Surgical Management of Subungual Tumors & Exostoses
Key Takeaway
Subungual and periungual lesions, including fibromas, exostoses, and glomus tumors, present unique diagnostic and surgical challenges. Accurate diagnosis relies on clinical suspicion, advanced imaging, and recognizing systemic associations like tuberous sclerosis. Surgical management requires meticulous nail bed preservation, precise tumor excision, and strategic flap design to eradicate the pathology while minimizing postoperative nail dystrophy and ensuring optimal functional recovery.
INTRODUCTION TO SUBUNGUAL PATHOLOGY
The subungual space is a unique anatomic and biomechanical environment. The perionychium—comprising the nail plate, nail bed (sterile and germinal matrices), and surrounding soft tissue folds—serves critical functions in tactile sensation, thermoregulation, and protection of the distal phalanx. Pathologic entities arising in this confined space, such as subungual fibromas, subungual exostoses, and glomus tumors, often present with disproportionate pain and nail dystrophy due to the rigid boundaries of the nail plate dorsally and the distal phalanx volarly.
Diagnosing these lesions preoperatively can be exceptionally challenging. Patients frequently present with a history of long-standing symptoms, having consulted multiple physicians without resolution. Localized tenderness beneath a specific portion of the nail plate, subtle color changes, and a highly frustrated patient should immediately raise the clinical index of suspicion for a subungual neoplasm.
SUBUNGUAL AND PERIUNGUAL FIBROMAS
Subungual and periungual fibromas are benign fibrous tissue tumors that emerge from the nail matrix or the surrounding nail folds. While isolated fibromas can occur spontaneously, their presence is highly indicative of underlying systemic genetic disorders.
Clinical Presentation and Systemic Associations
A high index of suspicion for this rare tumor is warranted, particularly in patients with Tuberous Sclerosis Complex (TSC). Up to 80% of patients with tuberous sclerosis will develop ungual fibromas, clinically referred to as Koenen tumors. These lesions typically manifest in post-pubertal patients and are more common on the toes than the fingers.
If the mass is readily visible, protruding from the proximal nail fold or extending distally beneath the nail plate, the diagnosis is straightforward. However, smaller, entirely subungual lesions may only present as a localized area of exquisite tenderness or as a longitudinal groove in the nail plate due to compression of the germinal matrix.
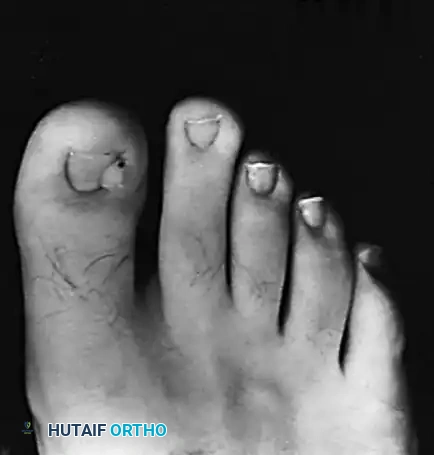
Clinical presentation of multiple periungual fibromas (Koenen tumors) characteristic of tuberous sclerosis.
Clinical Pearl: Always perform a comprehensive dermatologic and neurologic screening in patients presenting with multiple periungual fibromas to rule out Tuberous Sclerosis. Look for ash-leaf spots, facial angiofibromas, and periungual lesions on other digits.
Surgical Technique 87-13: Excision of Subungual Fibroma
Surgical excision is the definitive treatment for symptomatic fibromas. The primary goal is complete tumor eradication while minimizing iatrogenic damage to the germinal matrix, which could result in permanent nail dystrophy.
Preparation and Positioning:
1. Position the patient supine. Administer a digital block using 1% plain lidocaine or bupivacaine.
2. Apply a digital tourniquet (e.g., a sterile Penrose drain or rolled glove) at the base of the digit to ensure a bloodless surgical field.
3. Magnification and high-intensity lighting are absolutely critical for locating small, pearly-whitish changes in color compared with the surrounding normal matrix.
Surgical Steps:
1. Nail Plate Removal: If the mass is located entirely beneath the nail, carefully avulse and remove the portion of the nail plate overlying the area of tenderness.
2. Tumor Identification: Under loupe magnification, identify the fibroma. It typically appears as a firm, pearly-white nodule distinct from the pink, vascularized sterile matrix.
3. Excision: Excise the tumor sharply down to the periosteum of the distal phalanx. It is imperative to include a small, 1- to 2-mm margin of what appears to be normal matrix to prevent recurrence.
4. Tissue Assessment: Section the excised tissue on the back table. A subungual fibroma characteristically has a dense, "gritty" feel when sectioned with a scalpel.
5. Pathology: Send all specimens to surgical pathology with the suspected diagnosis to confirm the benign nature of the fibrous proliferation.
Postoperative Care:
* Place a non-adherent dressing (e.g., Adaptic or Xeroform) directly beneath the nail fold and over the exposed matrix defect.
* Allow the defect to granulate and heal by secondary intention.
* The postoperative care mirrors that of an incomplete matrixectomy. Patients must be counseled preoperatively that permanent deformity of the nail (such as longitudinal ridging or splitting) may occur, though it is generally less severe than the deformity seen after the removal of a large subungual exostosis.
SUBUNGUAL EXOSTOSIS
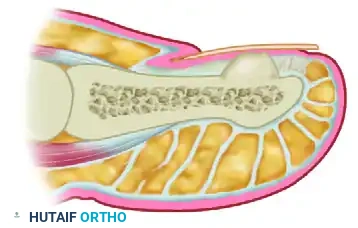
Subungual exostosis is a benign osteocartilaginous tumor that typically arises from the dorsal aspect of the distal phalanx, most commonly affecting the hallux. Unlike true osteochondromas, these lesions do not have a medullary cavity continuous with the underlying bone and are often considered reactive rather than purely neoplastic.
Biomechanics and Presentation
The exostosis grows dorsally, elevating the nail bed and nail plate. This creates a painful pinch mechanism between the rigid shoe upper and the expanding bony mass. Left untreated, the exostosis can ulcerate through the nail bed, leading to secondary bacterial infection.
Surgical Technique 87-11: Minimalist Approach (Lokiec et al.)
For smaller, well-localized exostoses, a tissue-sparing approach can be utilized to preserve the majority of the nail plate.

A narrow strip of the nail over the medial side of the exostosis is removed, and the nail is dislodged to expose the underlying bony mass.

A small osteotome, positioned parallel to the longitudinal axis of the distal phalanx, is used to resect the exostosis flush with the host bone in one piece.

The preserved nail plate is relocated to cover the raw phalangeal bone and stitched securely in place, acting as a biologic dressing.
Surgical Technique 87-12: Formal Excision (Walling)
For larger lesions or those that have severely distorted the nail bed, a formal exposure with complete nail avulsion is required.
The toenail is completely avulsed using a Freer elevator and straight hemostat to fully expose the exostosis and the distorted nail bed.
A precise longitudinal incision is made directly through the nail bed over the prominence of the exostosis, strictly avoiding injury to the proximal nail matrix.
The nail bed is carefully reflected medially and laterally using fine skin hooks or stay sutures to expose the osteocartilaginous cap.

The exostosis is excised at its base with wide margins using a rongeur or osteotome. The nail bed is then meticulously repaired using 6-0 absorbable sutures (e.g., chromic gut or Vicryl Rapide).
Postoperative Care for Exostosis Excision:
* Nonadhesive dressings are applied and changed every 3 days for the first 3 weeks.
* Patients are placed in a rigid postoperative shoe and allowed to bear weight as tolerated on the heel and lateral border of the foot.
* At 3 weeks, sutures are removed (if non-absorbable were used for the nail plate), and a gradual return to normal-width shoes is permitted as edema subsides.
GLOMUS TUMOR
The glomus tumor is an enigmatic, exquisitely painful neoplasm that represents a benign hamartomatous proliferation of the normal capsular-neural glomus apparatus (the Sucquet-Hoyer canal). These neuromyoarterial bodies are highly concentrated in the subungual reticular dermis and are responsible for thermoregulation via arteriovenous shunting.
Clinical Diagnosis and Imaging
Patients classically present with a triad of symptoms:
1. Severe, paroxysmal pain
2. Point tenderness (often localized using Love’s pin test)
3. Cold hypersensitivity
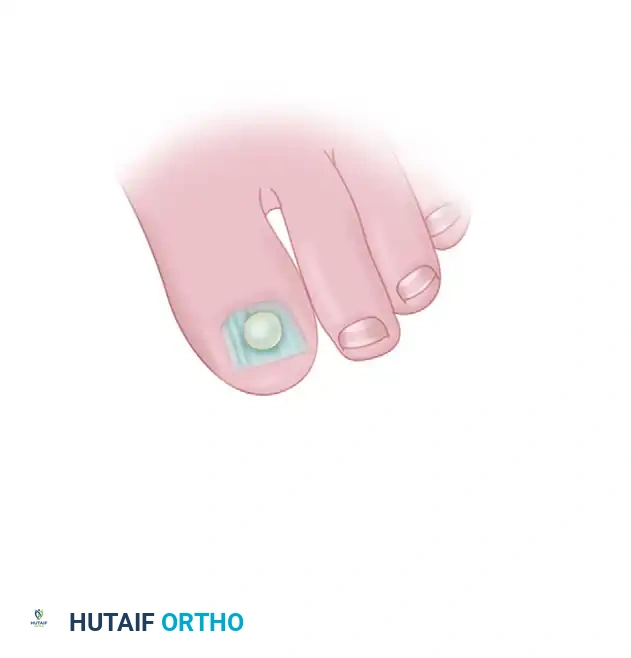
Except for a faint bluish or reddish-blue hue visible through the translucent nail plate, the nail itself may appear entirely normal. The pathology lies entirely within the mass seen through the nail plate.
Surgical Warning: Because the nail plate often appears normal, glomus tumors are frequently misdiagnosed as chronic paronychia, neuromas, or psychosomatic pain. Advanced imaging is highly recommended prior to surgical exploration.
High-resolution Magnetic Resonance Imaging (MRI) is the gold standard for preoperative localization. On T2-weighted MRI, a glomus tumor typically appears as a hyperintense, well-demarcated lesion.

T2-weighted MRI scan demonstrating a hyperintense glomus tumor located on the lateral aspect of the distal phalanx.
Surgical Technique 87-14: Flap Exposure (Horst and Nunley)
Historically, treatment involved removing the overlying nail plate and excising the involved matrix. While effective for tumor removal, this often resulted in unpredictable and severe nail deformities.
Horst and Nunley described an advanced, tissue-sparing technique utilizing a full-thickness vascular skin flap. This approach provides excellent exposure of the tumor while completely preserving the nail plate and the delicate nail matrix. In their series, this technique yielded complete pain relief, zero wound healing complications, and no recurrences.

Intraoperative exposure of the glomus tumor utilizing a matrix-sparing approach.
Step-by-Step Flap Technique:
1. Incision Design: Make an inverted L-shaped incision around the nail. The short leg of the "L" should run parallel to, and 5 mm distal to, the distal edge of the nail (hyponychium). The long leg of the "L" should run 5 mm medial or lateral to the nail fold, extending proximally past the nail matrix, usually reaching the level of the distal interphalangeal (DIP) joint.
2. Flap Elevation: Create a full-thickness flap down to the bone. Sharply and meticulously elevate this flap off the distal phalanx. It is critical to elevate the flap without penetrating or injuring the overlying nail matrix.
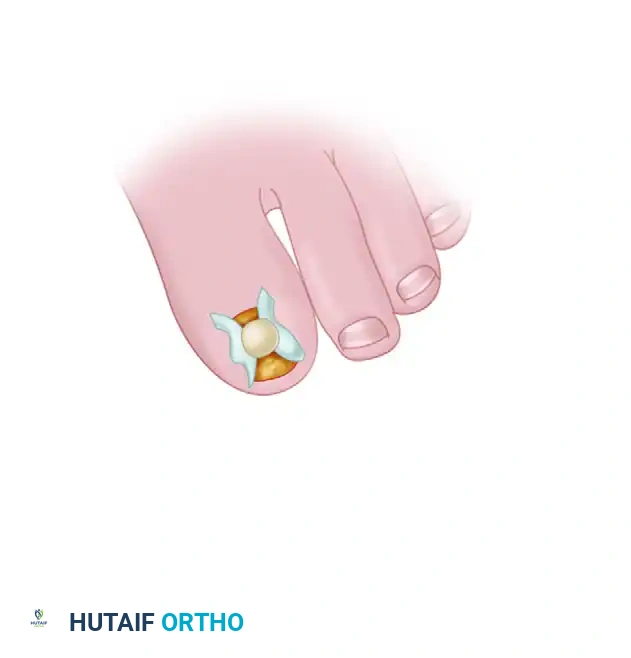
3. Tumor Identification: Reflect the skin and matrix flap dorsally and inspect the deep (volar) surface of the flap. The glomus tumor is usually obvious within the sub-matrix tissue, appearing as a ball-shaped or egg-shaped, opaque, semi-elastic, bluish-red structure.
4. Bone Assessment: Occasionally, chronic pulsatile pressure from the tumor causes a smooth, scalloped erosion into the dorsal cortex of the distal phalanx. Inspect the bone to ensure no tumor tissue remains in the bony crater.
5. Excision: The tumor is usually well-encapsulated. Excise it completely using a small #15 blade or a fine curette. Ensure the capsule is not breached to prevent seeding and recurrence.
6. Hemostasis and Closure: Release the digital tourniquet prior to closure. Control any reactive bleeding meticulously with bipolar electrocautery to prevent postoperative subungual hematoma, which can cause severe pain and compromise the flap. Close the wound in a single layer using interrupted nylon sutures.
Postoperative Care for Glomus Tumors:
* Apply a bulky, non-compressive soft dressing.
* The patient is provided a hard-soled postoperative shoe to protect the digit until the wound is fully healed.
* Suture removal is performed at 10 to 14 days.
* Patients can generally transition back to regular, comfortable footwear at 4 to 6 weeks postoperatively, depending on the resolution of soft tissue edema.
SUMMARY
The surgical management of subungual tumors requires a profound understanding of perionychial anatomy. Whether addressing a tuberous sclerosis-associated fibroma, a mechanically disruptive subungual exostosis, or an exquisitely painful glomus tumor, the surgeon must balance the complete eradication of the pathology with the meticulous preservation of the germinal and sterile matrices. Utilizing advanced techniques, such as the Horst and Nunley full-thickness flap, allows modern orthopedic surgeons to achieve excellent oncologic and functional outcomes while minimizing the risk of permanent nail dystrophy.
You Might Also Like
