Radial Dysplasia: Comprehensive Guide to Epidemiology, Classification, and Surgical Anatomy
Key Takeaway
Radial dysplasia, or radial longitudinal deficiency, is a congenital anomaly affecting the forearm and hand's radial side, varying from thumb hypoplasia to complete radius absence. It's often associated with syndromes like Holt-Oram or Fanconi anemia. The Bayne and Klug classification (Types 0-V) categorizes severity based on radiographic findings, guiding diagnosis and surgical planning.
Chapter Radial Dysplasia: Unlock Reconstruction Solutions
Introduction & Epidemiology
Radial dysplasia, also termed radial longitudinal deficiency, represents a spectrum of congenital anomalies characterized by hypoplasia or aplasia of the radial side of the forearm and hand. This longitudinal deficiency in radial growth can manifest in varying degrees of severity, from isolated radial hypoplasia to complete absence of the radius and associated carpal and digital structures. The condition is often bilateral, occurring in approximately 50% of cases, and demonstrates a slight male predominance. Its incidence is estimated at 1 in 30,000 to 1 in 100,000 live births, making it a relatively rare, yet clinically significant, upper extremity anomaly.
The embryological basis of radial dysplasia involves a disruption in the differentiation and growth of the apical ectodermal ridge and the underlying mesenchymal cells of the limb bud during the fourth to eighth weeks of gestation. This critical period coincides with the development of numerous other organ systems, accounting for the frequent association of radial dysplasia with systemic conditions. These conditions are pivotal in both diagnosis and management, influencing surgical timing and approach. The most commonly recognized associations include:
*
Holt-Oram Syndrome:
An autosomal dominant disorder characterized by cardiac abnormalities (septal defects, conduction defects) and upper limb anomalies, often including radial dysplasia.
*
Thrombocytopenia-Absent Radius (TAR) Syndrome:
An autosomal recessive condition featuring congenital thrombocytopenia (which often improves with age) and bilateral radial aplasia, but characteristically with preserved thumbs.
*
Fanconi Anemia:
An autosomal recessive chromosomal instability disorder leading to progressive bone marrow failure, various congenital anomalies (skeletal, renal, cardiac), and increased cancer risk. Radial dysplasia, often bilateral, is a common skeletal manifestation.
*
VACTERL Association:
A non-random association of birth defects affecting multiple systems, including
V
ertebral anomalies,
A
nal atresia,
C
ardiac defects,
T
racheo
E
sophageal fistula,
R
enal anomalies, and
L
imb anomalies (often radial dysplasia).
*
Other Associations:
Less commonly, radial dysplasia can be seen with Cornelia de Lange syndrome, fetal alcohol syndrome, or as an isolated anomaly.
A thorough understanding of these associated conditions is paramount. Preoperative assessment must extend beyond the orthopedic evaluation to include hematologic, cardiac, and renal workups, as these systemic issues frequently dictate the patient's overall health and suitability for surgical intervention.
Surgical Anatomy & Biomechanics
A precise understanding of the surgical anatomy and biomechanics of radial dysplasia is fundamental to successful reconstruction. The anomaly's severity dictates the degree of skeletal and soft tissue involvement.
The most widely accepted classification system is that proposed by Bayne and Klug, which categorizes radial dysplasia based on the radiographic appearance of the radius:
*
Type 0: Radial Ray Hypoplasia (Pre-axial Deficiency)
* Often involves thumb hypoplasia or aplasia without significant radial shortening or deviation. Radiographs may show subtle radial shortening or carpal anomalies.
*
Type I: Short Distal Radius
* The radius is mildly shortened, with normal proximal and distal epiphyses. The hand is mildly deviated radially, and the thumb may be hypoplastic. The wrist joint is congruent.
*
Type II: Hypoplastic Non-functional Radius (Miniature Radius)
* The radius is significantly shortened, with both proximal and distal epiphyses present but defective in growth. The bone is often miniature, leading to substantial radial deviation of the hand. The wrist joint is incongruent.
*
Type III: Partial Absence of the Radius
* The proximal portion of the radius is present, but the distal part is absent. The hand is severely radially deviated, and the wrist is unsupported. The ulna is often thickened and bowed.
*
Type IV: Total Absence of the Radius
* The entire radius is absent. The hand is severely radially deviated, often at a 90-degree angle, with the carpus articulating directly with the ulna or forming a pseudoarthrosis. The ulna is significantly thickened and bowed, and the carpal bones are frequently underdeveloped or fused. The thumb is typically absent or severely hypoplastic.
*
Type V: Ulnar Forearm Duplication (Mirror Hand)
* While not a direct deficiency, Type V is sometimes included as a severe manifestation of radial ray deficiency leading to absence of radial elements and duplication of ulnar structures.

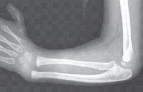
Figure 1: Radiograph demonstrating a severe form of radial dysplasia (Bayne and Klug Type IV) with complete absence of the radius, severe radial deviation, and ulnar bowing.

Figure 2: Clinical appearance of a patient with bilateral radial dysplasia, highlighting the characteristic radial deviation and forearm shortening.
Skeletal Anatomy
- Ulna: In Type III and IV deficiencies, the ulna becomes the primary forearm bone. It is frequently thickened, bowed, and shortened, often displaying hypertrophy of the distal epiphysis due to increased weight-bearing stress. The bowing is typically concave radially.
- Carpus: Carpal bones are often hypoplastic, abnormally shaped, or fused. The scaphoid and trapezium, which are typically on the radial side, are often absent or severely malformed. The carpus is displaced radially and proximally relative to the ulna.
- Metacarpals and Phalanges: The thumb (first ray) is frequently absent (aplasia) or severely hypoplastic, often lacking intrinsic muscles and proper joint mechanics. Other digits may also show anomalies, although less commonly.
- Elbow: While often spared, elbow joint contractures or instability can occur, particularly in severe cases.
Soft Tissue Anatomy
- Muscles and Tendons: There is often hypoplasia or absence of radial-sided muscles (e.g., brachioradialis, extensor carpi radialis longus/brevis, abductor pollicis longus, extensor pollicis longus/brevis). Ulnar-sided muscles may be relatively stronger, contributing to the deforming radial deviation. The flexor-pronator mass is often tight.
-
Neurovascular Structures:
- Median Nerve: In severe radial dysplasia, the median nerve can be compressed or stretched over the apex of the ulnar bow or constricted by tight fibrous bands (anlage) on the radial aspect. It often takes an abnormal course, deviating radially. Neurolysis and careful protection are critical during surgery.
- Radial Nerve: The radial nerve and its branches are often hypoplastic or absent, particularly in Type III and IV deficiencies.
- Radial Artery: The radial artery is frequently absent or vestigial. The forearm circulation is primarily supplied by the ulnar artery, which needs careful preservation.
- Skin and Fascia: The skin and subcutaneous tissues on the radial side are often tight and contracted, contributing to the deviation. Fibrous bands or anlage, representing remnants of the undeveloped radius, are frequently present and act as deforming forces.

Figure 3: Intraoperative view demonstrating the tight soft tissue anlage and displaced median nerve in a case of radial dysplasia, emphasizing the need for meticulous dissection.

Figure 4: Illustration depicting the typical course of the median nerve (yellow) draped over the ulnar bow and the potential for compression in severe radial dysplasia.
Biomechanics
The primary biomechanical challenges stem from the absence or deficiency of the radial support for the carpus. This leads to:
*
Radial Deviation:
The hand and carpus radially deviate due to the absence of the radial column and the unopposed pull of the ulnar wrist flexors and extensors, compounded by radial-sided soft tissue contractures. This significantly impairs wrist and hand function.
*
Forearm Shortening:
Overall shortening of the affected limb, impacting reach and bimanual activities.
*
Limited Forearm Rotation:
While supination and pronation are primarily controlled by the radioulnar joints, severe radial dysplasia with significant ulnar bowing or carpal malposition can indirectly affect forearm rotation.
*
Functional Impairment:
The radial deviation compromises grasp, pinch, and activities of daily living (ADLs). The functional goal of reconstruction is to center the hand over the ulna, providing a stable platform for hand function.

Figure 5: Radiographic image showcasing the severe radial deviation of the carpus and hand relative to the distal ulna in a patient with total radial aplasia.

Figure 6: Diagram illustrating the biomechanical forces contributing to radial deviation, with the ulna acting as a pivot point and unopposed ulnar-sided muscle pull.
Indications & Contraindications
The decision to intervene surgically in radial dysplasia is complex, balancing the potential functional and cosmetic benefits against inherent surgical risks and the patient's overall health status. The primary goals of surgical reconstruction are to:
1. Center the carpus over the distal ulna to establish a stable and functional wrist joint.
2. Correct the radial deviation of the hand.
3. Improve the functional length of the forearm.
4. Enhance cosmesis.
5. Address associated thumb aplasia/hypoplasia, typically through pollicization as a separate, but often coordinated, procedure.
Operative Indications
Surgical intervention is generally considered for patients with Bayne and Klug Type III and IV radial dysplasia, where significant functional impairment and progressive deformity are evident.
*
Severe Radial Deviation:
Patients with pronounced radial deviation (typically >60 degrees) that significantly compromises activities of daily living.
*
Functional Impairment:
Difficulty with grasp, pinch, object manipulation, or bimanual tasks due to the wrist deformity.
*
Progressive Deformity:
Documented worsening of radial deviation or subluxation despite conservative management (stretching, splinting).
*
Anticipation of Growth:
Early intervention (typically 6-12 months of age for centralization) aims to prevent further deformity progression and optimize long-term outcomes.
*
Consideration for Pollicization:
While thumb reconstruction is a distinct procedure, its functional benefits are often maximized when the wrist is stabilized.
Non-Operative Indications
Conservative management is appropriate for milder forms of radial dysplasia or when surgical risks outweigh potential benefits.
*
Bayne and Klug Type I and II:
These milder forms often maintain adequate function and may not require surgical intervention. Initial management typically involves stretching exercises and custom-molded splints to prevent contracture.
*
Mild Deformity:
Minimal functional limitation and acceptable cosmetic appearance.
*
Severe Systemic Comorbidities:
Patients with severe cardiac, hematologic, or renal issues (e.g., unmanaged Fanconi anemia, unstable Holt-Oram cardiac anomalies) may be poor surgical candidates.
*
Inadequate Soft Tissue Envelope:
Extreme skin and muscle deficiency may preclude successful surgical correction without extensive reconstructive procedures.
*
Poor Ulna Quality:
A severely hypoplastic or dysfunctional ulna may not provide a stable foundation for centralization.
*
Patient/Family Choice:
After thorough discussion of risks and benefits.
Contraindications
Absolute contraindications are rare and typically relate to the patient's overall health status or the severity of the local tissue involvement.
*
Uncontrolled Systemic Disease:
Unstable cardiac disease, active hematologic crisis (e.g., severe thrombocytopenia in TAR syndrome), or untreated renal failure.
*
Severe Forearm Hypoplasia:
In cases where the forearm is extremely short and stiff, and the ulna is also severely hypoplastic, the functional gains from wrist surgery may be minimal.
*
Active Infection:
Any local or systemic infection.
The following table summarizes the indications for operative versus non-operative management in radial dysplasia reconstruction:
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Bayne & Klug Type | Type III, Type IV (Centralization, Radialization, Forearm Lengthening) | Type I, Type II (Observation, stretching, splinting) |
| Functional Impairment | Significant wrist radial deviation affecting grasp, pinch, ADLs | Minimal functional deficit, effective compensatory movements |
| Progressive Deformity | Documented worsening of wrist subluxation/dislocation over time | Stable deformity, no progression with conservative measures |
| Associated Conditions | Medically stable patients; hematologic and cardiac workup cleared | Severe cardiac, hematologic, or renal comorbidities precluding surgery |
| Soft Tissue Envelope | Sufficient skin, muscle, and neurovascular integrity for closure | Significant soft tissue deficiency, severe chronic contractures |
| Patient Age | Typically 6-12 months for initial wrist surgery; later for staged procedures | Early infancy for stretching/splinting; severe comorbidities make surgery prohibitive |
| Thumb Anomalies | Pollicization considered in conjunction with wrist surgery for functional gain | Isolated thumb hypoplasia not requiring wrist reconstruction (e.g., web space deepening for pinch) |
| Ulna Quality | Ulna of sufficient size and stability to provide a platform for carpus | Severely hypoplastic or unstable ulna where centralization would not be durable |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount to optimize outcomes and mitigate complications in radial dysplasia reconstruction.
Comprehensive Assessment
-
Clinical Evaluation:
- History: Detailed birth history, family history of congenital anomalies, developmental milestones. Inquire about associated syndromes, specifically screening for cardiac symptoms (Holt-Oram), bleeding tendencies (TAR), and recurrent infections/anemia (Fanconi Anemia).
- Physical Examination: Assess the degree of radial deviation, forearm length discrepancy, wrist and elbow range of motion, and grip strength (if age-appropriate). Evaluate thumb status (aplasia, hypoplasia, mobility), as pollicization is often a concomitant or staged procedure. Document neurovascular status, paying particular attention to median nerve function and radial artery patency.
-
Imaging Studies:
- Plain Radiographs: Anteroposterior and lateral views of the forearm and hand are essential to classify the deformity according to Bayne and Klug. Assess the degree of ulnar bowing, carpal position relative to the ulna, and skeletal maturity.
- MRI: May be useful to delineate soft tissue structures, including the course of the median nerve, the extent of the radial anlage, muscle morphology, and carpal anomalies, particularly when considering complex soft tissue releases or tendon transfers.
- CT Angiography: In complex cases with questionable vascularity or for preoperative planning of free tissue transfers, CTA can map the dominant forearm vasculature (typically ulnar artery).
-

Figure 7: Preoperative radiograph demonstrating Bayne and Klug Type IV radial dysplasia with significant ulnar bowing and total absence of the radius, requiring careful planning for centralization and potentially ulnar osteotomy. -

Figure 8: Preoperative clinical photograph illustrating the marked radial deviation of the hand and severe forearm shortening in a patient with radial longitudinal deficiency.
-
Systemic Workup:
- Hematologic: Complete blood count, platelet count, and genetic testing for Fanconi Anemia or TAR syndrome are crucial. Patients with Fanconi Anemia require a bone marrow biopsy and often specialized anesthetic management due to bone marrow failure.
- Cardiac: Echocardiogram and cardiology consultation for all patients, especially those with suspected Holt-Oram syndrome.
- Renal: Renal ultrasound for VACTERL association.
- Genetic Counseling: Recommended for all patients and families to understand the inheritance patterns and recurrence risks.
Informed Consent
A detailed discussion with the family is imperative. This includes:
* Expected outcomes: Improved wrist stability and alignment, enhanced function, and cosmetic improvement. It is crucial to manage expectations regarding perfect correction or normal function.
* Potential complications: Recurrence, stiffness, infection, nerve injury, skin necrosis, ulnar growth issues.
* Alternatives: Conservative management, external fixation, or no intervention.
* Staged procedures: Explanation that centralization/radialization is often the first step, with pollicization, forearm lengthening, or revision procedures potentially required later.
* Long-term commitment to rehabilitation and follow-up.
Anesthesia Considerations
Pediatric anesthesia expertise is critical. Anesthetic choices should account for:
* Age and weight of the child.
* Presence of associated cardiac anomalies.
* Potential for difficult airway (e.g., some syndromic conditions).
* Hematologic status (e.g., thrombocytopenia in TAR syndrome).
Patient Positioning
- The patient is positioned supine on the operating table.
- The affected arm is abducted on a specialized hand table, allowing full access to the forearm and wrist.
- A tourniquet is applied to the upper arm. The limb is typically exsanguinated before inflation.
- Ensure adequate padding to prevent pressure neuropathies.
- The entire upper extremity, from shoulder to fingertips, is prepped and draped to allow visualization of the elbow and to facilitate full range of motion of the wrist and fingers during the procedure. This also allows for potential elbow joint mobilization if needed.
Detailed Surgical Approach / Technique
The primary surgical goal is to centralize the carpus over the distal ulna, providing a stable, functional platform for hand use. The procedure is typically performed between 6 and 12 months of age, allowing for adequate soft tissue development while minimizing the establishment of fixed contractures.
Anesthesia and Tourniquet
General anesthesia is administered. The upper arm tourniquet is inflated to appropriate pressure after careful exsanguination. Prophylactic antibiotics are administered.
Incision
A long, curvilinear incision is made on the radial aspect of the forearm and wrist, typically extending from the mid-forearm to the base of the thumb metacarpal. A zigzag or V-Y plasty extension may be used distally to accommodate skin tension during correction. The incision should allow for thorough soft tissue release and visualization of the ulna and carpus.
Soft Tissue Release and Lengthening
This is a critical initial step to allow for correction of the radial deviation without excessive tension.
1.
Skin and Subcutaneous Tissue:
Carefully elevate full-thickness skin flaps. Identify and protect superficial neurovascular structures.
2.
Radial Anlage and Fibrous Bands:
Identify and excise the rudimentary radial anlage, which is often a thick, fibrous band tethering the carpus radially. Release all constricting fibrous bands, fascia, and retinacula on the radial side.
3.
Muscle and Tendon Release:
* Release the origins of tight radial-sided muscles, such as the rudimentary radial wrist extensors or flexors, if present and contributing to the deformity.
* Perform Z-lengthening of any tight flexor carpi radialis or extensor carpi radialis tendons.
4.
Median Nerve Neurolysis:
Carefully identify and gently dissect the median nerve, which is frequently displaced radially and may be taut, bowed, or compressed by the anlage or fascia. Perform a thorough neurolysis to free it from all constricting tissues, ensuring it can accommodate the new, centralized position of the carpus without tension. This is a critical step to prevent postoperative median nerve palsy.
*

Figure 9: Intraoperative image showing the median nerve (yellow arrow) carefully dissected and protected after release of the surrounding tight fibrous tissue during centralization.
5.
Capsulotomy:
Perform a comprehensive radial and palmar capsulotomy of the radiocarpal (or ulnocarpal) joint. Release the radial collateral ligament and any tight portions of the joint capsule to allow full ulnar translation of the carpus.
Skeletal Reconstruction (Centralization vs. Radialization)
The goal is to align the carpus over the distal ulna.
1.
Preparation of the Ulna:
The distal ulna is often bulbous and may have an abnormal epiphyseal plate. Preserve the ulnar physis if possible, as it is the primary growth center of the forearm.
2.
Carpectomy (Optional):
In cases of severe carpal malformation or to facilitate carpal alignment, a partial carpectomy, typically involving the lunate or scaphoid, may be performed. This creates a recess for the distal ulna.
3.
Creating a Slot in the Carpus:
A central slot is created in the proximal carpal row (often by resecting a portion of the lunate or by separating the carpal bones) to accept the distal ulna.
4.
Centralization vs. Radialization:
*
Centralization:
The preferred technique. The distal ulna is seated centrally within the carpus, aligning the hand in a neutral position relative to the forearm. This provides balanced forces and maintains maximal forearm length.
*
Radialization (less common now):
The distal ulna is seated more ulnarly within the carpus, correcting the radial deviation by shifting the hand ulnarward. While it provides good correction, it can lead to increased stress on the ulnar side of the wrist and potentially progressive ulnar deviation over time.
*

Figure 10: Intraoperative photograph illustrating the carpus being centralized over the distal ulna, with a K-wire traversing the ulna and carpus for temporary stabilization.
*

Figure 11: Postoperative radiograph after successful centralization, showing the K-wire fixation aligning the carpus over the distal ulna, with corrected radial deviation.
- Ulnar Osteotomy (if indicated): If severe ulnar bowing persists after soft tissue release and centralization, a corrective ulnar osteotomy (often a closing wedge osteotomy) may be necessary to further straighten the forearm axis and improve cosmesis. This is usually performed in the mid-diaphysis.
- Distal Ulnar Epiphysiodesis (Controversial): If the ulna is projected to overgrow significantly or if there is severe ulnar positive variance after initial centralization, a temporary or permanent distal ulnar epiphysiodesis might be considered. However, this is controversial due to the risk of premature growth arrest and subsequent forearm shortening, and is generally avoided in the initial centralization. Forearm lengthening procedures with external fixators are preferred if significant length discrepancy persists later.
Stabilization
- K-wire Fixation: After achieving optimal alignment, the carpus is stabilized to the ulna with one or two smooth K-wires (typically 1.6-2.0 mm). The K-wires are usually driven from the dorsal aspect of the carpus, through the carpus, into the medullary canal of the ulna. Care must be taken to avoid the ulnar physis.
-
Tendon Transfers:
To maintain correction and provide dynamic stability, tendon transfers are often performed.
- Extensor Carpi Ulnaris (ECU) Transfer: A common technique involves detaching the ECU from its insertion and rerouting it radially, inserting it into the radial side of the carpus (e.g., into the rudimentary scaphoid/trapezium or the base of the second metacarpal). This provides a dynamic radially directed pull to counteract the deforming ulnar forces and prevent recurrence of radial deviation. The ECU is often split to create two slips, one for dorsal and one for volar stabilization.
- Alternatively, other expendable ulnar-sided tendons can be transferred to provide balance.
-

Figure 12: Schematic illustration demonstrating the rerouting and insertion of the Extensor Carpi Ulnaris (ECU) tendon to the radial side of the carpus to provide active stabilization after centralization.
External Fixation (for complex cases or staged lengthening)
In cases with severe, rigid deformities, significant forearm length discrepancy, or pronounced ulnar bowing, an external fixator (e.g., Ilizarov or unilateral fixator) may be used.
*
Gradual Correction:
The fixator can be applied to gradually distract and correct the soft tissue contractures and skeletal deformity over weeks, minimizing neurovascular compromise.
*
Distraction Osteogenesis:
If forearm lengthening is required, this can be performed through an ulnar osteotomy and gradual distraction. This is typically a staged procedure, performed after initial wrist stabilization and soft tissue maturation.

Figure 13: Clinical image of an external fixator applied for gradual correction and distraction lengthening in a patient with severe radial dysplasia and forearm shortening.
Wound Closure
After satisfactory correction and fixation, the wound is closed in layers.
* Deep fascia and subcutaneous tissues are carefully reapproximated.
* The skin is closed meticulously. A Z-plasty or V-Y plasty may be performed if necessary to prevent tension along the incision line.
* A bulky dressing and a long-arm cast, maintaining the wrist in neutral to slight ulnar deviation, are applied.

Figure 14: Postoperative image of the limb immobilized in a long-arm cast after centralization and internal fixation, ensuring stable maintenance of the corrected position.
Staged Procedures
- Pollicization: Reconstruction of a functional thumb (pollicization of the index finger) is a crucial component of overall hand function and is typically performed as a separate, staged procedure, often before or after wrist centralization. The timing depends on the surgeon's preference and the severity of the thumb deficiency.
- Forearm Lengthening: For significant forearm length discrepancy (e.g., >5 cm), distraction osteogenesis using an external fixator may be performed at a later age (e.g., 5-8 years old) to improve cosmesis and function.
Complications & Management
Despite meticulous surgical technique, complications can occur in radial dysplasia reconstruction. Surgeons must be adept at recognizing and managing these issues.
Common Complications and Management Strategies
| Complication | Incidence (%) | Salvage Strategy |
|---|---|---|
| Recurrence of Radial Deviation | 30-70 |
Description:
The most frequent and often inevitable complication, particularly with growth, due to persistent muscle imbalance and residual radial-sided soft tissue tethering.
Management: Initial conservative management with serial casting and dynamic bracing. For significant recurrence affecting function, revision centralization/radialization, repeat soft tissue releases, further tendon transfers (e.g., ECU or FCU rerouting), or external fixation with gradual correction may be necessary. Repeated osteotomy is an option in mature patients. |
| Wrist Stiffness / Limited ROM | Common |
Description:
Reduced flexion/extension and forearm rotation, impacting functional grasp.
Management: Intensive and prolonged physical and occupational therapy, dynamic splinting. If severe and recalcitrant, revision capsulotomy or arthrolysis may be considered, though this is rare in pediatric patients. The primary goal is stability and alignment, not necessarily full ROM. |
| Ulnar Growth Arrest / Deformity | Variable |
Description:
Accidental physeal damage from K-wire insertion during initial surgery, leading to premature cessation of ulnar growth or angular deformity.
Management: If mild, observation. For significant growth arrest leading to progressive forearm length discrepancy or ulnar bowing, future ulnar osteotomy (corrective or lengthening via distraction osteogenesis) may be required. Epiphysiodesis of the contralateral ulna might be considered in severe, bilateral cases at skeletal maturity. |
| Median Nerve Compression / Injury | 5-10 |
Description:
Intraoperative injury during dissection or postoperative compression from swelling or excessive tension after correction. Can lead to transient or permanent median nerve palsy.
Management: Meticulous intraoperative neurolysis and protection. Postoperatively, immediate cast splitting/removal if symptoms develop. Surgical decompression (neurolysis) if persistent or severe. Early recognition is crucial. |
| Skin Necrosis / Wound Breakdown | Variable |
Description:
Due to excessive tension on the skin flaps after correction, particularly in patients with pre-existing skin tightness.
Management: Local wound care, serial debridement. If significant, requires V-Y plasty, local flap coverage, or skin grafting. Prevention through adequate skin release and avoiding excessive tension is key. |
| Infection (Superficial/Deep) | 1-5 |
Description:
Superficial cellulitis or deep surgical site infection, potentially involving hardware.
Management: Systemic antibiotics (initially broad-spectrum, then culture-directed). Superficial infections may resolve with antibiotics. Deep infections often require surgical debridement and hardware removal, with repeat fixation if stability is lost. |
| Pin Tract Infection (External Fixation) | High (superficial) |
Description:
Inflammation or infection around external fixator pins. Common with prolonged use.
Management: Meticulous pin site care, oral or topical antibiotics for superficial infections. Deep infections may necessitate pin removal and exchange. |
| Fracture (Ulna) | Rare |
Description:
Intraoperative iatrogenic fracture during forceful manipulation or postoperative fracture due to weakened bone (e.g., after osteotomy).
Management: Internal fixation (plate and screws) or cast immobilization, depending on the fracture pattern and patient age. |
| Nonunion / Delayed Union | Low |
Description:
Failure of an osteotomy site to heal, particularly with distraction osteogenesis.
Management: Revision fixation, bone grafting, prolonged external fixation, or stimulation (e.g., pulsed electromagnetic fields). |
| Cosmetic Dissatisfaction | Common |
Description:
Persistent forearm shortening, residual wrist deformity, or visible scars.
Management: Counseling and realistic expectation setting. Further procedures like forearm lengthening can address length discrepancy, but a completely normal appearance is often unachievable. |
General Management Principles
- Early Recognition: Vigilant post-operative monitoring for signs of complications.
- Conservative Measures First: Many complications, especially mild recurrences or stiffness, can initially be managed with physical therapy, splinting, and observation.
- Patient and Family Education: Ongoing communication about potential complications and their management strategies is essential for compliance and shared decision-making.
- Multidisciplinary Approach: Collaboration with hand therapists, pediatricians, geneticists, and other specialists is crucial for comprehensive care.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful outcomes in radial dysplasia reconstruction. It aims to maintain surgical correction, prevent stiffness, improve functional range of motion, and optimize strength and overall hand function.
Immediate Post-Operative Phase (0-6/8 Weeks)
-
Immobilization:
- The limb is typically immobilized in a long-arm cast for 6 to 8 weeks, maintaining the wrist in neutral to slight ulnar deviation (approximately 10-15 degrees) and the elbow at 90 degrees of flexion. This protects the surgical site, allows for initial soft tissue healing, and prevents early recurrence of radial deviation.
- The cast is meticulously molded to ensure proper position and avoid pressure points, especially over the median nerve.
-
K-wire Removal:
- K-wires are typically removed in clinic or under light sedation at 6 to 8 weeks post-surgery, once radiographic evidence of initial soft tissue stability and/or bone healing (if osteotomy was performed) is observed.
-
Pain Management:
- Appropriate pediatric pain management protocols are instituted, involving analgesics and close monitoring.
-
Monitoring:
- Regular checks for neurovascular status, signs of infection, and cast integrity are essential. Swelling can lead to median nerve compression if not addressed promptly.
Early Mobilization Phase (6/8 Weeks - 6 Months)
Once K-wires are removed and initial healing is sufficient, a structured rehabilitation program with a hand therapist begins.
1.
Custom Splinting:
* A custom-molded thermoplastic resting splint (often a forearm-based splint that maintains the wrist in neutral to slight ulnar deviation) is fabricated. This splint is worn primarily at night and during periods of rest to maintain correction and prevent contracture recurrence.
* Dynamic splinting may be introduced later to assist with specific range of motion gains.
2.
Range of Motion (ROM) Exercises:
*
Active-Assisted and Active ROM:
Gently initiate active-assisted and active exercises for wrist flexion/extension, ulnar/radial deviation (within limits of stabilization), and forearm pronation/supination. The focus is on controlled, pain-free movement.
*
Finger and Thumb ROM:
Maintain full, active ROM of the fingers and thumb, emphasizing gentle stretching if thumb reconstruction has been performed.
*
Elbow ROM:
Continue full active elbow flexion and extension.
3.
Scar Management:
* Gentle scar massage, silicone sheeting, or topical creams are initiated to prevent scar hypertrophy and improve pliability.
4.
Edema Control:
* Elevation and gentle retrograde massage can help manage residual swelling.
Strengthening & Functional Integration Phase (6 Months - 1 Year+)
As ROM improves, the focus shifts to strengthening and integrating the limb into functional activities.
1.
Strengthening Exercises:
* Gradually introduce isometric and isotonic strengthening exercises for the wrist, forearm, and hand musculature. This includes grip strengthening, pinch strength, and exercises targeting the transferred tendons (if applicable).
* Thera-bands, light weights, and putty can be used.
2.
Functional Activities:
* Incorporate activities that promote bilateral hand use, object manipulation, and fine motor skills.
* Encourage participation in age-appropriate play and daily tasks, adapting as needed.
3.
Proprioception and Coordination:
* Exercises to improve proprioception and coordination of the hand and wrist.
4.
Long-Term Splinting:
* Night splinting is often continued for several years, or until skeletal maturity, to minimize the risk of recurrence of radial deviation, especially during periods of rapid growth.
5.
Monitoring for Recurrence:
* Regular clinical and radiographic follow-up appointments are crucial to monitor for signs of recurrence of radial deviation, forearm length discrepancy, or other growth-related issues.
* Adjustments to splinting or therapy protocols are made based on findings.
Special Considerations
- Distraction Osteogenesis: If external fixation was used for lengthening, the rehabilitation protocol will be significantly longer and more intensive, involving daily fixator adjustments, meticulous pin site care, and progressive weight-bearing/ROM exercises after fixator removal.
- Pollicization: If pollicization was performed, a separate but coordinated rehabilitation program will be necessary, focusing on thumb opposition, pinch, and grip strength.
- Psychosocial Support: Ongoing psychosocial support for the child and family is important, addressing body image, functional limitations, and integration into social activities.
The long-term success of radial dysplasia reconstruction is heavily dependent on a consistent and dedicated rehabilitation program, often requiring years of commitment from the patient, family, and rehabilitation team.
Summary of Key Literature / Guidelines
The management of radial dysplasia has evolved significantly, guided by seminal contributions and ongoing research. The primary objective remains to improve both functional utility and aesthetic appearance of the affected limb.
Seminal Works and Classification
The foundation for contemporary understanding and surgical planning was laid by Bayne and Klug (1987) , whose radiographic classification system (Types I-IV, with Type 0 sometimes added) remains the gold standard for guiding surgical decisions. Prior contributions by Bora (1970) highlighted the importance of soft tissue releases and centralization. Buck-Gramcko (1971) also contributed significantly, particularly to the concepts of pollicization for thumb aplasia. These early works underscored the complex interplay of skeletal and soft tissue pathology.
Centralization vs. Radialization
The debate between centralization and radialization has largely settled in favor of
centralization
for most cases.
*
Centralization
, first described by Sayre (1893) and popularized by Bora and Bayne, involves placing the carpus directly over the distal ulna. This technique aims to create a more balanced wrist joint, potentially reducing the risk of progressive ulnar deviation seen with radialization. Studies by Manske et al. (1995) and Watson et al. (2009) have demonstrated favorable long-term outcomes with centralization, emphasizing improved stability and functional range of motion, though recurrence of radial deviation remains a challenge.
*
Radialization
, where the ulna is placed more ulnar to the midline of the carpus, can achieve excellent initial correction but historically had a higher rate of long-term ulnar deviation or wrist stiffness. It is now less commonly performed as a primary procedure.
Role of Tendon Transfers
Dynamic tendon transfers, particularly the extensor carpi ulnaris (ECU) transfer to the radial side of the carpus, have become an integral part of centralization procedures. The rationale is to create active muscle balance across the wrist joint, counteracting the deforming forces and reducing the rate of recurrence. Louis et al. (1997) and Goldfarb et al. (2007) have reported on the efficacy of ECU transfers in maintaining correction and improving functional outcomes.
Timing of Surgery
Current consensus suggests that primary wrist centralization is best performed between 6 and 12 months of age . This timing allows for adequate size of the structures for surgical manipulation, while intervening before rigid contractures fully develop and before the child becomes too large to be effectively casted. Early intervention also aims to normalize the limb for bimanual activities during critical developmental periods.
Management of Forearm Length Discrepancy and Ulnar Bowing
For significant forearm length discrepancy and severe ulnar bowing, distraction osteogenesis using external fixators has become a viable option. Vilkki (1995) pioneered the "Vilkki procedure," a comprehensive, often staged, approach combining vascularized toe phalanx transfer for radial reconstruction and gradual lengthening with distraction. While technically demanding and associated with its own set of complications (e.g., pin tract infections, nerve irritation), distraction osteogenesis can significantly improve forearm length and correct ulnar bowing, enhancing overall limb function and cosmesis.
Long-Term Outcomes and Recurrence
Despite advances, recurrence of radial deviation remains the most common long-term issue, reported in 30-70% of cases. This is often attributed to persistent muscle imbalance, continued growth, and scar contracture. Long-term follow-up studies, such as those by James et al. (2007), underscore the need for prolonged bracing and potential revision surgeries. Functional outcomes generally show improved stability and a more neutral wrist position, but full range of motion is rarely achieved. Patient-reported outcomes (PROs) are increasingly recognized as important measures of success, focusing on the child's ability to participate in activities of daily living and social interactions.
Current Controversies and Future Directions
- Ulnar Epiphysiodesis: The role of temporary or permanent distal ulnar epiphysiodesis to prevent ulnar overgrowth is debated due to the risk of exacerbating forearm shortening. Most surgeons prefer to address length discrepancies with later distraction osteogenesis rather than risking growth arrest.
- Vascularized Epiphyseal Transfers: While experimental, vascularized physeal transfers from other sites (e.g., second metatarsal) aim to replace the missing radial epiphysis and provide biological growth potential. Clinical application remains limited to highly specialized centers.
- Tissue Engineering: Research into tissue-engineered cartilage or bone substitutes for radial reconstruction holds promise but is still in early developmental stages.
- Advanced Imaging: The increased use of 3D printing from CT/MRI data for presurgical planning offers enhanced precision for complex anatomical reconstructions.
In conclusion, the surgical management of radial dysplasia has matured into a systematic approach, combining soft tissue releases, skeletal centralization, and dynamic stabilization with tendon transfers. While significant functional and cosmetic improvements are achievable, a comprehensive understanding of the associated syndromes, meticulous surgical technique, and a dedicated, long-term rehabilitation strategy are essential for optimizing patient outcomes. Continuous research and refinement of techniques are vital to further address the inherent challenges of this complex congenital anomaly.
Clinical & Radiographic Imaging



You Might Also Like

