Comprehensive Surgical Management of Benign Soft-Tissue Tumors and Tumor-Like Lesions
Key Takeaway
Benign soft-tissue tumors and tumor-like lesions encompass a diverse group of pathologies, including lipomas, peripheral nerve sheath tumors, and synovial proliferative disorders. Accurate diagnosis relies heavily on advanced MRI modalities to differentiate these from malignant sarcomas. Surgical management typically involves marginal excision or meticulous enucleation, prioritizing the preservation of adjacent neurovascular structures while minimizing recurrence risk through complete lesional resection.
INTRODUCTION TO BENIGN SOFT-TISSUE TUMORS
The diagnosis and management of benign soft-tissue tumors and tumor-like lesions represent a fundamental pillar of operative orthopaedics and musculoskeletal oncology. While these lesions lack metastatic potential, their local behavior can range from indolent and asymptomatic to highly aggressive, causing significant neurovascular compromise, joint destruction, and functional impairment.
For the orthopaedic surgeon, the paramount challenge lies in accurately differentiating these benign entities from soft-tissue sarcomas prior to any surgical intervention. A meticulously planned approach—incorporating advanced magnetic resonance imaging (MRI), precise histopathological interpretation, and anatomically sound surgical execution—is mandatory. This masterclass delineates the evidence-based evaluation, biomechanical considerations, and step-by-step surgical management of the most frequently encountered benign soft-tissue tumors.
Clinical Pearl: Never assume a soft-tissue mass is benign based solely on clinical palpation. "Oops procedures" (unplanned excisions of unrecognized sarcomas) drastically increase local recurrence rates and patient morbidity. Always obtain an MRI with and without contrast prior to biopsy or excision of any deep, enlarging, or symptomatic mass.
ADIPOCYTIC TUMORS: LIPOMAS AND VARIANTS
Pathophysiology and Classification
Lipomas are the most ubiquitous benign tumors of mesenchymal origin, predominantly affecting middle-aged adults, with a slight predilection for females. While the vast majority develop within the subcutaneous tissues, deep-seated variants can involve subfascial spaces, intermuscular septa, or intramuscular planes.
Histologically, a classic lipoma is a well-encapsulated nodule composed of mature adipocytes devoid of nuclear atypia. However, several distinct variants exist, each with unique clinical implications:
* Angiolipoma: Features a prominent vascular network; often presents as multiple, painful subcutaneous nodules.
* Intramuscular Lipoma: Infiltrates between skeletal muscle fibers. Its infiltrative appearance on imaging can mimic malignancy, though it remains biologically benign.
* Hibernoma: A rare variant composed of fetal brown fat. It appears highly vascular, lobulated, and can grow to massive proportions.
* Lipoma Arborescens: A rare intra-articular condition characterized by lipomatous infiltration of the synovial membrane, typically affecting the suprapatellar pouch of the knee.
* Dercum Disease (Adiposis Dolorosa): Characterized by multiple, exquisitely painful fatty infiltrations, often refractory to standard surgical management.
Clinical Evaluation and Advanced Imaging
Clinically, superficial lipomas present as soft, mobile, painless, and circumscribed masses. Deep or intramuscular lipomas may present as firm masses due to the overlying fascial tension and muscle contraction.
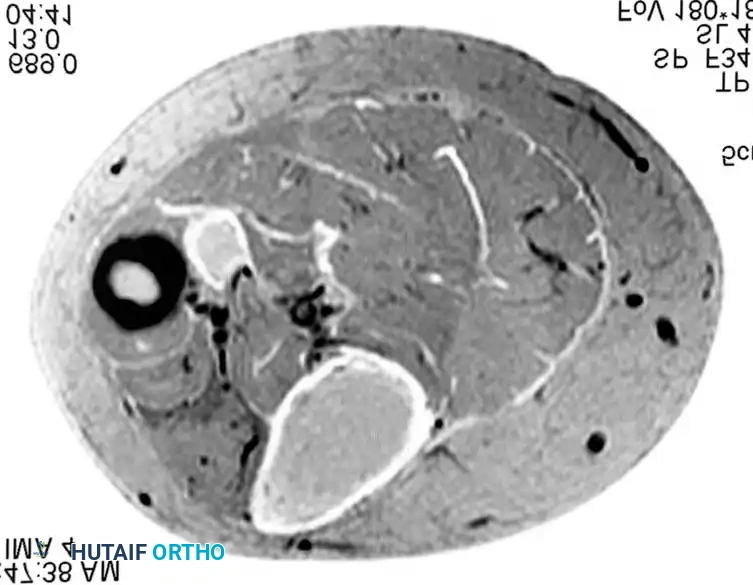
MRI is the gold standard for diagnosis. Lipomas exhibit signal characteristics identical to subcutaneous fat: uniformly hyperintense (bright) on T1-weighted sequences and completely suppressed (dark) on fat-suppressed or STIR sequences.
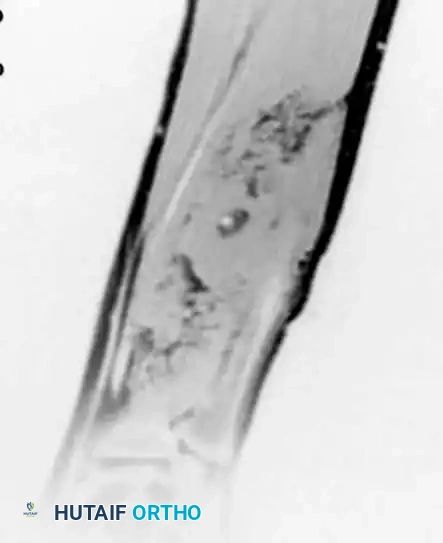
T1-weighted image (left) and fat-suppressed image (right) of intramuscular lipomas in the deep compartment of the leg. Note the uniform suppression of the lesion, confirming its lipomatous nature without thick septations or nodular enhancement.
Surgical Warning: Any lipomatous lesion demonstrating thick (>2 mm) septations, nodular non-adipose components, or heterogeneous enhancement must be treated as an Atypical Lipomatous Tumor (ALT) / Well-Differentiated Liposarcoma until proven otherwise via core needle biopsy.
Surgical Technique: Marginal Resection
Indications: Pain, functional impairment, rapid growth, or diagnostic uncertainty.
Positioning: Dependent on anatomical location. Ensure a tourniquet is available for extremity lesions to maintain a bloodless field.
- Incision: Plan a longitudinal incision parallel to the underlying muscle fibers and within standard extensile exposure lines.
- Dissection: Carry the incision through the skin and subcutaneous tissue. For deep lipomas, incise the deep fascia longitudinally.
- Tumor Delivery: Identify the thin, fibrous pseudocapsule of the lipoma. Use blunt finger dissection or a periosteal elevator to sweep the surrounding normal tissue away from the capsule.
- Hemostasis and Closure: Intramuscular lipomas may bleed from small perforating vessels at their base. Cauterize meticulously. Close the dead space over a closed-suction drain to prevent hematoma or seroma formation.
PERIPHERAL NERVE SHEATH TUMORS (PNSTs)
Benign peripheral nerve sheath tumors primarily include neurilemomas (schwannomas) and neurofibromas. Differentiating between the two is critical, as their surgical management and relationship to the parent nerve differ significantly.
Neurilemoma (Schwannoma)
Schwannomas are solitary, encapsulated tumors arising eccentrically from the Schwann cells of the nerve sheath. They typically involve major peripheral nerves (e.g., sciatic, peroneal, median, ulnar).
Histology: Characterized by a biphasic pattern of Antoni A (hypercellular, palisading spindle cells forming Verocay bodies) and Antoni B (hypocellular, myxoid, degenerative) tissue.
Clinical Presentation: Patients often report a mechanically induced radiating pain (Tinel's sign) along the nerve distribution. Motor deficits are rare.
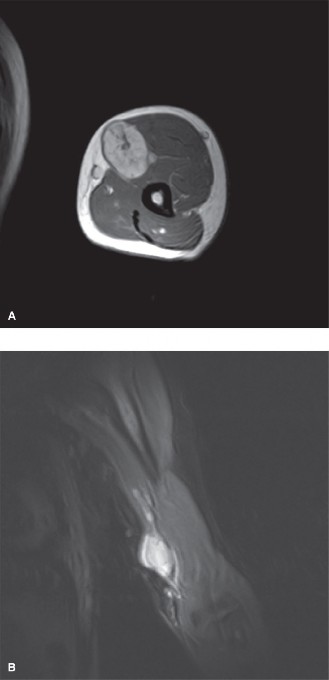
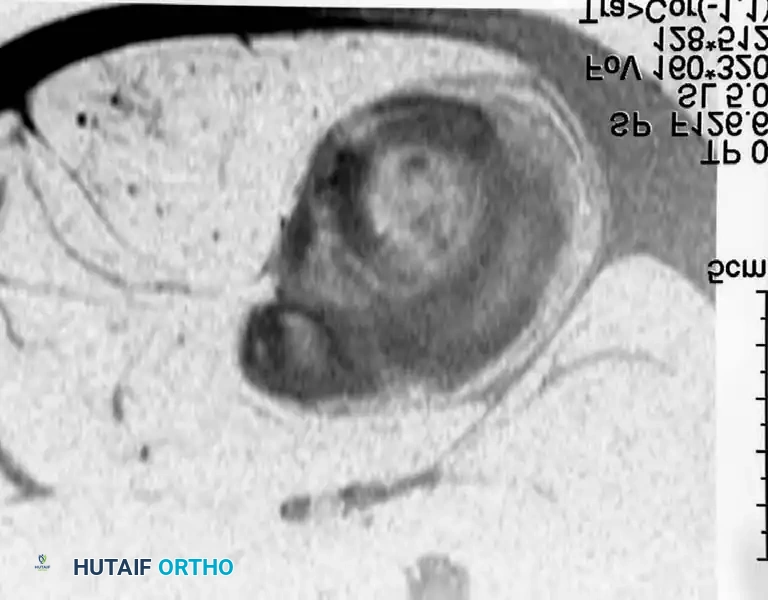
MRI demonstrating a fusiform mass along the peroneal nerve. The contrast-enhanced, fat-suppressed axial image shows peripheral enhancement with central low signal, classic for a schwannoma.

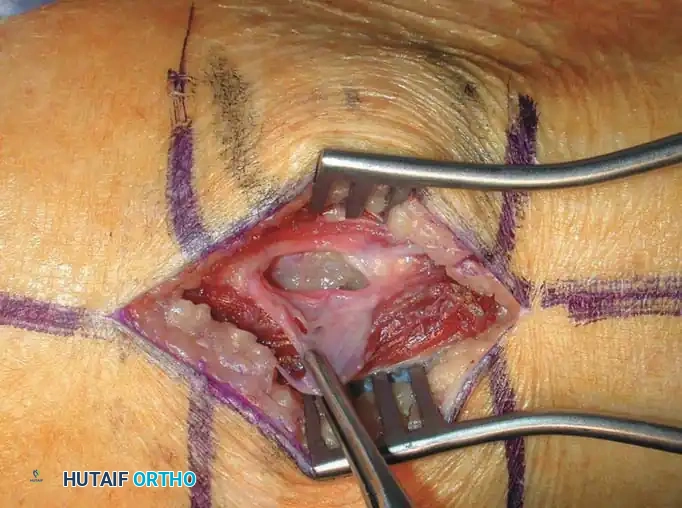
Intraoperative photographs showing the neurilemoma of the peroneal nerve. After incising the epineurium, the tumor is easily separated from the functioning nerve fibers using blunt dissection.
Neurofibroma
Unlike schwannomas, neurofibromas are intimately intertwined with the nerve fascicles, producing abundant collagen. They can be solitary or multiple (associated with Neurofibromatosis Type 1 / von Recklinghausen disease). The "plexiform" variant involves entire nerve plexuses and carries a higher risk of malignant peripheral nerve sheath tumor (MPNST) transformation.

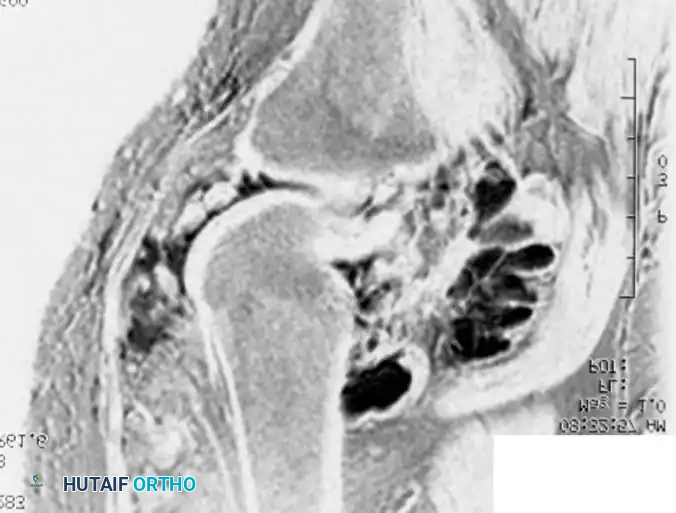
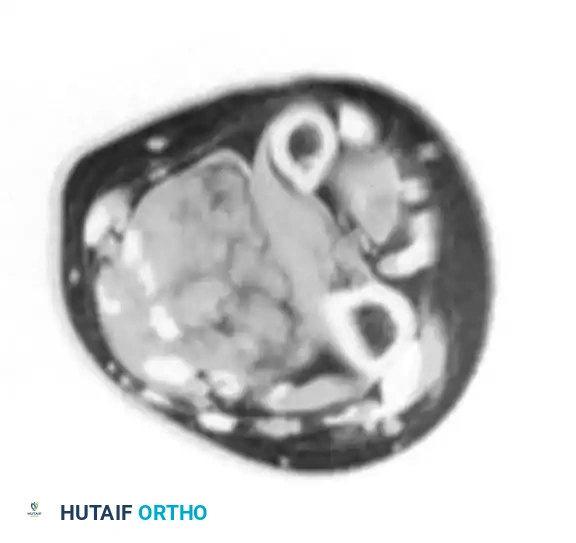
Axial and coronal MRI images showing a massive neurofibroma along the sciatic nerve in a patient with NF1.
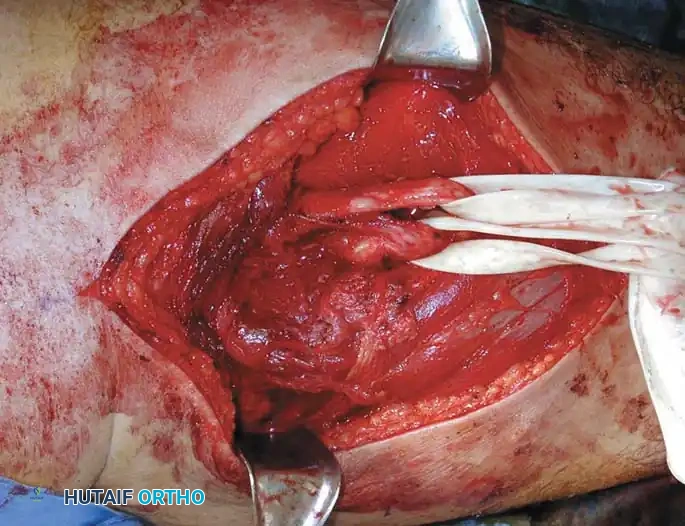

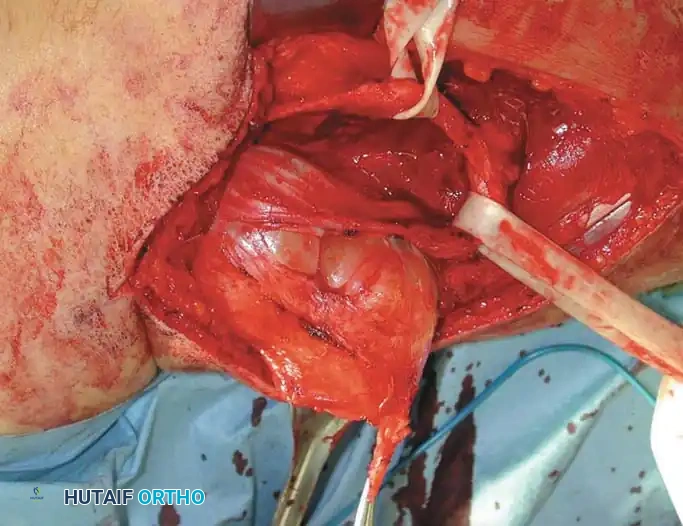
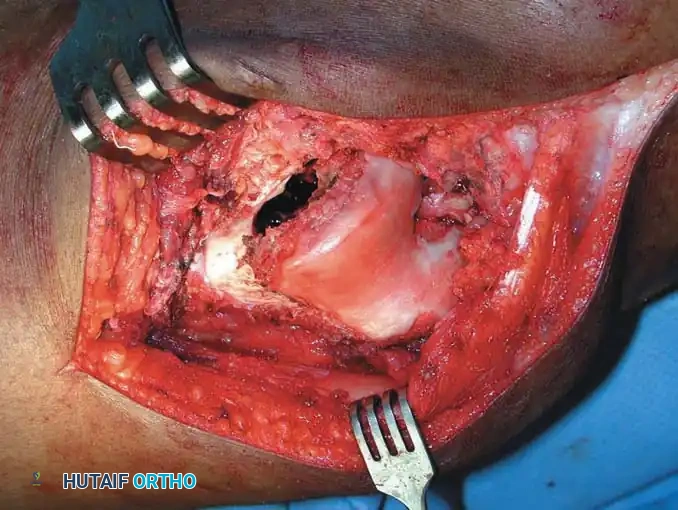
Intraoperative sequence: The epineurium is incised, and nerve fibers are meticulously dissected away. The tumor is removed while preserving the tibial and peroneal divisions of the sciatic nerve.
Surgical Approach to Nerve Sheath Tumors
Objective: Complete enucleation of the tumor with absolute preservation of neurological function.
1. Exposure: Expose the parent nerve proximally and distally to the tumor in virgin tissue planes. Utilize vessel loops for gentle retraction.
2. Epineurotomy: Under loupe or microscopic magnification, identify the splayed nerve fascicles draped over the tumor. Make a longitudinal incision through the epineurium in a safe zone devoid of crossing fascicles.
3. Enucleation: For schwannomas, establish the plane between the tumor capsule and the fascicles. Use micro-dissectors to gently peel the fascicles away. The tumor can usually be "shelled out" completely.
4. Neurofibroma Considerations: Solitary neurofibromas may require the sacrifice of a single, non-functional entering/exiting fascicle. Plexiform neurofibromas are often unresectable without causing severe neurological deficits; surgery is typically reserved for symptomatic relief or biopsy to rule out MPNST.
Pitfall: Never perform a transverse biopsy or aggressive sharp dissection on a suspected nerve sheath tumor. Iatrogenic transection of major motor fascicles is a devastating and entirely preventable complication.
SYNOVIAL PROLIFERATIVE LESIONS
Synovial Chondromatosis
Synovial chondromatosis is a rare, benign, monoarticular proliferative disorder characterized by cartilaginous metaplasia of the synovial membrane. It predominantly affects large joints (knee, hip, shoulder).
The disease progresses through three distinct Milgram phases:
1. Early: Active synovial disease with microscopic chondrometaplasia; no loose bodies.
2. Transitional: Active synovial disease with macroscopic, detached loose bodies.
3. Late: Multiple loose bodies with burnt-out, inactive synovium.
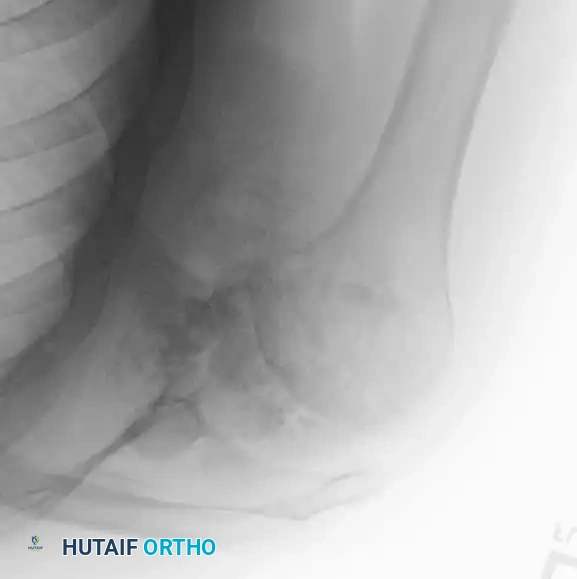
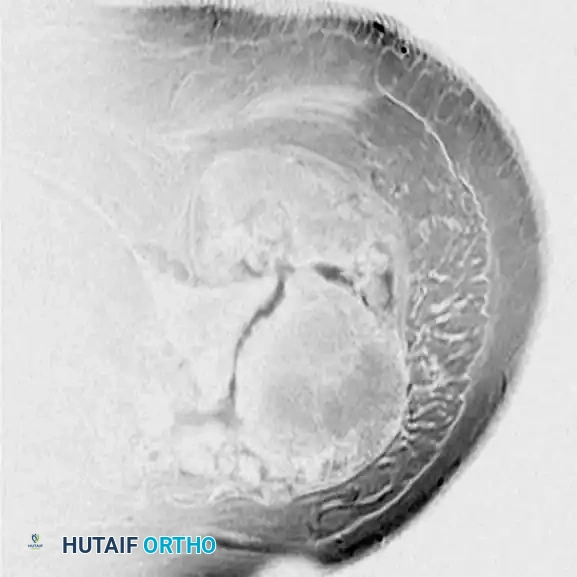

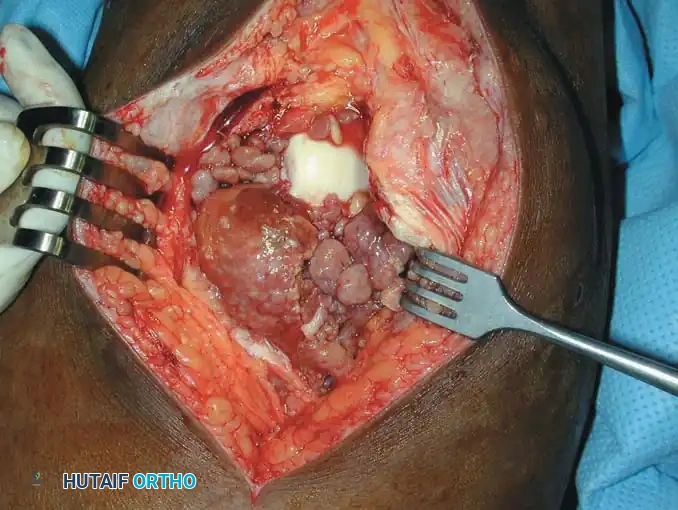
Radiograph and MRI of a shoulder with synovial chondromatosis, demonstrating multiple intra-articular ossified loose bodies. The gross specimen photograph highlights the sheer volume of cartilaginous bodies resected during synovectomy.
Surgical Management: Treatment dictates the removal of all loose bodies combined with an extensive anterior and posterior synovectomy. While arthroscopic management is preferred for the knee and shoulder, open arthrotomy is often required for the hip to ensure complete clearance and prevent secondary osteoarthritis.
Tenosynovial Giant Cell Tumors (GCTTS and PVNS)
These lesions represent a spectrum of the same neoplastic process, driven by an overexpression of Colony-Stimulating Factor 1 (CSF1).
- Localized Form (Giant Cell Tumor of Tendon Sheath - GCTTS): Typically presents as a painless, slow-growing, firm mass on the volar aspect of the digits. Histologically rich in multinucleated giant cells, foam cells, and hemosiderin.
- Diffuse Form (Pigmented Villonodular Synovitis - PVNS): Involves the entire synovial lining of a joint (most commonly the knee). Presents with recurrent, spontaneous hemarthrosis and joint destruction.


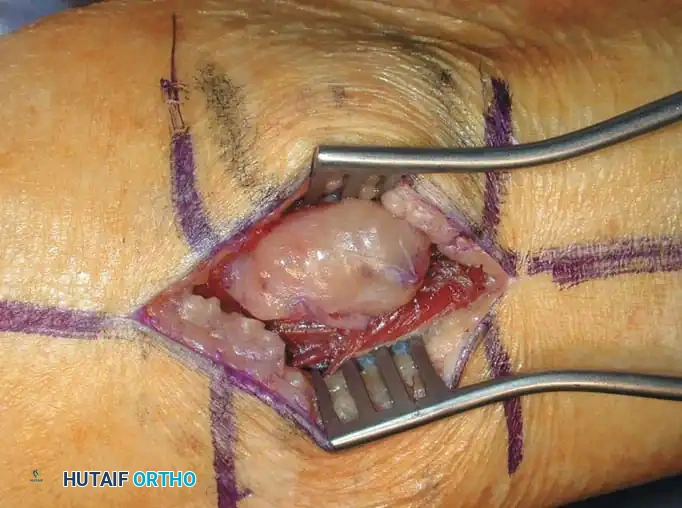
Clinical and intraoperative appearance of localized GCTTS. Marginal excision requires meticulous dissection off the flexor tendon sheath and digital neurovascular bundles.
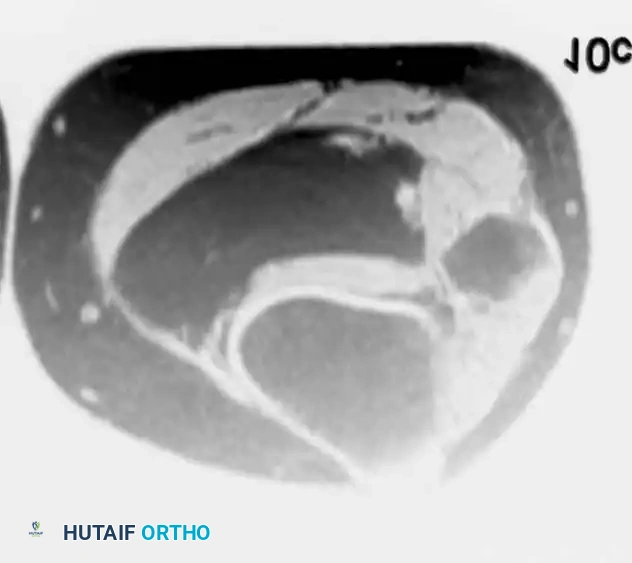
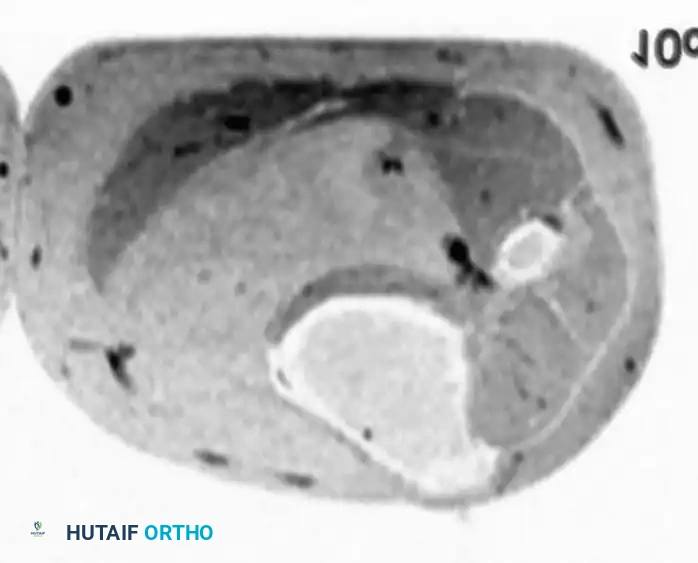
MRI of diffuse PVNS showing characteristic low-signal intensity on T2-weighted images due to profound hemosiderin deposition. Intraoperative view demonstrates the hypertrophic, villous, rust-colored synovium.
Surgical Management of PVNS:
1. Total Synovectomy: The goal is macroscopic eradication of all diseased synovium. In the knee, this requires a combined anterior (arthroscopic or open) and posterior open approach to access the posteromedial and posterolateral compartments.
2. Adjuvant Therapy: Due to high recurrence rates (up to 40% in diffuse forms), postoperative external beam radiotherapy (EBRT) or targeted systemic therapies (e.g., Pexidartinib, a CSF1R inhibitor) are increasingly utilized for refractory cases.
VASCULAR TUMORS AND MALFORMATIONS
Vascular anomalies are broadly divided into true neoplasms (e.g., hemangiomas) and vascular malformations (arteriovenous, venous, lymphatic).
Intramuscular Hemangiomas
Intramuscular hemangiomas are benign vascular neoplasms that can cause significant morbidity. They frequently present with pain that exacerbates with exercise or dependent positioning due to vascular engorgement.

MRI and intraoperative excision of an intramuscular hemangioma. Note the serpiginous vascular channels and interspersed adipose tissue.
Treatment Algorithm:
1. Conservative: Compression garments and activity modification.
2. Interventional: Preoperative embolization or sclerotherapy (e.g., sodium tetradecyl sulfate) to shrink the lesion and reduce intraoperative blood loss.
3. Surgical Resection: Indicated for well-circumscribed, symptomatic lesions. Wide marginal excision is required, as these lesions are highly infiltrative into the surrounding muscle fibers. Tourniquet use is mandatory.
Glomus Tumors (Glomangiomas)
A glomus tumor is a rare, benign hamartoma arising from the neuromyoarterial glomus body, which regulates thermoregulation.
Clinical Triad:
1. Exquisite point tenderness.
2. Severe paroxysmal pain.
3. Cold hypersensitivity.
They are classically located in the subungual region of the digits.
Clinical presentation showing a bluish-red discoloration beneath the nail plate. Surgical excision involves careful elevation of the nail plate, longitudinal incision of the nail bed, and marginal enucleation of the bluish tumor, followed by meticulous repair of the sterile matrix with 6-0 absorbable sutures to prevent nail deformity.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of benign soft-tissue tumor resections is dictated by the anatomical location, the extent of soft-tissue dissection, and the proximity to neurovascular structures.
- Wound Care: Compressive dressings are applied for 48 to 72 hours to minimize third-spacing and hematoma formation. Closed suction drains are removed when output is less than 30 cc per 24 hours.
- Immobilization: For extensive synovectomies (e.g., PVNS of the knee), a brief period of immobilization (24-48 hours) may be utilized to control hemarthrosis, followed immediately by Continuous Passive Motion (CPM) to prevent arthrofibrosis.
- Weight-Bearing: Generally, weight-bearing is permitted as tolerated unless a massive intramuscular resection compromises the structural integrity of the limb.
- Surveillance: While benign, lesions like PVNS, GCTTS, and intramuscular hemangiomas have notable local recurrence rates. Baseline postoperative MRI at 6 months, followed by annual clinical and radiographic surveillance for 2 to 5 years, is highly recommended.
Final Surgical Maxim: The successful management of benign soft-tissue tumors requires the same oncologic respect and anatomical precision as malignant sarcomas. Meticulous hemostasis, gentle tissue handling, and complete marginal resection are the cornerstones of preventing recurrence and optimizing patient outcomes.
You Might Also Like