetes mellitus has been associated with resistant cases of adhesive capsulitis. With other causes of onset, adhesive capsulitis frequently responds to nonsurgical management such as stretching exercises or, when this fails, manipulation under anesthesia and/or arthroscopic release. Manipulation is rarely successful for the treatment of adhesive capsulitis associated with diabetes mellitus, and arthroscopic release may be preferred.
REFERENCES: Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146.
Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
REFERENCES: Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146.
Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 49High Yield
Slide 1
A 29-year-old woman presents for treatment of a swollen foot. Although her foot is not painful, it has been swollen for 2 weeks. The patient walks into the office without any assistive device. On examination, the foot is swollen and warm. The patient does not have protective sensation in the foot, and she denies a history of diabetes and does not have a clinically relevant medical
history. A radiograph of her foot is presented (Slide). Which of the following tests will be most helpful in determining the etiology of her condition:
A 29-year-old woman presents for treatment of a swollen foot. Although her foot is not painful, it has been swollen for 2 weeks. The patient walks into the office without any assistive device. On examination, the foot is swollen and warm. The patient does not have protective sensation in the foot, and she denies a history of diabetes and does not have a clinically relevant medical
history. A radiograph of her foot is presented (Slide). Which of the following tests will be most helpful in determining the etiology of her condition:
Explanation
This patient most likely has diabetes. Patients may present for the first time with an acute neuroarthropathy of the foot as a result of diabetes, even without a clinical history of the disease. Although the sedimentation rate will likely be elevated, it will not help in the diagnosis. Infection is not a likely consideration in this patient.
Question 50High Yield
..If the patient were a college pitcher with a similar presentation and examination, what structure would most likely be injured?
Explanation
- Plain radiographs of both elbows PREFERRED RESPONSE: 1- To evaluate for apophyseal injury PREFERRED RESPONSE: 1- Ulnar collateral ligament
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon