Syndactyly and Macrodactyly: Operative Orthopaedic Techniques
Key Takeaway
Congenital toe deformities, including syndactyly, polydactyly, and macrodactyly, present unique reconstructive challenges. While syndactyly rarely impairs foot mechanics, macrodactyly often necessitates complex surgical intervention due to progressive hypertrophy and shoe-wear difficulties. This comprehensive guide details evidence-based operative strategies, including staged soft-tissue debulking, phalangeal epiphysiodesis, ray reduction, and ray amputation, providing orthopaedic surgeons with precise, step-by-step techniques to optimize both functional and cosmetic outcomes in pediatric patients.
INTRODUCTION TO CONGENITAL TOE ANOMALIES
Congenital anomalies of the foot, encompassing syndactyly, polydactyly, and macrodactyly, represent a complex spectrum of developmental disorders that require meticulous clinical evaluation and tailored surgical strategies. Unlike congenital anomalies of the hand, where fine motor function and independent digit articulation are paramount, the primary biomechanical imperatives of the foot are stable weight-bearing, ambulation, and the accommodation of standard footwear. Consequently, surgical decision-making in the pediatric foot is heavily weighted toward achieving a plantigrade, pain-free foot that fits comfortably into a shoe, with cosmetic considerations playing a secondary, though still significant, role.
SYNDACTYLY OF THE TOES
Pathoanatomy and Clinical Presentation
Syndactyly, the failure of differentiation or separation of adjacent digits, is one of the most common congenital malformations of the foot. It occurs due to a failure of apoptosis within the apical ectodermal ridge during the sixth to eighth weeks of gestation. In the foot, the second and third toes are most frequently involved.
Unlike syndactyly of the fingers, which severely restricts independent digit motion and grasp, syndactyly of the toes rarely interferes with the biomechanical function of the foot. The tethering of adjacent toes does not significantly alter the propulsive phase of the gait cycle, nor does it typically cause pain.
Indications for Surgery
Because functional impairment is exceedingly rare, surgical intervention for pedal syndactyly is indicated almost exclusively for cosmetic reasons or psychological distress experienced by the patient or parents.
Clinical Pearl: Routine surgical release of simple, incomplete syndactyly of the toes is generally discouraged. Surgeons must counsel parents extensively that the risks of surgery—including web creep, scar contracture, neurovascular injury, and graft failure—often outweigh the purely cosmetic benefits.
When surgery is elected, the operative principles mirror those utilized in the hand. The reconstruction requires the creation of a robust, skin-lined commissure, typically achieved via dorsal and plantar interdigitating zigzag flaps, supplemented by full-thickness skin grafts harvested from the groin or hypothenar eminence to cover the inevitable lateral defects of the newly separated digits.
POLYDACTYLY OF THE FOOT
While the primary text focuses on syndactyly and macrodactyly, the presence of supernumerary digits (polydactyly) frequently co-occurs or presents similar reconstructive challenges. Polydactyly is broadly categorized based on the anatomical location of the duplication.
Venn-Watson Classification
The Venn-Watson classification system provides a structural framework for understanding pedal polydactyly, dividing it primarily into preaxial (medial/tibial side) and postaxial (lateral/fibular side) duplications.
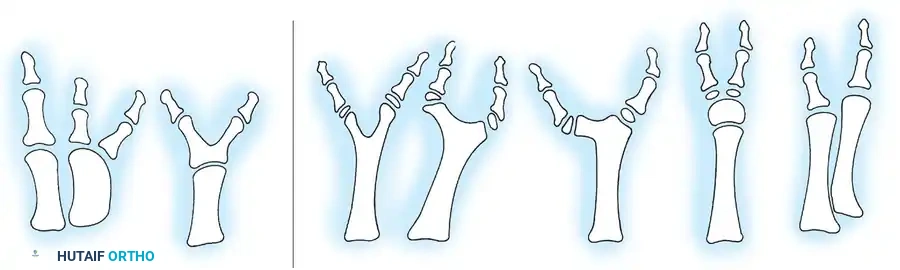
Fig. 26-3 Venn-Watson classifi cation of polydactyly. A, Preaxial polydactyly. B, Postaxial polydactyly. (Redrawn from Venn-Watson EA: Problems in polydactyly of the foot, Orthop Clin North Am 7:909, 1976.)
Postaxial polydactyly is the most common variant. The duplication may range from a rudimentary soft-tissue appendage (Type A) to a fully developed digit with its own metatarsal articulation (Type B).
Surgical Management of Polydactyly
The goal of surgery is to excise the supernumerary digit while preserving the normal contour of the foot and ensuring a stable metatarsophalangeal (MTP) joint for the retained digit.
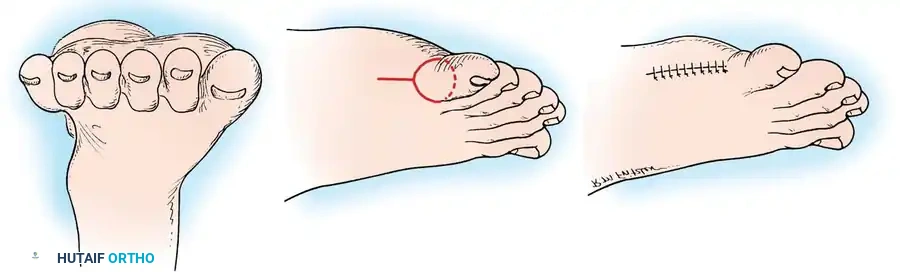
Fig. 26-4 Polydactyly. A, Front view of foot. B, Outline of incision passing through web space between fi fth and sixth toes and extending in racquet-shaped incision along lateral border of foot. C, Surgical excision of supernumerary digit.
Surgical Approach:
1. Incision: A racquet-shaped incision is outlined at the base of the supernumerary digit. The handle of the racquet extends proximally along the lateral border of the foot to allow access to the metatarsal articulation.
2. Dissection: The incision is deepened, and the neurovascular bundles supplying the duplicated digit are identified, ligated, and transected.
3. Capsular Management: The capsule of the MTP joint is carefully incised. It is critical to preserve the collateral ligaments and intrinsic muscle attachments of the retained digit to prevent postoperative angular deformities (e.g., a varus drift of the fifth toe).
4. Excision and Closure: The supernumerary bone is excised. The capsule is imbricated, and the skin is closed with interrupted non-absorbable sutures.
MACRODACTYLY OF THE FOOT
Pathophysiology and Associated Syndromes
Macrodactyly is a rare, complex congenital anomaly characterized by the disproportionate hypertrophy of all mesenchymal elements of a digit, including bone, tendon, nerve, fat, and skin. It is not merely a localized gigantism but a progressive hamartomatous overgrowth. The condition may be static (growing proportionally with the child) or progressive (growing at a faster rate than the rest of the body).
Macrodactyly is frequently associated with systemic overgrowth syndromes and neurocutaneous disorders, most notably:
* Neurofibromatosis Type 1 (NF1): Often presents with plexiform neurofibromas and localized gigantism.
* Klippel-Trenaunay-Weber Syndrome: Characterized by the triad of capillary malformations (port-wine stains), venous varicosities, and bony/soft-tissue hypertrophy.
* Congenital Lipofibromatosis: Massive infiltration of mature adipose tissue within the epineurium of peripheral nerves.
* Proteus Syndrome: Asymmetric, disproportionate overgrowth.

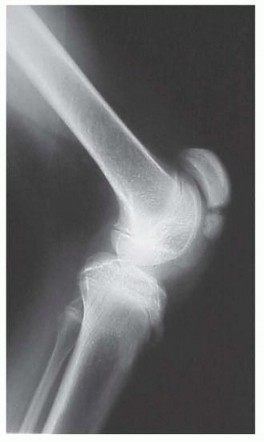
Fig. 26-5 A, Macrodactyly in 2-year-old child with Klippel-Trenaunay-Weber syndrome.

Fig. 26-5 B, Anteroposterior radiograph; note soft-tissue hypertrophy of second and third ray phalanges.

Fig. 26-5 C, Clinical appearance of macrodactyly in another child.
Clinical Evaluation and Indications for Surgery
The primary indications for surgical intervention in macrodactyly are functional impairment and severe cosmetic deformity. The hypertrophied digits frequently cause intractable pain, recurrent ulceration due to pressure, and a profound inability to fit into standard footwear. The cosmetic goal is to alter the grotesque appearance of the foot, achieving a size and contour that approximates the contralateral, unaffected foot.
Surgical Warning: The recurrence rate following simple soft-tissue debulking of a single macrodactylic digit is virtually 100%. Surgeons must employ a combination of osseous shortening, physeal ablation, and aggressive soft-tissue resection to achieve durable results.
Evidence-Based Surgical Strategies
The literature describes a multitude of operative procedures, reflecting the challenging nature of this condition. Options include reduction syndactyly, soft-tissue debulking combined with ostectomy or epiphysiodesis, toe amputation, and complete ray amputation.
- Grogan et al. demonstrated that the most reliable and durable results in patients with congenital lipofibromatosis and pedal macrodactyly were achieved through ray amputation, combined with phalangeal epiphysiodesis and debulking of adjacent rays. They noted that syndactylization and simple phalangeal resection yielded inferior outcomes.
- Chang et al. corroborated these findings, reporting superior cosmetic and functional results with ray resection compared to isolated toe amputation. However, they highlighted a critical caveat: when the great toe (first ray) is involved, ray resection yields only fair results due to the severe disruption of the medial column's weight-bearing mechanics. In such cases, repeated soft-tissue debulking and joint-preserving bone shortening are preferred.
- Topoleski et al. evaluated the efficacy of open epiphysiodesis combined with debulking in less severe cases. In a cohort with an average age of 3.7 years, they found that the overall length of the proximal phalanx did not increase over a 2-year follow-up, suggesting that early physeal arrest is a viable strategy for halting progressive longitudinal overgrowth.
Staged Soft-Tissue Debulking and Bone Shortening (Kotwal and Farooque Technique)
For digits where preservation is desired and overgrowth is moderate, Kotwal and Farooque described a highly effective staged procedure.
Stage 1: Unilateral Defatting
1. A mid-axial incision is made on the convex side of the deformed digit.
2. Aggressive defatting and excision of fibrofatty tissue are performed, taking care to preserve the neurovascular bundle on the operative side.
3. This stage typically achieves a 10% to 20% reduction in digital girth.
Stage 2: Contralateral Defatting and Osseous Shortening (3 Months Later)
1. A mid-axial incision is made on the contralateral side of the digit.
2. Further soft-tissue debulking is performed.
3. Bone Resection: An entire phalanx (typically the middle or proximal phalanx, depending on the locus of maximum hypertrophy) is excised subperiosteally.
4. Capsulorrhaphy: The capsules of the adjacent joints are meticulously sutured together to close the dead space and provide stability.
5. Stabilization: A smooth longitudinal Kirschner wire (K-wire) is driven retrograde from the distal phalanx across the newly approximated joint space into the proximal bone.
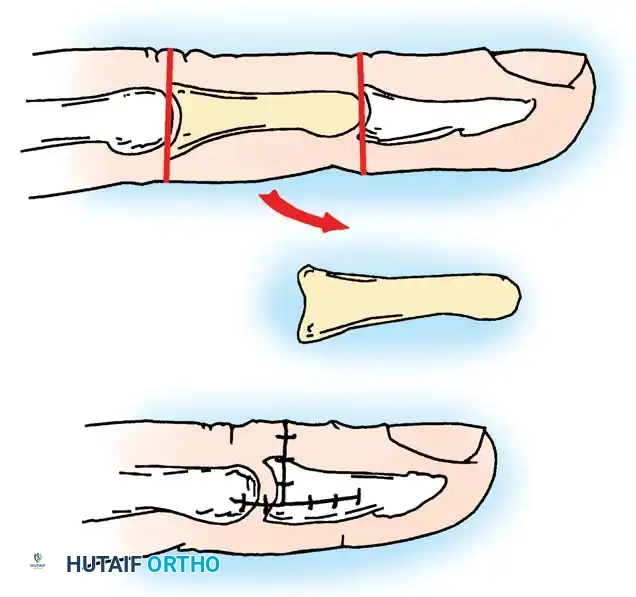
Fig. 26-6 Bone shortening with removal of whole phalanx for macrodactyly. (From Kotwal PP, Farooque M: Macrodactyly, J Bone Joint Surg 80B:651, 1998.)
Outcomes: At an average 9-year follow-up, this staged approach yielded good results (≥ 50% reduction in volume) in 57% of patients, and satisfactory results in 33%.
OPERATIVE TECHNIQUES FOR MACRODACTYLY
Technique 26-2: Ray Reduction
Ray reduction is indicated for moderate to severe macrodactyly where the entire ray (metatarsal and phalanges) is hypertrophied, but the surgeon aims to preserve the digit to maintain forefoot width and cosmetic appearance.
Preoperative Preparation:
* The patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position.
* A pneumatic thigh tourniquet is applied.
* Prophylactic intravenous antibiotics are administered.
Surgical Steps:
1. Incision Planning: Outline dorsal skin incisions along the longitudinal axis of the ray to be reduced. Depending on the extent of the hypertrophy, this may be a single long incision or multiple small, staggered incisions along the metatarsal and phalanges to prevent linear scar contracture.
2. Soft-Tissue Debulking: Deepen the incision through the subcutaneous tissues. Meticulously debulk the hypertrophic fibrofatty tissue.
> Pitfall: The digital nerves in macrodactyly are often massively enlarged, tortuous, and infiltrated with fat. Extreme caution must be exercised to identify and protect the digital neurovascular bundles during debulking to prevent distal ischemia and neuroma formation.
3. Metatarsal Osteotomy: Expose the metatarsal neck subperiosteally. Perform a transverse or step-cut osteotomy at the metatarsal neck. Shorten the metatarsal by resecting a cylindrical segment of bone of sufficient length to match the distal extent of this metatarsal head to the adjacent, normal metatarsal heads (restoring the normal metatarsal parabola).
4. Physeal Arrest (Epiphysiodesis): If the child is still growing, surgically fuse the physis at the level of the metatarsal head using a curette or high-speed burr to prevent recurrent longitudinal overgrowth.
5. Phalangeal Shortening: If the phalanges are also disproportionately long, repeat the osteotomy and shortening process for the proximal and/or middle phalanges until the entire ray has been reduced to a normal length.
6. Fixation: Insert a smooth, longitudinal Kirschner wire (typically 0.045 or 0.062 inches) retrograde from the tip of the toe, across the interphalangeal and MTP joints, and into the base of the metatarsal to align and stabilize the reconstructed ray.
7. Closure: Deflate the tourniquet and secure meticulous hemostasis. Close the wound with interrupted non-absorbable sutures.
Postoperative Protocol (Ray Reduction):
* Apply a sterile, non-adherent dressing and a well-padded short leg cast.
* The patient is kept strictly non-weight-bearing.
* The Kirschner wire is removed in the clinic at 6 weeks postoperatively.
* Following pin removal, the patient is transitioned to a short leg walking cast or a controlled ankle motion (CAM) boot for an additional 6 weeks to ensure complete osseous union.
Technique 26-3: Ray Amputation
Ray amputation is the procedure of choice for massive, grotesque enlargement of the bone and soft tissues that precludes shoe wear, or for severe recurrences following previous attempts at reduction syndactyly or soft-tissue debulking.
Surgical Warning: Resection of the second ray removes the "keystone" of the transverse metatarsal arch. This frequently leads to a progressive hallux valgus deformity as the first toe drifts laterally into the void. Parents must be counseled that subsequent surgical correction (e.g., first metatarsal osteotomy) may be required during adolescence.
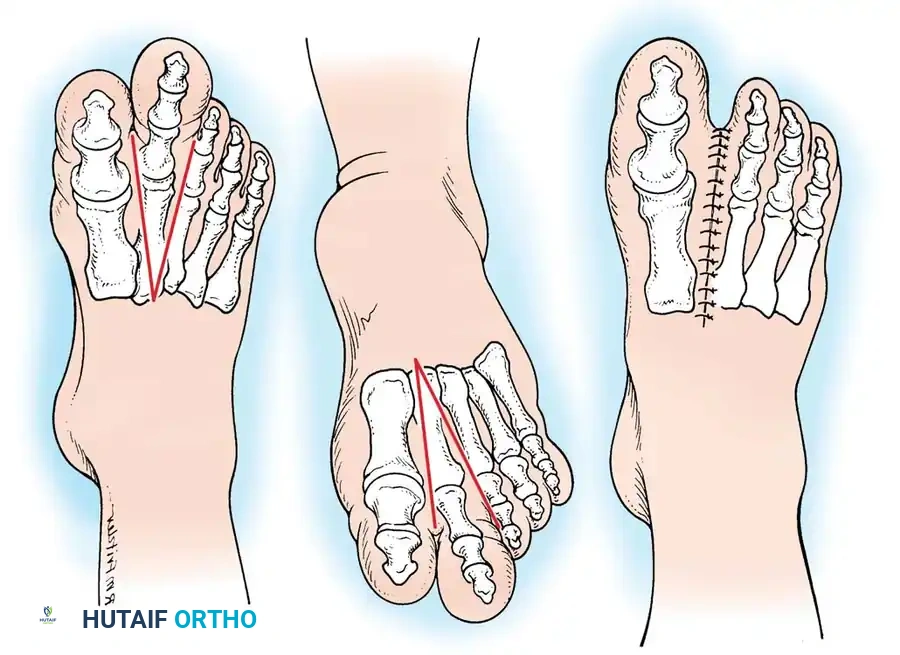
Fig. 26-7 Ray amputation for macrodactyly. A, Incision on dorsal surface of foot. B, Plantar incision. C, Closed incision after amputation.
Surgical Steps:
1. Incision Planning: Outline the ray to be amputated. Design dorsal and plantar V-shaped skin flaps. The apex of the V should be positioned proximally at the base of the metatarsal to be resected.
2. Web Space Incisions: Make dorsal and plantar incisions starting over the MTP joint, with connecting incisions passing through the web spaces of the adjacent, normal toes.
3. Proximal Extension: Continue the incisions proximally, both dorsally and plantarward, converging at the base of the metatarsal (Fig. 26-7).
4. Deep Dissection and Amputation: Deepen the incisions. Identify and ligate the digital arteries and veins supplying the hypertrophied ray.
> Clinical Pearl: Trace the digital nerves proximally and transect them under tension so they retract deep into the intrinsic musculature of the foot, minimizing the risk of a painful symptomatic neuroma on the plantar weight-bearing surface.
5. Bone Resection: Perform an osteotomy at the proximal metaphysis or disarticulate the metatarsal at the tarsometatarsal joint. Amputate the metatarsal, its associated phalanges, and the surrounding hypertrophied soft-tissue envelope en bloc.
6. Deep Transverse Metatarsal Ligament Reconstruction: To prevent splaying of the forefoot, it is imperative to approximate the adjacent metatarsals. Pass a heavy, non-absorbable suture (e.g., #1 or #2 FiberWire) through drill holes in the adjacent metatarsal necks or tightly imbricate the remaining deep transverse metatarsal ligament.
7. Closure: After adequate resection of the hamartomatous tissue and confirmation of hemostasis, close the skin flaps with interrupted sutures. Ensure there is no excessive tension on the skin edges, which could lead to marginal necrosis.
Postoperative Protocol (Ray Amputation):
* A bulky, compressive dressing is applied, followed by a short leg cast to protect the wound and maintain the narrowed forefoot contour.
* The patient remains non-weight-bearing for 3 to 4 weeks to allow for primary soft-tissue healing.
* Sutures are removed at 2 to 3 weeks.
* Protected weight-bearing in a stiff-soled postoperative shoe or CAM boot is initiated and continued until complete healing occurs, typically at 6 to 12 weeks.
* Long-term follow-up is essential to monitor for the development of adjacent toe deformities, particularly hallux valgus if the second ray was resected.
You Might Also Like