Orthopedic With Answer Anatomy Review | Dr Hutaif Basic -...
14 Apr 2026
108 min read
71 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer Anatomy Review | Dr Hu...
00:00
Start Quiz
Question 1High Yield
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

Explanation
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
Question 2High Yield
An 82-year-old woman presents for treatment of a painful second toe deformity. The toe is subluxated at the metatarsophalangeal (MP) joint, and a fixed claw toe deformity is present. Despite severe hallux valgus, and the hallux under riding the second toe, the hallux and bunion are not symptomatic. The procedure that will ideally correct this deformity is:
Explanation
This elderly patient has a symptomatic second toe deformity only, and surgery to the hallux should be avoided if possible. This is a common clinical problem, and although patients do not readily accept amputation of the toe, it is the preferred procedure because it does not involve reconstruction of the hallux. C orrection of the second toe without amputation will not work unless the hallux deformity is addressed.
Question 3High Yield
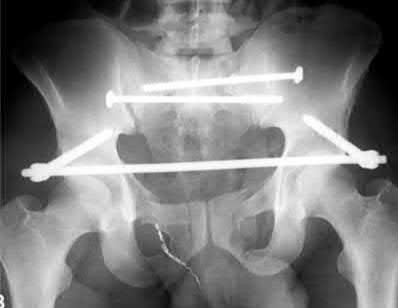
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?

Explanation
This patient was treated with posterior stabilization, and an anterior subcutaneous internal fixator (ASIF). The most common neurologic injury seen following placement of the ASIF construct is irritation of the lateral femoral cutaneous nerve (LFCN), causing numbness and/or pain of the lateral thigh.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Answer 1: Weakness of hip flexion would be due to injury to the femoral nerve, which is not commonly associated with this construct.
Answer 2: Weakness of ankle dorsiflexion would be due to injury to the L5 nerve root, which does not occur due to ASIF placement.
Answer 3: Numbness of the medial thigh is due to injury to the obturator nerve, which is not commonly associated with this construct.
Answer 5: Numbness of the perineum is due to injury to the sacral nerve roots, which is not commonly associated with this construct.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Answer 1: Weakness of hip flexion would be due to injury to the femoral nerve, which is not commonly associated with this construct.
Answer 2: Weakness of ankle dorsiflexion would be due to injury to the L5 nerve root, which does not occur due to ASIF placement.
Answer 3: Numbness of the medial thigh is due to injury to the obturator nerve, which is not commonly associated with this construct.
Answer 5: Numbness of the perineum is due to injury to the sacral nerve roots, which is not commonly associated with this construct.
Question 4High Yield
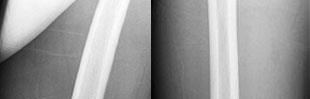
A 28-year-old male sustains the injury seen in Figure A. After discussing the risks and benefits of surgery, he elects to pursue nonoperative treatment. Of the following possible complications from nonoperative treatment, which is the most likely?

Explanation
In a patient with a displaced and shortened middle third clavicle fracture, nonunion would be expected to occur more often than any of the other complications listed.
The risk of nonunion following mid-shaft clavicle fractures is increased with
advanced age, female gender, displacement, and comminution ("Z-deformity"). Nonoperative management of mid-shaft clavicle fractures has also been associated with decreased shoulder strength and endurance.
Furthermore, range of motion and shoulder strength have not been shown to be sufficiently different between operative and nonoperative management.
Hoogervorst et al. reviewed the treatment of mid-shaft clavicle fractures. They cite that the rate of nonunion for fractures treated nonoperatively is about 15%. The authors note that those with >2cm of shortening and displacement
>100% of the shaft width are at a greater risk for nonunion and that nearly 66% of those who go on to nonunion eventually undergo surgical repair.
Robinson et al. performed a prospective observational cohort study to evaluate the prevalence of and risk factors for nonunion of clavicle fractures treated nonoperatively. They found that the risk of nonunion was significantly increased by advancing age, female gender, displacement of the fracture, and the presence of comminution.
Figure A shows a radiograph demonstrating a middle third clavicle shaft fracture with >100% displacement and >2cm shortening.
Incorrect Answers:
Answer 1: The rate of skin necrosis following nonoperative treatment has not been shown to be higher than nonunion.
Answer 3: The rate of complex regional pain syndrome (CRPS) was shown to be around 2% in nonoperatively treated patients.
Answer 4 ad 5: Sternoclavicular arthritis and acromioclavicular arthritis or abnormalities have been shown to be somewhere between 4-6%
The risk of nonunion following mid-shaft clavicle fractures is increased with
advanced age, female gender, displacement, and comminution ("Z-deformity"). Nonoperative management of mid-shaft clavicle fractures has also been associated with decreased shoulder strength and endurance.
Furthermore, range of motion and shoulder strength have not been shown to be sufficiently different between operative and nonoperative management.
Hoogervorst et al. reviewed the treatment of mid-shaft clavicle fractures. They cite that the rate of nonunion for fractures treated nonoperatively is about 15%. The authors note that those with >2cm of shortening and displacement
>100% of the shaft width are at a greater risk for nonunion and that nearly 66% of those who go on to nonunion eventually undergo surgical repair.
Robinson et al. performed a prospective observational cohort study to evaluate the prevalence of and risk factors for nonunion of clavicle fractures treated nonoperatively. They found that the risk of nonunion was significantly increased by advancing age, female gender, displacement of the fracture, and the presence of comminution.
Figure A shows a radiograph demonstrating a middle third clavicle shaft fracture with >100% displacement and >2cm shortening.
Incorrect Answers:
Answer 1: The rate of skin necrosis following nonoperative treatment has not been shown to be higher than nonunion.
Answer 3: The rate of complex regional pain syndrome (CRPS) was shown to be around 2% in nonoperatively treated patients.
Answer 4 ad 5: Sternoclavicular arthritis and acromioclavicular arthritis or abnormalities have been shown to be somewhere between 4-6%
Question 5High Yield
A 68-year-old woman who underwent left total hip arthroplasty 14 years ago now reports pain in her thigh. A radiograph is shown in Figure 14. What is the most reliable method for reconstructing the femoral component?

Explanation
DISCUSSION: The patient has a loose, cemented femoral component. The proximal femur is deficient and may not have adequate strength to support a proximally porous-coated cementless implant. Cemented hip implants have shown higher rates of failure when used for revision surgery. An extensively coated, cementless stem that engages the diaphysis has been shown to have excellent long-term durability in patients such as this, where the diaphysis is preserved and more than 4 cm of intact diaphysis is available for fixation. Allograft-prosthetic composites and tumor replacement prostheses are used for patients with more severe bone loss of the proximal femur and would not be indicated for this patient.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and
Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Paprosky WG: The femur in revision total hip arthroplasty: Evaluation and classification. Clin Orthop Relat Res 2004;420:55-62.
Engh CA Jr, Ellis TJ, Koralewicz LM, et al: Extensively porous-coated femoral revision for severe femoral bone loss: Minimum 10-year follow-up. J Arthroplasty 2002;8:955-960.
Figure 15
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and
Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Paprosky WG: The femur in revision total hip arthroplasty: Evaluation and classification. Clin Orthop Relat Res 2004;420:55-62.
Engh CA Jr, Ellis TJ, Koralewicz LM, et al: Extensively porous-coated femoral revision for severe femoral bone loss: Minimum 10-year follow-up. J Arthroplasty 2002;8:955-960.
Figure 15
Question 6High Yield
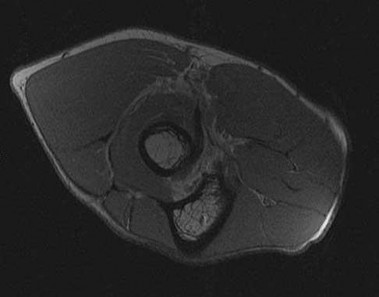
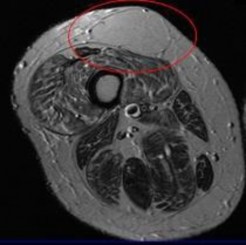
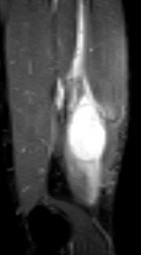
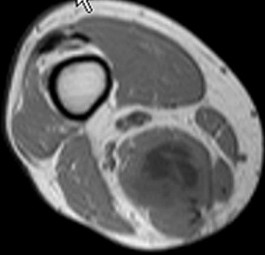
Rupture of the structure shown in the axial cross and the sagittal sections in Figures 100a and 100b causes weakness in

Explanation
87
The structure identified is the distal biceps tendon. Rupture of this tendon causes weakness in both flexion and supination. The biceps tendon does not affect extension or pronation.
RECOMMENDED READINGS
1. [Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. PubMed PMID: 3972865. ](http://www.ncbi.nlm.nih.gov/pubmed/3972865)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3972865)
2. [Mazzocca AD, Spang JT, Arciero RA. Distal biceps rupture. Orthop Clin North Am. 2008 Apr;39(2):237-49, vii. doi: 10.1016/j.ocl.2008.01.001. Review. PubMed PMID: 18374814. ](http://www.ncbi.nlm.nih.gov/pubmed/18374814)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18374814)
The structure identified is the distal biceps tendon. Rupture of this tendon causes weakness in both flexion and supination. The biceps tendon does not affect extension or pronation.
RECOMMENDED READINGS
1. [Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. PubMed PMID: 3972865. ](http://www.ncbi.nlm.nih.gov/pubmed/3972865)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3972865)
2. [Mazzocca AD, Spang JT, Arciero RA. Distal biceps rupture. Orthop Clin North Am. 2008 Apr;39(2):237-49, vii. doi: 10.1016/j.ocl.2008.01.001. Review. PubMed PMID: 18374814. ](http://www.ncbi.nlm.nih.gov/pubmed/18374814)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18374814)
Question 7High Yield
ORTHOPEDIC MCQS ONLINE 014 PATHOLOGY
..External beam radiotherapy
..External beam radiotherapy

































































































Explanation
..: 3- CT scan of the chest, abdomen, and pelvis. PREFERRED RESPONSE2…: 1- Metastatic adenocarcinoma
…: 4- Complex total hip arthroplasty
PREFERRED RESPONSE4 …: 1- should include the instrumented femur and periacetabular area.
..Li-Fraumeni syndrome (LFS) is associated with
1) multiple hemangiomas.
2) multiple hereditary osteochondromatosis.
3) soft-tissue sarcomas.
4) neurofibromatosis.
- soft-tissue sarcomas.
..A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized at the fracture site. Appropriate imaging studies are performed and show no other lesions. What is the next treatment step?
1) Cephalomedullary nail
2) Standard antegrade intramedullary nail
3) Resection and arthroplasty reconstruction
4) Open biopsy
- Open biopsy
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
…Based on the images and histopathology, how is this patient best treated?
1) Chemotherapy and external beam radiotherapy
2) Resection
3) Resection and chemotherapy
4) External beam radiation alone
…: 3- Chordoma PREFERRED RESPONSE14…: 2- Resection
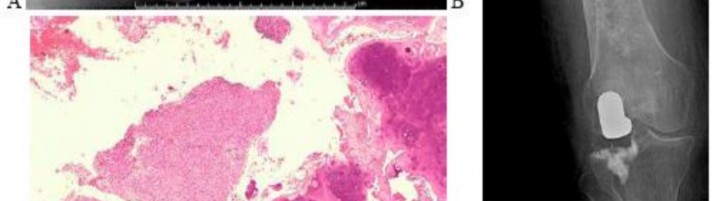
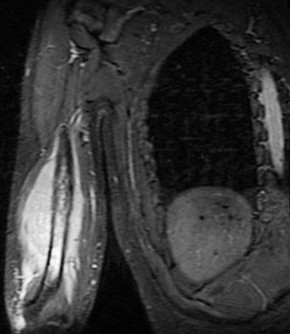
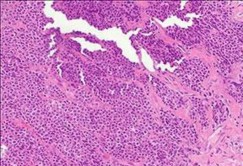
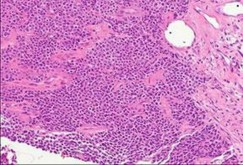
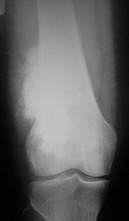
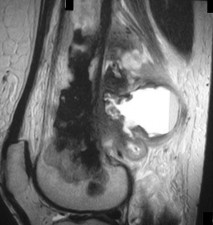
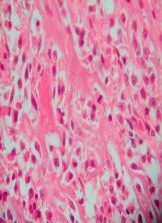
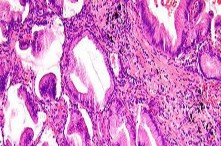
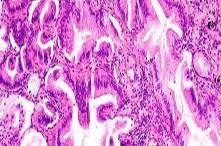
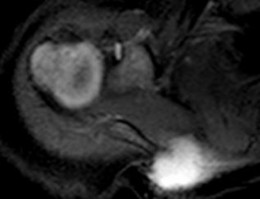
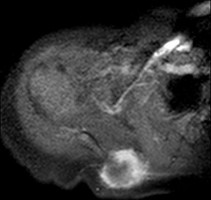
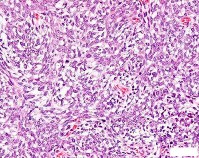
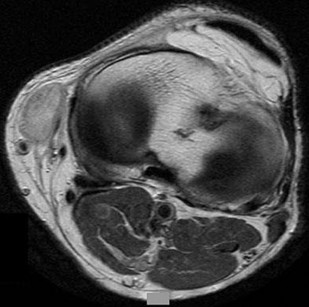
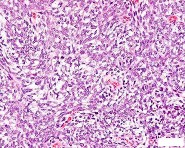
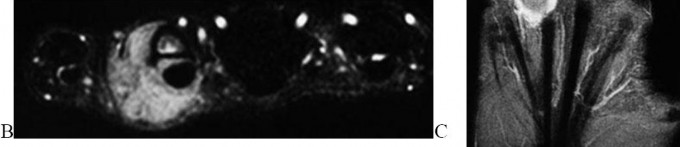
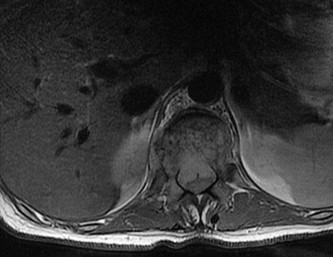
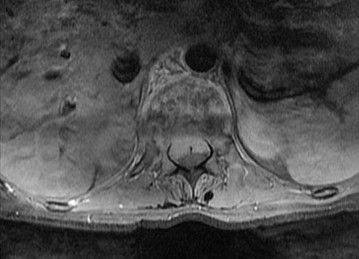
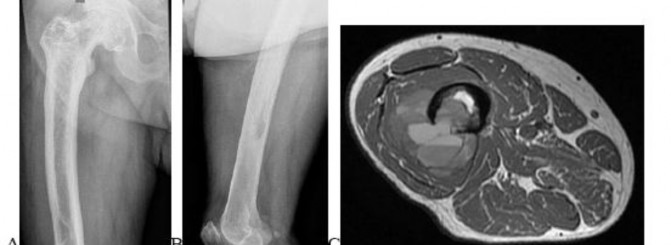
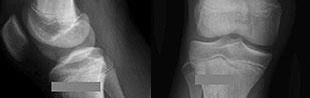
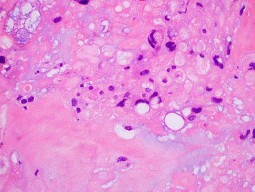
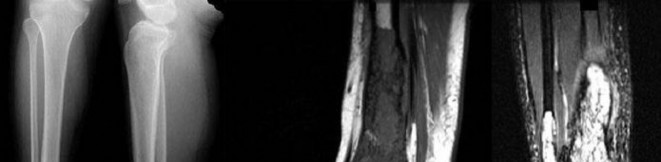
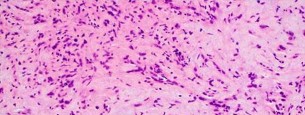
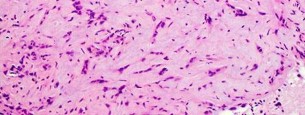
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
1) Localized pigmented villonodular synovitis (PVNS)
2) Biphasic synovial sarcoma
3) Nodular fasciitis
4) Synovial hemangioma
- Synovial hemangioma
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 19
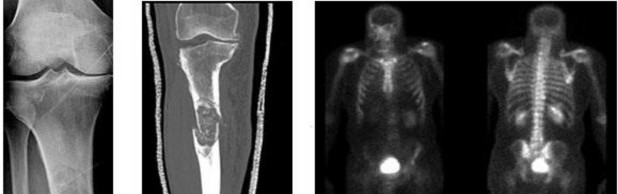
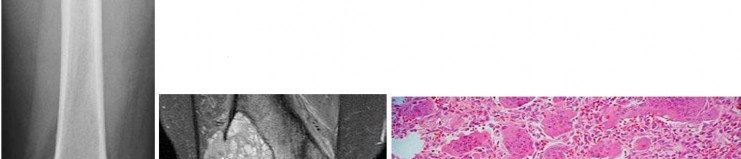
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.
..Approximately what percentage of the time does an unknown primary cancer get identified as part of a full metastatic work-up that includes radiographs; blood tests; a CT scan of the chest, abdomen and pelvis; whole-body bone scan; and biopsy of the metastatic focus?
1) 45%
2) 65%
3) 85%
4) 100%
..: 3- Biopsy of the fracture site
PREFERRED RESPONSE 18..: 3- Distal femoral resection with megaprosthesis PREFERRED RESPONSE 19..: 3- 85%...
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figures 20a and 20b are the radiographs of an 83-year-old active, independent, and healthy woman who has experienced 2 months of right lower thigh and knee pain. Her pain increased progressively over the course of several weeks. While exiting a car she “bumped” her knee against the door, felt a “crack,” and developed excruciating pain. She could no longer ambulate and was brought to the hospital.
..What is the most likely site of metastatic disease in patients with this diagnosis?
1) Liver
2) Lungs
3) Brain
4) Kidneys
-: 4- Enchondroma
PREFERRED RESPONSE21-..: 4- Dedifferentiated chondrosarcomas
PREFERRED RESPONSE22-..: 3- Above-the-knee amputation with wide surgical margin PREFERRED RESPONSE23-..: 2- Lungs
..A 14-year-old boy has had wrist pain for 3 weeks. Radiographs are shown in Figures 24a and 24b. His MRI scans are shown in Figures 24c through 24f. Representative histology is shown in Figures 24g through 24i. The most likely diagnosis is
1) aneurysmal bone cyst.
2) fibrous dysplasia.
3) giant-cell tumor.
4) osteoblastoma.
- osteoblastoma.
RESPONSES FOR QUESTIONS 25 THROUGH 29
..Figure 30a is the radiograph taken in the emergency department of a 20-year-old man with pain and swelling in his right-dominant arm. His MRI scan is seen in Figure 30b, and his histopathology is shown in Figure 30c. What is the most likely diagnosis?
1) Ewing sarcoma
2) Langerhans cell histiocytosis
3) Osteosarcoma
4) Osteomyelitis
- Ewing sarcoma
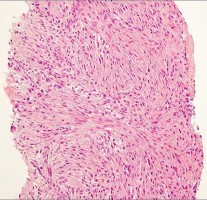
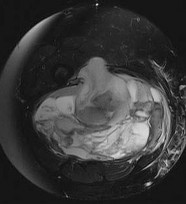
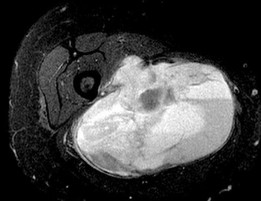
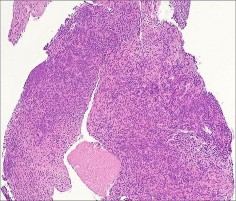
..An 18-year-old woman has had a right thigh mass for “a long time.” She has found it increasingly difficult to ambulate. Her medical history is unremarkable, with the exception of hypertension. On clinical examination, a fullness is appreciated in the popliteal fossa. The neurovascular status of the distal extremity is intact. Anteroposterior and lateral radiographs are shown in Figures 31a and 31b. A lateral T2-weighted MRI scan is shown in Figure 31c. The histology is seen in Figure 31d. What is the most likely diagnosis?
1) Aneurysmal bone cyst
2) Osteosarcoma
3) Periosteal lipoma
4) Parosteal osteosarcoma
- Osteosarcoma
CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 36
A 68-year-old woman is referred for left thigh pain. Her medical history includes Hypertension, diabetes, and adenocarcinoma of the breast treated with surgery, chemotherapy, and radiation 3 years ago. She currently is on aromatase therapy. She is unable to ambulate secondary to pain, is limited to a walker, and requires narcotic medications. She has no other pain but agrees to your recommendation that she urgently be sent to the hospital.
..Which intervention should be added to this patient’s care to best prevent future skeletally related events (SRE)?
1) Inferior vena cava (IVC) filter placement
2) Bisphosphonates
3) External beam radiation
4) Tc-99 whole-body bone scan at regular intervals
…: 3- Further imaging PREFERRED RESPONSE 33-..: 3- Location of the lesion PREFERRED RESPONSE 34-…: 2- 15%
PREFERRED RESPONSE 35…..:4- Lung carcinoma, breast carcinoma, multiple myeloma PREFERRED RESPONSE 36-…: 2- Bisphosphonates
..Figures 37a and 37b are the lateral and anteroposterior (AP) radiographs of a 60-year-old man with a remote history of renal cell cancer. A needle biopsy of the lesion is shown in Figure 37c. The bone destruction that occurs in this process is a result of
1) tumor cells.
2) cytokines secreted by the tumor.
3) host bone osteoblasts.
4) osteoprotegerin.
.
- cytokines secreted by the tumor
..Figures 38a and 38b are the histopathology of an otherwise healthy 31-year-old man who had a growing mass excised from his forearm with local anesthetic and no preoperative imaging. The mass was documented to be subfascial and larger than 5 cm.
What is the best local treatment option?
1) Observation
2) Radiation only
3) Chemotherapy only
4) Re-excision and radiation
- Re-excision and radiation
…Figure 39a is the anteroposterior radiograph of a 51-year-old man who has had a painless soft-tissue mass on his left wrist for 2 months. MR sequences are shown in Figures 39b through 39d. A biopsy was performed and shown in a low-power hematoxylin and eosin photomicrograph in Figure 39e. The most appropriate treatment for this lesion is
1) a diet that reduces uric acid production.
2) wide local resection followed by radiotherapy.
3) marginal excision.
4) observation until the mineralization matures, and then excision and radiotherapy to prevent recurrence.
- marginal excision.
CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 43
Figures 40a through 40c are the radiograph, bone scan, and histology of a 68-year-old man who has had 3 months of pain in his left thigh with weight bearing. He has no history of cancer and no illnesses.
..The orthopaedic surgeon obtains tissue with the histology shown in Figure 40c. Treatment should consist of
1) surgical stabilization.
2) surgical stabilization and radiation.
3) excision and endoprosthesis.
4) radiation.
- …..: 1- malignant.
PREFERRED RESPONSE 41..,,,,,,,: 1- CT scan of the chest, abdomen and pelvis. PREFERRED RESPONSE 42………: 2- biopsy.
PREFERRED RESPONSE 43……….: 2- surgical stabilization and radiation.
..First-line treatment recommendations include
1) synovectomy.
2) arthrocentesis, compressive wrap, and rest.
3) en bloc resection.
4) intra-articular radioactive nucleotide injection.
- pigmented villonodular synovitis (PVNS). PREFERRED RESPONSE: 1- synovectomy.
RESPONSES FOR QUESTIONS 47 THROUGH 52
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
1) Nonsurgical treatment of the fracture
2) Aspiration and injection with methylprednisolone
3) Curettage and augmentation with bone cement and internal fixation
4) Further imaging and biopsy
- Nonsurgical treatment of the fracture
..Figure 54 is the CT scan of a 70-year-old man with progressive neck pain; there is no history of trauma, and examination is notable only for mildly decreased cervical range of motion. He is neurologically intact. He has monoclonal gammopathy of undetermined significance that has been stable for many years. Current serum protein electrophoresis is unchanged. History and examination reveal no other causes for his pain. What is the next step in clinical management?
1) Corpectomy and anterior fusion
2) Radiation therapy followed by multiple myeloma protocol chemotherapy
3) CT-guided biopsy
4) CT scan of the chest, abdomen, and pelvis
- CT scan of the chest, abdomen, and pelvis
…A 27-year-old incarcerated man was found to have a fungating mass on his anterolateral right proximal thigh. A clinical photograph is shown in Figure 55a. T1- and T2-weighted coronal MRI scans are shown in Figures 55b and 55c. The hematoxylin and eosin and CD34 stained histology are shown in Figures 55d and 55e. What is the most likely diagnosis?
1) Squamous cell carcinoma
2) Melanoma
3) Dermatofibrosarcoma protuberans (DFSP)
4) Desmoid tumor
- Dermatofibrosarcoma protuberans (DFSP)
..Figures 56a and 56b are the axial short tau inversion recovery and T1 with contrast images of a 7-month-old infant who is found to have a right scapular soft-tissue mass. On examination, the mass is hard. A biopsy was performed and is shown in Figure 56c (hematoxylin and eosin, 400x). What is the optimal treatment for this patient?
1) Intralesional excision 2- Marginal excision
2) Wide excision 4- Observation
- Wide excision
…Figures 57a through 57d show the radiographs and T1- and T2-weighted MRI scan sequences of the proximal femur of a 60-year-old man with progressive thigh pain. A review of radiographs taken 3 years ago reveals that the lesion is new. The biopsy specimen is shown in Figure 57e; staging studies show no other lesions, and local imaging confirms the process is confined to bone (no soft-tissue mass). The next treatment step should include
1) hip disarticulation.
2) radiotherapy.
3) ifosfamide-based chemotherapy.
4) wide resection and reconstruction.
- wide resection and reconstruction.
…The characteristic translocation and genes involved in extraskeletal myxoid chondrosarcoma is
1) t(11;12) EWS;FLI1
2) t(12;16) TLS;CHOP.
3) t(9;22)EWS;CHN.
4) t(9;22) BCR-ABL.
.
- t(9;22) EWS;CHN
.Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg. The histopathology is shown in Figure 59c. A radiograph of her leg showed no mineralizations or osseous erosions. The chromosomal abnormality that is associated with this disease is
1) t(11;22).
2) t(2;13).
3) t(X;18).
4) t(12;16).
- t(X;18).
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The patient first noticed it about 6 months after she had a low-impact fall. The general surgeon evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient underwent a surgical procedure to remove the mass.
..What is the most common detrimental impact of an unplanned excision of a high-grade soft-tissue sarcoma?
1) Decreased mortality
2) Decreased recurrence
3) Increased wound complications
4) Increased functional outcome
-,…: 2- Imaging studies (MRI scan or CT scan) PREFERRED RESPONSE 61….: 1- Meticulous hemostasis and closure PREFERRED RESPONSE 62…..: 3- No imaging was obtained before surgery. PREFERRED RESPONSE 63…..: 3- Increased wound complications
CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 66
Figures 64a through 64c are the radiograph, MRI scan, and histology of a 53-year-old man with medial knee pain and swelling below the knee.
..Histology of the lesion is shown in Figure 64c. The best next treatment step is
1) radiation.
2) radiation and surgery.
3) chemotherapy.
4) observation.
- Translocation x;18 PREFERRED RESPONSE: 4- Biopsy
PREFERRED RESPONSE: 2- radiation and surgery.
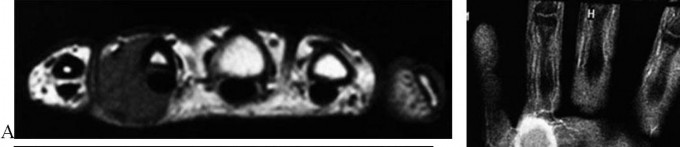
..A 26-year-old woman has had a slow-growing and painful mass at the base of her ring finger for several months. Radiographs of the affected digit show no mineralization or erosions of the underlying bone. An axial T1 MRI scan is shown in Figure 67a, and a corresponding short tau inversion recovery image is shown in Figure 67b. A coronal T1 MRI scan with contrast is shown in Figure 67c. The best next treatment step is
1) referral to a sarcoma center.
2) observation.
3) excisional biopsy.
4) marginal excision.
- referral to a sarcoma center.
..What is the most specific immunohistochemistry staining pattern that confirms the diagnosis of desmoid tumor?
1) Membranous beta-catenin staining
2) Nuclear beta-catenin staining
3) Nuclear SMAD4 staining
4) Vimentin positivity
- Nuclear beta-catenin staining
…A 30-year-old woman has progressive gait instability, back pain, and urinary retention. Figures 69a and 69b show the axial T2 and postcontrast MRI scans taken at the level of T11, and Figure 69c shows the sagittal T1-weighted image. Representative histology is shown in Figure 69d. The patient remains ambulatory, but symptoms have
progressed during the last week and she is beginning to feel weakness in her legs. Examination is notable for decreased rectal tone, lower-extremity hyperreflexia and clonus, and 4/5 motor strength throughout the lower extremities. What is the most appropriate treatment recommendation for this patient?
1) Margin-free en bloc spondylectomy of T11
2) Radiation therapy
3) Radiation therapy followed by anterior corpectomy and fusion
4) Transpedicular decompression and posterior stabilization followed by radiation therapy
- Transpedicular decompression and posterior stabilization followed by radiation therapy
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
1) Conventional chondrosarcoma
2) Aneurysmal bone cyst
3) Chondroblastoma
4) Osteoblastoma
- Chondroblastoma
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
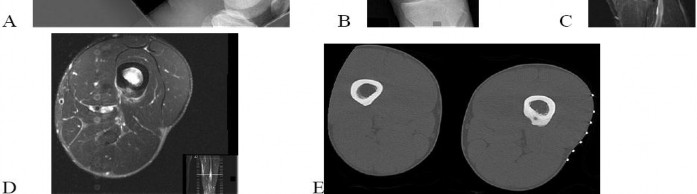
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
…What is the etiology of the pain associated with this lesion?
1) Prostaglandin production
2) Gram-positive cocci
3) Osteoclast activation
4) Loss of structural integrity of the bone
- Osteoid osteoma PREFERRED RESPONSE: 2- radiofrequency ablation. PREFERRED RESPONSE: 1- Prostaglandin production
...Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most influenced by
1) stage at presentation.
2) grade at presentation.
3) response to neoadjuvant chemotherapy.
4) histologic subtype.
- stage at presentation.
..Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old man who has had a several-month history of progressive pain in his right hip and groin region. Based on these images and histology, what is the most appropriate treatment?
1) Wide resection
2) Curetting and bone grafting
3) Percutaneous cementation and radiotherapy
4) Chemotherapy and radiotherapy
- Wide resection
..Figure 76 is the radiograph of a 77-year-old patient with a history of myeloma who has had severe arm pain after opening a jar. Pain was present for 3 months prior to injury. The most biomechanically stable construct for this fracture is
1) intramedullary nailing (IMN).
2) IMN and cement.
3) plate.
4) plate and cement.
- plate and cement.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
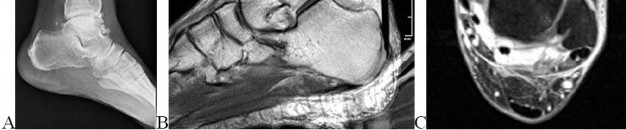
Figures 77a through 77c are the radiograph and MRI scans of a 45-year-old woman who enjoys dancing and has had left ankle pain for approximately 1 month with minimal trauma. She has slightly limited ankle dorsiflexion with a mechanical block with pain.
..The patient undergoes recommended surgery and minimal joint damage is found. How should she be counseled regarding her future prognosis?
1) High risk for local recurrence, moderate risk for metastases
2) High risk for local recurrence, no risk for metastases
3) Low risk for local recurrence, moderate risk for metastases
4) Low risk for local recurrence, no risk for metastases
- Synovial metaplasia
PREFERRED RESPONSE: 2- TA, EHL, anterior tibial artery, deep peroneal nerve, EDL PREFERRED RESPONSE: 4- Low risk for local recurrence, no risk for metastases
..Figures 80a through 80d are the radiographs and MRI scans of a 16-year-old girl who requires crutches because she is unable to bear weight on her right lower extremity. The pain has progressed over 2 months despite nonsurgical treatment.
Treatment at this point should include
1) continued observation.
2) aspiration and injection with methylprednisolone.
3) curettage and grafting.
4) wide margin resection.
- curettage and grafting.
..A previously healthy 60-year-old woman has a T5 pathologic compression fracture secondary to metastatic renal cell carcinoma. She has myelopathy with severe pain upon sitting from a supine position. The adjacent thoracic levels are unaffected. On MRI scan, there is minimal space available for the cord because of epidural involvement. What is the optimal treatment method at this time?
1) Surgical decompression and instrumented fusion
2) Surgical decompression without fusion
3) Image-guided intensity-modulated radiation therapy
4) Chemotherapy
- Surgical decompression and instrumented fusion
..Figures 82a and 82b are the MRI scans consisting of a T2 coronal sequence and axial T1 pulse sequence of a 38-year-old man who has had right thigh pain and a mass for 4 months since he pulled his hamstring. The presumed diagnosis considering his clinical history and evaluation of the MRI scan was hematoma and the mass was evacuated. The histology is shown in Figures 82c and 82d. Next treatment steps should include
1) physical therapy to accelerate healing and improve function.
2) a complete hematologic work-up to evaluate a bleeding disorder.
3) tumor bed excision and radiation to reduce local recurrence.
4) radiotherapy to complete definitive treatment of this problem.
- tumor bed excision and radiation to reduce local recurrence.
….Figures 83a through 83c are the radiograph and MRI scans of a 16-year-old girl who had posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the appropriate treatment for this patient?
1) Biopsy and resection of lesion
2) Observation and serial radiographs
3) Tc-99 whole-body bone scan and fine-cut CT scan
4) Evaluation by a pediatric oncologist
- Observation and serial radiographs
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figures 84a and 84b are the CT and MRI scans of a 17-year-old girl with a painful lumbosacral scoliosis that has been present for 12 months. Examination is notable only for pain over the left sacral region and a postural scoliosis leaning away from this side.
..With treatment, the spinal deformity is expected to
1) spontaneously resolve.
2) remain stable and nonprogressive.
3) respond in proportion to the family’s compliance with brace treatment.
4) resolve in the coronal plane and progress in the sagittal plane.
- is likely to respond to percutaneous intervention.
PREFERRED RESPONSE: 1- uses nonsteroidal anti-inflammatory or aspirin medications. PREFERRED RESPONSE: 1- spontaneously resolve.
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
1) external beam radiation.
2) curetting and cementation.
3) radiofrequency ablation.
4) wide local resection.
- wide local resection.
CLINICAL SITUATION FOR QUESTIONS 88 through 92
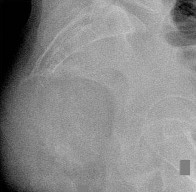
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.
..Oncologic outcome for this patient
1) is influenced by extraosseous tumor extension.
2) is more favorable if the lesion is solitary.
3) involves a predictable rapid demise.
4) hinges on the presence or absence of gene amplification.
- CT scan of the chest, abdomen, and pelvis.
PREFERRED RES: 3- Should be performed if the lesion is solitary, but not necessarily if multifocal PREFERRED RESPONSE: 4- resection and reconstruction.
PREFERRED RESPONSE: 3- inhibits vascular endothelial growth factor (VEGF) pathways. PREFERRED RESPONSE: 2- is more favorable if the lesion is solitary.
..Figures 93a and 93b are the MRI scans of a 24-year-old man with painless, persistent swelling in his left knee without any trauma. What is the best next treatment step?
1) Arthroscopic anterior synovectomy and posterior open resection
2) Arthroscopic anterior synovectomy only
3) Radiation therapy and wide excision
4) Observation
- Arthroscopic anterior synovectomy and posterior open resection
..What biopsy technique for a posterior thigh sarcoma is associated with the highest risk for adverse outcome?
1) Transverse incision open biopsy
2) Core needle biopsy
3) Fine-needle aspirate
4) Longitudinal incision open biopsy
- Transverse incision open biopsy
..A 60-year-old woman with a history of breast cancer has a rapidly enlarging arm mass. The lesion is situated outside of the prior irradiation field, but within an area of heavy lymphedema involvement. Needle biopsy reveals a high-grade sarcoma. What is the most likely diagnosis?
1) Lymphangiosarcoma
2) Acral myxoinflammatory fibroblastic sarcoma
3) Hemangioendothelioma
4) Hemangiopericytoma
- Lymphangiosarcoma
RESPONSES FOR QUESTIONS 96 THROUGH 100
..Figures 106a and 106b are the T1 sagittal and T2 coronal images of a 41-year-old woman who has been experiencing electric shock-type radiating pain over her right ankle for 4½ years. Her biopsy specimen is shown in Figure 106c. What is the best next treatment step?
1) Marginal excision
2) Wide excision
3) Wide excision and radiation
4) Observation
- Marginal excision
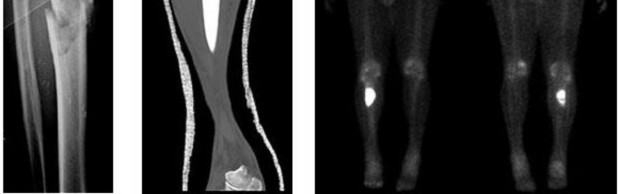
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
1) Staging studies to assess the extent of disease
2) Immediate stabilization of the fracture with an intramedullary nail
3) Curetting and bone culture
4) Segmental resection of the tibia and allograft reconstruction
- Staging studies to assess the extent of disease
RESPONSES FOR QUESTIONS 108 THROUGH 111
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
1) Secondary sarcoma in a pre-existing condition
2) Angiosarcoma
3) Metastatic lung carcinoma
4) Fibrous dysplasia
- Secondary sarcoma in a pre-existing condition
CLINICAL SITUATION FOR QUESTIONS 113 THROUGH 116
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
1) Before surgery
2) Intraoperatively after instrumentation
3) After surgery (reamings/curettings sent)
4) No biopsy is needed
- Positron emission tomography (PET) scan PREFERRED RESPONSE: 3- Curettage, cementation, and internal fixation PREFERRED RESPONSE: 4- resection and prosthetic reconstruction.
PREFERRED RESPONSE: 1- Before surgery
CLINICAL SITUATION FOR QUESTIONS 117 THROUGH 120
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.
Findings of multiple lesions in multiple skeletal sites may be associated with
1) decreased risk for malignancy.
2) a characteristic chromosomal translocation.
3) soft-tissue hemangiomas.
4) limb deformity and short stature.
- Osteochondroma
PREFERRED RESPONSE: 1- benign and simply can be observed with serial radiographs. PREFERRED RESPONSE: 4- growth beyond skeletal maturity.
PREFERRED RESPONSE: 4- limb deformity and short stature.
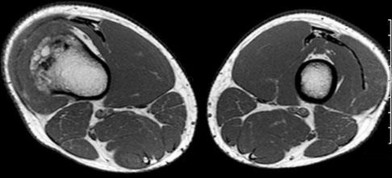
..Figure 121a is the axial T1 MRI scan and Figure 121b is the coronal T1 MRI scan of an 85-year-old man who has a mass in his medial thigh. The mass was present for years and recently grew. His biopsy specimen is shown in Figure 121c. What is the best treatment for this patient?
1) Chemotherapy and wide local resection
2) Wide local resection and radiotherapy
3) Marginal excision
4) Observation and reimaging in 6 months
- Wide local resection and radiotherapy
..What tumor commonly metastasizes to regional lymph nodes?
1) Fibromyxoid sarcoma
2) Epithelioid sarcoma
3) Leiomyosarcoma
4) Liposarcoma
- Epithelioid sarcoma
..A 64-year-old woman has significant right arm pain associated with a destructive proximal humeral bone lesion with an associated soft-tissue mass. Her medical history includes carcinoma of the breast treated 8 years ago with modified radical mastectomy, hormone receptor-based chemotherapy, and 45 Gy of radiation with 8 subsequent disease-free years. Biopsy reveals a high-grade osteogenic sarcoma. What factor is most likely related to her current disease?
1) Presence of metastatic disease
2) Dosage of radiation treatment
3) Type of prior surgical procedure
4) Type of chemotherapy given
- Dosage of radiation treatment
..Figures 124a and 124b are the MRI scans of a 25-year-old woman who has a painful mass in her left gluteal and thigh region. Her biopsy specimen is seen in Figure 124c. What is the most likely diagnosis?
1) Desmoid fibromatosis
2) Extraskeletal Ewing sarcoma
3) Metastatic breast cancer
4) Lymphoma
- Desmoid fibromatosis
CLINICAL SITUATION FOR QUESTIONS 125 THROUGH 128
A 45-year-old woman has increasing knee pain with activity and at rest. Her radiograph, MRI scan, and histology are shown in Figures 125a through 125c.
..The cell that directly causes osteolysis in this lesion is
1) giant cell.
2) stromal cell.
3) osteoblast.
4) fibroblast.
- benign aggressive. PREFERRED RESPONSE: 4- chest radiograph.
PREFERRED RESPONSE: 1- extended intralesional curettage. PREFERRED RESPONSE: 1- giant cell.
..Figures 129a through 129c are the lateral radiograph of the sacrum, axial CT scan, and a high-power view of a fine-needle biopsy of a 47-year-old man who has buttock pain and constipation. A large mass is palpable on rectal examination. The tumor cell that is the signature of this tumor is known as a(n)
1) giant cell.
2) physaliferous cell.
3) chondroblast.
4) adipocyte.
- physaliferous cell.
..Figures 130a through 130c show the CT scan and T1- and T2-weighted MRI scan sequences of an otherwise healthy 67-year-old woman with progressive left groin pain. Her biopsy specimen is shown in Figure 130d. Staging studies reveal no other lesions. Treatment should include
1) radiotherapy.
2) chemotherapy followed by surgical resection.
3) curettage with adjuvant treatment and grafting.
4) en bloc resection.
- en bloc resection.
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?
1) Chemotherapy and wide local excision
2) Chemotherapy and radiotherapy
3) Marginal excision
4) Extended intralesional curettage
- Extended intralesional curettage
CLINICAL SITUATION FOR QUESTIONS 132 THROUGH 134
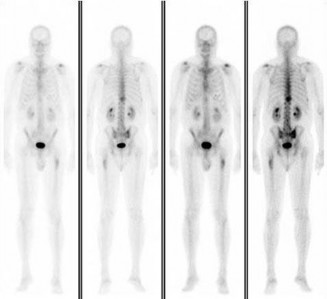
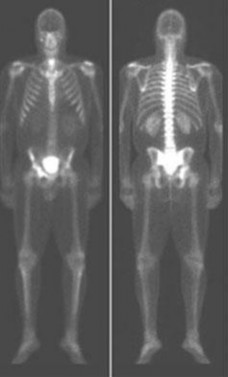
Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
1) The distal femoral lesion should undergo needle biopsy first.
2) Bone marrow biopsy should be done first.
3) Preoperative biopsy is not necessary because a metastatic process is present.
4) Biopsy is not necessary if the lesion demonstrates a standardized uptake value (SUV) greater than 3 on fluorodeoxyglucose positron emission tomography (PET) imaging.
.
- CT scan of the chest, abdomen, and pelvis and laboratory studies. PREFERRED RESPONSE: 3- intravenous bisphosphonate treatment.
PREFERRED RESPONSE: 3- Preoperative biopsy is not necessary because a metastatic process is present
…: 4- Complex total hip arthroplasty
PREFERRED RESPONSE4 …: 1- should include the instrumented femur and periacetabular area.
..Li-Fraumeni syndrome (LFS) is associated with
1) multiple hemangiomas.
2) multiple hereditary osteochondromatosis.
3) soft-tissue sarcomas.
4) neurofibromatosis.
- soft-tissue sarcomas.
..A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized at the fracture site. Appropriate imaging studies are performed and show no other lesions. What is the next treatment step?
1) Cephalomedullary nail
2) Standard antegrade intramedullary nail
3) Resection and arthroplasty reconstruction
4) Open biopsy
- Open biopsy
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
…Based on the images and histopathology, how is this patient best treated?
1) Chemotherapy and external beam radiotherapy
2) Resection
3) Resection and chemotherapy
4) External beam radiation alone
…: 3- Chordoma PREFERRED RESPONSE14…: 2- Resection
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
1) Localized pigmented villonodular synovitis (PVNS)
2) Biphasic synovial sarcoma
3) Nodular fasciitis
4) Synovial hemangioma
- Synovial hemangioma
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 19
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.
..Approximately what percentage of the time does an unknown primary cancer get identified as part of a full metastatic work-up that includes radiographs; blood tests; a CT scan of the chest, abdomen and pelvis; whole-body bone scan; and biopsy of the metastatic focus?
1) 45%
2) 65%
3) 85%
4) 100%
..: 3- Biopsy of the fracture site
PREFERRED RESPONSE 18..: 3- Distal femoral resection with megaprosthesis PREFERRED RESPONSE 19..: 3- 85%...
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figures 20a and 20b are the radiographs of an 83-year-old active, independent, and healthy woman who has experienced 2 months of right lower thigh and knee pain. Her pain increased progressively over the course of several weeks. While exiting a car she “bumped” her knee against the door, felt a “crack,” and developed excruciating pain. She could no longer ambulate and was brought to the hospital.
..What is the most likely site of metastatic disease in patients with this diagnosis?
1) Liver
2) Lungs
3) Brain
4) Kidneys
-: 4- Enchondroma
PREFERRED RESPONSE21-..: 4- Dedifferentiated chondrosarcomas
PREFERRED RESPONSE22-..: 3- Above-the-knee amputation with wide surgical margin PREFERRED RESPONSE23-..: 2- Lungs
..A 14-year-old boy has had wrist pain for 3 weeks. Radiographs are shown in Figures 24a and 24b. His MRI scans are shown in Figures 24c through 24f. Representative histology is shown in Figures 24g through 24i. The most likely diagnosis is
1) aneurysmal bone cyst.
2) fibrous dysplasia.
3) giant-cell tumor.
4) osteoblastoma.
- osteoblastoma.
RESPONSES FOR QUESTIONS 25 THROUGH 29
..Figure 30a is the radiograph taken in the emergency department of a 20-year-old man with pain and swelling in his right-dominant arm. His MRI scan is seen in Figure 30b, and his histopathology is shown in Figure 30c. What is the most likely diagnosis?
1) Ewing sarcoma
2) Langerhans cell histiocytosis
3) Osteosarcoma
4) Osteomyelitis
- Ewing sarcoma
..An 18-year-old woman has had a right thigh mass for “a long time.” She has found it increasingly difficult to ambulate. Her medical history is unremarkable, with the exception of hypertension. On clinical examination, a fullness is appreciated in the popliteal fossa. The neurovascular status of the distal extremity is intact. Anteroposterior and lateral radiographs are shown in Figures 31a and 31b. A lateral T2-weighted MRI scan is shown in Figure 31c. The histology is seen in Figure 31d. What is the most likely diagnosis?
1) Aneurysmal bone cyst
2) Osteosarcoma
3) Periosteal lipoma
4) Parosteal osteosarcoma
- Osteosarcoma
CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 36
A 68-year-old woman is referred for left thigh pain. Her medical history includes Hypertension, diabetes, and adenocarcinoma of the breast treated with surgery, chemotherapy, and radiation 3 years ago. She currently is on aromatase therapy. She is unable to ambulate secondary to pain, is limited to a walker, and requires narcotic medications. She has no other pain but agrees to your recommendation that she urgently be sent to the hospital.
..Which intervention should be added to this patient’s care to best prevent future skeletally related events (SRE)?
1) Inferior vena cava (IVC) filter placement
2) Bisphosphonates
3) External beam radiation
4) Tc-99 whole-body bone scan at regular intervals
…: 3- Further imaging PREFERRED RESPONSE 33-..: 3- Location of the lesion PREFERRED RESPONSE 34-…: 2- 15%
PREFERRED RESPONSE 35…..:4- Lung carcinoma, breast carcinoma, multiple myeloma PREFERRED RESPONSE 36-…: 2- Bisphosphonates
..Figures 37a and 37b are the lateral and anteroposterior (AP) radiographs of a 60-year-old man with a remote history of renal cell cancer. A needle biopsy of the lesion is shown in Figure 37c. The bone destruction that occurs in this process is a result of
1) tumor cells.
2) cytokines secreted by the tumor.
3) host bone osteoblasts.
4) osteoprotegerin.
.
- cytokines secreted by the tumor
..Figures 38a and 38b are the histopathology of an otherwise healthy 31-year-old man who had a growing mass excised from his forearm with local anesthetic and no preoperative imaging. The mass was documented to be subfascial and larger than 5 cm.
What is the best local treatment option?
1) Observation
2) Radiation only
3) Chemotherapy only
4) Re-excision and radiation
- Re-excision and radiation
…Figure 39a is the anteroposterior radiograph of a 51-year-old man who has had a painless soft-tissue mass on his left wrist for 2 months. MR sequences are shown in Figures 39b through 39d. A biopsy was performed and shown in a low-power hematoxylin and eosin photomicrograph in Figure 39e. The most appropriate treatment for this lesion is
1) a diet that reduces uric acid production.
2) wide local resection followed by radiotherapy.
3) marginal excision.
4) observation until the mineralization matures, and then excision and radiotherapy to prevent recurrence.
- marginal excision.
CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 43
Figures 40a through 40c are the radiograph, bone scan, and histology of a 68-year-old man who has had 3 months of pain in his left thigh with weight bearing. He has no history of cancer and no illnesses.
..The orthopaedic surgeon obtains tissue with the histology shown in Figure 40c. Treatment should consist of
1) surgical stabilization.
2) surgical stabilization and radiation.
3) excision and endoprosthesis.
4) radiation.
- …..: 1- malignant.
PREFERRED RESPONSE 41..,,,,,,,: 1- CT scan of the chest, abdomen and pelvis. PREFERRED RESPONSE 42………: 2- biopsy.
PREFERRED RESPONSE 43……….: 2- surgical stabilization and radiation.
..First-line treatment recommendations include
1) synovectomy.
2) arthrocentesis, compressive wrap, and rest.
3) en bloc resection.
4) intra-articular radioactive nucleotide injection.
- pigmented villonodular synovitis (PVNS). PREFERRED RESPONSE: 1- synovectomy.
RESPONSES FOR QUESTIONS 47 THROUGH 52
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
1) Nonsurgical treatment of the fracture
2) Aspiration and injection with methylprednisolone
3) Curettage and augmentation with bone cement and internal fixation
4) Further imaging and biopsy
- Nonsurgical treatment of the fracture
..Figure 54 is the CT scan of a 70-year-old man with progressive neck pain; there is no history of trauma, and examination is notable only for mildly decreased cervical range of motion. He is neurologically intact. He has monoclonal gammopathy of undetermined significance that has been stable for many years. Current serum protein electrophoresis is unchanged. History and examination reveal no other causes for his pain. What is the next step in clinical management?
1) Corpectomy and anterior fusion
2) Radiation therapy followed by multiple myeloma protocol chemotherapy
3) CT-guided biopsy
4) CT scan of the chest, abdomen, and pelvis
- CT scan of the chest, abdomen, and pelvis
…A 27-year-old incarcerated man was found to have a fungating mass on his anterolateral right proximal thigh. A clinical photograph is shown in Figure 55a. T1- and T2-weighted coronal MRI scans are shown in Figures 55b and 55c. The hematoxylin and eosin and CD34 stained histology are shown in Figures 55d and 55e. What is the most likely diagnosis?
1) Squamous cell carcinoma
2) Melanoma
3) Dermatofibrosarcoma protuberans (DFSP)
4) Desmoid tumor
- Dermatofibrosarcoma protuberans (DFSP)
..Figures 56a and 56b are the axial short tau inversion recovery and T1 with contrast images of a 7-month-old infant who is found to have a right scapular soft-tissue mass. On examination, the mass is hard. A biopsy was performed and is shown in Figure 56c (hematoxylin and eosin, 400x). What is the optimal treatment for this patient?
1) Intralesional excision 2- Marginal excision
2) Wide excision 4- Observation
- Wide excision
…Figures 57a through 57d show the radiographs and T1- and T2-weighted MRI scan sequences of the proximal femur of a 60-year-old man with progressive thigh pain. A review of radiographs taken 3 years ago reveals that the lesion is new. The biopsy specimen is shown in Figure 57e; staging studies show no other lesions, and local imaging confirms the process is confined to bone (no soft-tissue mass). The next treatment step should include
1) hip disarticulation.
2) radiotherapy.
3) ifosfamide-based chemotherapy.
4) wide resection and reconstruction.
- wide resection and reconstruction.
…The characteristic translocation and genes involved in extraskeletal myxoid chondrosarcoma is
1) t(11;12) EWS;FLI1
2) t(12;16) TLS;CHOP.
3) t(9;22)EWS;CHN.
4) t(9;22) BCR-ABL.
.
- t(9;22) EWS;CHN
.Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg. The histopathology is shown in Figure 59c. A radiograph of her leg showed no mineralizations or osseous erosions. The chromosomal abnormality that is associated with this disease is
1) t(11;22).
2) t(2;13).
3) t(X;18).
4) t(12;16).
- t(X;18).
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The patient first noticed it about 6 months after she had a low-impact fall. The general surgeon evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient underwent a surgical procedure to remove the mass.
..What is the most common detrimental impact of an unplanned excision of a high-grade soft-tissue sarcoma?
1) Decreased mortality
2) Decreased recurrence
3) Increased wound complications
4) Increased functional outcome
-,…: 2- Imaging studies (MRI scan or CT scan) PREFERRED RESPONSE 61….: 1- Meticulous hemostasis and closure PREFERRED RESPONSE 62…..: 3- No imaging was obtained before surgery. PREFERRED RESPONSE 63…..: 3- Increased wound complications
CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 66
Figures 64a through 64c are the radiograph, MRI scan, and histology of a 53-year-old man with medial knee pain and swelling below the knee.
..Histology of the lesion is shown in Figure 64c. The best next treatment step is
1) radiation.
2) radiation and surgery.
3) chemotherapy.
4) observation.
- Translocation x;18 PREFERRED RESPONSE: 4- Biopsy
PREFERRED RESPONSE: 2- radiation and surgery.
..A 26-year-old woman has had a slow-growing and painful mass at the base of her ring finger for several months. Radiographs of the affected digit show no mineralization or erosions of the underlying bone. An axial T1 MRI scan is shown in Figure 67a, and a corresponding short tau inversion recovery image is shown in Figure 67b. A coronal T1 MRI scan with contrast is shown in Figure 67c. The best next treatment step is
1) referral to a sarcoma center.
2) observation.
3) excisional biopsy.
4) marginal excision.
- referral to a sarcoma center.
..What is the most specific immunohistochemistry staining pattern that confirms the diagnosis of desmoid tumor?
1) Membranous beta-catenin staining
2) Nuclear beta-catenin staining
3) Nuclear SMAD4 staining
4) Vimentin positivity
- Nuclear beta-catenin staining
…A 30-year-old woman has progressive gait instability, back pain, and urinary retention. Figures 69a and 69b show the axial T2 and postcontrast MRI scans taken at the level of T11, and Figure 69c shows the sagittal T1-weighted image. Representative histology is shown in Figure 69d. The patient remains ambulatory, but symptoms have
progressed during the last week and she is beginning to feel weakness in her legs. Examination is notable for decreased rectal tone, lower-extremity hyperreflexia and clonus, and 4/5 motor strength throughout the lower extremities. What is the most appropriate treatment recommendation for this patient?
1) Margin-free en bloc spondylectomy of T11
2) Radiation therapy
3) Radiation therapy followed by anterior corpectomy and fusion
4) Transpedicular decompression and posterior stabilization followed by radiation therapy
- Transpedicular decompression and posterior stabilization followed by radiation therapy
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
1) Conventional chondrosarcoma
2) Aneurysmal bone cyst
3) Chondroblastoma
4) Osteoblastoma
- Chondroblastoma
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
…What is the etiology of the pain associated with this lesion?
1) Prostaglandin production
2) Gram-positive cocci
3) Osteoclast activation
4) Loss of structural integrity of the bone
- Osteoid osteoma PREFERRED RESPONSE: 2- radiofrequency ablation. PREFERRED RESPONSE: 1- Prostaglandin production
...Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most influenced by
1) stage at presentation.
2) grade at presentation.
3) response to neoadjuvant chemotherapy.
4) histologic subtype.
- stage at presentation.
..Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old man who has had a several-month history of progressive pain in his right hip and groin region. Based on these images and histology, what is the most appropriate treatment?
1) Wide resection
2) Curetting and bone grafting
3) Percutaneous cementation and radiotherapy
4) Chemotherapy and radiotherapy
- Wide resection
..Figure 76 is the radiograph of a 77-year-old patient with a history of myeloma who has had severe arm pain after opening a jar. Pain was present for 3 months prior to injury. The most biomechanically stable construct for this fracture is
1) intramedullary nailing (IMN).
2) IMN and cement.
3) plate.
4) plate and cement.
- plate and cement.
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
Figures 77a through 77c are the radiograph and MRI scans of a 45-year-old woman who enjoys dancing and has had left ankle pain for approximately 1 month with minimal trauma. She has slightly limited ankle dorsiflexion with a mechanical block with pain.
..The patient undergoes recommended surgery and minimal joint damage is found. How should she be counseled regarding her future prognosis?
1) High risk for local recurrence, moderate risk for metastases
2) High risk for local recurrence, no risk for metastases
3) Low risk for local recurrence, moderate risk for metastases
4) Low risk for local recurrence, no risk for metastases
- Synovial metaplasia
PREFERRED RESPONSE: 2- TA, EHL, anterior tibial artery, deep peroneal nerve, EDL PREFERRED RESPONSE: 4- Low risk for local recurrence, no risk for metastases
..Figures 80a through 80d are the radiographs and MRI scans of a 16-year-old girl who requires crutches because she is unable to bear weight on her right lower extremity. The pain has progressed over 2 months despite nonsurgical treatment.
Treatment at this point should include
1) continued observation.
2) aspiration and injection with methylprednisolone.
3) curettage and grafting.
4) wide margin resection.
- curettage and grafting.
..A previously healthy 60-year-old woman has a T5 pathologic compression fracture secondary to metastatic renal cell carcinoma. She has myelopathy with severe pain upon sitting from a supine position. The adjacent thoracic levels are unaffected. On MRI scan, there is minimal space available for the cord because of epidural involvement. What is the optimal treatment method at this time?
1) Surgical decompression and instrumented fusion
2) Surgical decompression without fusion
3) Image-guided intensity-modulated radiation therapy
4) Chemotherapy
- Surgical decompression and instrumented fusion
..Figures 82a and 82b are the MRI scans consisting of a T2 coronal sequence and axial T1 pulse sequence of a 38-year-old man who has had right thigh pain and a mass for 4 months since he pulled his hamstring. The presumed diagnosis considering his clinical history and evaluation of the MRI scan was hematoma and the mass was evacuated. The histology is shown in Figures 82c and 82d. Next treatment steps should include
1) physical therapy to accelerate healing and improve function.
2) a complete hematologic work-up to evaluate a bleeding disorder.
3) tumor bed excision and radiation to reduce local recurrence.
4) radiotherapy to complete definitive treatment of this problem.
- tumor bed excision and radiation to reduce local recurrence.
….Figures 83a through 83c are the radiograph and MRI scans of a 16-year-old girl who had posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the appropriate treatment for this patient?
1) Biopsy and resection of lesion
2) Observation and serial radiographs
3) Tc-99 whole-body bone scan and fine-cut CT scan
4) Evaluation by a pediatric oncologist
- Observation and serial radiographs
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figures 84a and 84b are the CT and MRI scans of a 17-year-old girl with a painful lumbosacral scoliosis that has been present for 12 months. Examination is notable only for pain over the left sacral region and a postural scoliosis leaning away from this side.
..With treatment, the spinal deformity is expected to
1) spontaneously resolve.
2) remain stable and nonprogressive.
3) respond in proportion to the family’s compliance with brace treatment.
4) resolve in the coronal plane and progress in the sagittal plane.
- is likely to respond to percutaneous intervention.
PREFERRED RESPONSE: 1- uses nonsteroidal anti-inflammatory or aspirin medications. PREFERRED RESPONSE: 1- spontaneously resolve.
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
1) external beam radiation.
2) curetting and cementation.
3) radiofrequency ablation.
4) wide local resection.
- wide local resection.
CLINICAL SITUATION FOR QUESTIONS 88 through 92
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.
..Oncologic outcome for this patient
1) is influenced by extraosseous tumor extension.
2) is more favorable if the lesion is solitary.
3) involves a predictable rapid demise.
4) hinges on the presence or absence of gene amplification.
- CT scan of the chest, abdomen, and pelvis.
PREFERRED RES: 3- Should be performed if the lesion is solitary, but not necessarily if multifocal PREFERRED RESPONSE: 4- resection and reconstruction.
PREFERRED RESPONSE: 3- inhibits vascular endothelial growth factor (VEGF) pathways. PREFERRED RESPONSE: 2- is more favorable if the lesion is solitary.
..Figures 93a and 93b are the MRI scans of a 24-year-old man with painless, persistent swelling in his left knee without any trauma. What is the best next treatment step?
1) Arthroscopic anterior synovectomy and posterior open resection
2) Arthroscopic anterior synovectomy only
3) Radiation therapy and wide excision
4) Observation
- Arthroscopic anterior synovectomy and posterior open resection
..What biopsy technique for a posterior thigh sarcoma is associated with the highest risk for adverse outcome?
1) Transverse incision open biopsy
2) Core needle biopsy
3) Fine-needle aspirate
4) Longitudinal incision open biopsy
- Transverse incision open biopsy
..A 60-year-old woman with a history of breast cancer has a rapidly enlarging arm mass. The lesion is situated outside of the prior irradiation field, but within an area of heavy lymphedema involvement. Needle biopsy reveals a high-grade sarcoma. What is the most likely diagnosis?
1) Lymphangiosarcoma
2) Acral myxoinflammatory fibroblastic sarcoma
3) Hemangioendothelioma
4) Hemangiopericytoma
- Lymphangiosarcoma
RESPONSES FOR QUESTIONS 96 THROUGH 100
..Figures 106a and 106b are the T1 sagittal and T2 coronal images of a 41-year-old woman who has been experiencing electric shock-type radiating pain over her right ankle for 4½ years. Her biopsy specimen is shown in Figure 106c. What is the best next treatment step?
1) Marginal excision
2) Wide excision
3) Wide excision and radiation
4) Observation
- Marginal excision
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
1) Staging studies to assess the extent of disease
2) Immediate stabilization of the fracture with an intramedullary nail
3) Curetting and bone culture
4) Segmental resection of the tibia and allograft reconstruction
- Staging studies to assess the extent of disease
RESPONSES FOR QUESTIONS 108 THROUGH 111
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
1) Secondary sarcoma in a pre-existing condition
2) Angiosarcoma
3) Metastatic lung carcinoma
4) Fibrous dysplasia
- Secondary sarcoma in a pre-existing condition
CLINICAL SITUATION FOR QUESTIONS 113 THROUGH 116
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.
..Staging studies show no other lesions and surgical treatment is planned; when should a biopsy be performed?
1) Before surgery
2) Intraoperatively after instrumentation
3) After surgery (reamings/curettings sent)
4) No biopsy is needed
- Positron emission tomography (PET) scan PREFERRED RESPONSE: 3- Curettage, cementation, and internal fixation PREFERRED RESPONSE: 4- resection and prosthetic reconstruction.
PREFERRED RESPONSE: 1- Before surgery
CLINICAL SITUATION FOR QUESTIONS 117 THROUGH 120
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He states that initially the area was painful, but now all symptoms other than the mass have resolved.
Findings of multiple lesions in multiple skeletal sites may be associated with
1) decreased risk for malignancy.
2) a characteristic chromosomal translocation.
3) soft-tissue hemangiomas.
4) limb deformity and short stature.
- Osteochondroma
PREFERRED RESPONSE: 1- benign and simply can be observed with serial radiographs. PREFERRED RESPONSE: 4- growth beyond skeletal maturity.
PREFERRED RESPONSE: 4- limb deformity and short stature.
..Figure 121a is the axial T1 MRI scan and Figure 121b is the coronal T1 MRI scan of an 85-year-old man who has a mass in his medial thigh. The mass was present for years and recently grew. His biopsy specimen is shown in Figure 121c. What is the best treatment for this patient?
1) Chemotherapy and wide local resection
2) Wide local resection and radiotherapy
3) Marginal excision
4) Observation and reimaging in 6 months
- Wide local resection and radiotherapy
..What tumor commonly metastasizes to regional lymph nodes?
1) Fibromyxoid sarcoma
2) Epithelioid sarcoma
3) Leiomyosarcoma
4) Liposarcoma
- Epithelioid sarcoma
..A 64-year-old woman has significant right arm pain associated with a destructive proximal humeral bone lesion with an associated soft-tissue mass. Her medical history includes carcinoma of the breast treated 8 years ago with modified radical mastectomy, hormone receptor-based chemotherapy, and 45 Gy of radiation with 8 subsequent disease-free years. Biopsy reveals a high-grade osteogenic sarcoma. What factor is most likely related to her current disease?
1) Presence of metastatic disease
2) Dosage of radiation treatment
3) Type of prior surgical procedure
4) Type of chemotherapy given
- Dosage of radiation treatment
..Figures 124a and 124b are the MRI scans of a 25-year-old woman who has a painful mass in her left gluteal and thigh region. Her biopsy specimen is seen in Figure 124c. What is the most likely diagnosis?
1) Desmoid fibromatosis
2) Extraskeletal Ewing sarcoma
3) Metastatic breast cancer
4) Lymphoma
- Desmoid fibromatosis
CLINICAL SITUATION FOR QUESTIONS 125 THROUGH 128
A 45-year-old woman has increasing knee pain with activity and at rest. Her radiograph, MRI scan, and histology are shown in Figures 125a through 125c.
..The cell that directly causes osteolysis in this lesion is
1) giant cell.
2) stromal cell.
3) osteoblast.
4) fibroblast.
- benign aggressive. PREFERRED RESPONSE: 4- chest radiograph.
PREFERRED RESPONSE: 1- extended intralesional curettage. PREFERRED RESPONSE: 1- giant cell.
..Figures 129a through 129c are the lateral radiograph of the sacrum, axial CT scan, and a high-power view of a fine-needle biopsy of a 47-year-old man who has buttock pain and constipation. A large mass is palpable on rectal examination. The tumor cell that is the signature of this tumor is known as a(n)
1) giant cell.
2) physaliferous cell.
3) chondroblast.
4) adipocyte.
- physaliferous cell.
..Figures 130a through 130c show the CT scan and T1- and T2-weighted MRI scan sequences of an otherwise healthy 67-year-old woman with progressive left groin pain. Her biopsy specimen is shown in Figure 130d. Staging studies reveal no other lesions. Treatment should include
1) radiotherapy.
2) chemotherapy followed by surgical resection.
3) curettage with adjuvant treatment and grafting.
4) en bloc resection.
- en bloc resection.
..A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure 131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy who has injured his right knee twice during the last 5 months. He has a reduced range of motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant cells, and blood-filled spaces without endothelial lining. What is the most appropriate treatment?
1) Chemotherapy and wide local excision
2) Chemotherapy and radiotherapy
3) Marginal excision
4) Extended intralesional curettage
- Extended intralesional curettage
CLINICAL SITUATION FOR QUESTIONS 132 THROUGH 134
Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion about the right knee and mild hyporeflexia.
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
1) The distal femoral lesion should undergo needle biopsy first.
2) Bone marrow biopsy should be done first.
3) Preoperative biopsy is not necessary because a metastatic process is present.
4) Biopsy is not necessary if the lesion demonstrates a standardized uptake value (SUV) greater than 3 on fluorodeoxyglucose positron emission tomography (PET) imaging.
.
- CT scan of the chest, abdomen, and pelvis and laboratory studies. PREFERRED RESPONSE: 3- intravenous bisphosphonate treatment.
PREFERRED RESPONSE: 3- Preoperative biopsy is not necessary because a metastatic process is present
Question 8High Yield
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time?
Explanation
■
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Nonsurgical treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise, without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Nonsurgical treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise, without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
Question 9High Yield
A 2-year-old child is brought to your office for evaluation of a "big hand." Upon examination, you notice that the child has mildly enlarged ring and small fingers. There is full range of motion without instability. After examination of the patient, you recommend:
Explanation
The child is not ready for surgery. Although surgery may coincide with the patient beginning school, this does not always occur. At this time, additional examination and testing are recommended.
Question 10High Yield
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge- shaped
**vertebrae. What name is associated with this process?**
**vertebrae. What name is associated with this process?**
Explanation
**
The Heuter-Volkmann principle shows that bone placed in longitudinal tension will tend to stimulate longitudinal growth, and that compressive longitudinal forces inhibit longitudinal growth, making this response the best choice. Hooke's law relates to stress being proportional to strain and is not directly related to bone growth. Kirchhoff's laws apply to electrical circuit design. Wolff's law states that bone remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
The Heuter-Volkmann principle shows that bone placed in longitudinal tension will tend to stimulate longitudinal growth, and that compressive longitudinal forces inhibit longitudinal growth, making this response the best choice. Hooke's law relates to stress being proportional to strain and is not directly related to bone growth. Kirchhoff's laws apply to electrical circuit design. Wolff's law states that bone remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
Question 11High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen.
REFERENCES: Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
REFERENCES: Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 12High Yield
Advantages of a resurfacing metal-on-metal hip arthroplasty over a large diameter metal-on-metal total hip arthroplasty include which of the following?
Explanation
DISCUSSION: A resurfacing hip arthroplasty preserves bone stock in the proximal femur, at the expense of a higher reoperation rate because of component loosening and femoral neck fracture. Wear rate is the same as both types of hip arthroplasty use a large head metal-on-metal bearing surface.
REFERENCES: Shimmin A, Beaule PE, Campbell P: Metal-on-metal hip resurfacing arthroplasty. J Bone Joint Surg Am 2008;90:637-654.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65.
REFERENCES: Shimmin A, Beaule PE, Campbell P: Metal-on-metal hip resurfacing arthroplasty. J Bone Joint Surg Am 2008;90:637-654.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65.
Question 13High Yield
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
Achilles tendon tension is not affected by knee position when the ankle is in 20° to 25° of plantar flexion. Skin perfusion overlying the Achilles tendon is maximal in 20° of plantar flexion and is reduced beyond 20° of plantar flexion. Neutral flexion or any amount of dorsiflexion compromises the repair.
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
Question 14High Yield
A 24-year-old right-hand-dominant professional baseball pitcher has valgus extension overload (VEO) syndrome of the right elbow, as seen in Figure 7. Which letter in the figure corresponds to the typical area of osteophyte formation in this condition?

Explanation
VEO most commonly is seen in throwers for whom valgus stress across the elbow causes impingement of the posteromedial olecranon tip against the medial wall of the olecranon fossa. With repeated impingement, a bony osteophyte may grow on the olecranon at the site of impingement in this posteromedial region of the olecranon. Bony growth within the olecranon
fossa also has been seen. The distinction between this condition and ulnar collateral ligament injury is difficult to make, but VEO often can be distinguished from UCL injury by determining the exact location of pain a patient experiences. With VEO, the pain typically occurs with direct palpation of the posterior medial tip of the olecranon. The valgus extension overload provocative test also aids in diagnosis. A supervised physical therapy program and arthroscopic surgical decompression when nonsurgical treatment is unsuccessful are typical treatments for this condition.
Locations C and D represent the origin and insertion, respectively, of the elbow medial collateral ligament (MCL) structure, and, although associated MCL pathology can exist in the setting of VEO syndrome, osteophyte formation is not typical in these areas. Location A is the radial head, and although the radiocapitellar joint is a known secondary stabilizer of elbow valgus stress, osteophyte formation in this area is less likely in this clinical scenario.
RECOMMENDED READINGS
8. [Reddy AS, Kvitne RS, Yocum LA, Elattrache NS, Glousman RE, Jobe FW. Arthroscopy of the elbow: a long-term clinical review. Arthroscopy. 2000 Sep;16(6):588-94. ](http://www.ncbi.nlm.nih.gov/pubmed/10976118)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976118)
9. [Andrews JR, Craven WM. Lesions of the posterior compartment of the elbow. Clin Sports Med. 1991 Jul;10(3):637-52. Review. PubMed PMID: 1868565.](http://www.ncbi.nlm.nih.gov/pubmed/1868565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1868565)
10. [Wilson FD, Andrews JR, Blackburn TA, McCluskey G. Valgus extension overload in the pitching elbow. Am J Sports Med. 1983 Mar-Apr;11(2):83-8. ](http://www.ncbi.nlm.nih.gov/pubmed/6846685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6846685)
fossa also has been seen. The distinction between this condition and ulnar collateral ligament injury is difficult to make, but VEO often can be distinguished from UCL injury by determining the exact location of pain a patient experiences. With VEO, the pain typically occurs with direct palpation of the posterior medial tip of the olecranon. The valgus extension overload provocative test also aids in diagnosis. A supervised physical therapy program and arthroscopic surgical decompression when nonsurgical treatment is unsuccessful are typical treatments for this condition.
Locations C and D represent the origin and insertion, respectively, of the elbow medial collateral ligament (MCL) structure, and, although associated MCL pathology can exist in the setting of VEO syndrome, osteophyte formation is not typical in these areas. Location A is the radial head, and although the radiocapitellar joint is a known secondary stabilizer of elbow valgus stress, osteophyte formation in this area is less likely in this clinical scenario.
RECOMMENDED READINGS
8. [Reddy AS, Kvitne RS, Yocum LA, Elattrache NS, Glousman RE, Jobe FW. Arthroscopy of the elbow: a long-term clinical review. Arthroscopy. 2000 Sep;16(6):588-94. ](http://www.ncbi.nlm.nih.gov/pubmed/10976118)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976118)
9. [Andrews JR, Craven WM. Lesions of the posterior compartment of the elbow. Clin Sports Med. 1991 Jul;10(3):637-52. Review. PubMed PMID: 1868565.](http://www.ncbi.nlm.nih.gov/pubmed/1868565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1868565)
10. [Wilson FD, Andrews JR, Blackburn TA, McCluskey G. Valgus extension overload in the pitching elbow. Am J Sports Med. 1983 Mar-Apr;11(2):83-8. ](http://www.ncbi.nlm.nih.gov/pubmed/6846685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6846685)
Question 15High Yield
A 4-year-old child has droopy shoulders. Examination shows that the child has a large head, short stature, and a narrow chest. Radiographs of the spine and chest show absent clavicles, delayed ossification of the pubis and ischium, and mild coxa vara. What is the inheritance pattern for this condition?
Explanation
DISCUSSION: The child has the clinical and radiographic features of cleidocranial dysostosis. This is a disorder of bones formed by intramembranous ossification. It is inherited as an autosomal-dominant condition. About two thirds of cases are familial.
REFERENCES: Dietz FR, Mathews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Joint Bone Surg Am 1996;78:1583-1598.
Lee B, Thirunavukkarasu K, Zhou L, et al: Missense mutations abolishing DNA binding of osteoblast- specific transcription factor OSF2/CBFA1 in cleidocranial dysplasia. Nat Genet 1997;16:307-310.
cU.u^Ml**_[**ORTHO MCQS 011 FREE BANK 02**](http://hutaifortho.com/878)_**
---
**_[**ORTHO MCQS 011 FREE BANK**](http://hutaifortho.com/877)_**
**_[**Orthopedic MCQS online Hip and knee ADULT...**](http://hutaifortho.com/876)_**
**_[**ORTHOPEDIC MCQS OB 20 TRAUMA1**](http://hutaifortho.com/875)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC5**](http://hutaifortho.com/874)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC7**](http://hutaifortho.com/873)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 6**](http://hutaifortho.com/872)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 44**](http://hutaifortho.com/871)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 4**](http://hutaifortho.com/870)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 3**](http://hutaifortho.com/869)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 2**](http://hutaifortho.com/868)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 1**](http://hutaifortho.com/867)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4**](http://hutaifortho.com/865)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3**](http://hutaifortho.com/864)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2**](http://hutaifortho.com/863)_**
**_[**1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW**](http://hutaifortho.com/862)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01**](http://hutaifortho.com/861)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01**](http://hutaifortho.com/860)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01**](http://hutaifortho.com/859)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02**](http://hutaifortho.com/858)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02**](http://hutaifortho.com/857)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02**](http://hutaifortho.com/856)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER FOOT 03**](http://hutaifortho.com/855)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPINE 03**](http://hutaifortho.com/854)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03**](http://hutaifortho.com/853)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER HIP 04**](http://hutaifortho.com/852)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER PEDS 04**](http://hutaifortho.com/851)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPORT 04**](http://hutaifortho.com/850)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05**](http://hutaifortho.com/849)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05**](http://hutaifortho.com/848)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05**](http://hutaifortho.com/847)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06**](http://hutaifortho.com/846)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...**](http://hutaifortho.com/845)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06**](http://hutaifortho.com/844)_**
**_[**ORTHOPEDIC MCQS with Answers ONLINE BASIC 06**](http://hutaifortho.com/843)_**
**_[**ORTHOPEDIC MCQS ONLINE PEDIATRICS 07**](http://hutaifortho.com/842)_**
**_[**ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07**](http://hutaifortho.com/841)_**
**_[**ONLINE ORTHOPEDIC MCQS SPORT07**](http://hutaifortho.com/840)_**
**_[**ONLINE ORTHOPEDIC MCQS UPPER LIMB08**](http://hutaifortho.com/839)_**
**_[**ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08**](http://hutaifortho.com/838)_**
**_[**ONLINE ORTHOPEDIC MCQS ANATOMY08**](http://hutaifortho.com/837)_**
**_[**ONLINE ORTHOPEDIC MCQS FOOT0 9**](http://hutaifortho.com/836)_**
**_[**ONLINE ORTHOPEDIC MCQS SPINE0 9**](http://hutaifortho.com/835)_**
**_[**ONLINE ORTHOPEDIC MCQS TRAUMA 9**](http://hutaifortho.com/834)_**
**_[**Orthopedic MCQS online sports Medicine**](http://hutaifortho.com/833)_**
**_[**Orthopedic MCQS online Shoulder and Elbow**](http://hutaifortho.com/832)_**
**_[**Orthopedic MCQS online Hip and knee**](http://hutaifortho.com/831)_**
**_[**online orthopedic mcqs**](http://hutaifortho.com/830)_**
**_[**Shoulder and elbow: Mcqs AND EMQS Answers**](http://hutaifortho.com/766)_**
**_[**Shoulder And Elbow: Questions Mcqs AND EMQS**](http://hutaifortho.com/765)_**
**_[**Hand and wrist: Answers MCQS EMQS**](http://hutaifortho.com/764)_**
**_[**Hand and wrist: MCQ AND EMQ Questions**](http://hutaifortho.com/763)_**
**_[**2021 SHOULDER AND ELBOW MCQS FREE**](http://hutaifortho.com/689)_**
**_[**Pediatric Orthopaedic MCQS Self-Assessment...**](http://hutaifortho.com/685)_**
**_[**Self-Assessment Examination 2020 Adult Spine MCQS**](http://hutaifortho.com/684)_**
**_[**Foot and Ankle free MCQS2020 Online**](http://hutaifortho.com/681)_**
**_[**UPDATED ORTHOPEDIC MCQS**](http://hutaifortho.com/680)_**
**_[**FREE Orthopedics MCQS 2022 1951.-2000.**](http://hutaifortho.com/677)_**
**_[**FREE Orthopedics MCQS 2022 1901.-1950.**](http://hutaifortho.com/676)_**
**_[**FREE Orthopedics MCQS 2022 1851-1900.**](http://hutaifortho.com/675)_**
**_[**FREE Orthopedics MCQS 2022 1751-1850..**](http://hutaifortho.com/674)_**
**_[**FREE Orthopedics MCQS 2022 1751-1800..**](http://hutaifortho.com/673)_**
**_[**Foot and Ankle FREE ORTHOPEDICS MCQS Question 11**](http://hutaifortho.com/672)_**
**_[**FREE Orthopedics MCQS 2022 1701-1750.**](http://hutaifortho.com/668)_**
**_[**FREE Orthopedics MCQS 2022 1651-1700**](http://hutaifortho.com/667)_**
**_[**FREE Orthopedics MCQS 2022 1601-1650.**](http://hutaifortho.com/666)_**
**_[**ORTHOPEDIC MCQS FREE 2023**](http://hutaifortho.com/665)_**
**_[**FREE Orthopedics MCQS 2022 1551-1600**](http://hutaifortho.com/664)_**
**_[**FREE Orthopedics MCQS 2022 1501-1550**](http://hutaifortho.com/663)_**
**_[**FREE Orthopedics MCQS 2022 1451-1500**](http://hutaifortho.com/662)_**
**_[**FREE Orthopedics MCQS 2022 1401-1450**](http://hutaifortho.com/661)_**
**_[**FREE Orthopedics MCQS 2022 1351 -1400**](http://hutaifortho.com/660)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350**](http://hutaifortho.com/659)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300**](http://hutaifortho.com/658)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200**](http://hutaifortho.com/656)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150**](http://hutaifortho.com/655)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100**](http://hutaifortho.com/654)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051**](http://hutaifortho.com/653)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 951-1000**](http://hutaifortho.com/652)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 901-950**](http://hutaifortho.com/651)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 851-900**](http://hutaifortho.com/650)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 800-850**](http://hutaifortho.com/649)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 751-800**](http://hutaifortho.com/647)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 701-750**](http://hutaifortho.com/646)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 651-700**](http://hutaifortho.com/645)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 601-650**](http://hutaifortho.com/644)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 551-600**](http://hutaifortho.com/643)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 501-550**](http://hutaifortho.com/642)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 451-500**](http://hutaifortho.com/641)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 401-450**](http://hutaifortho.com/640)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 351-400**](http://hutaifortho.com/639)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 301-350**](http://hutaifortho.com/638)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 251-300**](http://hutaifortho.com/637)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 201-250**](http://hutaifortho.com/636)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 151-200**](http://hutaifortho.com/635)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 101-150**](http://hutaifortho.com/634)_**
**_[**FREE Orthopedics MCQS 2022 51-100**](http://hutaifortho.com/633)_**
**_[**Orthopedics Hyperguide MCQ 1-50**](http://hutaifortho.com/631)_**
DISCUSSION: The child has the clinical and radiographic features of cleidocranial dysostosis. This is a disorder of bones formed by intramembranous ossification. It is inherited as an autosomal-dominant condition. About two thirds of cases are familial.
REFERENCES: Dietz FR, Mathews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Joint Bone Surg Am 1996;78:1583-1598.
Lee B, Thirunavukkarasu K, Zhou L, et al: Missense mutations abolishing DNA binding of osteoblast- specific transcription factor OSF2/CBFA1 in cleidocranial dysplasia. Nat Genet 1997;16:307-310.
cU.u^Ml
---
**_[**ORTHO MCQS 011 FREE BANK**](http://hutaifortho.com/877)_**
**_[**Orthopedic MCQS online Hip and knee ADULT...**](http://hutaifortho.com/876)_**
**_[**ORTHOPEDIC MCQS OB 20 TRAUMA1**](http://hutaifortho.com/875)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC5**](http://hutaifortho.com/874)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC7**](http://hutaifortho.com/873)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 6**](http://hutaifortho.com/872)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 44**](http://hutaifortho.com/871)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 4**](http://hutaifortho.com/870)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 3**](http://hutaifortho.com/869)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 2**](http://hutaifortho.com/868)_**
**_[**ORTHOPEDIC MCQS OB 20 BASIC 1**](http://hutaifortho.com/867)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4**](http://hutaifortho.com/865)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3**](http://hutaifortho.com/864)_**
**_[**ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2**](http://hutaifortho.com/863)_**
**_[**1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW**](http://hutaifortho.com/862)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01**](http://hutaifortho.com/861)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01**](http://hutaifortho.com/860)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01**](http://hutaifortho.com/859)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02**](http://hutaifortho.com/858)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02**](http://hutaifortho.com/857)_**
**_[**ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02**](http://hutaifortho.com/856)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER FOOT 03**](http://hutaifortho.com/855)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPINE 03**](http://hutaifortho.com/854)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03**](http://hutaifortho.com/853)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER HIP 04**](http://hutaifortho.com/852)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER PEDS 04**](http://hutaifortho.com/851)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER SPORT 04**](http://hutaifortho.com/850)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05**](http://hutaifortho.com/849)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05**](http://hutaifortho.com/848)_**
**_[**ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05**](http://hutaifortho.com/847)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06**](http://hutaifortho.com/846)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...**](http://hutaifortho.com/845)_**
**_[**ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06**](http://hutaifortho.com/844)_**
**_[**ORTHOPEDIC MCQS with Answers ONLINE BASIC 06**](http://hutaifortho.com/843)_**
**_[**ORTHOPEDIC MCQS ONLINE PEDIATRICS 07**](http://hutaifortho.com/842)_**
**_[**ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07**](http://hutaifortho.com/841)_**
**_[**ONLINE ORTHOPEDIC MCQS SPORT07**](http://hutaifortho.com/840)_**
**_[**ONLINE ORTHOPEDIC MCQS UPPER LIMB08**](http://hutaifortho.com/839)_**
**_[**ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08**](http://hutaifortho.com/838)_**
**_[**ONLINE ORTHOPEDIC MCQS ANATOMY08**](http://hutaifortho.com/837)_**
**_[**ONLINE ORTHOPEDIC MCQS FOOT0 9**](http://hutaifortho.com/836)_**
**_[**ONLINE ORTHOPEDIC MCQS SPINE0 9**](http://hutaifortho.com/835)_**
**_[**ONLINE ORTHOPEDIC MCQS TRAUMA 9**](http://hutaifortho.com/834)_**
**_[**Orthopedic MCQS online sports Medicine**](http://hutaifortho.com/833)_**
**_[**Orthopedic MCQS online Shoulder and Elbow**](http://hutaifortho.com/832)_**
**_[**Orthopedic MCQS online Hip and knee**](http://hutaifortho.com/831)_**
**_[**online orthopedic mcqs**](http://hutaifortho.com/830)_**
**_[**Shoulder and elbow: Mcqs AND EMQS Answers**](http://hutaifortho.com/766)_**
**_[**Shoulder And Elbow: Questions Mcqs AND EMQS**](http://hutaifortho.com/765)_**
**_[**Hand and wrist: Answers MCQS EMQS**](http://hutaifortho.com/764)_**
**_[**Hand and wrist: MCQ AND EMQ Questions**](http://hutaifortho.com/763)_**
**_[**2021 SHOULDER AND ELBOW MCQS FREE**](http://hutaifortho.com/689)_**
**_[**Pediatric Orthopaedic MCQS Self-Assessment...**](http://hutaifortho.com/685)_**
**_[**Self-Assessment Examination 2020 Adult Spine MCQS**](http://hutaifortho.com/684)_**
**_[**Foot and Ankle free MCQS2020 Online**](http://hutaifortho.com/681)_**
**_[**UPDATED ORTHOPEDIC MCQS**](http://hutaifortho.com/680)_**
**_[**FREE Orthopedics MCQS 2022 1951.-2000.**](http://hutaifortho.com/677)_**
**_[**FREE Orthopedics MCQS 2022 1901.-1950.**](http://hutaifortho.com/676)_**
**_[**FREE Orthopedics MCQS 2022 1851-1900.**](http://hutaifortho.com/675)_**
**_[**FREE Orthopedics MCQS 2022 1751-1850..**](http://hutaifortho.com/674)_**
**_[**FREE Orthopedics MCQS 2022 1751-1800..**](http://hutaifortho.com/673)_**
**_[**Foot and Ankle FREE ORTHOPEDICS MCQS Question 11**](http://hutaifortho.com/672)_**
**_[**FREE Orthopedics MCQS 2022 1701-1750.**](http://hutaifortho.com/668)_**
**_[**FREE Orthopedics MCQS 2022 1651-1700**](http://hutaifortho.com/667)_**
**_[**FREE Orthopedics MCQS 2022 1601-1650.**](http://hutaifortho.com/666)_**
**_[**ORTHOPEDIC MCQS FREE 2023**](http://hutaifortho.com/665)_**
**_[**FREE Orthopedics MCQS 2022 1551-1600**](http://hutaifortho.com/664)_**
**_[**FREE Orthopedics MCQS 2022 1501-1550**](http://hutaifortho.com/663)_**
**_[**FREE Orthopedics MCQS 2022 1451-1500**](http://hutaifortho.com/662)_**
**_[**FREE Orthopedics MCQS 2022 1401-1450**](http://hutaifortho.com/661)_**
**_[**FREE Orthopedics MCQS 2022 1351 -1400**](http://hutaifortho.com/660)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350**](http://hutaifortho.com/659)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300**](http://hutaifortho.com/658)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200**](http://hutaifortho.com/656)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150**](http://hutaifortho.com/655)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100**](http://hutaifortho.com/654)_**
**_[**ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051**](http://hutaifortho.com/653)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 951-1000**](http://hutaifortho.com/652)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 901-950**](http://hutaifortho.com/651)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 851-900**](http://hutaifortho.com/650)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 800-850**](http://hutaifortho.com/649)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 751-800**](http://hutaifortho.com/647)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 701-750**](http://hutaifortho.com/646)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 651-700**](http://hutaifortho.com/645)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 601-650**](http://hutaifortho.com/644)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 551-600**](http://hutaifortho.com/643)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 501-550**](http://hutaifortho.com/642)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 451-500**](http://hutaifortho.com/641)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 401-450**](http://hutaifortho.com/640)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 351-400**](http://hutaifortho.com/639)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 301-350**](http://hutaifortho.com/638)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 251-300**](http://hutaifortho.com/637)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 201-250**](http://hutaifortho.com/636)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 151-200**](http://hutaifortho.com/635)_**
**_[**ORTHOPEDICS HYPERGUIDE MCQ 101-150**](http://hutaifortho.com/634)_**
**_[**FREE Orthopedics MCQS 2022 51-100**](http://hutaifortho.com/633)_**
**_[**Orthopedics Hyperguide MCQ 1-50**](http://hutaifortho.com/631)_**
Question 16High Yield
A right-hand dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
Explanation
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on the radial tuberosity.
41
41
Question 17High Yield
A 75-year-old man with a 4-part proximal humerus fracture and comminuted tuberosities
Explanation
- Reverse total shoulder arthroplasty (rTSA)_
Question 18High Yield
A 45-year-old man presents to your clinic with a closed mid-shaft humerus fracture after a fall 1 week prior. He is neurovascularly intact. After a discussion of his treatment options, he is adamant about proceeding with surgical management. With respect to open reduction and internal fixation with a plate versus intramedullary nailing, what advice can you offer him?

Explanation
Current literature on the management of humeral shaft fractures shows no difference in the rate of radial nerve palsy between nailing (IMN) or with plate fixation (ORIF).
Both ORIF and IMN are appropriate means of definitive fixation of diaphyseal humeral fractures. Numerous studies have directly compared the risks and
outcomes associated with each of the two methods, and the current literature supports that there is no difference in the rates of fracture union, radial nerve palsy, or surgical site infection. Findings on overall complication rates have varied among the literature. In some studies however, IMN has been associated with an increased rate of shoulder pain and as a result a higher reoperation rate as compared to ORIF, though functional outcomes at 1-year show no difference.
Zhao et al. performed a systematic review of recent meta-analyses of randomized clinical trials (RCTs) to compare IMN and plate fixation for treatment humeral shaft fractures. The authors concluded that there was no difference between IMN and plate fixation with respect to fracture union, radial nerve injury, or infection. But they did note that IMN significantly increased the risk of shoulder complications (shoulder impingement and shoulder ROM) and reoperation.
Chen et al. performed a retrospective cohort study evaluating the incidence of humeral shaft fractures within the non-cancer Medicare population and comparing differences between IMN and plate fixation with respect to procedure times, secondary operations, and 1-year mortality. The authors found that IMN was performed more often than plate fixation most years over a 15-year period and was associated with significantly less anesthesia time (27.1 minutes, P < 0.0001). They concluded that there were no significant differences in the complication rates between the 2 groups as measured by the incidence of secondary operations and 1-year mortality.
Bisaccia et al. compared IMN, ORIF, and external fixation for the treatment of midshaft humeral fractures in 79 patients with a median follow-up of 11.5 months. The authors performed clinical and radiographic evaluation at 6 weeks, 6 months and 12 months. They found no differences in the duration of hospitalization, SF-36 scores, or complications between the 3 treatment arms. There were 2 cases of non-union in the ORIF group, 1 case in the IMN group and no cases in the external fixation group, and there was one case of transient radial nerve palsy in the IMN cohort.
Figure A is a radiograph showing a displaced transverse midshaft humeral fracture.
Incorrect Answers:
Answer 1: Though some studies have suggested an increased rate of shoulder-related complications with IMN fixation, there is not significant difference in the rate of surgical site infections for humeral shaft fractures when treated with IMN or ORIF.
Answer 2: There is no significant difference in the rate of radial nerve palsy among humeral shaft fractures treated with IMN or ORIF.
Answer 3: There is no difference in the rate of fracture union for humeral shaft fractures treated with IMN or ORIF.
Answer 3: Some studies have found an increased rate of shoulder complications such as pain and impingement with IMN fixation, leading to an increased rate of revision surgery. However many large meta-analyses contradict these findings.
Both ORIF and IMN are appropriate means of definitive fixation of diaphyseal humeral fractures. Numerous studies have directly compared the risks and
outcomes associated with each of the two methods, and the current literature supports that there is no difference in the rates of fracture union, radial nerve palsy, or surgical site infection. Findings on overall complication rates have varied among the literature. In some studies however, IMN has been associated with an increased rate of shoulder pain and as a result a higher reoperation rate as compared to ORIF, though functional outcomes at 1-year show no difference.
Zhao et al. performed a systematic review of recent meta-analyses of randomized clinical trials (RCTs) to compare IMN and plate fixation for treatment humeral shaft fractures. The authors concluded that there was no difference between IMN and plate fixation with respect to fracture union, radial nerve injury, or infection. But they did note that IMN significantly increased the risk of shoulder complications (shoulder impingement and shoulder ROM) and reoperation.
Chen et al. performed a retrospective cohort study evaluating the incidence of humeral shaft fractures within the non-cancer Medicare population and comparing differences between IMN and plate fixation with respect to procedure times, secondary operations, and 1-year mortality. The authors found that IMN was performed more often than plate fixation most years over a 15-year period and was associated with significantly less anesthesia time (27.1 minutes, P < 0.0001). They concluded that there were no significant differences in the complication rates between the 2 groups as measured by the incidence of secondary operations and 1-year mortality.
Bisaccia et al. compared IMN, ORIF, and external fixation for the treatment of midshaft humeral fractures in 79 patients with a median follow-up of 11.5 months. The authors performed clinical and radiographic evaluation at 6 weeks, 6 months and 12 months. They found no differences in the duration of hospitalization, SF-36 scores, or complications between the 3 treatment arms. There were 2 cases of non-union in the ORIF group, 1 case in the IMN group and no cases in the external fixation group, and there was one case of transient radial nerve palsy in the IMN cohort.
Figure A is a radiograph showing a displaced transverse midshaft humeral fracture.
Incorrect Answers:
Answer 1: Though some studies have suggested an increased rate of shoulder-related complications with IMN fixation, there is not significant difference in the rate of surgical site infections for humeral shaft fractures when treated with IMN or ORIF.
Answer 2: There is no significant difference in the rate of radial nerve palsy among humeral shaft fractures treated with IMN or ORIF.
Answer 3: There is no difference in the rate of fracture union for humeral shaft fractures treated with IMN or ORIF.
Answer 3: Some studies have found an increased rate of shoulder complications such as pain and impingement with IMN fixation, leading to an increased rate of revision surgery. However many large meta-analyses contradict these findings.
Question 19High Yield
An 18-month-old boy is brought to your office for a clawing deformity of his right hand. The parents inform you that he was born full term after a difficult delivery complicated by shoulder dystocia. The boy weighed 9½ lbs at birth. The child had a brief episode of apnea with an APGAR score of 5 at birth and needed resuscitation and admission to the natal intensive care unit. Parents recall having noted a bump on his right clavicle, which was tender and was diagnosed as clavicle fracture. They also noticed a week later that the child did not flex the fingers of his right hand. The neonatologist had informed them that the
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
Explanation
This is a case of obstetric brachial plexus injury involving the C 8, T1 roots (Klumpke Palsy). Erbâs palsy involves upper roots only. C ombined nerve injuries can present in a similar fashion; however, low ulnar and median nerve lesions will not have weakness of flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS).
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
Question 20High Yield
A 34-year-old woman presents for treatment of pain in the hallux. She notes pain upon weight bearing and wearing high-heel shoes. Upon examination, the range of motion of the hallux metatarsophalangeal (MP) joint is 10° dorsiflexion and 30° plantarflexion, with pain upon passive dorsiflexion. Radiographs demonstrate osteophytes over the dorsal surface of the metatarsal head, maintenance of the joint space, and a metatarsal declination angle of 10°. The first metatarsal is elevated above the second metatarsal at the level of the metatarsal neck by 4 mm. The ideal procedure to correct this problem and alleviate pain is:
Explanation
This patient has mild hallux rigidus with a normal alignment of the first metatarsal. The average elevation of the first metatarsal above the second metatarsal at the level of the metatarsal neck is 7.5 mm, thus, 4 mm is within normal limits. Arthrodesis is not indicated for mild rigidus and osteotomy is indicated only for severe elevation of the first metatarsal. C heilectomy combined with osteotomy of the proximal phalanx (the Moberg osteotomy) is the preferred procedure.
Question 21High Yield
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event.
REFERENCES: Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Roy S, Caine D, Singer KM: Stress changes of the distal radial epiphysis in young gymnasts: A report of twenty-one cases and a review of the literature. Am J Sports Med 1985;13:301-308.
REFERENCES: Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Roy S, Caine D, Singer KM: Stress changes of the distal radial epiphysis in young gymnasts: A report of twenty-one cases and a review of the literature. Am J Sports Med 1985;13:301-308.
Question 22High Yield
Hallux rigidus is associated with:
Explanation
In a large series of patients with hallux rigidus, risk factors were evaluated. The only factor that had a positive correlation with having hallux rigidus was the radiographic shape of the 1st metatarsal head. Metatarsus primus elevatus, first ray hypermobility, or long first metatarsal head were not significantly associated with hallux rigidus.
Question 23High Yield
Figure 55 is the radiographs of a 37-year-old patient who reports pain and swelling over the lateral forefoot (fifth metatarsal) that has become progressively worse over time. Shoe wear modifications have not been successful. Based on the radiographs, what is the appropriate treatment at this time?
---
---

Explanation
The most appropriate treatment is a diaphyseal osteotomy. The patient has a painful bunionette with a large 4-5 intermetatarsal (IM) angle (a type 3 bunionette) that is best treated with a diaphyseal or proximal osteotomy. Exostectomy of the lateral eminence applies to type 1 bunionettes that can
also have a fifth hammer toe. A Chevron osteotomy is best used for a type 1 or 2 bunionette with a normal 4-5 IM angle. A metatarsal head resection is not indicated as a primary procedure for a bunionette,especially in a younger patient because it sacrifices the fifth metatarsophalangel joint.
also have a fifth hammer toe. A Chevron osteotomy is best used for a type 1 or 2 bunionette with a normal 4-5 IM angle. A metatarsal head resection is not indicated as a primary procedure for a bunionette,especially in a younger patient because it sacrifices the fifth metatarsophalangel joint.
Question 24High Yield
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
Osteolysis of the distal clavicle is common in weightlifters; therefore, distal clavicle excision is the treatment of choice. A subacromial decompression alone would not alleviate the acromioclavicular joint symptoms. Interval closure, biceps degeneration, and superior labrum anterior and posterior repair would limit superior migration but would not explain the abnormal bone scan. Thermal capsular shrinkage does not have a role here.
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 25High Yield
As the most direct and predictable preoperative diagnostiCtest for hip infection, the false-positive rate for hip aspiration is:
Explanation
Hip aspiration has a false-positive rate of 0% to 15%. Many authors have warned against its routine use before revision surgery
Question 26High Yield
What condition favors pollicization in hypoplasia of the thumb?
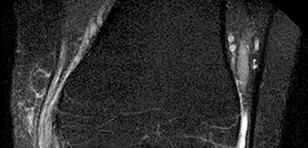
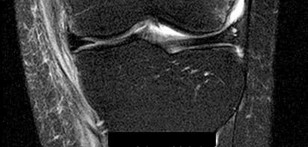
Explanation
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
Question 27High Yield
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
The anterior border of the PCL is the most accurate and reproducible landmark for appropriate placement of the tibial tunnel for an ACL reconstruction. The central sagittal insertion point of the ACL is consistently 10 to 11 mm anterior to the anterior border of the PCL ligament. The anterior border of the tibia is not well visualized and does not serve as a reference point. While the posterior border of the anterior horn of the lateral meniscus could be used as a reference point, it has twice the variability of the PCL reference point. The posterior border of the tibia is difficult to identify and has greater variability than the PCL relative to the AP dimension of the proximal tibial surface. The anterior horn of the medial meniscus is also more variable than the PCL.
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 28High Yield
A 12-year-old boy is seen 1 week after injuring his knee while playing soccer. He notes pain and swelling. Examination reveals an effusion, laxity with Lachman testing, and he walks with a limp. Radiographs and an MRI scan are shown in Figures 95a through 95d. Treatment should consist of which of the following?

Explanation
DISCUSSION: The radiographs and MRI scan show a displaced tibial eminence fracture. Meyer and McKeever classified these injuries, with type 1 being a nondisplaced tibial eminence fracture; type 2 being a displaced tibial eminence fracture with a posterior hinge, and type 3 being a displaced tibial eminence fracture. Tibial eminence fractures in children are equivalent to anterior cruciate ligament tears in adults. Treatment should be anatomic reduction, which often requires an arthroscopic or open procedure, followed by fixation.
REFERENCES: Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp xvi, 452-455, 638.
Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-355.
2010 Pediatric Orthopaedic Examination Answer Book • 79
Figure 96
REFERENCES: Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp xvi, 452-455, 638.
Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-355.
2010 Pediatric Orthopaedic Examination Answer Book • 79
Figure 96
Question 29High Yield
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
[9/. PubMed PMID: 16166889.](http://www.ncbi.nlm.nih.gov/pubmed/16166889)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16166889)
[Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976). 2006 Sep 15;31(20):2359-66. PubMed PMID: 16985465.](http://www.ncbi.nlm.nih.gov/pubmed/16985465)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985465)
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
[9/. PubMed PMID: 16166889.](http://www.ncbi.nlm.nih.gov/pubmed/16166889)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16166889)
[Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976). 2006 Sep 15;31(20):2359-66. PubMed PMID: 16985465.](http://www.ncbi.nlm.nih.gov/pubmed/16985465)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16985465)
Question 30High Yield
Figures 1 and 2 are the radiographs of a 64-year-old woman with a history of rheumatoid arthritis (RA) who complains of right elbow pain. She has been treated with tumor necrosis factor-alpha inhibitors and oral corticosteroids for several years. What process is primarily responsible for the radiographic joint destruction?
Explanation
RA is a systemic inflammatory disorder marked by erosive arthritis in multiple joints. Elbow involvement is common. The pathologic lesion in RA is pannus, a hyperplastic synovial proliferation that ultimately results in proteoglycan and collagen digestion. Rheumatoid factor mutations, traumatic insults resulting in complement activation, and osteoblast paracrine signaling are not involved in the pathologic process. The Larsen classification assesses the progression of rheumatoid changes in the elbow. Stage I is characterized by osteopenia without joint space narrowing. Stage II indicates joint space narrowing but a normal joint contour. Stage III is marked by joint space loss. This patient has stage IV disease, as seen by the advanced erosive changes with trochlear groove deepening and resulting deformity. Stage V is ankylosis.
68
68
Question 31High Yield
A 86-year-old man slips on the ice and falls sustaining the injury shown in Figure A. He has Type 2 diabetes mellitus, atrial fibrillation, coronary artery disease, end-stage renal disease on dialysis and chronic obstructive lung disease. All of the following variables are associated with increased mortality at one year after injury EXCEPT?

Explanation
Operative fixation within 48 hours is not associated with increased mortality. However, operative delay of 3 or more days results in increased mortality.
Medical optimization and surgery for hip fractures in elderly patients should be performed as soon as possible following admission to hospital. Surgical intervention in elderly hip fracture patients reduces morbidity and mortality.
Postoperatively, weightbearing as tolerated decreases the risk for poor outcomes and decreases complications e.g. muscle atrophy, pressure sores, pneumonia, urinary retention.
Zuckerman et al. reviewed mortality associated with operative delay in older patients with hip fractures. They found that operative delay of 3 or more calendar days results in greater 1-year mortality. Other predictors of mortality include age >85yrs, male sex, presence of 2 or more pre-existing medical conditions, ASA grade III or IV, and inter-trochanteric fracture.
Switzer et al. reviewed perioperative considerations in the geriatric patient. They showed that hip fracture repair after 2 days results in decrease in independent living, pressure sores and longer hospital stay. They found with early surgery, pain, length of hospital stay and 1-month mortality was reduced.
Figure A shows unstable intertrochanteric fracture. Incorrect Answers:
Answers 1, 2, 3: These conditions are all associated with increased 1-year
mortality.
Answer 4: One-year mortality after hip fracture is greater in men (25-30%) than in women (20%).
Medical optimization and surgery for hip fractures in elderly patients should be performed as soon as possible following admission to hospital. Surgical intervention in elderly hip fracture patients reduces morbidity and mortality.
Postoperatively, weightbearing as tolerated decreases the risk for poor outcomes and decreases complications e.g. muscle atrophy, pressure sores, pneumonia, urinary retention.
Zuckerman et al. reviewed mortality associated with operative delay in older patients with hip fractures. They found that operative delay of 3 or more calendar days results in greater 1-year mortality. Other predictors of mortality include age >85yrs, male sex, presence of 2 or more pre-existing medical conditions, ASA grade III or IV, and inter-trochanteric fracture.
Switzer et al. reviewed perioperative considerations in the geriatric patient. They showed that hip fracture repair after 2 days results in decrease in independent living, pressure sores and longer hospital stay. They found with early surgery, pain, length of hospital stay and 1-month mortality was reduced.
Figure A shows unstable intertrochanteric fracture. Incorrect Answers:
Answers 1, 2, 3: These conditions are all associated with increased 1-year
mortality.
Answer 4: One-year mortality after hip fracture is greater in men (25-30%) than in women (20%).
Question 32High Yield
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
Explanation
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma _but would not lead to the clinical condition this patient has._
Question 33High Yield
In congenital lesions characterized by failure of formation of parts, the most functional, without treatment, is/are:
Explanation
C entral deficiencies allow a wide grasp, good release and pinch. These are also termed "cleft hand". The other conditions produce greater impairment.
Question 34High Yield
..A 45-year-old woman has a 3-month history of left shoulder pain. She has tried 2 months of physical therapy focused on rotator cuff strengthening without experiencing relief. A subacromial corticosteroid injection fails to provide lasting relief. Examination reveals no atrophy or winging. She has anterior and posterior shoulder tenderness, full symmetric forward elevation and abduction, and pain with maximal passive forward elevation. She has pain with internal rotation in 90 degrees of forward elevation.
She has an increased distance between the antecubital fossa and coracoid process with cross chest adduction compared to the contralateral side. No weakness is appreciated. Radiographs reveal a type II acromion. What is the best next step?
She has an increased distance between the antecubital fossa and coracoid process with cross chest adduction compared to the contralateral side. No weakness is appreciated. Radiographs reveal a type II acromion. What is the best next step?
Explanation
- Posterior capsular stretching
CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 49
A 13-year-old pitcher reports the immediate onset of medial elbow pain after throwing a pitch. Upon examination, the patient is tender to palpation at the medial epicondyle and has pain and instability with valgus testing of the elbow.
CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 49
A 13-year-old pitcher reports the immediate onset of medial elbow pain after throwing a pitch. Upon examination, the patient is tender to palpation at the medial epicondyle and has pain and instability with valgus testing of the elbow.
Question 35High Yield
Figure 1 is the T2 coronal MRI scan(Massive atraumatic rotator cuff tear) of a 52-year-old woman with
a 6-month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
a 6-month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
The MRI reveals a large full thickness supraspinatus tear. A large, prospective study showed that physical therapy can be effective in the treatment of atraumatic full-thickness rotator cuff tears. Patient expectations regarding the role of rehabilitation were the strongest predictor of surgery. Other factors associated with surgery were higher activity level and not smoking. Anatomic features of the rotator
cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
Question 36High Yield
An 18-year-old male wrestler is injured while picking up an opponent over his head. Witnesses observed his knee buckle out from under him. He is immediately taken to the hospital. On physical examination, his knee is swollen and grossly unstable in multiple planes. Radiographs reveal a located joint without fracture. Distal pulses are palpable. What is the best next step?
67
67
Explanation
Multiple factors need to be considered in the setting of the acutely dislocated knee, but beyond the joint being located, the vascular status of the knee needs to be established to avoid an ischemic limb and possibility of amputation. While palpation for pulses certainly can be performed, an ABI should be performed first in this setting. The patient should be supine and ideally Doppler ultrasonography should be used to detect the pulse. ABI <0.9 has been demonstrated to be 100% sensitive and 100% specific for vascular injury (Mills and associates). Selective angiography can be employed if ABI measures indicate a possible injury. ABI measurements can be affected by existing distal arterial sclerosis or calcification, which would not be expected in this young patient. If pulses are absent or other hard ischemic signs are present, ABI can be foregone for operating room (OR) angiography or an equivalent study to determine the exact location of the vascular injury.
A missed compartment syndrome in the setting of a knee dislocation can be a devastating event leading to ischemia and limb dysfunction or tissue death leading to need for amputation. If a suspected compartment syndrome exists, compartment pressures can be measured directly after ABI, and if needed, compartments can be released in the OR in conjunction with vascular repair (if required). Urgent stabilization can also be done in the OR at the time of vascular repair but is not the most important priority in this setting. Angiograms can be performed in the OR to reduce warm ischemia time if ABI measures are concerning, with vascular repair if indicated. This has been superseded by CT-arteriogram in many trauma centers, which can be performed just prior to OR if indicated.
68
A missed compartment syndrome in the setting of a knee dislocation can be a devastating event leading to ischemia and limb dysfunction or tissue death leading to need for amputation. If a suspected compartment syndrome exists, compartment pressures can be measured directly after ABI, and if needed, compartments can be released in the OR in conjunction with vascular repair (if required). Urgent stabilization can also be done in the OR at the time of vascular repair but is not the most important priority in this setting. Angiograms can be performed in the OR to reduce warm ischemia time if ABI measures are concerning, with vascular repair if indicated. This has been superseded by CT-arteriogram in many trauma centers, which can be performed just prior to OR if indicated.
68
Question 37High Yield
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
An immediate appointment for magnetic resonance imagine (MRI) and computed tomography (C T) scan are not available, and a genetic evaluation has been carried out previously. As you await the report from the geneticist office, you decide to get a skeletal radiograph series on the patient. The radiograph of the opposite forearm (Slide 1) and right leg are shown (Slide 2).
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 3). Your suspected diagnosis is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
An immediate appointment for magnetic resonance imagine (MRI) and computed tomography (C T) scan are not available, and a genetic evaluation has been carried out previously. As you await the report from the geneticist office, you decide to get a skeletal radiograph series on the patient. The radiograph of the opposite forearm (Slide 1) and right leg are shown (Slide 2).
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 3). Your suspected diagnosis is:
Explanation
Diaphyseal achalasia, also called multiple hereditary exostoses, classically presents in a young individual with multiple sites of involvement. The more involved the disease, the more likely hand involvement becomes. Forearm involvement is also common. The radius is bowed due to the shortened ulna. The risk of radial head dislocation is higher if the radius does not bow. While infection or traumatic injury could have produced early physeal arrest as seen in the first radiograph, presence of lesions elsewhere indicates multiple hereditary exostoses and should be investigated with skeletal surveys. Multiple epiphyseal dysplasia is not a possible diagnosis as only the ulna is involved in the first radiograph and radius alone in the left forearm. No enchondromas are present.
Question 38High Yield
A 12-year-old patient with osteogenic sarcoma metastatic to the spine is noted to have new onset of weakness of both lower extremities. Magnetic resonance imaging shows a mass expanding posteriorly and encroaching on the spinal cord. The recommended initial step is:
Explanation
Radiation therapy combined with steroids should be tried first to try to halt progression of the tumor. Unfortunately, the prognosis for this child is extremely poor.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
Question 39High Yield
During an anterior approach to the bicipital 53
tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the
tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the





Explanation
The structure shown is the lateral antebrachial cutaneous nerve (LABC). It is the terminal sensory branch of the musculocutaneous nerve and runs superficial to the brachioradialis. It supplies sensation to the anterolateral surface of the forearm. The flexor pollicis longus is innervated by the anterior interosseous nerve. The extensor indicis proprius is innervated by the radial nerve. The LABC does not innervate the skin of the anteromedial forearm. Careful
identification and protection of this nerve is critical to prevent the most common nerve injury during distal biceps repair.
RECOMMENDED READINGS
1. Agur AM. Grant's Atlas of Human Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:460.
2. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1994:118-125.
RESPONSES FOR QUESTIONS 59 THROUGH 61
Please select the image that represents the most appropriate response to the question or statement below.
54
A B
C D
identification and protection of this nerve is critical to prevent the most common nerve injury during distal biceps repair.
RECOMMENDED READINGS
1. Agur AM. Grant's Atlas of Human Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:460.
2. Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1994:118-125.
RESPONSES FOR QUESTIONS 59 THROUGH 61
Please select the image that represents the most appropriate response to the question or statement below.
54
A B
C D
Question 40High Yield
This is the definition of translocation. Examples of translocation include Ewing's sarcoma, Rhabdomyosarcoma, and Synovial sarcoma
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?











Explanation
Etanercept is a biochemically designed tumor necrosis factor receptor immunoglobulin G fusion protein, which binds to TNF-alpha and is thus a TNF- alpha antagonist.
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its
receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and
malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-9.1) and for serious infection was
2.0 (95% CI, 1.3-3.1) with use of TNF-alpha antagonist.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Incorrect Answers:
: Rituximab is a monoclonal antibody to CD20 antigen (inhibits B cells). It is often used with good clinical outcomes as monotherapy in patients who are intolerant of methotrexate or have contraindications to methotrexate or other DMARDs.
Answer 3: Abatacept is a selective costimulation modulator that binds to CD80 and CD86 (inhibits T cells). It is often prescribed for treatment of moderate to severe rheumatoid arthritis, or after failure of a disease-modifying anti- rheumatic agent (DMARD), like methotrexate but it can be used as first-line therapy.
Answer 4: Methotrexate is a folic acid analogue. It binds dihydrofolate reductase and prevents synthesis of tetrahydrofolate. It is usually a first line treatment for moderate to severe rheumatoid arthritis.
Answer 5: Leflunomide is an inhibitor of pyrimidine synthesis. It is approved to treat adult moderate to severe rheumatoid arthritis, usually as a monotherapy or failure of other DMARDs.
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
1) As strain rate increases, both elastic modulus and ultimate strength increase
2) As strain rate increases, elastic modulus remains unchanged but ultimate strength increases
3) As strain rate increases, elastic modulus increases but ultimate strength decreases
4) As strain rate increases, both elastic modulus and ultimate strength decrease
5) As strain rate increases, elastic modulus increases but ultimate strength remains unchanged
As strain rate increases, both elastic modulus and ultimate strength increase. For LOW strain rates typical of normal activity (physiological strain rates of
0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress- strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone.
Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Illustration B shows that the ultimate strength and elastic modulus increase with rapid loading or deformation. The ultimate strength increases by roughly a factor of 3, while the elastic modulus increases by a factor of
approximately 2 over the strain rate range.
Incorrect Answers:
Answers 2, 3, 4, 5: As strain rate increases, elastic modulus and ultimate strength increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
In regards to a genetic disorder, which of the following is an example of "anticipation?"
1) Gene characteristics more severe and earlier in onset in subsequent generations
2) A disorder inherited from a genetic mutation specific to maternal DNA
3) Gene characteristics expressed to varying degrees in different individuals
4) Variation in the relative frequency of a genotype due to chance
5) The presence of an extra copy of a chromosome
Genetic anticipation is a phenomenon in which a genetic disorder becomes progressively more severe and earlier in onset with each generation. Examples of disorders exhibiting anticipation include Huntington's disease and myotonic dystrophy.
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Answer 2: "Genomic imprinting" is when a disorder is linked to a parent- specific origin. An example of maternal genomic imprinting is Angelman Syndrome. An example of paternal genomic imprinting is Prader Willi.
Answer 3: "Variable penetrance" is when gene characteristics are expressed in varying degrees.
Answer 4: "Genetic drift" is the chance variation in the relative frequency of a genotype within a population.
Answer 5: "Trisomy" is the presence of an extra copy of a chromosome. Down Syndrome is trisomy 21, which is due to an extra copy of chromosome 21.
A researcher is working on Medication A, a drug FDA-approved for the treatment of osteoporosis in men and women. It is an anti- resorptive agent that inhibits the formation, function and survival of osteoclasts. It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non- detectable. It can be used in the presence of cancer metastases to bone. What is Medication A?
1) Denosumab
2) Alendronate
3) Abaloparatide
4) Teriparatide
5) Strontium ranelate
Denosumab is FDA-approved for the treatment of osteoporosis in men and women. It inhibits the formation, function and survival of osteoclasts (OC). It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non-detectable.
Denosumab is a human monoclonal antibody against RANKL. By binding RANKL, it prevents interaction of RANKL with RANK (on OC and osteoclast precursors, OCP), and inhibits OC-mediated bone resorption, and the formation, function and survival of OC. In contrast, bisphosphonates bind to calcium hydroxyapatite in bone, and decrease resorption by decreasing function and survival (but not formation) of OC.
Vaananen et al. reviewed the cell biology of OC. During bone resorption, 3 membrane domains appear: ruffled border, sealing zone and functional secretory domain. The resorption cycle starts with migration, bone attachment, polarization (formation of membrane domains), dissolution of hydroxyapatite, degradation of organic matrix, removal of degradation
products from resorption lacuna, and apoptosis of the OC or return to the non- resorbing stage.
Boyce et al. reviewed the regulation of osteoclasts and their functions. OCPs are held in bone marrow by chemokines e.g. stroma-derived factor-1 (SDF1) and attracted to blood by sphingosine-1 phosphate (S1P) (increased in synovial fluid of patients with RA). All aspects of osteoclast formation and functions are regulated by M-CSF and RANKL. More recent studies indicate that osteoclasts and their precursors regulate immune
responses and
osteoblast formation and functions by means of direct cell-cell contact through ligands and receptors, such as ephrins and Ephs, and semaphorins and
plexins, and through expression of clastokines.
Warriner and Saag reviewed the diagnosis and treatment of osteoporosis. They defined osteoporosis as T-score of = -2.5 or a history of fragility fracture. Incident hip and vertebral fractures increase future risk of these fractures (hazard ratio 7.3 and 3.5, respectively).
Cummings et al. compared subcutaneous denosumab (60mg every 6mths) vs placebo in prevention of fractures in 7868 osteoporotic (T-score -2.5 to -4.0) postmenopausal women. They found that denosumab reduced risk of vertebral fracture by 68% (risk ratio, 0.32), hip fracture by 40% (hazard ratio 0.6), nonvertebral fracture by 20% (hazard ratio 0.8). There was no increased risk of cancer, infection, delayed fracture healing, cardiovascular disease, osteonecrosis of the jaw or adverse reactions. They concluded that it was useful for reduction of fractures in osteoporotic women.
The video shows the action of denosumab (prolia). Illustration A shows the different osteoclast zones.
Incorrect Answers:
Answers 2: Alendronate (and other bisphosphnates) inhibit resorption of bone, decrease function and survival of osteoclasts. Because of binding to calcium hydroxyapatite, they are detectable years after dosing. They reduce function and survival of OC, but do not affect the formation of osteoclasts.
Answer 3: Abaloparatide is a PTH analog that has completed phase III trials for osteoporosis. As of mid-2016, it is not yet approved for treatment of osteoporosis. Answer 4: Teriparatide (recombinant PTH 1-34) is the only anabolic (not antiresorptive) agent approved for osteoporosis treatment. It is administered by daily subcutaneous injection. Osteosarcoma, cancer metastases to bone and Paget's disease are contraindications.
Answer 5: Strontium ranelate (marketed as Protelos or Protos) both increases deposition of new bone by osteoblasts and reduces the resorption of bone by osteoclasts ("dual action bone agent", DABA). It is not FDA approved for use in the United States. Increased risk of myocardial infarction has been detected.
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
1) Patient Protection and Affordable Care Act
2) Medicare Payment Reform Act
3) Physician Financial Transparency Act
4) Physician Payments Sunshine Act
5) Health Insurance Portability and Accountability Act
The Physician Payments Sunshine Act requires all payments by corporations to physicians beyond $10 per year to be reported to the Centers for Medicare and Medicaid Services.
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Answers 1: The Patient Protection and Affordable Care Act (PPACA), known also by its shorter name of the Affordable Care Act (ACA) or it's nickname
"Obamacare", was passed in March 2010. The Sunshine Act was one of many provisions passed within the PPACA (after the Sunshine Act failed to pass on its own in prior years), but the PPACA focused primarily on improving the quality and affordability of healthcare insurance and lowering the costs of healthcare.
Answer 2: The Medicare Payment Reform Act of 1983 was a quickly drafted revision to the way Medicare payments were made, changing from fee-for- service to prospective payments allowing Medicare to determine payment amount rather than providers/hospitals.
Answer 3: This is a fictitious act.
Answer 5: HIPPA is the 1996 legislation defining standards and protections for patient private health information and electronic exchange of records.
Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?
1) Titanium
2) Cobalt-chrome alloy
3) Alumina
4) Zirconia
5) Stainless steel
Of the materials listed titanium (100GPa) has an elastic modulus closest to cortical bone (approximately 18GPa) as well as cancellous bone (approximately 2GPa).
Titanium is a material that is light, highly ductile, strong and corrosion resistant. However, titanium has poor wear resistance and is notch sensitive. It is commonly used as an orthopaedic implant materials because it has torsional and axial stiffness (moduli) that most closely mimics bone. Young’s modulus is constant and different for each material and represents the material's ability to maintain shape under external loading.
Rho et al found that the average Young's modulus for trabecular bone measured ultrasonically and mechanically was 14.8 GPa (S.D. 1.4) and 10.4 (S.D. 3.5), respectively. The average Young's modulus of microspecimens of cortical bone measured ultrasonically and mechanically was 20.7 GPa (S.D.
1.9) and 18.6 GPa (S.D. 3.5), respectively.
Illustration A depicts a stress vs. strain curve. The slope of the line in the elastic zone represents the Young Modulus of Elasticity.
Incorrect Answers:
Answer 2: Cobalt-chrome alloy is approximately 240 GPa Answer 3: Alumina is approximately 340 GPa
Answer 4: Zirconia (Ceramic) = 248 GPa
Answer 5: Stainless steel is approximately 240 GPa
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
1) VDDR I is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
2) VDDR I is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
3) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
4) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3.
5) VDDR I is a deficiency of an enzyme predominantly found in the liver. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to
1a,25(OH)2D3]. Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
Answers 1, 2, 4, 5: VDDR I is a deficiency of 1a-hydroxylase (predominantly
found in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
A 73-year-old female sustains a left hip fracture that is treated with hemiarthroplasty. She has continued pain two months after surgery, and comes to you for a second opinion. Her radiograph is shown in Figure A. Which of the following best describes your responsibility in disclosing to the patient that the pain may be from a medical error?
1) You do not need to disclose this information
2) You legally must disclose this information to the patient
3) You legally must disclose this information to the original hospital's peer review panel
4) You ethically must disclose this information to the patient
5) You ethically must disclose this information to the original surgeon
As a practicing orthopaedic surgeon, you ethically are required to disclose the potential impact of medical errors on patient outcome.
The orthopaedic surgeon is bound ethically but not legally to give his or her best medical opinion, regardless of whether the orthopaedist is the treating physician or the physician who is asked to render a second or additional medical opinion. The best interest of the patient should clearly remain the guiding principal. It is illegal to slander the original physician if the slanderous
information is known or can be proven to be false.
Bhattacharyya et al. review the importance of documentation and ethical treatment of patients when providing second opinions. They note that it is unethical for the consulting orthopaedic surgeon to solicit care of the patient. However, at the sole discretion of the patient, the patient ethically may choose to terminate his or her relationship with his or her treating physician and then enter into another treatment relationship with the consulting
orthopaedic surgeon.
Figure A shows a left hip hemiarthroplasty with the distal component perforated through the medial proximal femur.
Incorrect Answers:
1) This information must be disclosed per ethical recommendations. 2 and 3) There is no legal requirement to disclose this information.
5) There is no documented ethical requirement to disclose this to the original surgeon.
A patient is consented for a right wrist open reduction and internal fixation. After the patient is prepped and draped, a skin incision is made. It is recognized intra-operatively, however, that a skin incision was made on the incorrect side (left). Subsequent right wrist open reduction and internal fixation goes uneventfully. What is the next best course of action?
1) do not tell the patient or family
2) contact the Risk Management department
3) immediately discuss the situation with the patient and family
4) alter the medical record
5) only discuss the situation with the patient if he or she brings it up.
Patients should be approached after a medical error and all errors must be promptly and completely disclosed. The physician should take the lead in the disclosure and not wait for the patient to ask. Risk management should be called as well, but the patient and family should be informed first. It is never appropriate to alter the medical record.
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior
**to her rectal surgery?**
1) C-reactive protein (CRP)
2) Synovial fluid analysis of affected joints
3) Blood cultures
4) Cervical radiographs
5) Bethesda assay
This patient has a diagnosis of Juvenile Idiopathic Arthritis (JIA). Flexion- extension c-spine radiographs should be ordered to rule out atlantoaxial instability prior to surgery.
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Answer 1: Both ESR and CRP are usually elevated in this condition and provide no further benefit for the operative management of this patient.
Answer 2: This patient has chronic joint swelling and pain. Joint aspirates and synovial fluid analysis would not be required.
Answer 3: There is no suspicion for an acute infection. Therefore, blood cultures are not required.
Answer 5: A Bethesda assay is used to measure the amount of factor VIII or IX antibody in the blood, for patients with hemophilia.
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
1) Increased proliferation of osteoblasts
2) Decreased osteoclast differentiation
3) Increase release of TGF-beta1
4) Increased expression of BMP2
5) Increased expression of BMP7
Induction coupling stimulates bone growth by increasing expression of BMP7, BMP2, TGF-beta1, and by increasing osteoblasts proliferation. Induction coupling has not been shown to have the effect of decreasing osteoclast differentiation.
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Answers 1,3-5: All are true effects of electrical stimulation on bone.
Two patients are discharged from a surgicenter after upper extremity procedures. The surgeon gives them prescriptions for oral opioid analgesics. Patient A had open reduction and internal fixation of a distal radius fracture. Patient B had cubital tunnel release without transposition. Which of the following is most likely true regarding analgesic use?
1) Patient A will use more medication than Patient B
2) Patient A will use less medication than Patient B
3) Analgesic use will be similar between Patients A and B
4) Both patients will consume more than 30 pills
5) A reasonable prescription is 40 pills with 1 refill for Patient A, and 40 pills with no refills for Patient B
A patient that has had ORIF will require MORE oral analgesia than a patient who has had a cubital tunnel release.
Patients undergoing bony procedures (e.g. ORIF and arthroplasty) require more analgesia than patients undergoing soft tissue procedures (e.g. carpal/cubital tunnel release, trigger finger release, elbow or shoulder arthroscopy). Overprescribing of opioid analgesia is a common problem. Many opioids are unused in the postoperative period by the patients for whom they were prescribed.
Rodgers et al. reviewed opioid use (oxycodone, hydrocodone, propoxyphene) after outpatient upper extremity surgery. Patients undergoing bony procedures used the most analgesia (14 pills) while those undergoing soft tissue
procedures used the least (9 pills). Half took medication for =
What property of titanium alloys accounts for their high corrosion resistance in vivo?
1) Self-passivation
2) Ductility
3) Hardness
4) Modulus of elasticity
5) Conductivity
In both room temperature air and physiologic fluids, titanium alloys self- passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown.
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
1) Fat only
2) Fat and air
3) Fat and marrow
4) Fat and cement
5) Fat and bone
Emboli are created during TKA. Usually there is an increased incidence with
the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli
to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury.
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
1) Industry-paid travel, hotel (for the surgeon and spouse), and registration at a university- sponsored CME course
2) Industry-paid travel and hotel for a faculty member at an industry- sponsored meeting that is not CME approved
3) Consultation agreement ($50,000/annum) between the surgeon and the company for evaluation of the implant system with required oral reporting of impressions
4) A restricted grant from a company to an orthopaedic residency program with the stipulation that the third year residents be sent to an industry- sponsored course
5) Industry-paid dinner at a premium restaurant ($200/person) for surgeon and office staff at which a new set of surgical instrumentation is presented
It is appropriate for orthopaedic surgeons to have relationships with industry as long as the relationship is for the good of the patient and no “quid pro quo” intent exists. A grant to cover registration at a CME event is appropriate but travel and hotel for a spouse is not.
For orthopaedists who are faculty at a meeting sponsored by industry, it is appropriate for travel and expenses to be covered for that faculty member. Care must be exercised that the faculty member contributes in an amount appropriate for the expenses paid. The faculty member must ensure that information presented is unbiased and based on reasonable data and opinion. Consulting agreements should spell out specifically the duties of the agreement and payment should be appropriate for the time spent. There should be a defined work product for the consulting. Agreements that are thinly veiled payments for use of a company’s products must be avoided. In all cases, the agreements must stand up to public
scrutiny. Restricted grants for specific industry-sponsored programs aimed at residents are not appropriate. Unrestricted grants intended for attendance at approved CME courses are appropriate. Dinners at which information is presented about topics that can aid in patient care are appropriate as long as the expense is reasonable ($100 or less/person) and the guest list includes individuals who can use the information in a patient case. Clearly a “premium” dinner for office staff to review new surgical instrumentation would not pass this test.
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
1) IV
2) V
3) VI
4) VII
5) VIII
Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase.
This inhibition results in lack of carboxylation of vitamin
K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors.
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
1) It is a disease caused by an abnormality of platelets that leads to increased blood clotting.
2) It is a disease caused by an abnormality of vascular endothelium that leads to increased blood clotting.
3) It is a disease caused by an abnormality of hepatic metabolism that leads to decreased production of factor V and decreased blood clotting.
4) It is a disease caused by an abnormality of factor V that leads to decreased inactivation of factor Va by activated protein C (aPC) and increased blood clotting.
5) It is a familial, genetic disease that requires placement of a Greenfield filter in all
individuals who have the abnormality, prior to surgery.
Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.
Which of the following terms best describes the probability of finding a significant association in a research study when one truly exists?
1) Type-1 (alpha) error
2) Type-2 (beta) error
3) Power
4) Alpha level
5) Relative Risk
**
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists.
The
Etanercept is a biochemically designed tumor necrosis factor receptor immunoglobulin G fusion protein, which binds to TNF-alpha and is thus a TNF- alpha antagonist.
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its
receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and
malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-9.1) and for serious infection was
2.0 (95% CI, 1.3-3.1) with use of TNF-alpha antagonist.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Incorrect Answers:
: Rituximab is a monoclonal antibody to CD20 antigen (inhibits B cells). It is often used with good clinical outcomes as monotherapy in patients who are intolerant of methotrexate or have contraindications to methotrexate or other DMARDs.
Answer 3: Abatacept is a selective costimulation modulator that binds to CD80 and CD86 (inhibits T cells). It is often prescribed for treatment of moderate to severe rheumatoid arthritis, or after failure of a disease-modifying anti- rheumatic agent (DMARD), like methotrexate but it can be used as first-line therapy.
Answer 4: Methotrexate is a folic acid analogue. It binds dihydrofolate reductase and prevents synthesis of tetrahydrofolate. It is usually a first line treatment for moderate to severe rheumatoid arthritis.
Answer 5: Leflunomide is an inhibitor of pyrimidine synthesis. It is approved to treat adult moderate to severe rheumatoid arthritis, usually as a monotherapy or failure of other DMARDs.
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
1) As strain rate increases, both elastic modulus and ultimate strength increase
2) As strain rate increases, elastic modulus remains unchanged but ultimate strength increases
3) As strain rate increases, elastic modulus increases but ultimate strength decreases
4) As strain rate increases, both elastic modulus and ultimate strength decrease
5) As strain rate increases, elastic modulus increases but ultimate strength remains unchanged
As strain rate increases, both elastic modulus and ultimate strength increase. For LOW strain rates typical of normal activity (physiological strain rates of
0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress- strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone.
Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Illustration B shows that the ultimate strength and elastic modulus increase with rapid loading or deformation. The ultimate strength increases by roughly a factor of 3, while the elastic modulus increases by a factor of
approximately 2 over the strain rate range.
Incorrect Answers:
Answers 2, 3, 4, 5: As strain rate increases, elastic modulus and ultimate strength increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
In regards to a genetic disorder, which of the following is an example of "anticipation?"
1) Gene characteristics more severe and earlier in onset in subsequent generations
2) A disorder inherited from a genetic mutation specific to maternal DNA
3) Gene characteristics expressed to varying degrees in different individuals
4) Variation in the relative frequency of a genotype due to chance
5) The presence of an extra copy of a chromosome
Genetic anticipation is a phenomenon in which a genetic disorder becomes progressively more severe and earlier in onset with each generation. Examples of disorders exhibiting anticipation include Huntington's disease and myotonic dystrophy.
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Answer 2: "Genomic imprinting" is when a disorder is linked to a parent- specific origin. An example of maternal genomic imprinting is Angelman Syndrome. An example of paternal genomic imprinting is Prader Willi.
Answer 3: "Variable penetrance" is when gene characteristics are expressed in varying degrees.
Answer 4: "Genetic drift" is the chance variation in the relative frequency of a genotype within a population.
Answer 5: "Trisomy" is the presence of an extra copy of a chromosome. Down Syndrome is trisomy 21, which is due to an extra copy of chromosome 21.
A researcher is working on Medication A, a drug FDA-approved for the treatment of osteoporosis in men and women. It is an anti- resorptive agent that inhibits the formation, function and survival of osteoclasts. It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non- detectable. It can be used in the presence of cancer metastases to bone. What is Medication A?
1) Denosumab
2) Alendronate
3) Abaloparatide
4) Teriparatide
5) Strontium ranelate
Denosumab is FDA-approved for the treatment of osteoporosis in men and women. It inhibits the formation, function and survival of osteoclasts (OC). It does not bind to calcium hydroxyapatite. At 1-year after the initial dose, tissue levels are non-detectable.
Denosumab is a human monoclonal antibody against RANKL. By binding RANKL, it prevents interaction of RANKL with RANK (on OC and osteoclast precursors, OCP), and inhibits OC-mediated bone resorption, and the formation, function and survival of OC. In contrast, bisphosphonates bind to calcium hydroxyapatite in bone, and decrease resorption by decreasing function and survival (but not formation) of OC.
Vaananen et al. reviewed the cell biology of OC. During bone resorption, 3 membrane domains appear: ruffled border, sealing zone and functional secretory domain. The resorption cycle starts with migration, bone attachment, polarization (formation of membrane domains), dissolution of hydroxyapatite, degradation of organic matrix, removal of degradation
products from resorption lacuna, and apoptosis of the OC or return to the non- resorbing stage.
Boyce et al. reviewed the regulation of osteoclasts and their functions. OCPs are held in bone marrow by chemokines e.g. stroma-derived factor-1 (SDF1) and attracted to blood by sphingosine-1 phosphate (S1P) (increased in synovial fluid of patients with RA). All aspects of osteoclast formation and functions are regulated by M-CSF and RANKL. More recent studies indicate that osteoclasts and their precursors regulate immune
responses and
osteoblast formation and functions by means of direct cell-cell contact through ligands and receptors, such as ephrins and Ephs, and semaphorins and
plexins, and through expression of clastokines.
Warriner and Saag reviewed the diagnosis and treatment of osteoporosis. They defined osteoporosis as T-score of = -2.5 or a history of fragility fracture. Incident hip and vertebral fractures increase future risk of these fractures (hazard ratio 7.3 and 3.5, respectively).
Cummings et al. compared subcutaneous denosumab (60mg every 6mths) vs placebo in prevention of fractures in 7868 osteoporotic (T-score -2.5 to -4.0) postmenopausal women. They found that denosumab reduced risk of vertebral fracture by 68% (risk ratio, 0.32), hip fracture by 40% (hazard ratio 0.6), nonvertebral fracture by 20% (hazard ratio 0.8). There was no increased risk of cancer, infection, delayed fracture healing, cardiovascular disease, osteonecrosis of the jaw or adverse reactions. They concluded that it was useful for reduction of fractures in osteoporotic women.
The video shows the action of denosumab (prolia). Illustration A shows the different osteoclast zones.
Incorrect Answers:
Answers 2: Alendronate (and other bisphosphnates) inhibit resorption of bone, decrease function and survival of osteoclasts. Because of binding to calcium hydroxyapatite, they are detectable years after dosing. They reduce function and survival of OC, but do not affect the formation of osteoclasts.
Answer 3: Abaloparatide is a PTH analog that has completed phase III trials for osteoporosis. As of mid-2016, it is not yet approved for treatment of osteoporosis. Answer 4: Teriparatide (recombinant PTH 1-34) is the only anabolic (not antiresorptive) agent approved for osteoporosis treatment. It is administered by daily subcutaneous injection. Osteosarcoma, cancer metastases to bone and Paget's disease are contraindications.
Answer 5: Strontium ranelate (marketed as Protelos or Protos) both increases deposition of new bone by osteoblasts and reduces the resorption of bone by osteoclasts ("dual action bone agent", DABA). It is not FDA approved for use in the United States. Increased risk of myocardial infarction has been detected.
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
1) Patient Protection and Affordable Care Act
2) Medicare Payment Reform Act
3) Physician Financial Transparency Act
4) Physician Payments Sunshine Act
5) Health Insurance Portability and Accountability Act
The Physician Payments Sunshine Act requires all payments by corporations to physicians beyond $10 per year to be reported to the Centers for Medicare and Medicaid Services.
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Answers 1: The Patient Protection and Affordable Care Act (PPACA), known also by its shorter name of the Affordable Care Act (ACA) or it's nickname
"Obamacare", was passed in March 2010. The Sunshine Act was one of many provisions passed within the PPACA (after the Sunshine Act failed to pass on its own in prior years), but the PPACA focused primarily on improving the quality and affordability of healthcare insurance and lowering the costs of healthcare.
Answer 2: The Medicare Payment Reform Act of 1983 was a quickly drafted revision to the way Medicare payments were made, changing from fee-for- service to prospective payments allowing Medicare to determine payment amount rather than providers/hospitals.
Answer 3: This is a fictitious act.
Answer 5: HIPPA is the 1996 legislation defining standards and protections for patient private health information and electronic exchange of records.
Which of the following materials best approximates the Young's modulus of elasticity of cortical bone?
1) Titanium
2) Cobalt-chrome alloy
3) Alumina
4) Zirconia
5) Stainless steel
Of the materials listed titanium (100GPa) has an elastic modulus closest to cortical bone (approximately 18GPa) as well as cancellous bone (approximately 2GPa).
Titanium is a material that is light, highly ductile, strong and corrosion resistant. However, titanium has poor wear resistance and is notch sensitive. It is commonly used as an orthopaedic implant materials because it has torsional and axial stiffness (moduli) that most closely mimics bone. Young’s modulus is constant and different for each material and represents the material's ability to maintain shape under external loading.
Rho et al found that the average Young's modulus for trabecular bone measured ultrasonically and mechanically was 14.8 GPa (S.D. 1.4) and 10.4 (S.D. 3.5), respectively. The average Young's modulus of microspecimens of cortical bone measured ultrasonically and mechanically was 20.7 GPa (S.D.
1.9) and 18.6 GPa (S.D. 3.5), respectively.
Illustration A depicts a stress vs. strain curve. The slope of the line in the elastic zone represents the Young Modulus of Elasticity.
Incorrect Answers:
Answer 2: Cobalt-chrome alloy is approximately 240 GPa Answer 3: Alumina is approximately 340 GPa
Answer 4: Zirconia (Ceramic) = 248 GPa
Answer 5: Stainless steel is approximately 240 GPa
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
1) VDDR I is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
2) VDDR I is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3. VDDR II is a deficiency of an enzyme predominantly found in the kidney.
3) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
4) VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an activating mutation of the receptor for 1,25 (OH)2 vitamin D3.
5) VDDR I is a deficiency of an enzyme predominantly found in the liver. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of an enzyme predominantly found in the kidney. VDDR II is caused by an inactivating mutation of the receptor for 1,25 (OH)2 vitamin D3.
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to
1a,25(OH)2D3]. Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
Answers 1, 2, 4, 5: VDDR I is a deficiency of 1a-hydroxylase (predominantly
found in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
A 73-year-old female sustains a left hip fracture that is treated with hemiarthroplasty. She has continued pain two months after surgery, and comes to you for a second opinion. Her radiograph is shown in Figure A. Which of the following best describes your responsibility in disclosing to the patient that the pain may be from a medical error?
1) You do not need to disclose this information
2) You legally must disclose this information to the patient
3) You legally must disclose this information to the original hospital's peer review panel
4) You ethically must disclose this information to the patient
5) You ethically must disclose this information to the original surgeon
As a practicing orthopaedic surgeon, you ethically are required to disclose the potential impact of medical errors on patient outcome.
The orthopaedic surgeon is bound ethically but not legally to give his or her best medical opinion, regardless of whether the orthopaedist is the treating physician or the physician who is asked to render a second or additional medical opinion. The best interest of the patient should clearly remain the guiding principal. It is illegal to slander the original physician if the slanderous
information is known or can be proven to be false.
Bhattacharyya et al. review the importance of documentation and ethical treatment of patients when providing second opinions. They note that it is unethical for the consulting orthopaedic surgeon to solicit care of the patient. However, at the sole discretion of the patient, the patient ethically may choose to terminate his or her relationship with his or her treating physician and then enter into another treatment relationship with the consulting
orthopaedic surgeon.
Figure A shows a left hip hemiarthroplasty with the distal component perforated through the medial proximal femur.
Incorrect Answers:
1) This information must be disclosed per ethical recommendations. 2 and 3) There is no legal requirement to disclose this information.
5) There is no documented ethical requirement to disclose this to the original surgeon.
A patient is consented for a right wrist open reduction and internal fixation. After the patient is prepped and draped, a skin incision is made. It is recognized intra-operatively, however, that a skin incision was made on the incorrect side (left). Subsequent right wrist open reduction and internal fixation goes uneventfully. What is the next best course of action?
1) do not tell the patient or family
2) contact the Risk Management department
3) immediately discuss the situation with the patient and family
4) alter the medical record
5) only discuss the situation with the patient if he or she brings it up.
Patients should be approached after a medical error and all errors must be promptly and completely disclosed. The physician should take the lead in the disclosure and not wait for the patient to ask. Risk management should be called as well, but the patient and family should be informed first. It is never appropriate to alter the medical record.
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior
**to her rectal surgery?**
1) C-reactive protein (CRP)
2) Synovial fluid analysis of affected joints
3) Blood cultures
4) Cervical radiographs
5) Bethesda assay
This patient has a diagnosis of Juvenile Idiopathic Arthritis (JIA). Flexion- extension c-spine radiographs should be ordered to rule out atlantoaxial instability prior to surgery.
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Answer 1: Both ESR and CRP are usually elevated in this condition and provide no further benefit for the operative management of this patient.
Answer 2: This patient has chronic joint swelling and pain. Joint aspirates and synovial fluid analysis would not be required.
Answer 3: There is no suspicion for an acute infection. Therefore, blood cultures are not required.
Answer 5: A Bethesda assay is used to measure the amount of factor VIII or IX antibody in the blood, for patients with hemophilia.
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
1) Increased proliferation of osteoblasts
2) Decreased osteoclast differentiation
3) Increase release of TGF-beta1
4) Increased expression of BMP2
5) Increased expression of BMP7
Induction coupling stimulates bone growth by increasing expression of BMP7, BMP2, TGF-beta1, and by increasing osteoblasts proliferation. Induction coupling has not been shown to have the effect of decreasing osteoclast differentiation.
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Answers 1,3-5: All are true effects of electrical stimulation on bone.
Two patients are discharged from a surgicenter after upper extremity procedures. The surgeon gives them prescriptions for oral opioid analgesics. Patient A had open reduction and internal fixation of a distal radius fracture. Patient B had cubital tunnel release without transposition. Which of the following is most likely true regarding analgesic use?
1) Patient A will use more medication than Patient B
2) Patient A will use less medication than Patient B
3) Analgesic use will be similar between Patients A and B
4) Both patients will consume more than 30 pills
5) A reasonable prescription is 40 pills with 1 refill for Patient A, and 40 pills with no refills for Patient B
A patient that has had ORIF will require MORE oral analgesia than a patient who has had a cubital tunnel release.
Patients undergoing bony procedures (e.g. ORIF and arthroplasty) require more analgesia than patients undergoing soft tissue procedures (e.g. carpal/cubital tunnel release, trigger finger release, elbow or shoulder arthroscopy). Overprescribing of opioid analgesia is a common problem. Many opioids are unused in the postoperative period by the patients for whom they were prescribed.
Rodgers et al. reviewed opioid use (oxycodone, hydrocodone, propoxyphene) after outpatient upper extremity surgery. Patients undergoing bony procedures used the most analgesia (14 pills) while those undergoing soft tissue
procedures used the least (9 pills). Half took medication for =
What property of titanium alloys accounts for their high corrosion resistance in vivo?
1) Self-passivation
2) Ductility
3) Hardness
4) Modulus of elasticity
5) Conductivity
In both room temperature air and physiologic fluids, titanium alloys self- passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown.
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
1) Fat only
2) Fat and air
3) Fat and marrow
4) Fat and cement
5) Fat and bone
Emboli are created during TKA. Usually there is an increased incidence with
the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli
to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury.
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
1) Industry-paid travel, hotel (for the surgeon and spouse), and registration at a university- sponsored CME course
2) Industry-paid travel and hotel for a faculty member at an industry- sponsored meeting that is not CME approved
3) Consultation agreement ($50,000/annum) between the surgeon and the company for evaluation of the implant system with required oral reporting of impressions
4) A restricted grant from a company to an orthopaedic residency program with the stipulation that the third year residents be sent to an industry- sponsored course
5) Industry-paid dinner at a premium restaurant ($200/person) for surgeon and office staff at which a new set of surgical instrumentation is presented
It is appropriate for orthopaedic surgeons to have relationships with industry as long as the relationship is for the good of the patient and no “quid pro quo” intent exists. A grant to cover registration at a CME event is appropriate but travel and hotel for a spouse is not.
For orthopaedists who are faculty at a meeting sponsored by industry, it is appropriate for travel and expenses to be covered for that faculty member. Care must be exercised that the faculty member contributes in an amount appropriate for the expenses paid. The faculty member must ensure that information presented is unbiased and based on reasonable data and opinion. Consulting agreements should spell out specifically the duties of the agreement and payment should be appropriate for the time spent. There should be a defined work product for the consulting. Agreements that are thinly veiled payments for use of a company’s products must be avoided. In all cases, the agreements must stand up to public
scrutiny. Restricted grants for specific industry-sponsored programs aimed at residents are not appropriate. Unrestricted grants intended for attendance at approved CME courses are appropriate. Dinners at which information is presented about topics that can aid in patient care are appropriate as long as the expense is reasonable ($100 or less/person) and the guest list includes individuals who can use the information in a patient case. Clearly a “premium” dinner for office staff to review new surgical instrumentation would not pass this test.
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
1) IV
2) V
3) VI
4) VII
5) VIII
Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase.
This inhibition results in lack of carboxylation of vitamin
K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors.
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
1) It is a disease caused by an abnormality of platelets that leads to increased blood clotting.
2) It is a disease caused by an abnormality of vascular endothelium that leads to increased blood clotting.
3) It is a disease caused by an abnormality of hepatic metabolism that leads to decreased production of factor V and decreased blood clotting.
4) It is a disease caused by an abnormality of factor V that leads to decreased inactivation of factor Va by activated protein C (aPC) and increased blood clotting.
5) It is a familial, genetic disease that requires placement of a Greenfield filter in all
individuals who have the abnormality, prior to surgery.
Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.
Which of the following terms best describes the probability of finding a significant association in a research study when one truly exists?
1) Type-1 (alpha) error
2) Type-2 (beta) error
3) Power
4) Alpha level
5) Relative Risk
**
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists.
The
Scientific References
- by Kocher and Wojtys are excellent reviews of basic biostatistic principles. Incorrect Answers:
Answer 1: The power is defined by 1 - probability of type-II (beta) error, and is often set at 80%. For example, a power of 80% means that if the
intervention works, the study has an 80% chance of detecting this and a 20% chance of randomly missing it.
Answer 2: A type-II or beta error occurs when one falsely concludes that there is no significant association when there actually is an association (resulting in
a false-negative study that rejects a true alternative hypothesis). The type-II or beta error can be determined if Type I error rate and sample size are known. A type-I or alpha error occurs when a significant association is found when there is no true association (resulting in a false-positive study that rejects a true null hypothesis).
Answer 4:The alpha level refers to the probability of a type-I (alpha) error and is usually set for most studies at 0.05.
Answer 5:The relative risk is a term used in prospective cohorts studies and is the risk of developing disease for people with known exposure compared to risk of developing disease without exposure.
Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
1) Keratin sulfate
2) Collagen type II
3) Water
4) Protein
5) Chondroitin sulfate
The extracellular matrix consists of water, proteoglycans, and collagen. Water makes up the majority (approximately 65% to 80%) of wet weight; 95% of the collage is type II with much smaller amounts of other collagens, including types IV, VI, IX, X, and XI. The exact functions of these other collagens are unknown, but they are believed to be important in matrix attachment and stabilization of the diameter of collagen fibrils.
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist’s office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?
1) No additional consent needed
2) Verbal approval
3) Written approval
4) Written approval with notarization
5) Telephone consent witnessed by a nurse
The privacy rules do not require an individual’s written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry’s most fundamental activities such as providing care.
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?
1) Cervical spine assessment
2) Temporomandibular joint (TMJ)/jaw assessment
3) Dental assessment
4) Stress dosing with corticosteroids
5) Opthalmology examination
**
The cervical spine may be involved in a child with polyarticular or systemic JRA; fusion or instability can occur. Radiographic assessment of the cervical spine should include lateral flexion-extension views. The potential exists for spinal cord injury during intubation or positioning in t
he presence of an unstable cervical spine. Limitations of the TMJ and micrognathia may affect ease of intubation and administration of anesthesia via a mask. If the TMJ and jaw are involved, some patients may have dental findings such as dental caries and even abscesses which can affect surgery. Some children, particularly those with systemic arthritis, may be taking corticosteroids long- term and may need stress dosing with complex surgeries. Although it is important to routinely check for uveitis and iritis in children with JRA, this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 41High Yield
Which of the following is not a factor in the setting time of cement:
Explanation
Storage temperature, ambient temperature, handling and kneading of bone cement, and introducing cement in a warm environment are factors of the setting time of cement. Use of a cement gun is not a factor
Question 42High Yield
Which of the following are characteristic of osteoarthritis:
Explanation
The characteristic findings in osteoarthritis are:
Asymmetric loss of the joint space Subchondral sclerosis and cysts Osteophyte formation
As the cartilage degenerates, progressive bone remodeling occurs. The other responses refer to other synovial proliferative disorders:
Pigmented villonodular synovitis: Synovial proliferation, cysts/erosions on both sides of the joint
Rheumatoid arthritis: Synovial proliferation with lymphocytic infiltration, periarticular osteopenia, symmetric joint space loss
C harcot neuropathy: Subluxation, bone fragmentation, dissolution of the articular surfaces
Gout: Periarticular erosions, soft tissue masses, preservation of the articular surfaces
Asymmetric loss of the joint space Subchondral sclerosis and cysts Osteophyte formation
As the cartilage degenerates, progressive bone remodeling occurs. The other responses refer to other synovial proliferative disorders:
Pigmented villonodular synovitis: Synovial proliferation, cysts/erosions on both sides of the joint
Rheumatoid arthritis: Synovial proliferation with lymphocytic infiltration, periarticular osteopenia, symmetric joint space loss
C harcot neuropathy: Subluxation, bone fragmentation, dissolution of the articular surfaces
Gout: Periarticular erosions, soft tissue masses, preservation of the articular surfaces
Question 43High Yield
Which of the following statements best describes labral tears in the hip?
Explanation
DISCUSSION: Labral and chondral lesions are observed within the anterosuperior quadrant of the acetabulum. Tearing of the labrum markedly reduces resistance to joint motion, leading to instability.
The most common associated lesions are chondral injuries. They can occur with or without abnormal bone morphology. The etiology for labral tears can be from traumatic and degenerative causes, structural abnormalities from femoroacetabular impingement, developmental abnormalities, and hip instability.
REFERENCES: Beck M, Kalhor M, Leunig M, et al: Hip morphology influences the pattern of damage to the acetabular cartilage: Femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005;87:1012-1018.
Ito K, Leunig M, Ganz R: Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res 2004;429:262-271.
Crawford MJ, Dy CJ, Alexander JW, et al: The 2007 Frank Stinchfield Award. The biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res 2007;465:16-22.
DISCUSSION: Labral and chondral lesions are observed within the anterosuperior quadrant of the acetabulum. Tearing of the labrum markedly reduces resistance to joint motion, leading to instability.
The most common associated lesions are chondral injuries. They can occur with or without abnormal bone morphology. The etiology for labral tears can be from traumatic and degenerative causes, structural abnormalities from femoroacetabular impingement, developmental abnormalities, and hip instability.
REFERENCES: Beck M, Kalhor M, Leunig M, et al: Hip morphology influences the pattern of damage to the acetabular cartilage: Femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005;87:1012-1018.
Ito K, Leunig M, Ganz R: Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res 2004;429:262-271.
Crawford MJ, Dy CJ, Alexander JW, et al: The 2007 Frank Stinchfield Award. The biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res 2007;465:16-22.
Question 44High Yield
..A 54-year-old pipefitter falls from a ladder at work and dislocates his nondominant shoulder. His MRI scan shows supraspinatus and infraspinatus tears with retraction to the glenoid. He cannot actively raise his arm away from his side. He denies prior shoulder symptoms before his fall. Three weeks of physical therapy have failed to improve his function. You and the patient decide to proceed with surgical repair. Which is a risk factor for a poor outcome?
Explanation
- Work-related injury
RESPONSES FOR QUESTIONS 64 THROUGH 68
RESPONSES FOR QUESTIONS 64 THROUGH 68
Question 45High Yield
1240) Which of the following factors is associated with the highest rate of nonunion of a midshaft clavicle fracture?

Explanation
The risk of nonunion in patients sustaining middle 1/3 clavicle fractures is increased in female patients.
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Question 46High Yield
What muscles are responsible for the most common deformity after antegrade intramedullary nailing for a subtrochanteric femur fracture?
Explanation
The most common deformity after antegrade nailing of a subtrochanteric femur fracture is varus and procurvatum (or flexion). This is caused by the hip abductors and iliopsoas pulling the proximal fragment into abduction and flexion, while the distal fragment is pulled into adduction from the adductors.
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
Question 47High Yield
A 45-year-old coach sustains a complete distal biceps tendon rupture at the elbow. Surgical repair is most indicated to
Explanation
DISCUSSION: The biceps is primarily responsible for supination of the forearm. The brachialis muscle is primarily repsonsible for elbow flexion strength. Failure to repair the distal biceps tendon will result in loss of 40% supination strength and 10% loss in flexion strength. Therefore, surgical repair of a complete distal biceps tendon rupture is most indicated to maximize supination strength. Improved cosmesis should not be the primary indication for surgical repair. Degenerative changes of the elbow have no bearing on whether the distal biceps is repaired or not. Loss of terminal extension is common in distal biceps tendon repairs.
REFERENCES: Altcheck DW, Altcheck AJ: The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, p 288.
Morrey BF, Askew LJ, An KN, et al: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418^4-21.
REFERENCES: Altcheck DW, Altcheck AJ: The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, p 288.
Morrey BF, Askew LJ, An KN, et al: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418^4-21.
Question 48High Yield
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Explanation
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. 20
Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis
.
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
A. directly posterior to the posterior cruciate ligament (PCL).
B. posteromedial to the PCL.
C. posterolateral to the PCL.
D. in the posteromedial corner of the knee.
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Correct answer : C
A 70-year-old woman has severe stiffness of her knee following a primary total knee arthroplasty (TKA) 3 years ago. The patient has well-fixed femoral and tibial components, and a preoperative work-up for infection is negative. The decision is made to proceed with a revision TKA of both the femoral and tibial components. An extensile exposure is planned to facilitate removal of the components. What extensile exposure would require the least modification of postoperative rehabilitation with regards to weight bearing and range of motion?
A. Quadriceps snip
B. Lateral parapatellar approach
C. V-Y quadriceps turndown
D. Tibial tubercle osteotomy
Achievement of adequate exposure in revision TKA is critical as it reduces the surgical time, enhances the ability for both component removal and reconstruction, and avoids devastating complications such as extensor mechanism disruption. Numerous extensile exposures in revision TKA have been described.
21
A tibial tubercle osteotomy, V-Y tendon plasty, and V-Y quadriceps turndown all provide excellent exposure, but require a modification in postoperative rehabilitation as they often require a period of immobilization followed by limits in range of motion. In contrast, the quadriceps snip allows immediate weight bearing along with progressive range of motion; no modification of postoperative rehabilitation is required. Lateral parapatellar approach would offer no benefit for exposure.
Correct answer : A
Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis
.
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
A. directly posterior to the posterior cruciate ligament (PCL).
B. posteromedial to the PCL.
C. posterolateral to the PCL.
D. in the posteromedial corner of the knee.
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Correct answer : C
A 70-year-old woman has severe stiffness of her knee following a primary total knee arthroplasty (TKA) 3 years ago. The patient has well-fixed femoral and tibial components, and a preoperative work-up for infection is negative. The decision is made to proceed with a revision TKA of both the femoral and tibial components. An extensile exposure is planned to facilitate removal of the components. What extensile exposure would require the least modification of postoperative rehabilitation with regards to weight bearing and range of motion?
A. Quadriceps snip
B. Lateral parapatellar approach
C. V-Y quadriceps turndown
D. Tibial tubercle osteotomy
Achievement of adequate exposure in revision TKA is critical as it reduces the surgical time, enhances the ability for both component removal and reconstruction, and avoids devastating complications such as extensor mechanism disruption. Numerous extensile exposures in revision TKA have been described.
21
A tibial tubercle osteotomy, V-Y tendon plasty, and V-Y quadriceps turndown all provide excellent exposure, but require a modification in postoperative rehabilitation as they often require a period of immobilization followed by limits in range of motion. In contrast, the quadriceps snip allows immediate weight bearing along with progressive range of motion; no modification of postoperative rehabilitation is required. Lateral parapatellar approach would offer no benefit for exposure.
Correct answer : A
Question 49High Yield
The best clinical outcome following a primarily ligamentous Lisfranc injury is with:
Explanation
Forty-one patients were prospectively randomized into traditional open reduction internal fixation (ORIF) versus primary arthrodesis. The American Orthopaedic Foot & Ankle Society scores at 2-year follow-up were significantly better in the fusion group versus the ORIF group. Of the patients in the ORIF group, 25% later developed arthritis and were converted to fusions.
Question 50High Yield
An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacromial injection. The groups have similar baseline demographics and shoulder pathologies. Ten patients are randomized in each group and findings show that there is no significant difference in any patient-reported outcome measure. An increase in sample size would reduce the risk of what parameter?
Explanation
This study represents a randomized clinical trial with two groups. However, the sample size is small, increasing the risk for type II error, or false-negative findings. Increasing the number of patients in each group would lead to increased power, thereby reducing the risk of a type II error. A type I error is the rejection of a true null hypothesis (false-positive). A randomized trial reduces the risk of selection bias as patients are assigned to groups in a random fashion. Recall bias occurs when participants do not accurately remember previous events or experiences from the past.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon