Tumorous Conditions of the Hand: Surgical Excision Guide
Key Takeaway
Tumorous conditions of the hand, such as ganglion cysts, mucous cysts, and epidermoid inclusion cysts, require precise surgical management to minimize recurrence and preserve neurovascular function. This comprehensive guide details evidence-based operative techniques, including open and arthroscopic dorsal ganglion excision, volar ganglion resection, and osteophyte debridement for mucous cysts. Mastery of regional anatomy and meticulous capsular dissection are paramount for optimal postoperative outcomes in hand oncology.
TUMOROUS CONDITIONS OF THE HAND AND WRIST
Tumorous conditions of the hand encompass a broad spectrum of benign neoplastic and non-neoplastic soft-tissue and osseous lesions. Because the hand is a highly complex anatomical structure with minimal subcutaneous tissue, even small space-occupying lesions can produce profound functional impairment, neurovascular compromise, and significant cosmetic concern. The orthopedic surgeon must approach these lesions with a thorough understanding of regional anatomy, biomechanics, and evidence-based surgical oncology principles.
GANGLION CYSTS
Ganglions represent the most common cause of focal masses in the hand and wrist. These mucin-filled cysts characteristically arise from the synovium of joints, tendon sheaths, or directly from the substance of tendons. When originating from the flexor tendon sheath, they may cause mechanical impingement, leading to snapping or trigger finger phenomena.
Although the precise etiology of ganglion cysts remains a subject of debate, a history of acute trauma or recurrent chronic micro-trauma—often occupational—is a common denominator. The pathogenesis is widely believed to involve a one-way valve mechanism at the capsular level, allowing synovial fluid to extravasate into the periarticular tissues where it concentrates into a thick, highly viscous, hyaluronic acid-rich mucin.
Clinical Presentation and Anatomical Distribution
The anatomical distribution of ganglion cysts follows a predictable pattern:
1. Dorsal Wrist Ganglions (Most Common): The most frequent site of origin is the dorsal scapholunate (SL) interosseous ligament. These cysts typically present as firm, smooth, fluctuant, and round masses palpable between the second and fourth extensor tendon compartments. Cysts extending proximally along the extensor tendons may feel less firm, multilocular, and irregular, yet they consistently contain the characteristic slightly yellow, gelatinous, stringy fluid.
2. Volar Wrist Ganglions (Second Most Common): These typically arise from the radiocarpal or scaphotrapezial joint and present volarly, just radial to the flexor carpi radialis (FCR) tendon. They are intimately associated with the radial artery.
3. Flexor Tendon Sheath Ganglions: The most common site is at the level of the metacarpophalangeal (MCP) joint flexor skin crease (A1 pulley region). These masses are small, round, hard, and often tender to firm pressure.
Clinical Pearl: Ganglions are frequently associated with a deep, aching pain or a subjective feeling of grip weakness. Mild discomfort may precede the clinical appearance of a palpable mass, often due to occult capsular distension or compression of the posterior interosseous nerve (PIN).
Westbrook et al. evaluated the primary motivations for patients seeking medical intervention for ganglion cysts:
* 38% were concerned about cosmetic appearance.
* 28% harbored fears of malignancy.
* 26% sought relief from pain.
* 8% reported abnormal sensation or mechanical dysfunction.
Atypical and Intraosseous Ganglions
While most ganglions are superficial, they can occasionally present within the carpal bones or deep within the palmar spaces, leading to secondary compressive neuropathies.

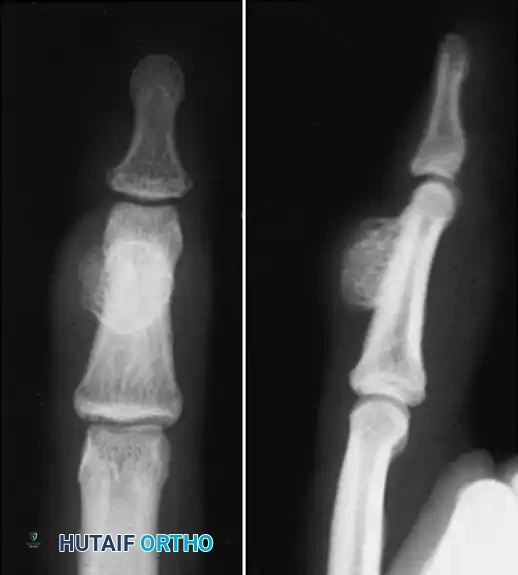
Anteroposterior radiograph demonstrating erosion at the base of the fourth metacarpal and distal capitate.

Sagittal section view revealing an intraarticular ganglion bridging the carpometacarpal joint with extensions into the substance of the capitate and fourth metacarpal.
Ganglions seldom occur deep in the palm. When they do, their presence is often heralded not by an external mass, but by secondary neurological changes caused by mass effect. For instance, cysts arising in or distal to Guyon's canal can cause profound motor neuropathy.
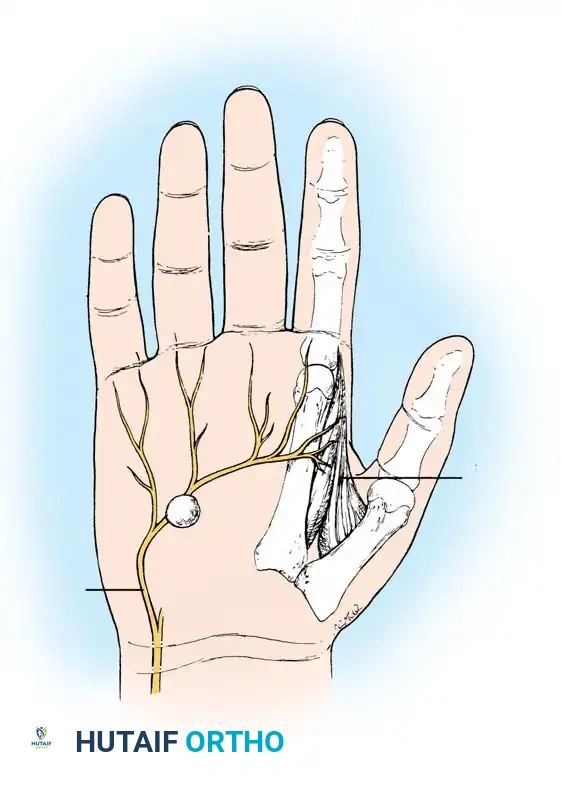
Ganglion in the palm producing pressure on the deep branch of the ulnar nerve, causing severe atrophy of the first dorsal interosseous muscle.
Non-Operative Management and Outcomes
Ganglions occasionally resolve spontaneously, but recurrence is common when treated by simple rupture or aspiration. Historically, dorsal cysts were ruptured by digital pressure or by striking the flexed wrist with a heavy object (the "Bible bump" treatment). We strongly condemn and do not use this archaic technique.
Nelson et al. reported the following cure rates based on treatment modality:
* 94% cure rate with formal surgical excision under general anesthesia or axillary block.
* 84% cure rate with excision under local anesthesia and tourniquet.
* 65% cure rate with closed rupture or needle aspiration combined with corticosteroid injection.
For flexor tendon sheath ganglions, multiple punctures with an 18-gauge needle under local anesthesia frequently yield a high cure rate. Conversely, volar wrist ganglions should never be treated with blind needle rupture due to the intimate and often intertwined relationship with the radial artery.
SURGICAL TECHNIQUES FOR GANGLION CYSTS
Surgical excision remains the gold standard for symptomatic or recurrent ganglions. The critical principle of ganglion surgery is the complete excision of the cyst complex, including its stalk and a generous margin of the involved joint capsule, without attempting to close the resulting capsular defect.
TECHNIQUE 74-1: Open Excision of a Dorsal Wrist Ganglion
Surgical Warning: The dorsal cutaneous branch of the radial nerve and the dorsal branch of the ulnar nerve must be meticulously identified and protected during the superficial dissection to prevent painful postoperative neuromas.
- Positioning & Exposure: Place the patient supine with the arm on a hand table. Apply a well-padded pneumatic tourniquet.
- Incision: Make a transverse incision over the proximal third of the ganglion, following Langer’s lines. Carry the incision through the dermis only. Spread the underlying subcutaneous tissues longitudinally using blunt dissection and place retractors.
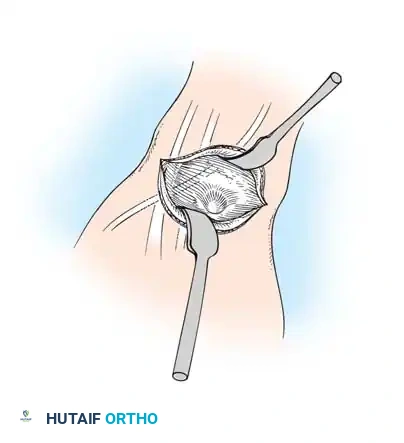
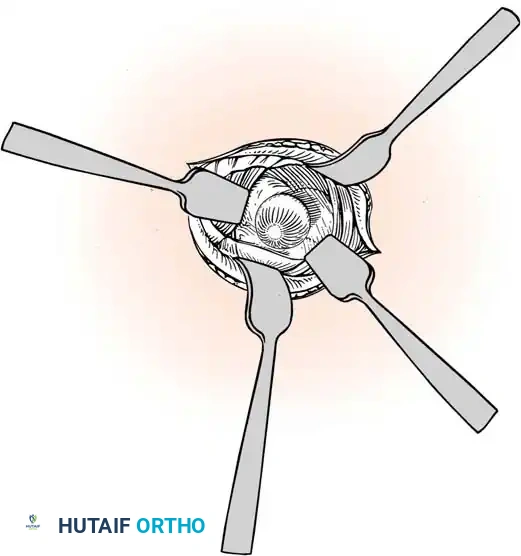
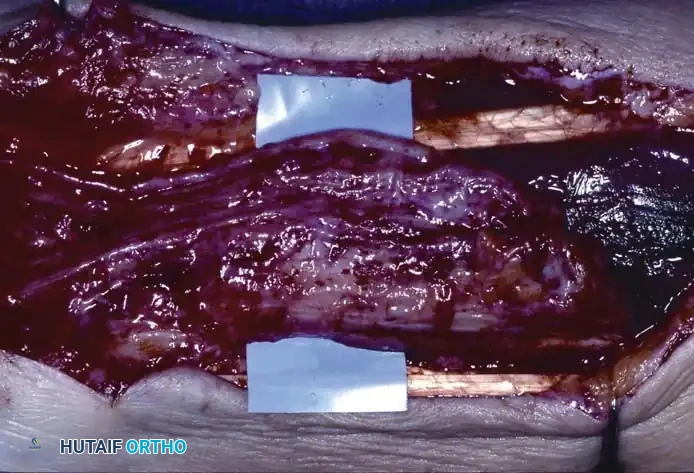
Initial exposure of the dorsal ganglion, identifying the extensor retinaculum.
- Retinacular Incision: Incise the extensor retinaculum directly over the ganglion. Isolate the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) tendons, retracting them radially.
- Tendon Retraction: Dissect the extensor digitorum communis (EDC) tendons to the index finger and retract them, along with the remaining extensor tendons, ulnarward.
Retraction of the extensor pollicis longus (EPL) and isolation of the cyst.
- Deep Dissection: Identify and protect the extensor pollicis longus (EPL) in the proximal portion of the surgical field.
Careful separation of the ganglion from the surrounding extensor tendon sheaths.
- Stalk Excision: Using a combination of sharp and blunt dissection, mobilize the ganglion in its entirety. Trace the stalk down to its capsular origin at the dorsal scapholunate ligament. Excise the cyst along with a 1-cm margin of the dorsal capsule. Do not excise the substance of the scapholunate interosseous ligament itself, as this will cause carpal instability.
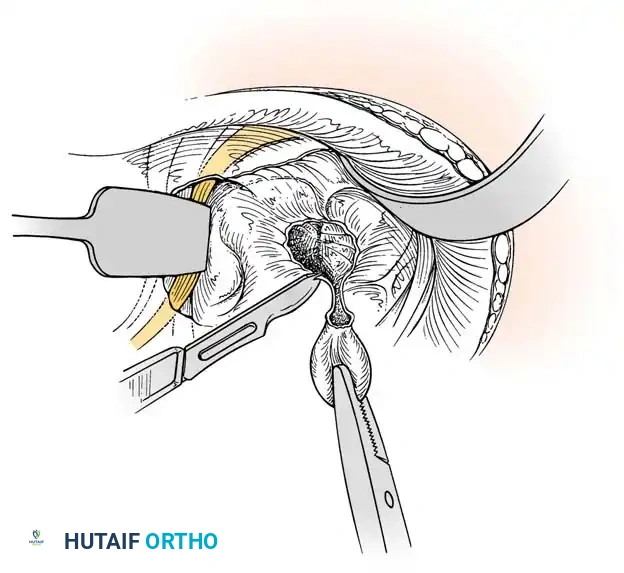
Excision of the ganglion stalk along with a generous margin of the dorsal joint capsule.
- Neurectomy: Identify the terminal sensory fibers of the posterior interosseous nerve (PIN) at the floor of the fourth compartment. Divide the nerve and gently cauterize the proximal end to denervate the dorsal capsule and reduce postoperative pain.
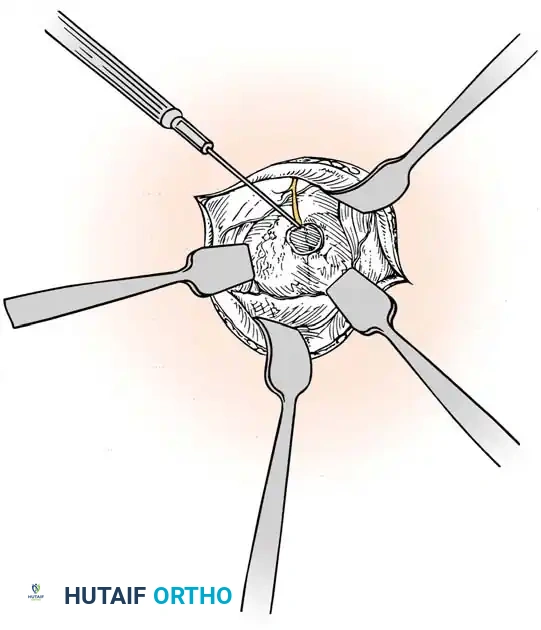
Cauterization of the capsular margins and the terminal branches of the posterior interosseous nerve.
- Closure: Deflate the tourniquet, irrigate the wound copiously, and obtain meticulous hemostasis. Do not close the joint capsule. Close the skin with a running, subcuticular 4-0 nylon or Monocryl suture. Apply a sterile compressive dressing and a volar splint.
POSTOPERATIVE CARE: The wrist is splinted in mild extension for 2 weeks. Sutures are removed at 10 to 14 days, and active range-of-motion (ROM) exercises are initiated immediately thereafter to prevent extensor tendon adhesions.
TECHNIQUE 74-2: Excision of a Volar Wrist Ganglion
Surgical Warning: The radial artery frequently arborizes around or directly through the lobules of a volar ganglion. Meticulous dissection under loupe magnification is mandatory.
- Preoperative Assessment: Perform a modified Allen test preoperatively to confirm the integrity of the ulnar collateral circulation to the hand.
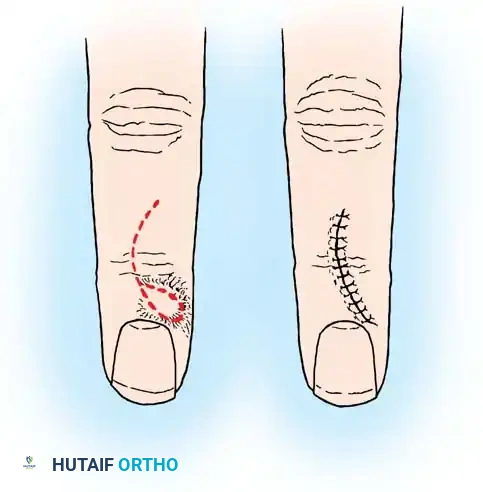
- Incision: Under tourniquet control, make a longitudinal or lazy-S incision centered over the ganglion, typically situated just radial to the FCR tendon. Carefully avoid injury to the palmar cutaneous branch of the median nerve, which lies ulnar to the FCR.
- Arterial Dissection: Dissect the radial artery carefully under loupe magnification. Retract the artery radially using vessel loops.
- Cyst Mobilization: Dissect the ganglion cyst using blunt and sharp dissection in a proximal-to-distal direction. Carry the dissection down along the stalk to its origin, which is usually at the radiocarpal or scaphotrapezial joint.
- Capsular Excision: Excise the origin with a small portion of the surrounding volar capsule. Cauterize the capsular margins.
- Hemostasis & Closure: Deflate the tourniquet to inspect the integrity of the radial artery. Control any bleeding with bipolar electrocautery. Irrigate and close the skin with a running 4-0 subcuticular suture. Apply a volar splint.
TECHNIQUE 74-3: Arthroscopic Resection of a Dorsal Wrist Ganglion
Arthroscopic resection has gained popularity due to decreased postoperative stiffness and smaller incisions. Luchetti et al. and Rizzo et al. reported excellent outcomes with minimal recurrences (approx. 5%) at long-term follow-up.
- Setup: Apply longitudinal distraction using finger traps attached to the index, long, and ring fingers with 3 to 4 kg of countertraction at the upper arm.
- Anesthesia: Utilize an axillary block or general anesthesia with a pneumatic tourniquet.
- Portals: Establish standard 3-4 and 4-5 radiocarpal portals. Insert a 1.9-mm or 2.7-mm arthroscope into the 3-4 portal. If exposure is inadequate, utilize the 1-2 or 6R portals.
- Identification: Locate the scapholunate ligament. Direct the arthroscope dorsally to visualize the ganglion stalk or the capsular defect.
- Resection: Introduce a probe through the 4-5 portal to palpate the dorsal capsule. Introduce a 2.0-mm or 2.9-mm full-radius shaver or end-cutting resector. Excise a 1-cm diameter area of the dorsal capsule and the ganglion stalk.
- Safety Check: Stop the capsular resection as soon as the extensor tendons are visualized to prevent iatrogenic tendon injury. Avoid damaging the intrinsic scapholunate ligament.
- Closure: Convert to an open procedure if complete arthroscopic resection is doubtful. Otherwise, close the portals with Steri-Strips or a single suture. Apply a palmar wrist splint.
POSTOPERATIVE CARE: The splint is removed after 1 week. Physiotherapy is continued for 2 weeks. Strenuous work is avoided for at least 3 weeks.
EPIDERMOID CYST (INCLUSION CYST)
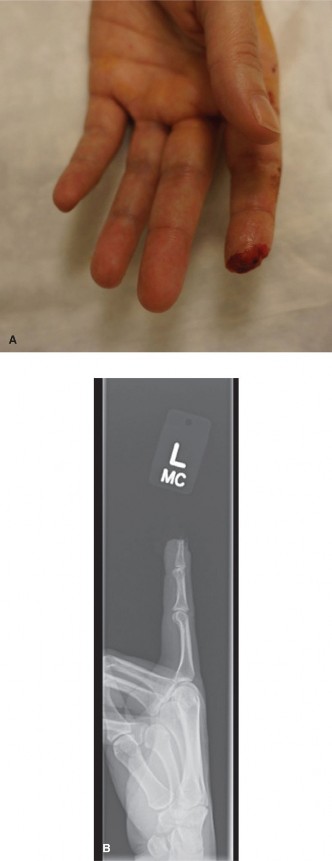
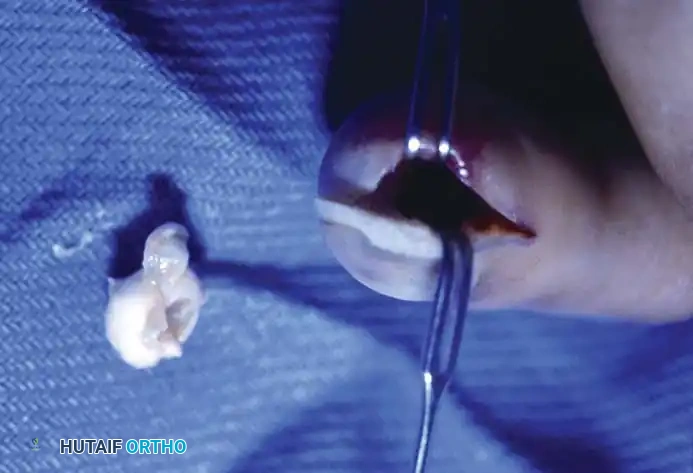
Epidermoid inclusion cysts develop from the traumatic implantation of epithelial cells into the deep subcutaneous tissues or bone. The clinical history almost universally involves a penetrating wound (e.g., a needle prick, thorn, or crush injury) to the palm or fingertip several months or even years prior to presentation.
Clinically, the patient develops a hard, rubbery, non-tender subcutaneous mass. The distal phalanx is the most common osseous site, where the expanding cyst can cause pressure erosion of the bone.

Clinical appearance of an epidermoid inclusion cyst on the index finger following a remote puncture wound.









You Might Also Like