Orthopedic Basic Science MCQs: Comprehensive Study & Exam Prep
14 Apr 2026
53 min read
63 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Basic Science MCQs: Comprehensive ...
00:00
Start Quiz
Question 1High Yield
In the pediatric population, CECS most commonly presents in females involved in running sports. In this cohort, recurrence occurs at a rate of 18%. Wound complications are the next most common at a rate of 11.2%.
A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
Explanation
The hockey player is suffering from commotio cordis, in which a cardiac arrhythmia occurs after a sudden blunt impact to the chest. Treatment of commotio cordis is defibrillation. As the time to defibrillation increases, the likelihood of survival decreases. In animal models, chest protectors have not shown efficacy
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
Question 2High Yield
The most appropriate treatment of this lesion involves
Explanation
- radiofrequency ablation (RFA)._
Question 3High Yield
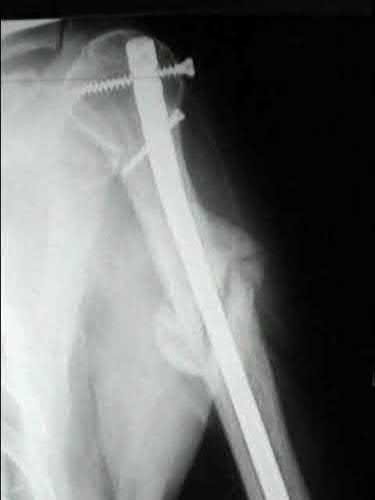
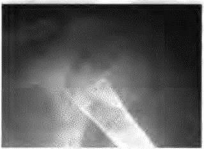
1246) A 42-year-old man reports persistent arm pain after undergoing intramedullary nailing of a humeral shaft fracture 13 months ago.
Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
A. What is the next most appropriate step in treatment?
Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
A. What is the next most appropriate step in treatment?
Explanation
Plate fixation (with bone graft as needed) is the procedure of choice for humeral shaft nonunions.
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
Question 4High Yield
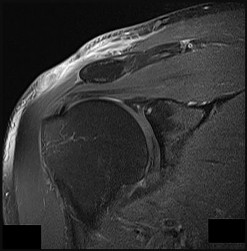
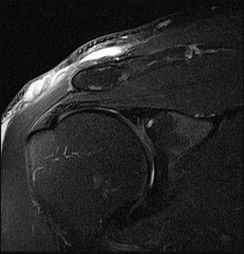
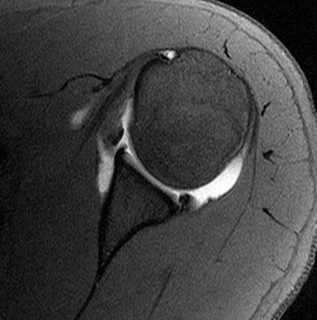
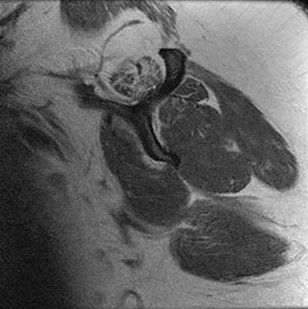
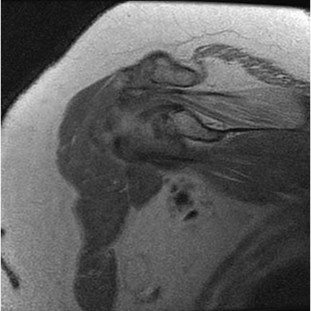
A 44-year-old recreational weight lifter reports chronic deep pain in his left shoulder that is aggravated by any pressing exercises. He also notes a painful catch in the shoulder occurring with rotational movements. Physical therapy and nonsteroidal anti-inflammatory drugs for 3 months have failed to provide relief. Examination reveals pain with O’Brien’s test but no signs of instability. MRI scans are shown in Figures 4a
and 4b. Treatment should now consist of
and 4b. Treatment should now consist of
Explanation
The MRI scans show a large paralabral ganglion cyst in the spinoglenoid notch that communicates with an extensive tear of the glenoid labrum. Snyder and associates have classified superior labral tears into several subtypes that reflect the location and extent of the injury. Arthroscopic repair of the labral tear and aspiration of the ganglion cyst is the treatment of choice. Open excision of the cyst does not address the underlying problem of the labral tear.
REFERENCE: Snyder SJ, Karzel RP, Delpizzo W: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch cysts. J Shoulder Elbow Surg 2002;11:600-604.
McFarland EG, Kim TK, Savino RM: Clinical assessment of three common tests for superior labral anterior-posterior lesions. Am J Sports Med 2002;30:810-815.
O’Brien SJ, Pagnani MJ, Fealy S, et al: The active compression test: A new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med
1998;26:610-613.
REFERENCE: Snyder SJ, Karzel RP, Delpizzo W: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch cysts. J Shoulder Elbow Surg 2002;11:600-604.
McFarland EG, Kim TK, Savino RM: Clinical assessment of three common tests for superior labral anterior-posterior lesions. Am J Sports Med 2002;30:810-815.
O’Brien SJ, Pagnani MJ, Fealy S, et al: The active compression test: A new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. Am J Sports Med
1998;26:610-613.
Question 5High Yield
Figure 1 is a representative MRI scan of a 45-year-old man who was lifting a couch 2 days ago when he felt a pop in the elbow and had immediate pain in this area. He had no problems with the elbow prior to this injury. Examination reveals full range of motion; however, he has significant bruising and swelling in the antecubital fossa. A hook test is positive. If choosing to perform single-incision surgical repair for this injury, what is the most common complication associated with this procedure?
Explanation
This patient has a complete distal biceps rupture, as evidenced by history, examination and imaging. Surgical repair is typically recommended in otherwise healthy patients to restore supination strength of the forearm. Surgical repair can be undertaken using either a single- or dual-incision approach. The single-incision approach is associated with injury to the lateral
antebrachial cutaneous nerve, whereas the dual-incision approach carries an increased risk of radioulnar synostosis. Tendon retear and radial nerve injury, while possible, are less common.
71
antebrachial cutaneous nerve, whereas the dual-incision approach carries an increased risk of radioulnar synostosis. Tendon retear and radial nerve injury, while possible, are less common.
71
Question 6High Yield
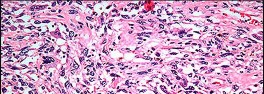
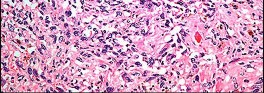
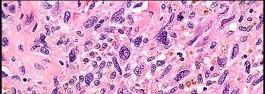
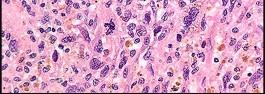
Figures 82a and 82b are the histopathology of an otherwise healthy 50-year-old man who had a growing mass marginally excised from his shoulder with local anesthetic and no presurgical imaging. The mass includes the deep fascia and muscle and is larger than 5 cm. Postsurgical MR imaging was obtained, and T2 and T1+C images are shown in Figures 82c and 82d. What is the best local treatment option?




Explanation
The misdiagnosis of a soft-tissue mass is fairly common. However, in this scenario, the first indication that the presumed diagnosis was incorrect is supported by rapid growth over a short time period. Generally, lipomas and many other benign soft-tissue masses grow slowly over years rather than weeks or months. On MRI, a lipoma classically demonstrates homogenous high-signal intensity on a T1 sequence and fairly low-signal intensity on a T2 sequence. No imaging was done
before surgery, but a high-grade sarcoma generally shows a heterogenous signal on T1 and T2 sequences that is distinctly different than the pattern of a lipoma. The histopathology is consistent with a high-grade sarcoma; a spindle-cell tumor with hypercellularity, anaplasia, and pleomorphism. Mitotic figures are also noted, suggesting rapid turnover and growth. This is a high-grade sarcoma that is treated with wide surgical excision, and observation is not recommended. External beam radiation is often used as an adjuvant either before or after surgery to help decrease the local recurrence rate. Radiation alone would not be sufficient treatment. The use of chemotherapy is controversial. In the setting of a “whoops” or unintended resection of a high-grade soft-tissue sarcoma, reexcision of the tumor bed with radiation is generally indicated. The radiation is used to eliminate microscopic contamination. However, evidence supports surgery alone for superficial (subcutaneous) sarcomas.
RECOMMENDED READINGS
67. [Mankin HJ, Mankin CJ, Simon MA. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am. 1996 May;78(5):656-63. PubMed PMID: 8642021.](http://www.ncbi.nlm.nih.gov/pubmed/8642021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8642021)
68. Noria S, Davis A, Kandel R, Levesque J, O'Sullivan B, Wunder J, Bell R. Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am. 1996 May;78(5):650-
[5/. PubMed PMID: 8642020.](http://www.ncbi.nlm.nih.gov/pubmed/8642020)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8642020)
69. [Gibbs CP, Peabody TD, Mundt AJ, Montag AG, Simon MA. Oncological outcomes of operative treatment of subcutaneous soft-tissue sarcomas of the extremities. J Bone Joint Surg Am. 1997 Jun;79(6):888-97. PubMed PMID: 9199387.](http://www.ncbi.nlm.nih.gov/pubmed/9199387)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9199387)
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 86
Figures 83a through 83d are the prefracture and postfracture radiographs of a previously healthy 19-year-old man who learned he had a high-grade conventional osteosarcoma of his left distal femur after undergoing open biopsy of a large left thigh mass. Staging study findings were negative for evidence of metastases, and he began neoadjuvant chemotherapy. Despite use of a hinged knee brace and weight bearing limitations with crutches, he experienced a sudden increase in pain while rising from bed between his first and second cycles of chemotherapy.
before surgery, but a high-grade sarcoma generally shows a heterogenous signal on T1 and T2 sequences that is distinctly different than the pattern of a lipoma. The histopathology is consistent with a high-grade sarcoma; a spindle-cell tumor with hypercellularity, anaplasia, and pleomorphism. Mitotic figures are also noted, suggesting rapid turnover and growth. This is a high-grade sarcoma that is treated with wide surgical excision, and observation is not recommended. External beam radiation is often used as an adjuvant either before or after surgery to help decrease the local recurrence rate. Radiation alone would not be sufficient treatment. The use of chemotherapy is controversial. In the setting of a “whoops” or unintended resection of a high-grade soft-tissue sarcoma, reexcision of the tumor bed with radiation is generally indicated. The radiation is used to eliminate microscopic contamination. However, evidence supports surgery alone for superficial (subcutaneous) sarcomas.
RECOMMENDED READINGS
67. [Mankin HJ, Mankin CJ, Simon MA. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am. 1996 May;78(5):656-63. PubMed PMID: 8642021.](http://www.ncbi.nlm.nih.gov/pubmed/8642021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8642021)
68. Noria S, Davis A, Kandel R, Levesque J, O'Sullivan B, Wunder J, Bell R. Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am. 1996 May;78(5):650-
[5/. PubMed PMID: 8642020.](http://www.ncbi.nlm.nih.gov/pubmed/8642020)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8642020)
69. [Gibbs CP, Peabody TD, Mundt AJ, Montag AG, Simon MA. Oncological outcomes of operative treatment of subcutaneous soft-tissue sarcomas of the extremities. J Bone Joint Surg Am. 1997 Jun;79(6):888-97. PubMed PMID: 9199387.](http://www.ncbi.nlm.nih.gov/pubmed/9199387)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9199387)
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 86
Figures 83a through 83d are the prefracture and postfracture radiographs of a previously healthy 19-year-old man who learned he had a high-grade conventional osteosarcoma of his left distal femur after undergoing open biopsy of a large left thigh mass. Staging study findings were negative for evidence of metastases, and he began neoadjuvant chemotherapy. Despite use of a hinged knee brace and weight bearing limitations with crutches, he experienced a sudden increase in pain while rising from bed between his first and second cycles of chemotherapy.
Question 7High Yield
A 3-year-old girl is seen for an evaluation of short stature. Physical examination reveals angular deformities of the upper and lower extremities, as well as blue coloration of the sclera and abnormal dentition. Lower extremity imaging shows diffuse osteopenia and mild angular deformities of the tibia and femur bilaterally. These physical and radiographic findings are consistent with a genetic abnormality that most commonly affects the formation of which type of collagen?
Explanation
■
The physical and radiographic findings are consistent with a diagnosis of osteogenesis imperfecta (OI). Approximately 90% of cases of OI are secondary to defects in the COLIA1 or COLIA2 genes, which affect the production of type 1 collagen. The incidence of OI is between 1 in 10,000 and 1 in 20,000. Type II collagen abnormalities have been associated with achondrogenesis type 2. Type IV abnormalities with Alport syndrome, and type X defects with Schmid metaphyseal chondrodysplasia.
The physical and radiographic findings are consistent with a diagnosis of osteogenesis imperfecta (OI). Approximately 90% of cases of OI are secondary to defects in the COLIA1 or COLIA2 genes, which affect the production of type 1 collagen. The incidence of OI is between 1 in 10,000 and 1 in 20,000. Type II collagen abnormalities have been associated with achondrogenesis type 2. Type IV abnormalities with Alport syndrome, and type X defects with Schmid metaphyseal chondrodysplasia.
Question 8High Yield
Figures 92a through 92c are the radiographs of a 34-year-old man with low-back pain and an inability to walk upright. What is the appropriate surgical treatment?
A B C
A B C



Explanation
This patient has a marked fixed sagittal imbalance and a mild coronal imbalance. His fused sacroiliac joints indicate ankylosing spondylitis. Sufficient correction likely can be achieved with a pedicle subtraction osteotomy in the midlumbar spine. Smith-Petersen osteotomies necessitate flexibility of the anterior column, which is not associated with this diagnosis. Also, osteoclasis can result in vascular injuries. Vertebral column resection should not be needed in this case.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
[Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. ](http://www.ncbi.nlm.nih.gov/pubmed/11884909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884909)
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
[Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. ](http://www.ncbi.nlm.nih.gov/pubmed/11884909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11884909)
Question 9High Yield
Figure 75 shows the radiograph of a healthy 52-year-old woman who has severe right hip pain that has been unresponsive to nonsurgical management. What is the most appropriate surgical procedure at this time?
Explanation
DISCUSSION: The patient has developmental dysplasia of the right hip, as can be noted by the shallow acetabulum and lack of femoral head coverage. She has secondary osteoarthritis, manifested radiographically by joint space narrowing, periarticular sclerosis, and subchondral acetabular cyst formation. Femoral and/or acetabular redirectional osteotomies are most effective when performed before the onset of arthritis. After osteoarthritis has set in, total hip arthroplasty is the most reliable procedure for reducing pain. Hemiarthroplasties are not indicated in the presence of arthritic changes of the acetabulum.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 403-414.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 403-414.
Question 10High Yield
All of the following suggest a possibility of malignant transformation in multiple hereditary exostoses except:
Explanation
Stippling on radiographs in the cap is due to calcification and is a common characteristic of cartilaginous tumors.
Question 11High Yield
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome?
Explanation
The only factor that is prognostic for outcomes is the quality of the reduction. None of the other factors has any effect on the outcome. Early range of motion or physical therapy may offer temporary effects, but these small advantages do not last beyond 3 months after surgery.
Question 12High Yield
Which of the following is the best method of treatment for a dominant vertebral artery injury during an occipitocervical fusion?
Explanation
In dominant vertebral artery injury (usually left sided), direct repair is the best method of treatment despite the technical demands of the exposure and microvascular repair. Direct repair can minimize immediate and delayed risks of injury and ischemia. Aggressive packing can result in delayed hemorrhage or fistula formation. Ligation-associated morbidities such as cerebellar infarction, cranial nerve palsies, hemiplegia, and even a mortality rate of 12% have been reported. Screw placement is usually sufficient to control bleeding, but should be considered as a last resort in cases of dominant vertebral artery injury.
Question 13High Yield
Normal activities, such as walking 1 km/hour, create forces across the hip joint of times body weight:
Explanation
Normal activities increase forces over the hip to three times body weight. Jogging increases forces across the hip by five to eight times body weight
Question 14High Yield
..The best initial treatment would entail
Explanation
- isointense signal to the rotator cuff. PREFERRED RESPONSE: 1- calcium carbonate apatite.
PREFERRED RESPONSE: 1- physical therapy and nonsteroidal anti-inflammatory medications.
PREFERRED RESPONSE: 1- physical therapy and nonsteroidal anti-inflammatory medications.
Question 15High Yield
Slide 1
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
Explanation
The extensor hallucis longus or the extensor hallucis brevis (rarely the abductor hallucis) may be used as a tendon transfer for correction. Arthrodesis of the hallux interphalangeal joint may be performed for correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.
Question 16High Yield
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should
consist of
consist of
Explanation
Rupture of the pectoralis major tendon most commonly occurs during bench pressing. Wolfe and associates have shown that the most inferiorly located fibers of the sternal head lengthen disproportionately during the final 30 degrees of humeral extension during the bench press. This creates a mechanical disadvantage in the final portion of the eccentric phase of the lift; with forceful flexion of the shoulder these maximally stretched fibers may rupture. In most patients, particularly in young athletes, the treatment of choice is anatomic repair of the ruptured tendon to its insertion in the proximal humerus either with suture anchors or transosseous sutures. Following surgery, most patients experience a near normal return of strength and significant improvement in the cosmetic appearance of the deformity. While more technically challenging, repair of chronic rupture is possible and is indicated in some patients.
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 17High Yield
Which of the following muscle groups comprises the mobile wad of the forearm:
Explanation
The forearm contains the anterior, dorsal, and mobile wad. The following muscles are located in each compartment: Mobile wad
Brachioradialis
Extensor carpi radialis brevis
Extensor carpi radialis longus
Volar compartment
Flexor carpi ulnaris
Flexor digitorum profundus Flexor digitorum superficialis Palmaris longus
Flexor carpi radialis
Flexor pollicis longus
Brachioradialis
Extensor carpi radialis brevis
Extensor carpi radialis longus
Volar compartment
Flexor carpi ulnaris
Flexor digitorum profundus Flexor digitorum superficialis Palmaris longus
Flexor carpi radialis
Flexor pollicis longus
Question 18High Yield
What are the most common primary sites for carcinomas metastatic to bone?
Explanation
The lung, breast, prostate, kidney, and thyroid are the most common primary sites metastatic to bone. Thyroid cancer metastases are becoming less common when patients pursue treatment. Other metastatic disease including metastases from cervical, hepatocellular, adrenal, and bladder cancers is less common. Metastatic disease most commonly involves the spine and pelvis.
RECOMMENDED READINGS
108. Nielsen GP, Rosenberg AE. _Diagnostic Pathology Bone_. Manitoba, Canada: Amirsys; 2013:14.1-14.7.
109. Coleman R, Brown J, Terpos E, Lipton A, Smith MR, Cook R, Major P. Bone markers and their prognostic value in metastatic bone disease: clinical evidence and future directions. Cancer Treat Rev. 2008 Nov;34(7):629-39. doi: 10.1016/j.ctrv.2008.05.001. Epub 2008 Jun 24. Review. PubMed PMID:
[18579314.](http://www.ncbi.nlm.nih.gov/pubmed/18579314)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18579314)
RECOMMENDED READINGS
108. Nielsen GP, Rosenberg AE. _Diagnostic Pathology Bone_. Manitoba, Canada: Amirsys; 2013:14.1-14.7.
109. Coleman R, Brown J, Terpos E, Lipton A, Smith MR, Cook R, Major P. Bone markers and their prognostic value in metastatic bone disease: clinical evidence and future directions. Cancer Treat Rev. 2008 Nov;34(7):629-39. doi: 10.1016/j.ctrv.2008.05.001. Epub 2008 Jun 24. Review. PubMed PMID:
[18579314.](http://www.ncbi.nlm.nih.gov/pubmed/18579314)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18579314)
Question 19High Yield
During the course of a revision total knee arthroplasty via a medial parapatellar exposure, the surgeon does a complete intra-articular release and synovectomy but exposure is still inadequate. A quadriceps snip is performed and, at the end of the procedure, the knee is stable throughout a range of motion and the postoperative radiographs show acceptable alignment of the components. The patient’s postoperative physical therapy regimen should include which of the following?


Explanation
**DISCUSSION** : A quadriceps snip is performed by extending a medial parapatellar approach superiorly and laterally across the quadriceps tendon. It is then repaired primarily at the end of the procedure. The primary advantage of this technique over other surgical maneuvers that improve exposure at the time of revision total knee arthroplasty is that the postoperative regimen for physical therapy does not need to be altered.
**
**DISCUSSION** : A quadriceps snip is performed by extending a medial parapatellar approach superiorly and laterally across the quadriceps tendon. It is then repaired primarily at the end of the procedure. The primary advantage of this technique over other surgical maneuvers that improve exposure at the time of revision total knee arthroplasty is that the postoperative regimen for physical therapy does not need to be altered.
**
Scientific References
- : Younger AS, Duncan CP, Masri BA: Surgical exposures in revision total knee arthroplasty. J Am Acad Orthop Surg 1998;6:55-64.
Della Valle CJ, Berger RA, Rosenberg AG: Surgical exposures in revision total knee arthroplasty. Clin Orthop Relat Res 2006;446:59-68.
Barrack RL, Smith P, Munn B, et al: The Ranawat Award. Comparison of surgical approaches in total knee
arthroplasty. Clin Orthop Relat Res 1998;356:16-21.
Question 2
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
1. ### initiation of a first-generation cephalosporin while awaiting culture results.
2. ### initiation of broad-spectrum antibiotics while awaiting culture results.
3. ### ultrasound to evaluate for fluid collection around the knee.
4. ### surgical debridement of the knee before culture results are available.
5. ### inpatient observation and no antibiotics until culture results are available.
PREFERRED RESPONSE: 4**
**DISCUSSION** : Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
Figure 3a Figure 3b
Question 20High Yield
The use of bisphosphonates in children with osteogenesis imperfecta is becoming more widely accepted as treatment to improve quality of life and to decrease the risks of fracture. What is the mechanism by which bisphosphonates work?

Explanation
DISCUSSION: The mechanism by which bisphosphonates act is by inhibiting osteoclasts. One mechanism of bisphosphonates is to cause osteoclast apoptosis. Another mechanism of bisphosphonates is to disrupt the cytoskeleton of osteoclasts, resulting in loss of the ruffled border. The uncoupling of bone resorption and bone formation with decreased bone resorption results in increased bone mineralization. This translates into fewer fractures in patients with osteogenesis imperfecta and improved quality of life.
REFERENCES: Bumei G, Vlad C, Georgescu I, et al: Osteogenesis imperfecta: Diagnosis and treatment. J Am Acad Orthop Surg 2008;16:356-366.
Lin JT, Lane JM: Bisphosphonates. J Am Acad Orthop Surg 2003; 11:1-4.
Seikaly MG, Kopanati S, Salhab N, et al: Impact of alendronate on quality of life in children with osteogenesis imperfecta. J Pediatr Orthop 2005;25:786-791.
Figure 40
REFERENCES: Bumei G, Vlad C, Georgescu I, et al: Osteogenesis imperfecta: Diagnosis and treatment. J Am Acad Orthop Surg 2008;16:356-366.
Lin JT, Lane JM: Bisphosphonates. J Am Acad Orthop Surg 2003; 11:1-4.
Seikaly MG, Kopanati S, Salhab N, et al: Impact of alendronate on quality of life in children with osteogenesis imperfecta. J Pediatr Orthop 2005;25:786-791.
Figure 40
Question 21High Yield
A 15-year-old football player was diagnosed with infectious mononucleosis 2 weeks ago. Today he states that he is relatively asymptomatic and would like to return to play. At what point can the patient return to full contact practice?
Explanation
Infectious mononucleosis presents with fever, pharyngitis, fatigue and lymph node enlargement. It is common among individuals in their teens and early twenties. Participation in contact activities during an acute illness with unresolved splenomegaly increases the risk of splenic rupture. Evidence- based return to play criteria recommend that a patient may return to full- contact activities 4 weeks after the onset of their symptoms with resolution of splenomegaly. An ultrasonography of the spleen can help confirm that the spleen has returned to normal size.
75
75
Question 22High Yield
What is the most common cause of early failure for patellofemoral arthroplasty?

Explanation
DISCUSSION: In properly selected patients who have no or minimal tibiofemoral arthritis, the most common cause of early failure is patellofemoral instability secondary to uncorrected patellar malalignment, soft-tissue imbalance, or component malposition. Progression of tibiofemoral arthritis is also a leading cause of failure, but occurs late in about 25% of patients. Loosening of components has occurred in less than 1% of knees with cemented implants. A higher rate of loosening has been reported in cementless implants.
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.
Figure 48
DISCUSSION: In properly selected patients who have no or minimal tibiofemoral arthritis, the most common cause of early failure is patellofemoral instability secondary to uncorrected patellar malalignment, soft-tissue imbalance, or component malposition. Progression of tibiofemoral arthritis is also a leading cause of failure, but occurs late in about 25% of patients. Loosening of components has occurred in less than 1% of knees with cemented implants. A higher rate of loosening has been reported in cementless implants.
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.
Figure 48
Question 23High Yield
81
Figures 94a and 94b show T1 sagittal and coronal MR images of the right shoulder of a 45-year-old woman. She has insidious onset of dull, aching right shoulder pain localized at the superior aspect of her shoulder. The nerve that supplies the atrophied muscle arises from the upper trunk from contributions of which nerve roots?
A
B
Figures 94a and 94b show T1 sagittal and coronal MR images of the right shoulder of a 45-year-old woman. She has insidious onset of dull, aching right shoulder pain localized at the superior aspect of her shoulder. The nerve that supplies the atrophied muscle arises from the upper trunk from contributions of which nerve roots?
A
B
Explanation
The suprascapular nerve innervates the supraspinatus muscle. Patients with suprascapular neuropathy usually have insidious onset of dull, aching shoulder pain at the superior or posterior aspect of the shoulder. There can be several causes of nerve compression, and the nerve is susceptible to compression at the suprascapular and spinoglenoid notches. Extrinsic compression can be secondary to joint-related fluid filled cysts of soft-tissue masses. Traction neuropathy may occur as the result of excessive nerve excursion during athletic activity (usually overhead sports) or after a massive, retracted rotator cuff tear. The suprascapular nerve originates from the upper trunk from predominantly the C5 and C6 nerve roots, with an occasional contribution from the C4 nerve root.
RECOMMENDED READINGS
1. Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64. doi: 10.2106/JBJS.I.01743. Review. 81
[PubMed PMID: 20926731. ](http://www.ncbi.nlm.nih.gov/pubmed/20926731)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20926731)
2. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677 ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
RECOMMENDED READINGS
1. Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64. doi: 10.2106/JBJS.I.01743. Review. 81
[PubMed PMID: 20926731. ](http://www.ncbi.nlm.nih.gov/pubmed/20926731)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20926731)
2. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677 ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
Question 24High Yield
Figures 10a through 10c are the radiographs and MR image of a 65-year-old woman with rheumatoid arthritis who has posterior headaches, hand and gait clumsiness, and dizziness. What is the most likely diagnosis?



Explanation
Rheumatoid arthritis is a chronic inflammatory synovitis. The neck is a common site of involvement, after hands and feet. Fortunately, radiographic evidence of instability does not equal neurological deficits. The 3 most common cervical presentations are atlantoaxial subluxation, basilar invagination, and subaxial subluxation. Atlantoaxial subluxation is attributable to an incompetent transverse ligament or erosion of the dens. It is demonstrated by a widened anterior atlantodental interval. Basilar invagination is attributable to cranial settling with the tip of the dens pressing on the spinal cord or midbrain. Subaxial subluxation is attributable to the destabilization of the facet joints.
Basilar invagination symptoms can include posterior headaches, cervical myelopathy, dizziness, and sudden death from compression of the medulla oblongata. In this scenario, there is no subaxial or atlantoaxial subluxation or rheumatoid plaque.
RECOMMENDED READINGS
17. [Fujiwara K, Owaki H, Fujimoto M, Yonenobu K, Ochi T. A long-term follow-up study of cervical lesions in rheumatoid arthritis. J Spinal Disord. 2000 Dec;13(6):519-26. PubMed PMID: 11132984. ](http://www.ncbi.nlm.nih.gov/pubmed/11132984)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11132984)
18. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A longterm analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993 Sep;75(9):1282-
[97/. PubMed PMID: 8408150. ](http://www.ncbi.nlm.nih.gov/pubmed/8408150)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8408150)
19. [Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001 Feb;83-A(2):194-200. PubMed PMID: 11216680. ](http://www.ncbi.nlm.nih.gov/pubmed/11216680)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216680)
Basilar invagination symptoms can include posterior headaches, cervical myelopathy, dizziness, and sudden death from compression of the medulla oblongata. In this scenario, there is no subaxial or atlantoaxial subluxation or rheumatoid plaque.
RECOMMENDED READINGS
17. [Fujiwara K, Owaki H, Fujimoto M, Yonenobu K, Ochi T. A long-term follow-up study of cervical lesions in rheumatoid arthritis. J Spinal Disord. 2000 Dec;13(6):519-26. PubMed PMID: 11132984. ](http://www.ncbi.nlm.nih.gov/pubmed/11132984)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11132984)
18. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A longterm analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993 Sep;75(9):1282-
[97/. PubMed PMID: 8408150. ](http://www.ncbi.nlm.nih.gov/pubmed/8408150)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8408150)
19. [Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001 Feb;83-A(2):194-200. PubMed PMID: 11216680. ](http://www.ncbi.nlm.nih.gov/pubmed/11216680)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11216680)
Question 25High Yield
A 31-year-old woman underwent a left Kidner procedure 3 months ago. She now has pain overlying the medial column of the foot. She withdraws the foot when touching of the medial foot is attempted. Examination reveals allodynia, pain, hyperalgesia, and edema of the medial foot. What is the most likely diagnosis?
Explanation
**
Patients with reflex sympathetic dystrophy (RSD) have a history of trauma, minor rather than major (eg, Colles fracture), in about 50% to 65% of cases. The condition may also follow a surgical procedure. Patients usually have symptoms and signs of RSD including: pain, described as burning, throbbing, shooting, or aching; hyperalgesia; allodynia; and hyperpathia. There are trophic changes within 10 days of onset of RSD in 30% of the extremities affected, including stiffness and edema and atrophy of hair, nails, and/or skin.
Finally there can be autonomic dysfunction, such as abnormal sweating, either
in excess or anhydrosis, heat and cold insensitivity, or redness or bluish discoloration of the extremities. Shingles, also called herpes zoster or zoster, is a painful skin rash caused by the varicella zoster virus (VZV). VZV is the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays in the body.
Usually the virus does not cause any problems; however, the virus can reappear years later, causing shingles. Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from
0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature),
erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin.
Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Patients with reflex sympathetic dystrophy (RSD) have a history of trauma, minor rather than major (eg, Colles fracture), in about 50% to 65% of cases. The condition may also follow a surgical procedure. Patients usually have symptoms and signs of RSD including: pain, described as burning, throbbing, shooting, or aching; hyperalgesia; allodynia; and hyperpathia. There are trophic changes within 10 days of onset of RSD in 30% of the extremities affected, including stiffness and edema and atrophy of hair, nails, and/or skin.
Finally there can be autonomic dysfunction, such as abnormal sweating, either
in excess or anhydrosis, heat and cold insensitivity, or redness or bluish discoloration of the extremities. Shingles, also called herpes zoster or zoster, is a painful skin rash caused by the varicella zoster virus (VZV). VZV is the same virus that causes chickenpox. After a person recovers from chickenpox, the virus stays in the body.
Usually the virus does not cause any problems; however, the virus can reappear years later, causing shingles. Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from
0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature),
erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin.
Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Question 26High Yield
A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan is shown in Figure 17. Management should consist of
Explanation
The MRI findings reveal a disruption of the humeral insertion of the glenohumeral ligaments and joint capsule (humeral avulsion of the glenohumeral ligament). This lesion has been reported to account for an 8% rate of recurrent dislocation in a subset of patients who are typically older than those with the more common lesions of the glenoid labrum (Bankart lesion). Open repairs have been reported to be successful in the prevention of recurrent instability. Since there is no Bankart lesion, open or arthroscopic labral repairs are not indicated. Nonsurgical management is possible if the patient does not want to undergo surgery; however, the recurrence rate is very high.
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bokor DJ. Conboy VB. Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br
1999;81:93-96.
Coates MH, Breidahl W: Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661-666.
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bokor DJ. Conboy VB. Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br
1999;81:93-96.
Coates MH, Breidahl W: Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661-666.
Question 27High Yield
A patient experienced a nondisplaced fracture of the medial and middle cuneiforms. His nonoperative treatment consisted of cast immobilization for 2 weeks with no weight bearing permitted, followed by ambulation as tolerated. He presents for treatment 1 week later with severe swelling in the foot, stiffness of the toes, and limited motion of the hindfoot. The fracture of the
cuneiforms appears healed. The ideal management of the stiffness and swelling of the foot is:
cuneiforms appears healed. The ideal management of the stiffness and swelling of the foot is:
Explanation
Patients who develop swelling of the foot and ankle following trauma and surgery can be effectively treated with application of an intermittent foot pump device. The bladder of the foot pump can be inserted into either a removable boot or cast, or applied to the foot in combination with other methods of rehabilitation. The foot pump is an effective device for decreasing swelling of the foot in association with acute trauma.
Question 28High Yield
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching. Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a wide-based gait, intrinsic wasting, and a positive Hoffman's sign bilaterally. An MRI scan of the cervical spine is shown in Figure

Explanation
■
The patient has classic symptoms of myelopathy with upper motor neuron signs on examination. His symptoms have been present for years, and are getting worse. The cervical spine MRI scan shows spinal stenosis with multilevel spondylosis causing spinal cord compression at multiple levels. With the longstanding duration of the patient's signs and symptoms, combined with involvement of multiple levels in the cervical spine, posterior multilevel laminectomy and fusion is the best treatment option. Two-level anterior diskectomy and fusion would address the two areas of most severe narrowing, but it would fail to decompress the other stenotic areas which also require decompression. Posterior cervical foraminotomies would only address radicular symptoms, which are not present in this patient, and would not succeed in decompression of the spinal cord. Cervical epidural injections are not indicated for myelopathy symptoms, and may in fact place this patient at risk for neurologic deterioration.
The patient has classic symptoms of myelopathy with upper motor neuron signs on examination. His symptoms have been present for years, and are getting worse. The cervical spine MRI scan shows spinal stenosis with multilevel spondylosis causing spinal cord compression at multiple levels. With the longstanding duration of the patient's signs and symptoms, combined with involvement of multiple levels in the cervical spine, posterior multilevel laminectomy and fusion is the best treatment option. Two-level anterior diskectomy and fusion would address the two areas of most severe narrowing, but it would fail to decompress the other stenotic areas which also require decompression. Posterior cervical foraminotomies would only address radicular symptoms, which are not present in this patient, and would not succeed in decompression of the spinal cord. Cervical epidural injections are not indicated for myelopathy symptoms, and may in fact place this patient at risk for neurologic deterioration.
Question 29High Yield
Which complication is most common after syndesmotic fixation?
Explanation
The injury radiographs reveal a supination external rotation IV ankle fracture with evidence of medial clear space widening exceeding 4 mm and an increase relative to the superior tibiotalar clear space. This indicates injury to the deltoid ligament and necessitates surgical reduction and fixation to restore and maintain ankle stability. Following stabilization of the fibula, an intraoperative stress examination of the syndesmosis such as an external rotation stress test under fluoroscopy or lateral pull on the fibula (the Cotton test) should be performed to determine the integrity of the syndesmosis. Radiographic evidence of tibiofibular clear space widening, medial clear space widening with external rotation, and lateral displacement of the distal fibula when pulled is consistent with syndesmotic injury. In contrast to the presurgical stress test, once the fibula has been reduced and stabilized lateral talar translation can occur only if the syndesmosis is injured in addition to the deltoid ligament. Failure of the syndesmotic screw without evidence of malalignment of the mortise and a pain-free ankle are not indications for further surgery because these patients have satisfactory outcomes when compared to those who have intact or removed screws. Hardware removal following fibula ORIF is indicated when patients have pain directly related to hardware prominence. Resolution of joint pain or stiffness is not a reliable outcome following hardware removal. Although fibular fracture can occur, this is a rare complication. Malreduction of the syndesmosis is the most common complication following ORIF of the syndesmosis and is improved with direct visualization; however, malreduction still may occur with direct visualization.
RECOMMENDED READINGS
[Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. doi: 10.1097/BOT.0b013e3181a9f7a5. PubMed PMID: 20035170. ](http://www.ncbi.nlm.nih.gov/pubmed/20035170)[View](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005 Oct;19(9):604-9. PubMed PMID: 16247304. ](http://www.ncbi.nlm.nih.gov/pubmed/16247304)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16247304)
[Stark E, Tornetta P 3rd, Creevy WR. Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma. 2007 Oct;21(9):643-6. PubMed PMID: 17921840. ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[View](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17921840)
[Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4. PubMed PMID: 11371792. ](http://www.ncbi.nlm.nih.gov/pubmed/11371792)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11371792)
RECOMMENDED READINGS
[Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. doi: 10.1097/BOT.0b013e3181a9f7a5. PubMed PMID: 20035170. ](http://www.ncbi.nlm.nih.gov/pubmed/20035170)[View](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20035170)
[Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005 Oct;19(9):604-9. PubMed PMID: 16247304. ](http://www.ncbi.nlm.nih.gov/pubmed/16247304)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16247304)
[Stark E, Tornetta P 3rd, Creevy WR. Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma. 2007 Oct;21(9):643-6. PubMed PMID: 17921840. ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[View](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17921840)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17921840)
[Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4. PubMed PMID: 11371792. ](http://www.ncbi.nlm.nih.gov/pubmed/11371792)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11371792)
Question 30High Yield
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
FOR QUESTIONS 108 THROUGH 110:**_
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 31High Yield
Pagetâs disease is common in all of the listed locations except:
Explanation
Key features of Pagetâs disease
Remodeling disease caused by excessive osteoclastiCactivity
Rarely diagnosed in patients younger than 40 years of age; most patients diagnosed after age 50
Most common sites include pelvis, femur, spine, skull, and tibia
Less common sites include clavicles, scapulae, ribs, and facial bones
Rarely found in the hands and feet
PagetiCbone
is more susceptible to fracture is less compact
is more vascular
tends to bow in weight bearing areas
GeographiCclustering (up to 4% in patients older than 55 years of age) England
Northern Europe North America Australia, New Zealand
Rare in Asia, China, Indonesia, Malaysia, and sub-Saharan Africa
Possibly a slow viral disease
RNA paramyxovirus (e.g., respiratory syncytial virus and measles) Correct Answer: Sub-Saharan Africa
Remodeling disease caused by excessive osteoclastiCactivity
Rarely diagnosed in patients younger than 40 years of age; most patients diagnosed after age 50
Most common sites include pelvis, femur, spine, skull, and tibia
Less common sites include clavicles, scapulae, ribs, and facial bones
Rarely found in the hands and feet
PagetiCbone
is more susceptible to fracture is less compact
is more vascular
tends to bow in weight bearing areas
GeographiCclustering (up to 4% in patients older than 55 years of age) England
Northern Europe North America Australia, New Zealand
Rare in Asia, China, Indonesia, Malaysia, and sub-Saharan Africa
Possibly a slow viral disease
RNA paramyxovirus (e.g., respiratory syncytial virus and measles) Correct Answer: Sub-Saharan Africa
Question 32High Yield
Slide 1 Slide 2
You are planning a tendon transfer to help correct deformity in a patient with hereditary sensory motor neuropathy. Which of the following muscles will be used for the transfer based upon the clinical appearance of the foot (Slide 1 and Slide 2):
You are planning a tendon transfer to help correct deformity in a patient with hereditary sensory motor neuropathy. Which of the following muscles will be used for the transfer based upon the clinical appearance of the foot (Slide 1 and Slide 2):
Explanation
The posterior tibial tendon transfer is a commonly performed surgery for correction of cavus foot deformity associated with weakness of the anterior tibial muscle and varying degrees of drop foot deformity. The removal of the force of the posterior tibial tendon adds to the correction of the deformity of the foot by balancing the absent peroneus brevis. Although the extensor hallucis longus can be used as a tendon transfer, it will not be the primary muscle used or sufficient to correct deformity.
Question 33High Yield
2010 Pediatric Orthopaedic Examination Answer Book *15
Achondroplasia is caused by an abnormality of which of the following?
Achondroplasia is caused by an abnormality of which of the following?
Explanation
Achondroplasia results from mutation of the fibroblast growth factor receptor 3. Bone morphogenic proteins are regulators of growth differentiation and morphogenic embryology. Anomalies of this protein are seen in increasing defects in limbs distally. Parathyroid-related protein is seen in Jensen-type metaphyseal chondrodysplasia. Transforming growth factors and the morphogenic proteins affect the production of matrix.
REFERENCES: Leet Al, Chomey GS: The physis, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 327-332.
van der Eerden BC, Karperian M, Wit JM: Systemic and local regulators of the growth plate. Endocr Rev 2003;24:782-801.
Figure 12
REFERENCES: Leet Al, Chomey GS: The physis, in Cramer KE, Scherl SA, Einhom TA (eds): Orthopaedic Surgery Essentials: Pediatrics. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 327-332.
van der Eerden BC, Karperian M, Wit JM: Systemic and local regulators of the growth plate. Endocr Rev 2003;24:782-801.
Figure 12
Question 34High Yield
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Explanation
DISCUSSION: The examination and radiographs are consistent with a sleeve fracture of the patella, which is an avulsion fracture of the distal pole of the patella with a disruption of the extensor mechanism. Treatment is open reduction and internal fixation of the patella, and repair of the extensor mechanism.
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
1. ##### Lateral femoral circumflex
2. ##### Medial femoral circumflex
3. ##### Superior gluteal
4. ##### Inferior gluteal
5. ##### Obturator PREFERRED RESPONSE: 2
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the
posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
**34 • American Academy of Orthopaedic Surgeons**
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419- 424.
DISCUSSION: The examination and radiographs are consistent with a sleeve fracture of the patella, which is an avulsion fracture of the distal pole of the patella with a disruption of the extensor mechanism. Treatment is open reduction and internal fixation of the patella, and repair of the extensor mechanism.
The distal fragment can be much larger than it appears on the radiographs because it consists largely of cartilage.
REFERENCES: Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990; 10:721 - 730. Question 37
When addressing a proximal intertrochanteric or subtrochanteric fracture in a juvenile with open growth plates, the arterial supply from what artery at the neck must be preserved?
1. ##### Lateral femoral circumflex
2. ##### Medial femoral circumflex
3. ##### Superior gluteal
4. ##### Inferior gluteal
5. ##### Obturator PREFERRED RESPONSE: 2
DISCUSSION: The medial femoral circumflex artery supplies blood to the femoral head. Its position along the
posterior-superior femoral neck places this structure at risk with intramedullary nailing of the femur. Therefore, lateral entry through the greater trochanter is preferred when intramedullary fixation is performed.
**34 • American Academy of Orthopaedic Surgeons**
REFERENCES: Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295- 1301.
Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 419- 424.
Question 35High Yield
Figure 53 is the radiograph obtained at the time of transfer to the trauma center of a 41-year-old man who was involved in a motor vehicle accident. What is the most appropriate initial management?

Explanation
No detailed explanation provided for this question.
Question 36High Yield
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a
small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis? **
small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis? **
Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%.
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 37High Yield
Swan-neck deformity can be caused by which of the following:
Explanation
A chronic mallet finger results in proximal retraction of the extensor mechanism and overpull of the central slip. Isolated central slip rupture does not cause this deformity. Rupture of the flexor digitorum sublimis can cause Swan-neck deformity. MP arthroplasty is not associated with this deformity. The sequalae of dorsal proximal interphalangeal joint dislocation (e.g., volar plate laxity or deficiency) leads to Swan-neck deformity.
Question 38High Yield
A 55-year-old male is involved in a motor vehicle accident and sustains the injury seen in Figure A. What is the most appropriate treatment for this type of injury?


Explanation
The radiographs demonstrate a reverse obliquity intertrochanteric femur fracture. Compared to the more stable intertrochanteric femur fracture, a reverse oblique intertrochanteric hip fracture is not optimally treated with a sliding hip screw. Compression along a sliding hip screw is designed to create compression along the plane of the fracture, however in a reverse obliquity fracture pattern as seen here, shear force is created causing medial displacement of the femoral shaft and screw cutout.
Haidukewych et al showed in their retrospective review of 55 consecutively treated reverse obliquity intertrochanteric fractures, that patients treated with a sliding hip screw had nearly a 56% failure rate (9/16). The failure rate of patients treated with a blade plate was only 13%.
Sadowski et al showed in their prospective randomized trial in patients with a reverse obliquity or transverse intertrochanteric fracture who were randomized to either a 95 degree screw-plate or cephalomedullary nail a much higher failure rate for the plate-screw implant. Implant failure was seen in 7/19 patients treated with the 95 degree screw plate and only 1/30 in the intramedullary nail group. Both articles support the use of a blade plate or cephalomedullary nail for reverse obliquity fractures.
An example of screw cutout and medial displacement is seen in Illustration A.
Haidukewych et al showed in their retrospective review of 55 consecutively treated reverse obliquity intertrochanteric fractures, that patients treated with a sliding hip screw had nearly a 56% failure rate (9/16). The failure rate of patients treated with a blade plate was only 13%.
Sadowski et al showed in their prospective randomized trial in patients with a reverse obliquity or transverse intertrochanteric fracture who were randomized to either a 95 degree screw-plate or cephalomedullary nail a much higher failure rate for the plate-screw implant. Implant failure was seen in 7/19 patients treated with the 95 degree screw plate and only 1/30 in the intramedullary nail group. Both articles support the use of a blade plate or cephalomedullary nail for reverse obliquity fractures.
An example of screw cutout and medial displacement is seen in Illustration A.
Question 39High Yield
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
Explanation
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred.
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
Question 40High Yield
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
Explanation
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended _by some authors to prevent this complication._
Question 41High Yield
Figure 19 is an anteroposterior pelvis radiograph of a 60-year-old woman who has a 4-month history of right hip pain. She has a
medical history of lupus and has used
21
prednisone in the past, but not currently.
Her pain is persistent despite use of over-the-counter pain medications and activity modifications. What is the most appropriate treatment at this point?
medical history of lupus and has used
21
prednisone in the past, but not currently.
Her pain is persistent despite use of over-the-counter pain medications and activity modifications. What is the most appropriate treatment at this point?

Explanation
This scenario describes osteonecrosis of the hip, likely attributable to chronic corticosteroid use. Her radiographs show bilateral hip involvement with whole-head involvement and collapse of the femoral head. Observation, protected weight bearing, and bisphosphonates have been advocated during the precollapse stage, but, considering the advanced
involvement of the femoral heads, these treatments are not indicated. Hip arthroplasty is the most reliable treatment option at this point to resolve her symptoms. Total hip resurfacing is not indicated for multiple reasons, including poor bone stock from corticosteroid use and her age. Large-head involvement and concerns about metal-on-metal articulation in someone with potential for renal impairment (such as a patient with lupus) also are contraindications to total hip resurfacing. Total hip arthroplasty will offer the best chance for success.
RECOMMENDED READINGS
1. Mont M, Bezwasa H. Osteonecrosis: Strategies for treatment. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:477-499.
2. [Lieberman JR, Berry DJ, Mont MA, Aaron RK, Callaghan JJ, Rajadhyaksha AD, Urbaniak JR. Osteonecrosis of the hip: management in the 21st century. Instr Course Lect. 2003;52:337-55. Review. PubMed PMID: 12690862.](http://www.ncbi.nlm.nih.gov/pubmed/12690862)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690862)
involvement of the femoral heads, these treatments are not indicated. Hip arthroplasty is the most reliable treatment option at this point to resolve her symptoms. Total hip resurfacing is not indicated for multiple reasons, including poor bone stock from corticosteroid use and her age. Large-head involvement and concerns about metal-on-metal articulation in someone with potential for renal impairment (such as a patient with lupus) also are contraindications to total hip resurfacing. Total hip arthroplasty will offer the best chance for success.
RECOMMENDED READINGS
1. Mont M, Bezwasa H. Osteonecrosis: Strategies for treatment. In: Callaghan JJ, Rosenberg AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:477-499.
2. [Lieberman JR, Berry DJ, Mont MA, Aaron RK, Callaghan JJ, Rajadhyaksha AD, Urbaniak JR. Osteonecrosis of the hip: management in the 21st century. Instr Course Lect. 2003;52:337-55. Review. PubMed PMID: 12690862.](http://www.ncbi.nlm.nih.gov/pubmed/12690862)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690862)
Question 42High Yield
Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformity
include a
include a


Explanation
The radiographs show a hallux valgus deformity with a laterally deviated distal metatarsal articular surface, a large intermetatarsal angle with medial deviation at the first metatarsocuneiform joint, an elongated medial collateral ligament, and a contracted lateral collateral ligament. There is no distal 1-2 transverse intermetatarsal ligament. The distal transverse ligament in the first interspace extends from the second metatarsal to the lateral (fibular) sesamoid, remains intact, and keeps the sesamoids in a lateral position as the first metatarsal head migrates medially.
RECOMMENDED READINGS
1. Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8589807)
2. Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
RECOMMENDED READINGS
1. Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8589807)
2. Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
Question 43High Yield
82 • American Academy of Orthopaedic Surgeons
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
DISCUSSION: Nonsurgical management of OCD of the talus in skeletally immature individuals frequently results in a fairly rapid decrease in symptoms, but radiographic abnormalities can frequently be found even 6 months after treatment. Spontaneous resolution of this condition is rare. Hyperbaric oxygen treatment has not been shown to be beneficial for this condition. Progression of the condition to the point of requiring ankle fusion is rare.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
DISCUSSION: Nonsurgical management of OCD of the talus in skeletally immature individuals frequently results in a fairly rapid decrease in symptoms, but radiographic abnormalities can frequently be found even 6 months after treatment. Spontaneous resolution of this condition is rare. Hyperbaric oxygen treatment has not been shown to be beneficial for this condition. Progression of the condition to the point of requiring ankle fusion is rare.
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 44High Yield
Mallet finger injuries refer to:
Explanation
Mallet finger injuries may be associated with fractures of the bony tuft, fractures of the middle phalanx, flexor tendon injuries, and intrinsic tightness. However, mallet injuries refer to lack of continuity at the DIP joint.
Question 45High Yield
A 21-year-old Division 1 collegiate track and field athlete has had acute worsening right anterior shin pain for the past week. He reports having shin pain since sophomore year of high school but has continued to run through the pain. Upon presentation, he was diagnosed with a tibial stress fracture and underwent 8 weeks of nonoperative treatment and correction of vitamin D levels. His follow-up radiograph is shown in Figure
Explanation
The case and radiograph describe a chronic anterior tibial stress fracture with radiographic evidence of the "dreaded black line". Both tibial IM nailing and compression plating are acceptable treatment options in the high-level athlete and are associated with a high rate of return to sport. Compression plating results in a higher rate of symptomatic hardware (20%) as compared with tibial IM nailing. Time to radiographic union may be faster with compression plating. This may be due to the mechanical advantage of neutralizing tensile forces and fracture micromotion. Plating avoids disruption of the knee extensor mechanism and the anterior knee pain associated with IM nailing. There are several reports of fracture completion after tibial IM nailing, requiring revision open reduction and internal fixation.
Question 46High Yield
A 55-year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee
arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 47High Yield
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
Indications for open reduction of glenoid intra-articular fractures include those fractures with a 5-mm articular surface displacement or when the humeral head is subluxated with the fracture fragment. Kavanaugh and associates and Leung and Lam have shown that the posterior approach with plate fixation is best for most glenoid fractures, including the Ideberg type II fracture shown here. The anterior approach is best used for anterior rim and transverse fractures.
REFERENCES: Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
REFERENCES: Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 48High Yield
A 68-year-old man presents with chronic progressive right shoulder pain and loss of motion. He has active shoulder elevation of 120° and 5-/5 shoulder forward flexion strength limited by pain. He has exhausted nonsurgical management over the past year and is now interested in surgical intervention. Figure 1 is the preoperative axial CT scan of his shoulder. During surgical reconstruction, the surgeon should anticipate the location of maximal glenoid erosion to be
58
58
Explanation
In patients with primary osteo- arthritis of the shoulder, eccent- ric wear on the face of the glenoid is frequently combined with static subluxation of the humeral head. Current studies have clarified that patients with Walch B2 glenoid develop wear along the posterior inferior face of the glenoid and not directly posterior. At the time of shoulder arthroplasty, the eccentric center of rotation must be corrected by soft-tissue, bony, and/or implant
techniques to minimize the risk for poor outcomes. The surgeon should orient
his correction along the posterior inferior to anterior superior plane.
techniques to minimize the risk for poor outcomes. The surgeon should orient
his correction along the posterior inferior to anterior superior plane.
Question 49High Yield
An obese 62-year-old man (BMI 38) who underwent a cementless total hip arthroplasty 14 months ago fell from a ladder and is now unable to bear weight on the extremity. A radiograph from his 3-month visit is shown in Figure 77a and a radiograph from the time of the injury is shown in Figure 77b. Appropriate management includes which
of the following?
of the following?
Explanation
The patient has a Vancouver type B1 fracture of the femur with a well-fixed femoral component. When comparing the two radiographs, the proximal femoral component position has not changed and remodeling is seen around the component. Nonsurgical management is associated with the complications of extended recumbency. As the femoral component is well-fixed, revision of the femoral component is not necessary.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
Question 50High Yield
A 35-year-old man reports a 2-year history of right groin pain. The pain is made worse with hip flexion, prolonged sitting, and cycling. A radiograph and MRI scan are shown in Figures 16a and 16b. Nonsurgical management has failed to provide relief. What is the best surgical option?

Explanation
DISCUSSION: The patient has cam-type femoral acetabular impingement. He still has a well-maintained joint space without significant degenerative changes, and given his age a joint preserving procedure would be the procedure of choice. A reverse periacetabular osteotomy may be considered in a retroverted acetabulum; however, that is not the case here. A femoral neck osteochondroplasty is required to remove the cam of bone and reshape the femoral head- neck junction to improve the femoral head/neck ratio (femoral head offset). Typically, in isolated cam impingement, cartilage damage in the anterior-superior acetabulum precedes labral damage. Labral debridement alone does not address the pathology of impingement. In cases where labral detachment is present, reattachment has been shown to be superior to labral resection.
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Figure 17a Figure 17b Figure 17c
DISCUSSION: The patient has cam-type femoral acetabular impingement. He still has a well-maintained joint space without significant degenerative changes, and given his age a joint preserving procedure would be the procedure of choice. A reverse periacetabular osteotomy may be considered in a retroverted acetabulum; however, that is not the case here. A femoral neck osteochondroplasty is required to remove the cam of bone and reshape the femoral head- neck junction to improve the femoral head/neck ratio (femoral head offset). Typically, in isolated cam impingement, cartilage damage in the anterior-superior acetabulum precedes labral damage. Labral debridement alone does not address the pathology of impingement. In cases where labral detachment is present, reattachment has been shown to be superior to labral resection.
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Figure 17a Figure 17b Figure 17c
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon