Principles of Orthopaedic Oncology: Limb Salvage and Surgical Margins
Key Takeaway
The decision between limb salvage and amputation in orthopaedic oncology requires a multidisciplinary approach, balancing oncological clearance with functional outcomes. Advances in neoadjuvant chemotherapy, radiation, and advanced imaging have made limb salvage the standard of care for most sarcomas. This guide details the Enneking classification of surgical margins, extended curettage techniques, and complex reconstructive strategies essential for modern orthopedic surgeons managing bone and soft-tissue malignancies.
Principles of Surgical Oncology in Orthopaedics
The surgical management of musculoskeletal tumors has undergone a paradigm shift over the last four decades. Advances in diagnostic imaging, neoadjuvant chemotherapy, radiation therapy, and sophisticated surgical techniques for resection and reconstruction now allow limb salvage to be a highly viable, standard-of-care option for the vast majority of patients presenting with bone or soft-tissue sarcomas.
Specifically, the integration of preoperative radiation therapy for soft-tissue sarcomas and neoadjuvant chemotherapy for bone sarcomas has enabled orthopedic oncologists to successfully resect tumors that historically would have necessitated amputation. However, limb salvage is not universally applicable. Involvement of critical neurovascular bundles, displaced pathological fractures with extensive hematoma contamination, or complications secondary to a poorly executed, non-compartmental biopsy may still preclude limb salvage.
Amputation Versus Limb Salvage: Decision Making
The choice between limb salvage and amputation is complex and must be individualized, heavily weighing the expectations, functional demands, and desires of the patient and their family. Simon classically described four critical issues that must be addressed when contemplating limb salvage over amputation:
- Survival: Would overall survival be affected by the treatment choice?
- Morbidity: How do the short-term and long-term morbidities of the procedures compare?
- Function: How would the biomechanical function of a salvaged limb compare with that of a modern prosthesis following amputation?
- Psychosocial Impact: Are there significant psychosocial consequences associated with either choice?
Clinical Pearl: No study has demonstrated a significant difference between amputation and limb salvage regarding psychological outcomes or quality of life in long-term sarcoma survivors. The decision must align with the patient's long-term lifestyle goals.
With the advent of multimodal treatment protocols, long-term survival for patients with osteosarcoma has dramatically improved from approximately 20% to nearly 70%. For osteosarcoma of the distal femur, the rate of local recurrence following wide resection and limb salvage is approximately 5% to 10%, which is statistically equivalent to the local recurrence rate following a transfemoral amputation.
While radical procedures like hip disarticulation carry an extremely low rate of local recurrence, no evidence suggests a survival advantage over limb salvage, provided that wide surgical margins are obtained. Patients who experience local recurrence despite wide margins often harbor highly aggressive or chemo-resistant disease, conferring a poor prognosis regardless of the initial surgical intervention.
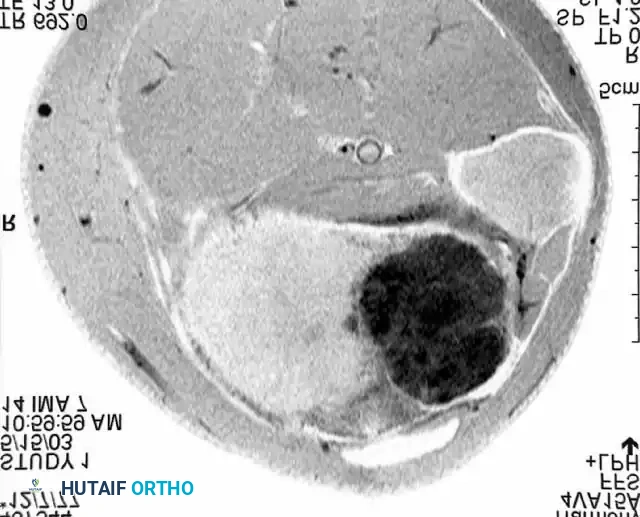
Advanced imaging, such as the MRI cross-section above, is mandatory for preoperative planning to delineate the tumor's relationship to neurovascular structures and compartmental boundaries.
Functional Outcomes and Energy Expenditure
The anatomical location of the tumor is the primary determinant of functional outcome.
* Upper Extremity: Resection of an upper extremity lesion with limb salvage—even requiring the sacrifice of major nerves—generally yields superior function compared to amputation and prosthetic fitting.
* Pelvis and Proximal Femur: Local reconstruction provides significantly better function than hemipelvectomy or hip disarticulation.
* Knee: Treatment must be highly individualized. Otis, Lane, and Kroll demonstrated that patients undergoing resection and prosthetic knee replacement exhibited higher self-selected walking velocities and more efficient gait (lower oxygen consumption) compared to transfemoral amputees. Transfemoral amputees often function at >50% of their maximal aerobic capacity during free walking, forcing reliance on anaerobic metabolism and drastically reducing endurance.
* Foot and Ankle: Large sarcomas in this region are frequently treated with below-knee amputation followed by prosthetic fitting, as the functional outcome of a modern dynamic-response prosthesis often exceeds that of a complex, stiff, and insensate salvaged foot.
Systemic Adjuvant and Neoadjuvant Therapy
The success of modern orthopaedic oncology relies heavily on systemic chemotherapy. The table below outlines the chemotherapeutic agents commonly utilized for bone and soft-tissue tumors, along with their primary side effects.
Chemotherapeutic Agents and Side Effects
- Alkylating Agents (Mustards):
- Cyclophosphamide: Myelosuppression (leukopenia), hemorrhagic cystitis, alopecia, nausea/vomiting.
- Ifosfamide: Hemorrhagic cystitis, myelosuppression, nephrotoxicity, neurotoxicity.
- Platinum Compounds:
- Cisplatin: Nephrotoxicity and ototoxicity (both cumulative and irreversible), severe nausea/vomiting, reversible peripheral neuropathy.
- Carboplatin: Myelosuppression, hepatotoxicity, nephrotoxicity.
- Antimetabolites:
- Methotrexate: Mucositis, myelosuppression, hepatotoxicity, pneumonitis.
- Topoisomerase Interactive Agents (Antitumor Antibiotics):
- Doxorubicin: Acute and chronic cardiotoxicity (dose-dependent cardiomyopathy), severe tissue necrosis upon extravasation, myelosuppression.
- Dactinomycin: Myelosuppression, diarrhea, tissue necrosis.
- Antimicrotubule Agents (Vinca Alkaloids):
- Vincristine: Irreversible peripheral neuropathy, seizures, tissue necrosis.
Surgical Margins: The Enneking Classification
When documenting an oncological procedure, the terms "resection" or "amputation" are meaningless without defining the surgical margin. The Enneking classification standardizes these margins into four distinct categories: Intralesional, Marginal, Wide, and Radical.
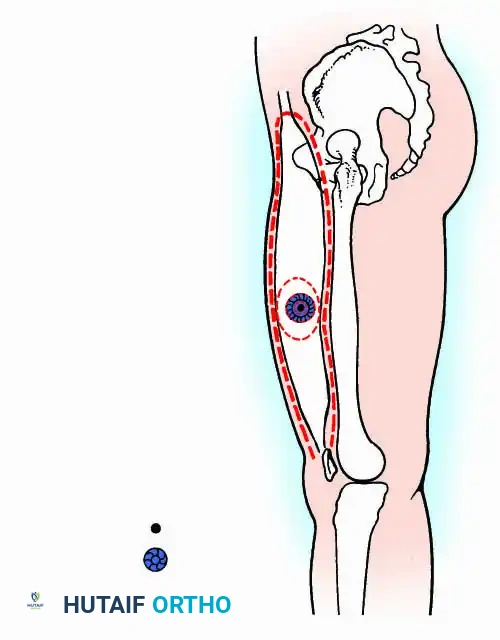
Fig. 19-6 Enneking classification of local procedures.
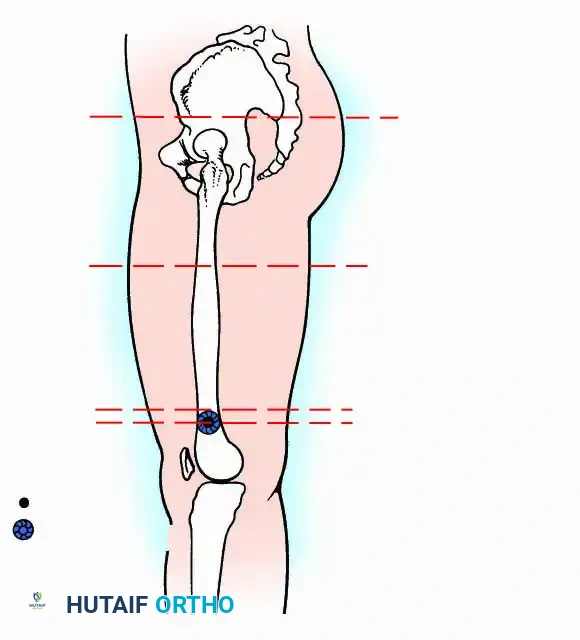
Fig. 19-7 Enneking classification of amputations.
1. Intralesional Margin
The plane of surgical dissection passes directly through the tumor. Often termed "debulking," this leaves macroscopic gross residual tumor.
* Indications: Symptomatic benign lesions where complete resection would sacrifice critical structures, or as a palliative measure in metastatic disease.
2. Marginal Margin
As tumors grow, they compress surrounding normal tissue, forming a "pseudocapsule." A marginal margin is achieved when the dissection plane passes directly through this pseudocapsule.
* Indications: Adequate for most benign lesions and select low-grade malignancies.
* Warning: In high-grade sarcomas, the pseudocapsule contains microscopic "satellite" lesions. A marginal resection here leaves microscopic disease, risking high local recurrence unless sterilized by adjuvant radiation.
3. Wide Margin
The plane of dissection is entirely within normal, healthy tissue. The tumor, its pseudocapsule, and the reactive zone are removed en bloc, surrounded by a continuous cuff of normal tissue.
* Indications: The gold standard and primary goal for the surgical treatment of high-grade malignancies.
4. Radical Margin
Achieved when the entire anatomical compartment containing the tumor is removed en bloc. For bone tumors, this means resection of the entire bone from joint to joint. For soft tissue, it requires excision of the entire muscle compartment from origin to insertion.
* Indications: Previously the standard for high-grade neoplasms, radical margins are now rarely required due to the efficacy of neoadjuvant therapies allowing for wide margins.
Understanding compartmental anatomy, as illustrated in this cross-section of the thigh, is paramount when planning wide or radical resections.
Surgical Techniques: Curettage and Adjuvants
Many benign and aggressive-benign bone tumors (e.g., Giant Cell Tumor of bone, aneurysmal bone cysts) are adequately treated with curettage. While curettage carries a higher local recurrence rate than en bloc resection, it preserves joint anatomy and provides vastly superior functional outcomes.
Principles of Simple Curettage
- Cortical Window: A large cortical window must be created over the lesion. Crucially, this window must be at least as large as the maximum diameter of the underlying lesion. A small window inevitably leads to retained tumor on the undersurface of the near cortex.
- Gross Removal: The bulk of the tumor is meticulously scooped out using various sizes of curettes.
- High-Speed Burr: The cavity must be expanded by 1 to 2 cm in all directions using a high-speed power burr. This step is absolutely mandatory to break down the bony ridges that harbor microscopic tumor cells.
- Irrigation: Copious pulsatile lavage is used to clear debris.
Extended Curettage
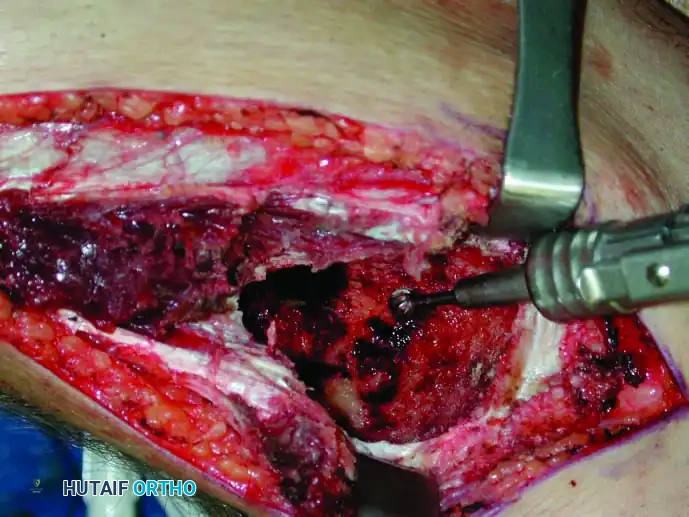
To further reduce recurrence rates in aggressive benign tumors, "extended" curettage employs chemical or physical adjuvants to induce necrosis of any remaining microscopic cells in the reactive zone.

Intraoperative use of thermal cautery (argon beam coagulation) to extend the zone of necrosis within the curetted bone cavity.
Common adjuvants include:
* Liquid Nitrogen (Cryotherapy): Induces cell death via intracellular ice crystal formation.
* Phenol: A chemical cauterizing agent (must be neutralized with alcohol).
* Thermal Cautery / Argon Beam: Delivers uniform surface coagulation.
* Polymethyl Methacrylate (PMMA): Bone cement generates an exothermic reaction (up to 70°C), causing thermal necrosis of adjacent cells.
Surgical Warning: When using liquid nitrogen, the surrounding soft tissues and neurovascular structures must be meticulously protected to prevent catastrophic iatrogenic frostbite and nerve palsy.
Cavity Reconstruction
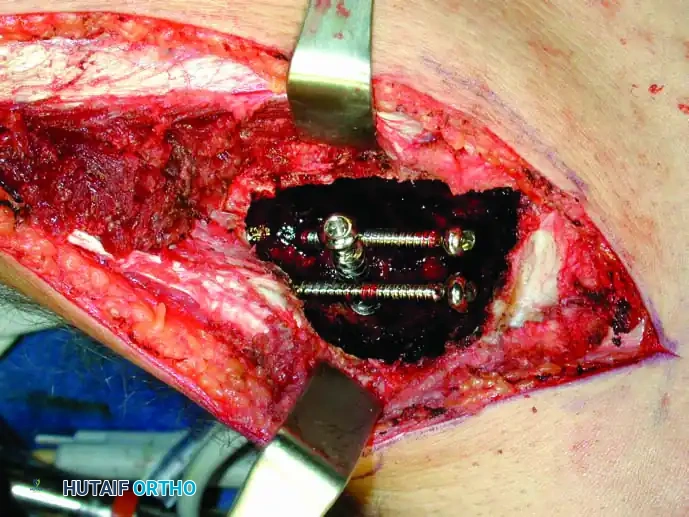
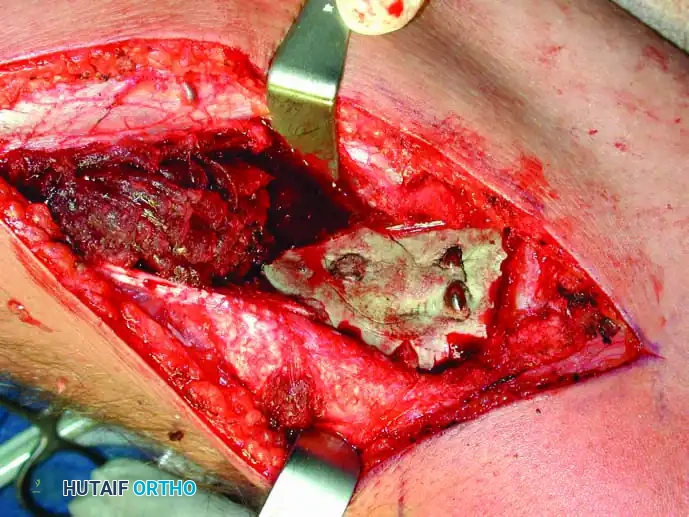
Following extended curettage, the structural integrity of the bone is compromised. The defect is typically reconstructed using PMMA cement, often augmented with internal fixation (screws or plates) to prevent pathological fracture.

Intraoperative view of a curetted cavity packed with PMMA cement and augmented with structural screws.


Postoperative radiographs demonstrating successful extended curettage, cementation, and screw augmentation of a distal tibial lesion.
Complex Reconstructions: Limb Salvage
When a wide resection of a bone sarcoma is performed, the resulting massive segmental defect requires complex reconstruction. Options include endoprosthetic replacement (megaprostheses), osteoarticular allografts, and Allograft-Prosthetic Composites (APCs).
Allograft-Prosthetic Composites (APCs)
APCs combine the biological advantages of a massive structural allograft (which allows for soft-tissue and tendon reattachment) with the immediate mechanical stability and articular longevity of a metallic endoprosthesis.
Preparation of the allograft on the back table. Precise measurements are critical to restore exact leg length and biomechanical offset.
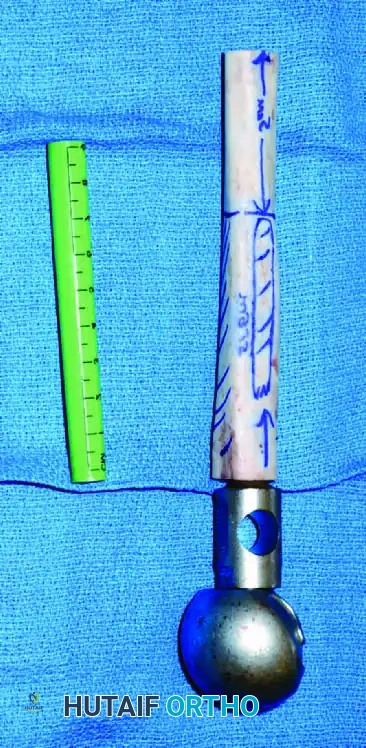
The Allograft-Prosthetic Composite (APC) assembled and ready for implantation into the proximal femur.
Intraoperative insertion and plating of the APC at the host-graft junction.
The durability of these reconstructions is highly dependent on anatomical location. Proximal femoral reconstructions generally outlast distal femoral reconstructions, which in turn outlast proximal tibial reconstructions. A successful arthrodesis is the most durable long-term option, though it sacrifices joint mobility.
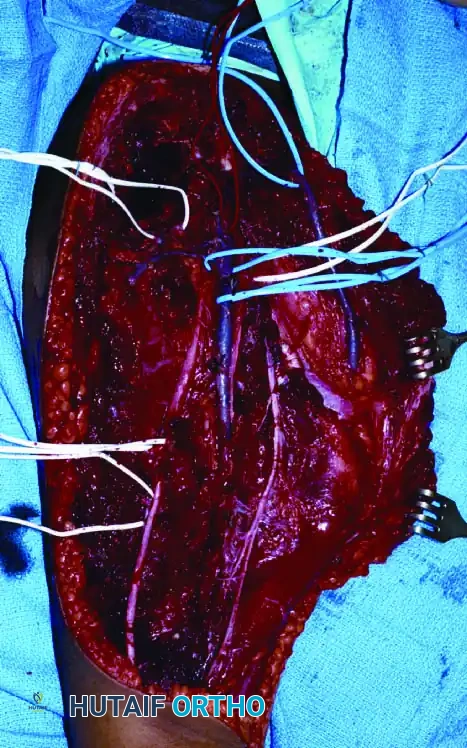
Careful soft-tissue handling and meticulous hemostasis are required during the exposure and resection phases to ensure flap viability.

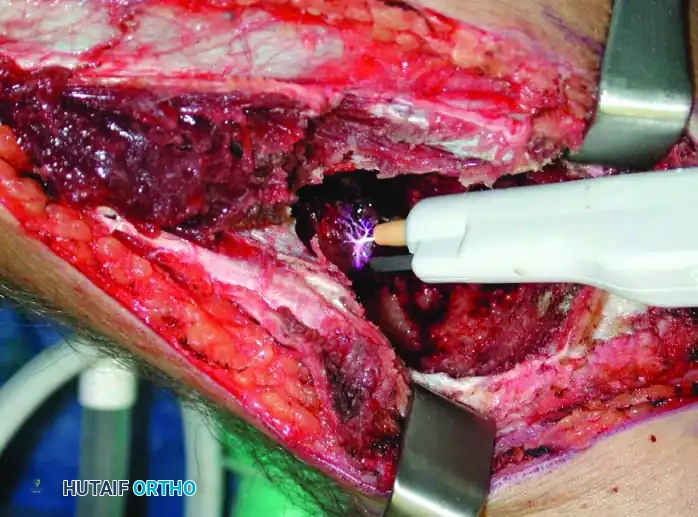
Intraoperative evaluation of the neurovascular bundle, which must be carefully mobilized and protected during wide resection.
Extensive soft-tissue mobilization is often required to achieve adequate coverage over massive endoprostheses.

Final soft-tissue closure over a reconstructed limb. Flap necrosis and wound dehiscence are major risks that require vigilant postoperative care.
Upper Extremity Reconstruction
Limb salvage in the upper extremity prioritizes the preservation of hand function. Resections of the proximal humerus or elbow joint can be reconstructed with modular endoprostheses.

Postoperative radiograph demonstrating a complex modular endoprosthetic reconstruction of the humerus and elbow joint following wide resection.
Complications and Postoperative Management
Limb salvage surgery is inherently associated with greater perioperative and long-term morbidity compared to amputation. The procedures are extensive, carrying elevated risks for:
* Early Complications: Deep infection, wound dehiscence, flap necrosis, massive blood loss, and deep venous thrombosis.
* Late Complications: Aseptic loosening, periprosthetic fracture, nonunion at the graft-host junction, allograft fracture, leg-length discrepancy, and late hematogenous infection.
Patients with salvaged limbs are statistically much more likely to require multiple revision surgeries over their lifetime. Following initially successful limb salvage, up to one-third of long-term survivors may ultimately require a secondary amputation due to intractable infection or local recurrence.
Postoperative Rehabilitation
Rehabilitation protocols must be strictly tailored to the type of reconstruction.
* Cemented Endoprostheses: Generally allow for immediate weight-bearing as tolerated.
* Allografts and APCs: Require protected weight-bearing (often 3 to 6 months) until radiographic evidence of bridging callus is observed at the host-graft osteosynthesis site.
* Soft Tissue: Range of motion is often restricted initially to allow for the healing of muscle transfers and capsular reconstructions.
Routine oncological surveillance, including local imaging (MRI) and systemic staging (Chest CT), is mandatory to monitor for local recurrence and pulmonary metastasis. The ultimate success of orthopaedic oncology relies on this meticulous, multidisciplinary continuum of care.
📚 Medical References
- orthopaedic oncology patients, Instr Course Lect 48:603, 1999.
- Levine SE, Dormans JP, Meyer JS, et al: Langerhans’ cell histiocytosis of the spine in children, Clin Orthop Relat Res 323:288, 1996.
- Lewis MM: Bone tumor surgery: limb-sparing technique , Philadelphia, 1988, JB Lippincott. Lewis MM, Chekofsky KM: Proximal femur replacement for neoplastic disease, Clin Orthop Relat Res 171:72, 1982.
- Lietman SA, Tomford WW, Gebhardt MC, et al: Complications of irradiated allografts in orthopaedic tumor surgery, Clin Orthop Relat Res 375:214, 2000.
- Lin PP, Schupak KD, Boland PJ, et al: Pathologic femoral fracture after periosteal excision and radiation for the treatment of soft tissue sarcoma, Cancer 82:2356, 1998.
- Linberg BE: Interscapulothoracic resection for malignant tumors of the shoulder joint region, J Bone Joint Surg 10:344, 1928.
- Localio SA, Francis KC, Rossano PG: Abdominosacral resection of sacrococcygeal
You Might Also Like