Benign Hand Tumors: Comprehensive Surgical Management Guide
Key Takeaway
Benign tumors of the hand, including lipomas, giant cell tumors of the tendon sheath, and glomus tumors, require meticulous surgical management to preserve neurovascular function and minimize recurrence. This comprehensive guide details the pathophysiology, clinical presentation, and step-by-step surgical techniques for excising these lesions. Emphasizing precise dissection, appropriate imaging, and evidence-based postoperative protocols, it serves as an essential resource for orthopedic surgeons and hand specialists.
Introduction to Benign Tumors of the Hand
Benign tumors of the hand encompass a diverse group of neoplasms arising from adipose, synovial, fibrous, neural, and vascular tissues. Although lacking malignant potential, these lesions frequently cause significant morbidity due to the complex, unyielding, and densely packed neurovascular anatomy of the hand and wrist. Surgical management requires a profound understanding of hand biomechanics, meticulous microsurgical technique, and strict adherence to oncologic principles to minimize recurrence while preserving maximal function.
Clinical Pearl: Always approach a "simple" hand mass with a high index of suspicion. Inadequate preoperative imaging or marginal excision of an unrecognized aggressive lesion can lead to catastrophic functional loss or complex recurrences.
Adipose Tissue Tumors
Lipoma
Although lipomas are ubiquitous throughout the body, they are also the most common solid cellular tumors found in the hand. These lightly encapsulated tumors are composed of mature mesenchymal primordial fatty tissue cells. Histologically, they are characterized by the classic signet-ring cell, formed by a central lipid droplet that displaces the nucleus to the periphery.
Clinical Presentation and Biomechanics
Lipomas in the hand present in two distinct anatomical patterns:
* Superficial Lipomas: Arise from subcutaneous tissues, presenting as soft, fluctuant, bulging masses.
* Deep Lipomas: Arise within confined anatomical spaces such as the Guyon canal, the carpal tunnel, or the deep palmar space.
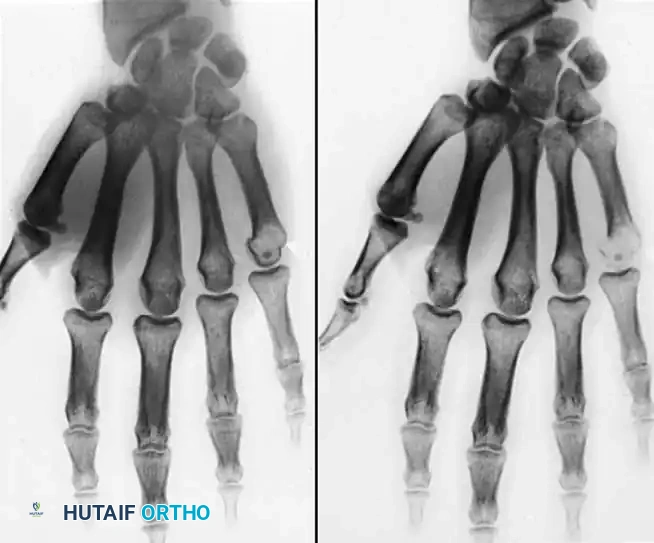
Due to the unyielding nature of the overlying palmar aponeurosis, lipomas originating in the deep palmar space tend to migrate and present at the periphery of the hand. Patients typically report a painless mass that mechanically impairs grasp. If the tumor is located adjacent to the metacarpophalangeal (MCP) joints, lateral deviation of the digits may occur. Furthermore, local mass effect within the carpal tunnel or Guyon canal can precipitate compressive neuropathies, manifesting as median or ulnar nerve sensory deficits and intrinsic muscle weakness.

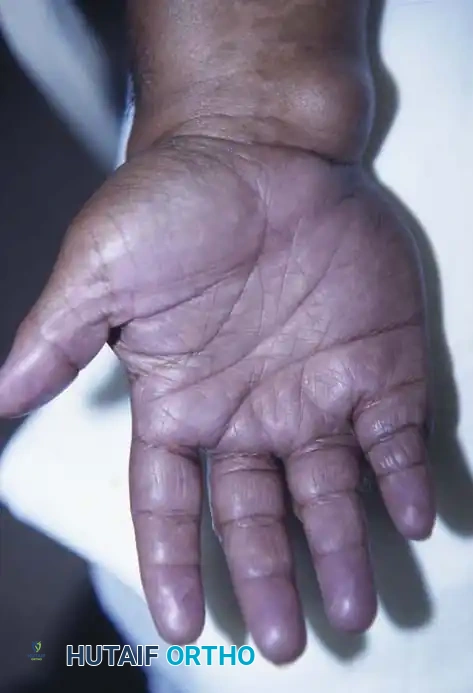
Fig. 1: Large palmar lipoma causing significant mechanical interference with grasp and digital flexion.

Fig. 2: Intraoperative view demonstrating extensive lobulation of the lipoma winding around digital nerves and flexor tendons.
Surgical Technique: Excision of Palmar Lipoma
1. Positioning: Supine with the arm extended on a hand table.
2. Tourniquet: Exsanguinate the limb and inflate the pneumatic tourniquet to 250 mm Hg to ensure a bloodless field.
3. Incision: Utilize a Brunner zigzag or extensile palmar incision directly over the mass, avoiding crossing flexion creases at a right angle.
4. Dissection: Careful blunt and sharp dissection is mandatory. Deep lipomas frequently sequester digital nerves and are invariably larger than clinically apparent.
5. Excision: Perform a marginal excision, ensuring the delicate capsule is not breached to prevent leaving lobules behind.
6. Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with non-absorbable sutures. Recurrence after complete marginal excision is exceptionally rare.
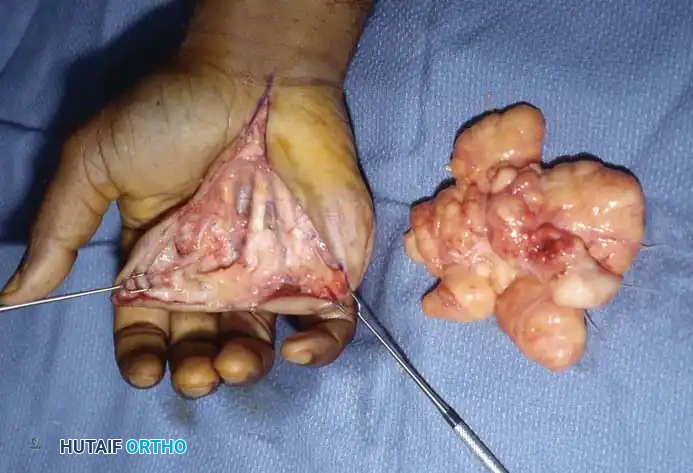
Fig. 3: Complete excision of the lipoma with surgical sparing of the flexor tendons and digital nerves.
Infiltrating Lipomas
Infiltrating lipomas are rare, nonencapsulated tumors occurring predominantly in adults. They are classified into two subtypes:
* Intermuscular: Growing between large muscle bellies and arising from fascial septa.
* Intramuscular: Arising directly between individual muscle fibers.
Despite their aggressive tissue infiltration, malignant transformation has not been reported. However, due to their nonencapsulated nature, they carry a formidable recurrence rate of up to 60%. Wide excision is recommended, balancing oncologic clearance with the preservation of essential motor function.
Lipoblastomas
Lipoblastomas are rare, benign tumors composed of immature, spindle-shaped cells, exclusively occurring in children younger than 7 years of age. They present in two forms: a deeply seated, poorly circumscribed variant, and a superficial, well-circumscribed variant.
Surgical Warning: The absence of cellular atypia and mitosis is critical to differentiate lipoblastomas from exceptionally rare congenital liposarcomas. Preoperative MRI is mandatory to assess the extent of the mass.
Surgical excision is the treatment of choice, carrying a reported recurrence rate of 14%.
Intraneural Lipofibromas
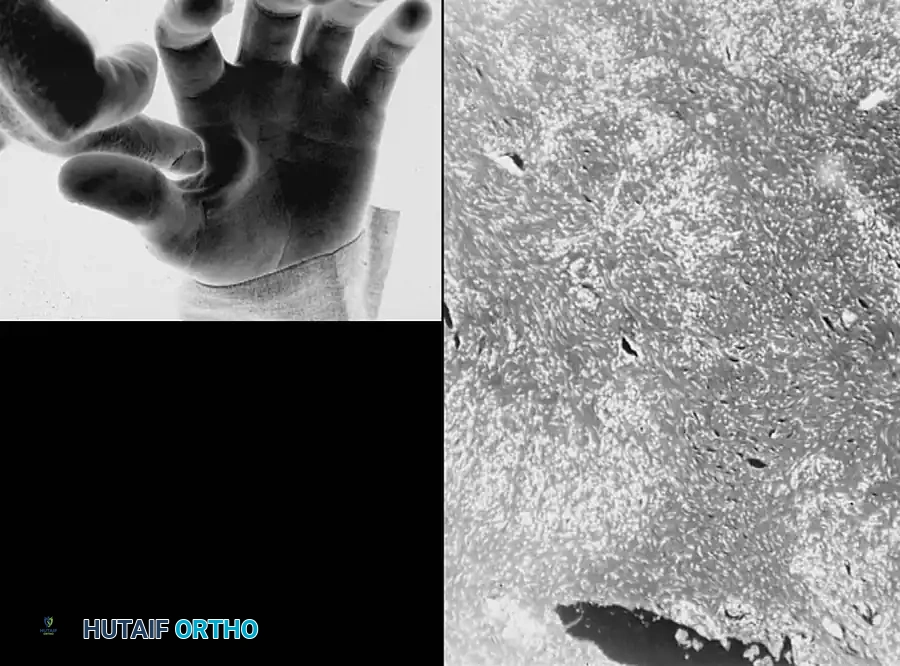
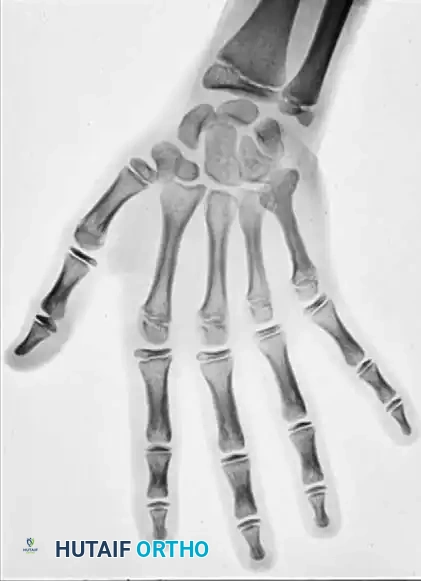
Intraneural lipofibromas are rare, benign lesions that exhibit a strong predilection for the median nerve. Patients typically present in the first three decades of life with a slowly enlarging mass in the palmar aspect of the hand or wrist, often accompanied by altered median nerve function and macrodactyly of the affected digits.
Pathophysiology
Microscopically, the lesion is characterized by fibroadipose tissue infiltrating the epineurium, which separates and compresses the individual nerve fascicles.

Fig. 4: Intraneural lipofibroma of the median nerve presenting with mild thumb enlargement and volar wrist pain.

Fig. 5: Surgical exposure revealing lipofibromatous tissue interspersed within and around the median nerve fascicles.
Surgical Management Principles
A strictly conservative approach is mandated.
* Decompression: If extrinsic neural compression exists, surgical decompression via carpal tunnel release or forearm fasciotomy is the gold standard.
* Contraindication: Intraneural excision or aggressive debulking of the median nerve is not recommended. Attempting to dissect the fibroadipose tissue from the fascicles invariably leads to severe intraneural fibrosis, ischemia, and a devastating increase in neural deficit.
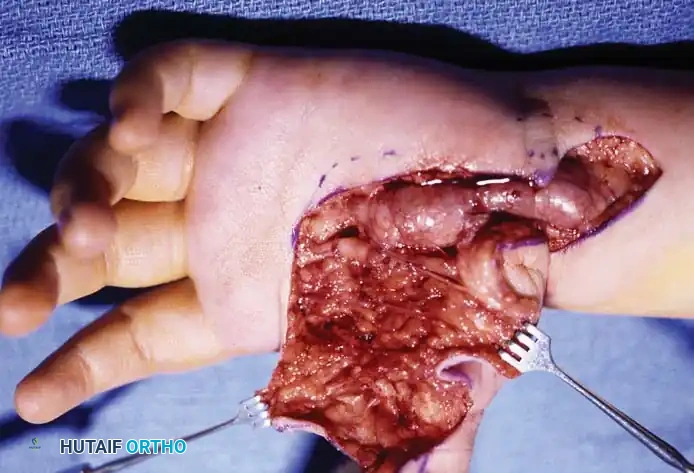
Fig. 6: Following conservative debulking and carpal tunnel release, the median nerve fascicles remain enlarged and tortuous, highlighting the infiltrative nature of the disease.
If a non-critical digital nerve is exclusively involved, an en bloc excision of the nerve segment followed by primary nerve grafting may be successful, though the patient must be counseled regarding permanent sensory alteration.
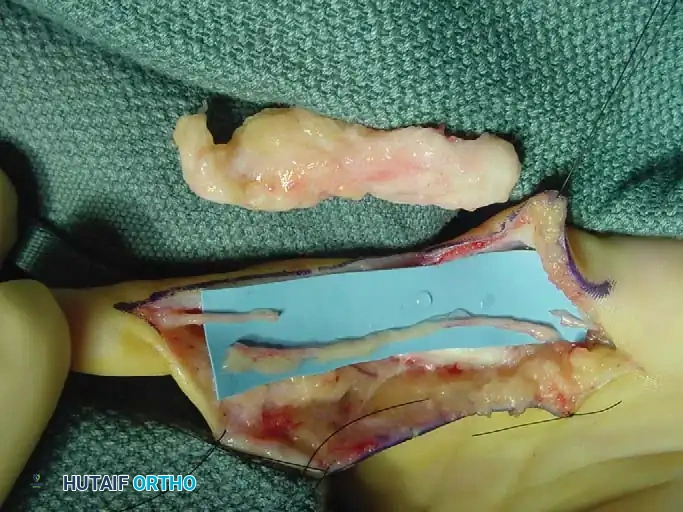
Fig. 7: Recurrent intraneural lipofibroma of the ulnar digital nerve to the small finger.
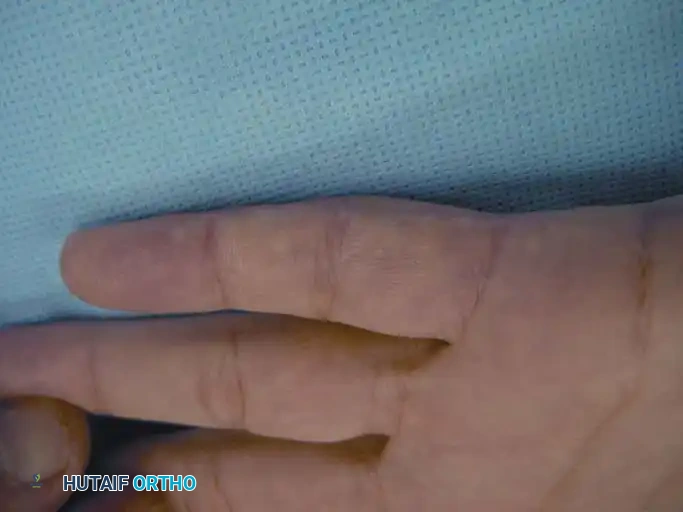
Fig. 8: Surgical exposure demonstrating a 4-cm segment of involved ulnar digital nerve with normal-appearing proximal and distal segments.

Fig. 9: En bloc excision of the digital nerve and tumor, with an interpositional nerve graft placed in proximity.
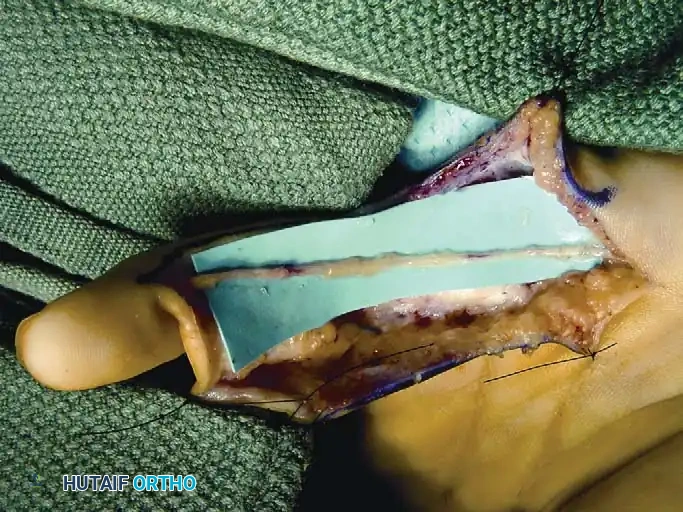
Fig. 10: Nerve graft meticulously sutured in place using 8-0 or 9-0 epineurial sutures under microscopic magnification.
Synovial and Tendon Sheath Tumors
Giant Cell Tumor of the Tendon Sheath (Xanthoma)
Giant cell tumors of the tendon sheath (GCTTS) are the second most common solid cellular tumors of the hand. They occur most frequently between the ages of 8 and 80 years and exhibit a strong predilection for the palmar aspect of the digits. Multiple xanthomas may be indicative of underlying hypercholesterolemia.
Clinical and Histological Profile
GCTTS are typically slow-growing, painless masses. However, when located adjacent to a joint (most commonly the proximal interphalangeal joint), they can mechanically block flexion or extension. Grossly, they appear as yellow or tan lobulated masses. Histologically, they are composed of spindle cells, fibrous tissue, cholesterol-laden histiocytes, multinucleated giant cells, and hemosiderin deposits.

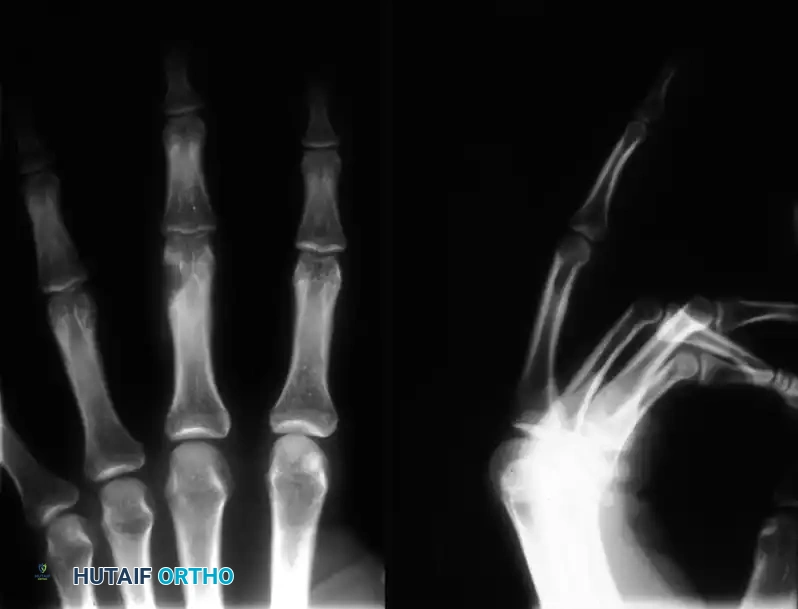
Fig. 11: Giant cell tumor of the tendon sheath demonstrating nearly circumferential involvement of the index finger tip.

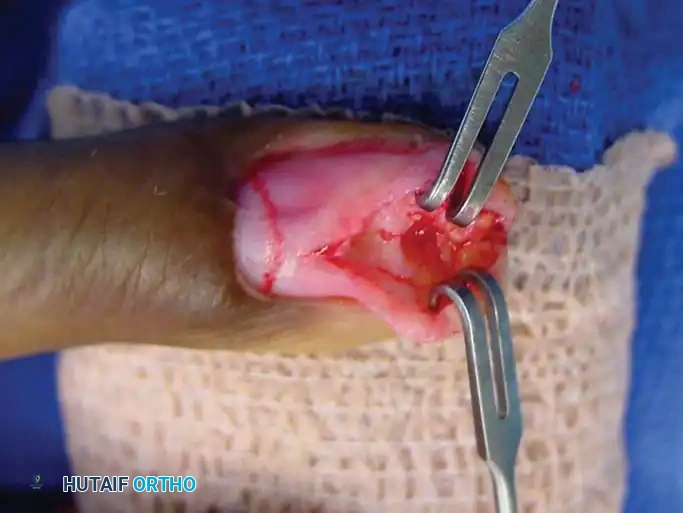
Fig. 12: Surgical dissection showing a well-encapsulated giant cell tumor with its pathognomonic yellowish-brown color.
Surgical Excision and Recurrence
Excision is notoriously difficult. These tumors frequently wind in and around the flexor tendons, their synovial sheaths, digital nerves, and occasionally the extensor mechanism, sometimes encompassing three-fourths of
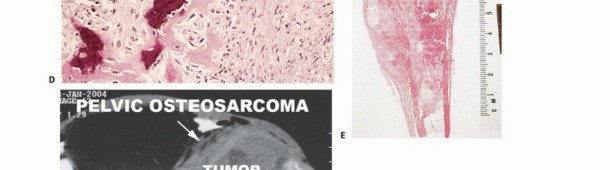
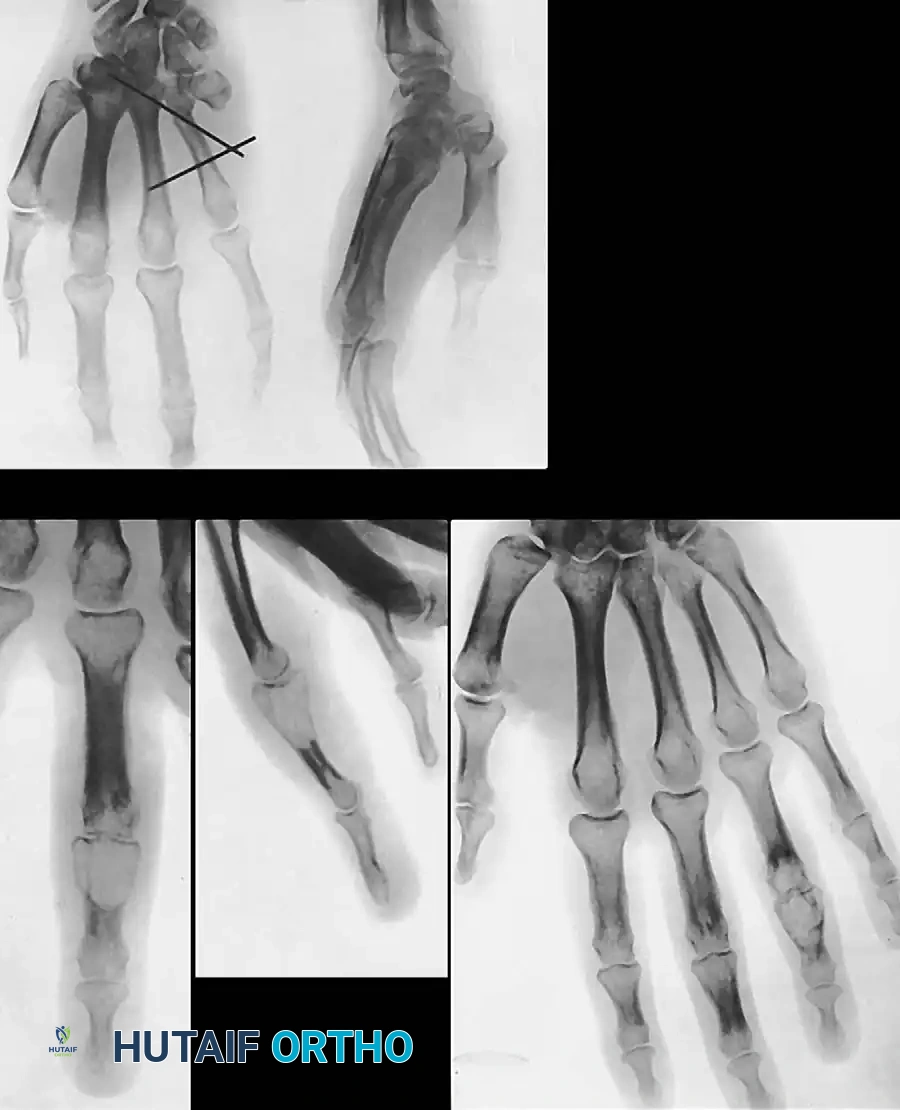
Associated Surgical & Radiographic Imaging











You Might Also Like