Operative Management of Poliomyelitis: Orthopaedic Principles
Key Takeaway
Poliomyelitis causes asymmetrical flaccid paralysis due to viral destruction of anterior horn cells. Orthopaedic management focuses on preventing contractures during the acute and convalescent stages, followed by surgical reconstruction in the chronic stage. Interventions include targeted tendon transfers to restore dynamic balance and arthrodesis for definitive joint stabilization. Successful outcomes rely on strict adherence to biomechanical principles, meticulous surgical technique, and comprehensive postoperative rehabilitation.
Introduction to Poliomyelitis in Orthopaedics
Acute anterior poliomyelitis is a highly infectious viral disease caused by one of three serotypes of the poliovirus, a member of the enterovirus family. The hallmark of the disease is its profound affinity for the central nervous system, specifically localizing in the anterior horn cells of the spinal cord and certain brainstem motor nuclei. While global eradication efforts spearheaded by the World Health Organization (WHO) have drastically reduced its incidence, orthopaedic surgeons must remain intimately familiar with its sequelae. Endemic pockets remain in developing nations, and the orthopaedic management of adult survivors presenting with post-polio syndrome or chronic paralytic deformities continues to be a critical component of reconstructive surgery.
Epidemiology and Immunization
Initial invasion by the virus occurs via the oropharyngeal and gastrointestinal tracts, subsequently spreading to the central nervous system through a hematogenous route. The introduction of the Salk inactivated poliovirus vaccine (IPV) and the Sabin live oral poliovirus vaccine (OPV) revolutionized the epidemiological landscape.
Clinical Pearl: While OPV provides superior intestinal immunity and is crucial for halting wild-type virus circulation in endemic areas, it carries a rare but significant risk of vaccine-associated paralytic poliomyelitis (VAPP). Consequently, in developed nations where wild-type circulation has ceased, exclusive use of IPV is the gold standard to eliminate VAPP while maintaining systemic immunity.
Pathophysiology and Biomechanics of Paralysis
Upon entering the central nervous system, the virus acutely attacks the alpha motor neurons in the anterior horn ganglion cells, with a pronounced predilection for the cervical and lumbar enlargements. The incubation period ranges from 6 to 20 days.
Motor cell destruction occurs through direct viral multiplication, toxic by-products, and secondary ischemic necrosis from surrounding glial edema and hemorrhage. Within 72 hours of cellular death, Wallerian degeneration propagates throughout the length of the affected nerve fibers. Macrophages clear the necrotic debris, and over the ensuing months, the destroyed motor cells are replaced by dense gliosis.
The Threshold of Clinical Weakness
The severity of the resulting asymmetrical flaccid paralysis is directly proportional to the absolute number of lost motor units.
Surgical Warning: According to Sharrard’s seminal topographical studies of the spinal cord, clinical weakness in a specific muscle group only becomes detectable when more than 60% of its innervating anterior horn cells have been irreversibly destroyed.
Paralysis occurs twice as frequently in the lower extremities compared to the upper extremities. The most commonly afflicted muscles include:
* Lower Extremity: Quadriceps femoris, gluteus medius and maximus, tibialis anterior, medial hamstrings, and hip flexors.
* Upper Extremity: Deltoid, triceps brachii, and pectoralis major.
Recovery potential hinges entirely on the survival of damaged, but not destroyed, anterior horn cells and the subsequent collateral sprouting of surviving axons. The vast majority of neurological recovery occurs within the first month, plateauing by 6 months. A muscle that remains completely paralyzed at 6 months will not spontaneously recover.
Clinical Staging and Non-Operative Management
The clinical continuum of poliomyelitis is divided into three distinct stages, each dictating a specific orthopaedic approach.
1. The Acute Stage (7 to 10 Days)
The acute phase is characterized by systemic viremia, encephalomyelitis, and the onset of widespread paralysis. Symptoms include hyperesthesia, severe muscle pain, nuchal rigidity, and asymmetrical loss of deep tendon reflexes.
Management: Treatment is strictly supportive. Absolute bed rest is mandated, as physical exertion during the viremic phase exacerbates motor neuron destruction. The orthopaedic priority is the prevention of contractures through meticulous anatomical positioning. Limbs must be supported with padded footboards, sandbags, and splints to counteract the deforming forces of gravity and unopposed antagonist muscles. Gentle, passive range-of-motion (ROM) exercises are initiated to preserve joint suppleness.
2. The Convalescent Stage (Up to 24 Months)
Beginning 48 hours after defervescence, this stage represents the window of spontaneous neurological recovery.
Management: Physical therapy is the cornerstone of treatment, emphasizing muscle re-education and the prevention of substitution patterns. Muscle strength must be meticulously charted using the Medical Research Council (MRC) grading system every month for the first 6 months, then quarterly.
* Muscles demonstrating >80% return of strength will generally recover fully.
* Muscles with <30% strength at 3 months are considered permanently paralyzed.
Dynamic splinting and orthoses (e.g., Ankle-Foot Orthoses [AFOs], Knee-Ankle-Foot Orthoses [KAFOs]) are utilized to prevent overstretching of paralyzed muscles and to control dynamic joint instability. Mild contractures are managed with serial casting, while persistent contractures (>6 months) may require percutaneous fascial releases or tendon lengthenings.
3. The Chronic Stage (>24 Months)
The chronic stage marks the cessation of spontaneous recovery. The orthopaedic focus shifts to definitive surgical reconstruction to maximize functional independence, correct fixed deformities, and eliminate the need for cumbersome orthoses.
Principles of Tendon Transfers in Poliomyelitis
Tendon transfers are the workhorse of paralytic reconstruction. They are indicated when dynamic muscle imbalance causes progressive deformity or significantly impairs gait and upper extremity function. Surgery must be delayed until the chronic stage, ensuring no further spontaneous recovery will occur.
To achieve predictable outcomes, the surgeon must adhere to the following absolute biomechanical principles:
- Adequate Strength: A transferred muscle universally loses at least one full MRC grade of power following transposition. Therefore, the donor muscle must have a preoperative rating of Grade 4 (Good) or Grade 5 (Normal). Transferring a weakened muscle guarantees failure.
- Direct Line of Pull: The tendon must be routed as directly as possible from its origin to its new insertion. Acute angles diminish mechanical advantage and increase friction.
- Amplitude and Excursion: The donor tendon should possess a natural excursion similar to the paralyzed muscle it is replacing.
- Supple Joints: A tendon transfer cannot overcome a fixed bony or soft-tissue contracture. All contractures must be completely released prior to, or concurrent with, the transfer.
- Preservation of Neurovascular Supply: The neurovascular pedicle of the donor muscle must be meticulously protected during mobilization. Excessive tension or kinking of the pedicle will result in ischemic necrosis of the transfer.
- Optimal Tissue Bed: The tendon must be routed through healthy, gliding tissues (e.g., subcutaneous fat or native tendon sheaths). Routing through fascial defects or bare bone tunnels invites dense adhesions.
- Secure Fixation and Tensioning: The tendon must be securely anchored to bone (via interference screws, suture anchors, or transosseous tunnels) under slightly greater than resting tension. Insufficient tension wastes muscle contraction on taking up slack.
- Synergism and Phasic Activity: Muscles are categorized by their activity during the gait cycle (stance phase vs. swing phase).
Biomechanical Principle: Phasic transfers (e.g., substituting a swing-phase muscle for another swing-phase muscle) are highly successful and require minimal cortical retraining. Non-phasic transfers can undergo "phasic conversion" through extensive postoperative physical therapy, but mixing swing and stance phase transfers in a single procedure significantly increases the failure rate.
Regional Surgical Reconstruction
The Foot and Ankle
The foot and ankle are the most common sites of paralytic deformity. Imbalances between the dorsiflexors, plantarflexors, invertors, and evertors rapidly lead to complex, multiplanar deformities.

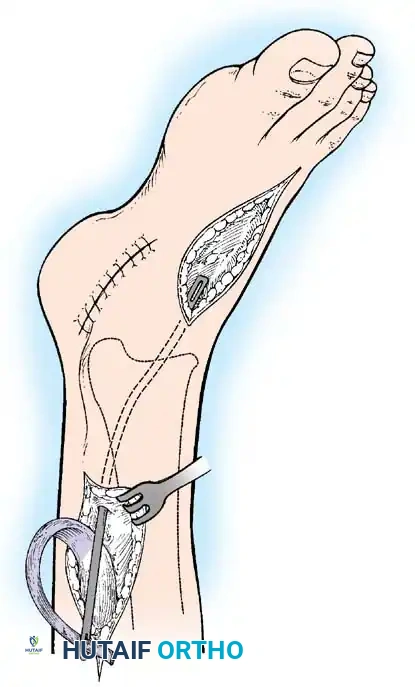
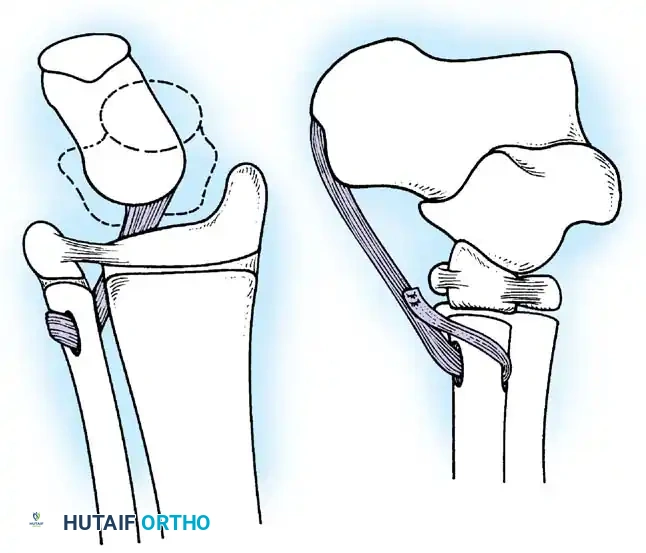
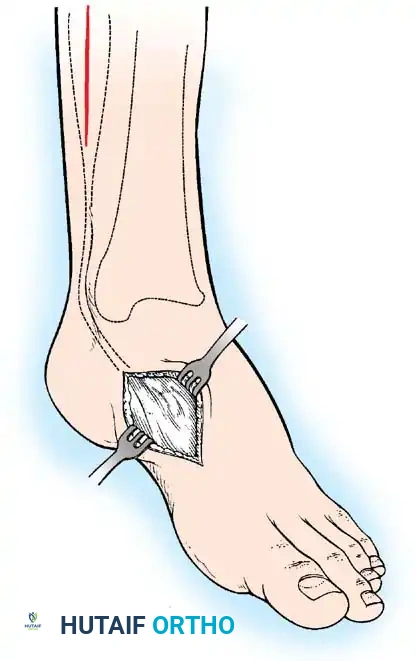
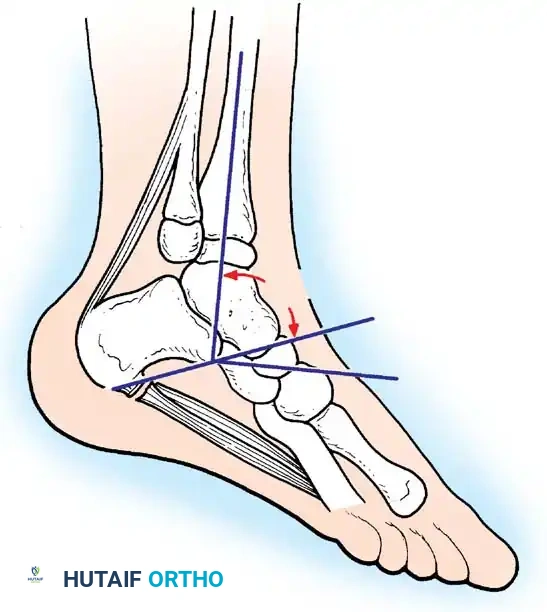
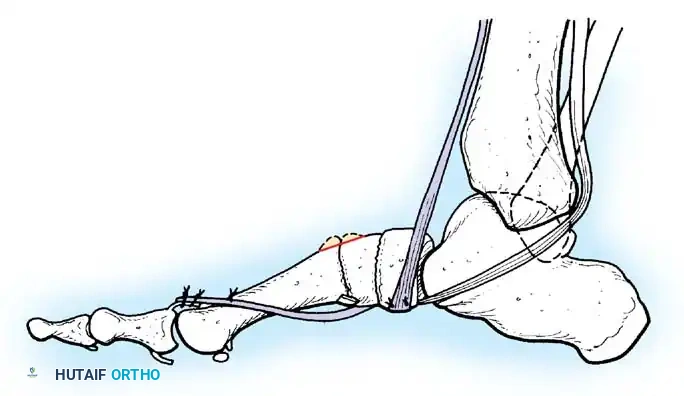
Paralytic Equinus:
Caused by paralysis of the anterior tibial muscles with sparing of the triceps surae. If dynamic, it is managed with a posterior tibial tendon transfer through the interosseous membrane to the dorsum of the foot.
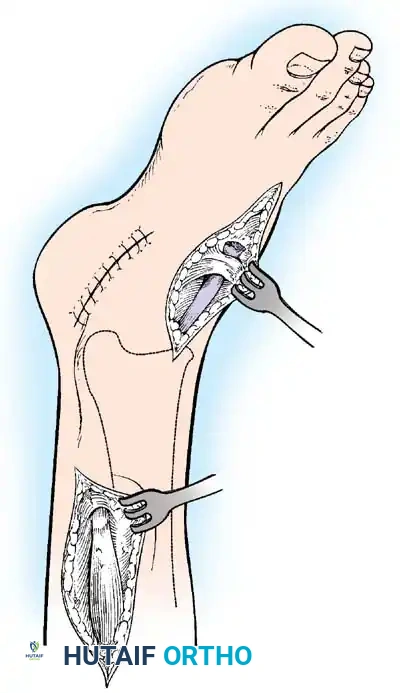
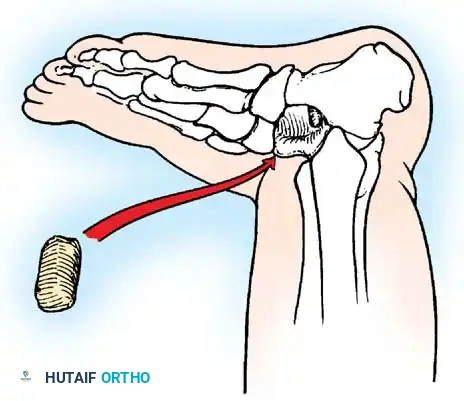
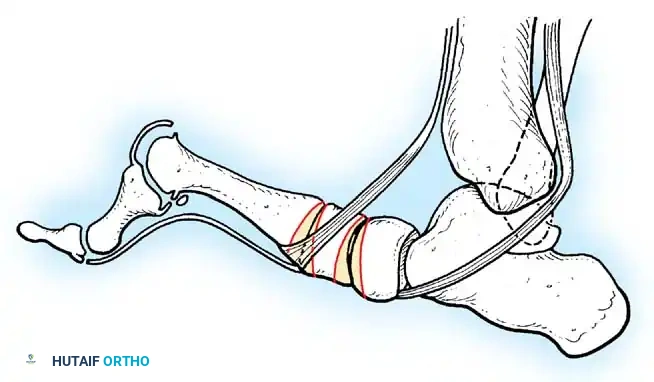
Paralytic Calcaneus:
A devastating deformity resulting from triceps surae paralysis. The unopposed dorsiflexors pull the foot into calcaneus, while the intrinsic muscles and plantar fascia contract, creating a calcaneocavus deformity. Reconstruction requires plantar fascia release, followed by transfer of the tibialis posterior, peroneus longus, and flexor hallucis longus to the os calcis to restore plantarflexion power.
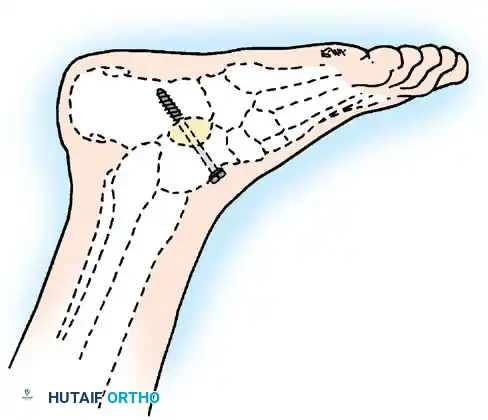
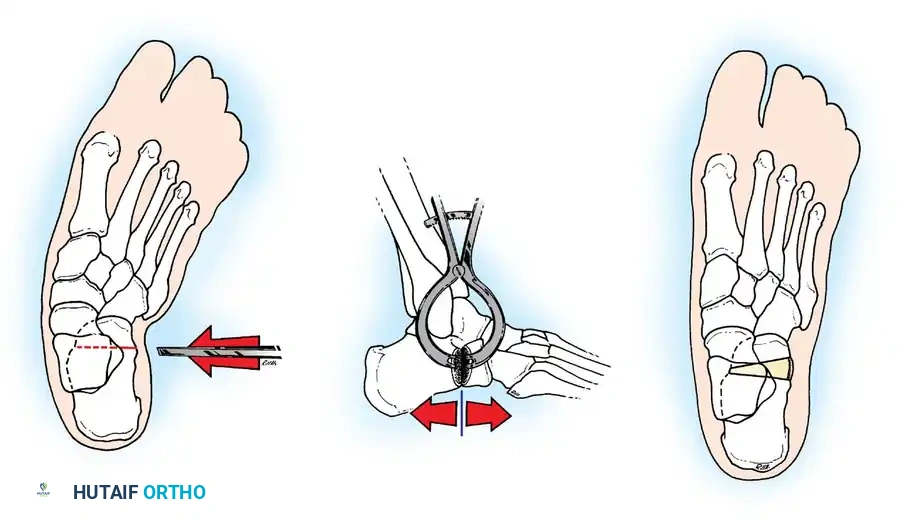
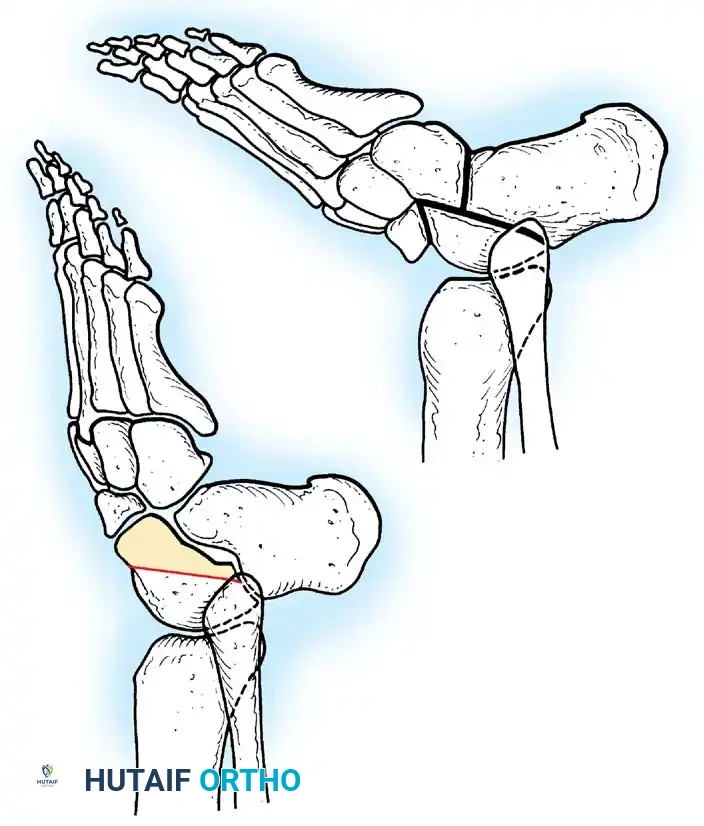
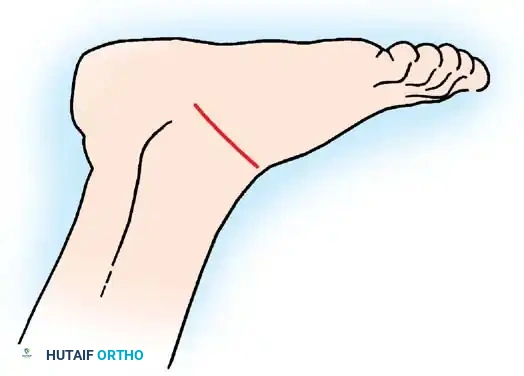
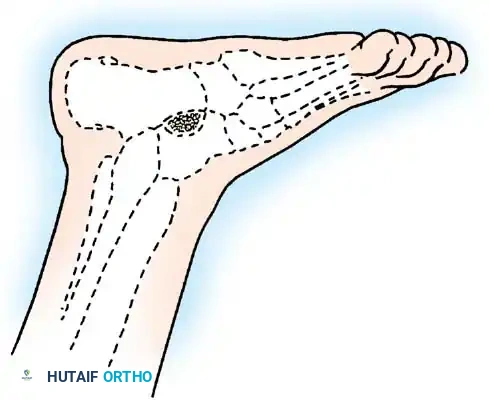
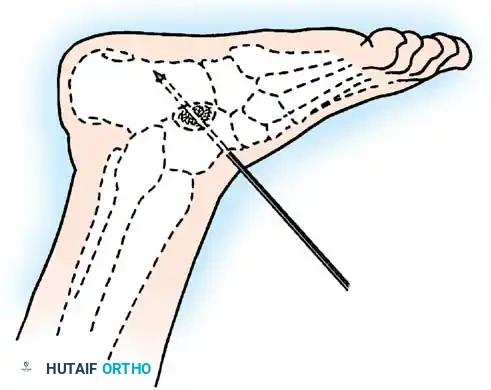
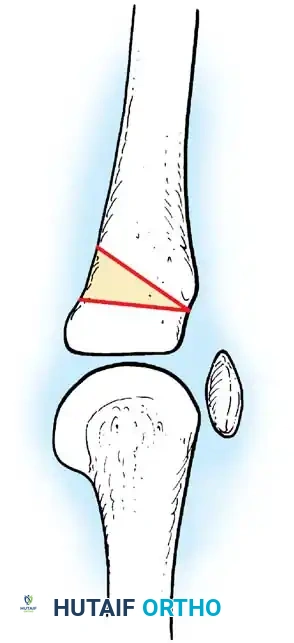
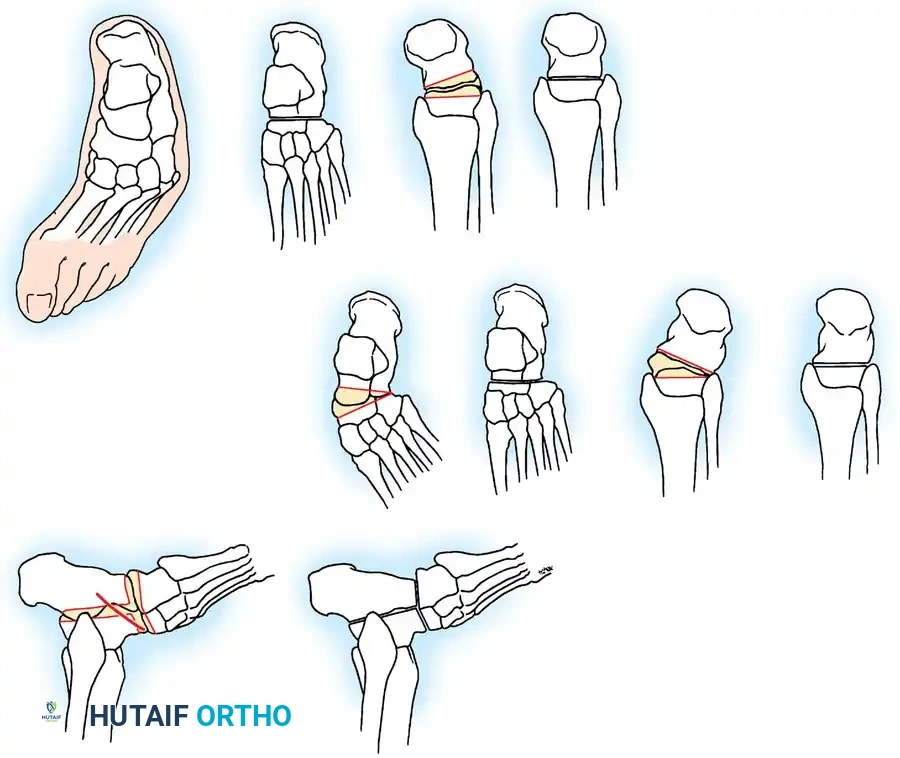
Arthrodesis of the Foot:
In adults or older adolescents with fixed, static deformities, tendon transfers alone are insufficient. The Triple Arthrodesis (fusion of the subtalar, calcaneocuboid, and talonavicular joints) is the definitive procedure for stabilizing a flail hindfoot and midfoot.
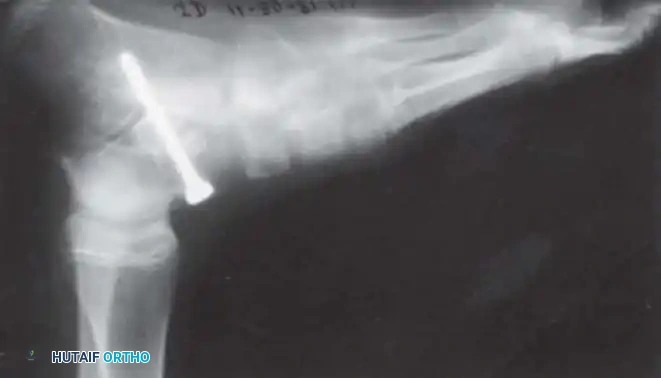
Surgical Warning: In growing children, bony procedures should be delayed until skeletal maturity (typically >12 years of age) to prevent severe growth arrest and secondary deformities. Extra-articular subtalar arthrodesis (Grice-Green procedure) can be utilized in younger children to stabilize the hindfoot without violating the physes.
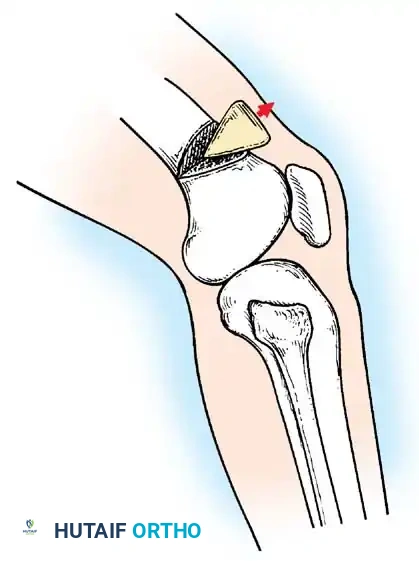
The Knee
Paralysis of the quadriceps femoris is a profound disability, forcing the patient to manually lock the knee into hyperextension (genu recurvatum) during the stance phase to prevent buckling.
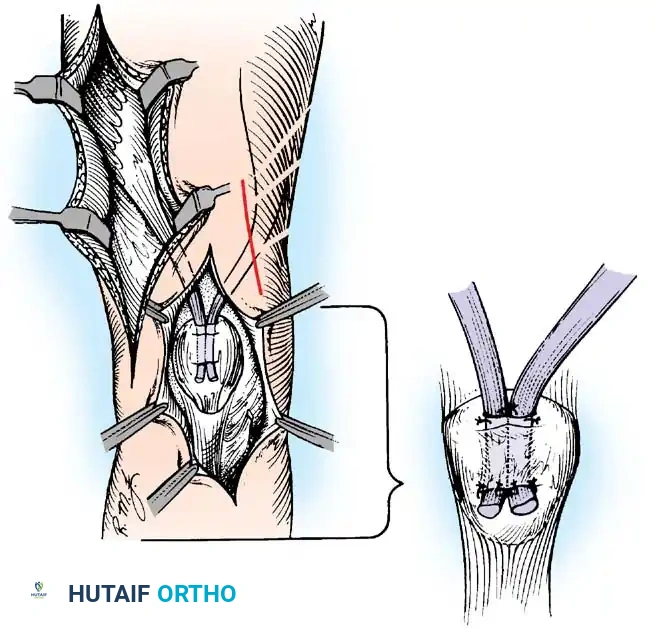
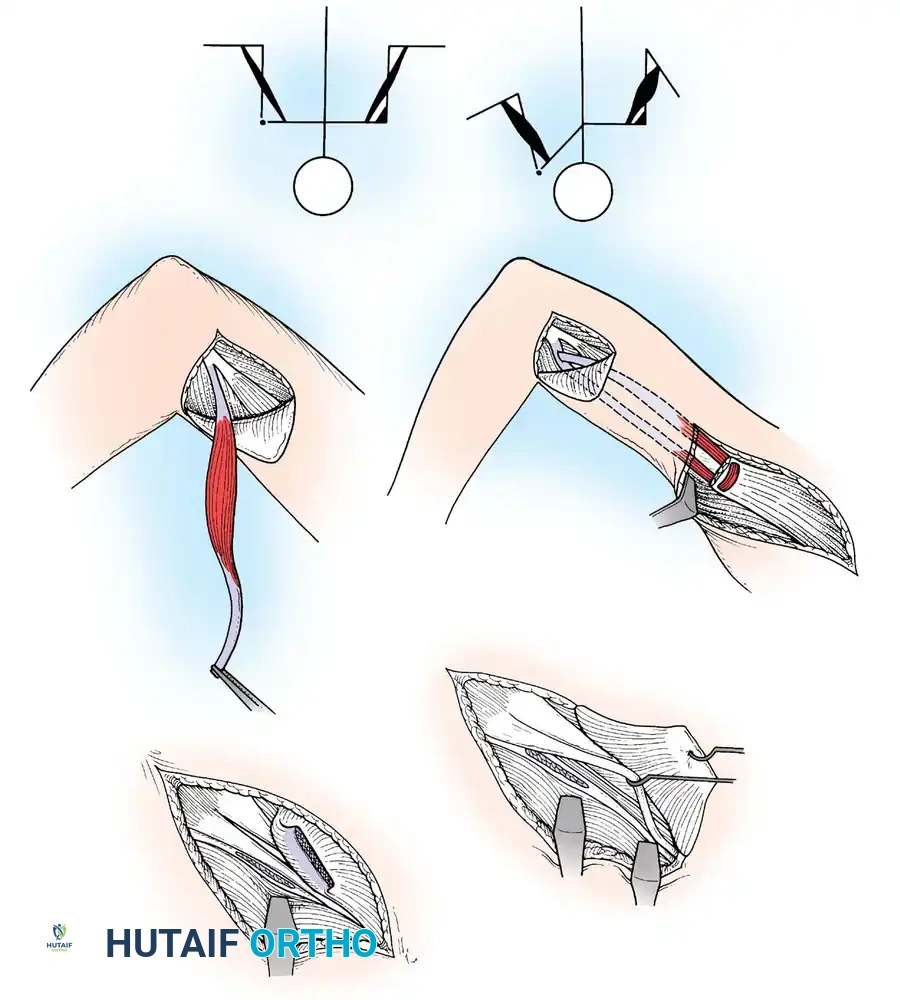
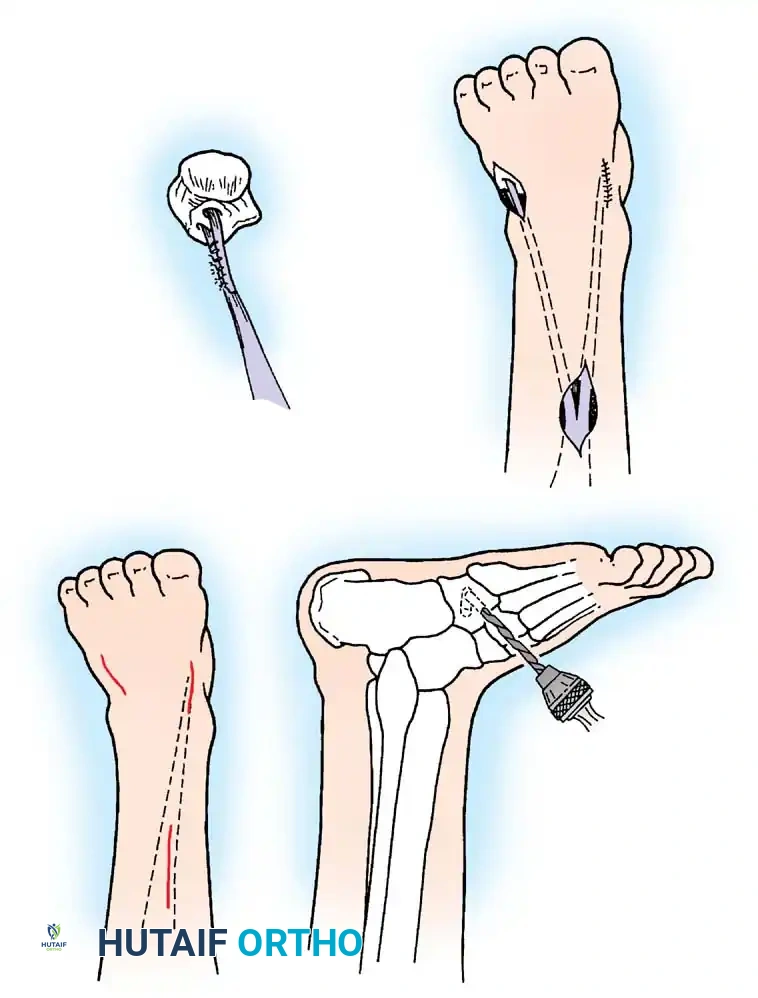
Tendon Transfers for Quadriceps Paralysis:
If the hamstrings are strong (Grade 4 or 5), the biceps femoris and semitendinosus can be transferred anteriorly to the patella or tibial tubercle.
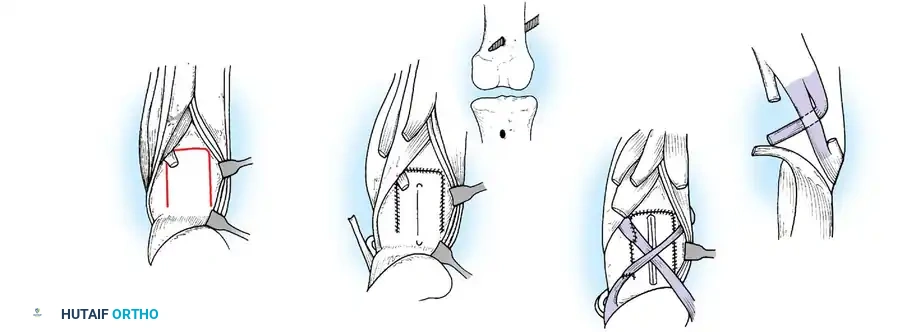
The tendons are mobilized, routed subcutaneously, and woven into the quadriceps tendon or fixed directly to the patella. Postoperatively, the knee is immobilized in extension for 6 weeks, followed by aggressive rehabilitation to achieve phasic conversion of the hamstrings from flexors to extensors.
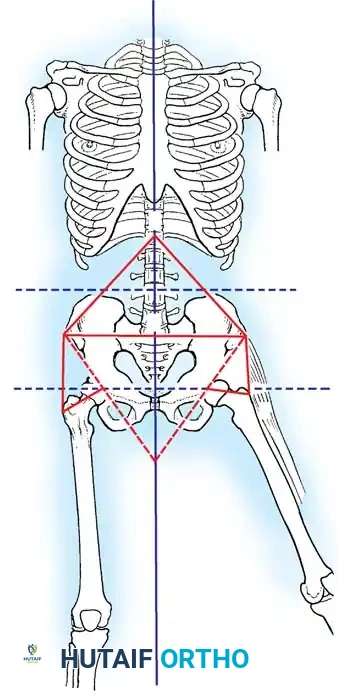
The Hip and Pelvis
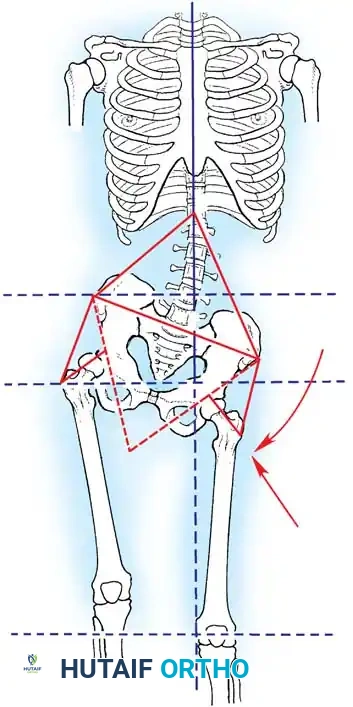
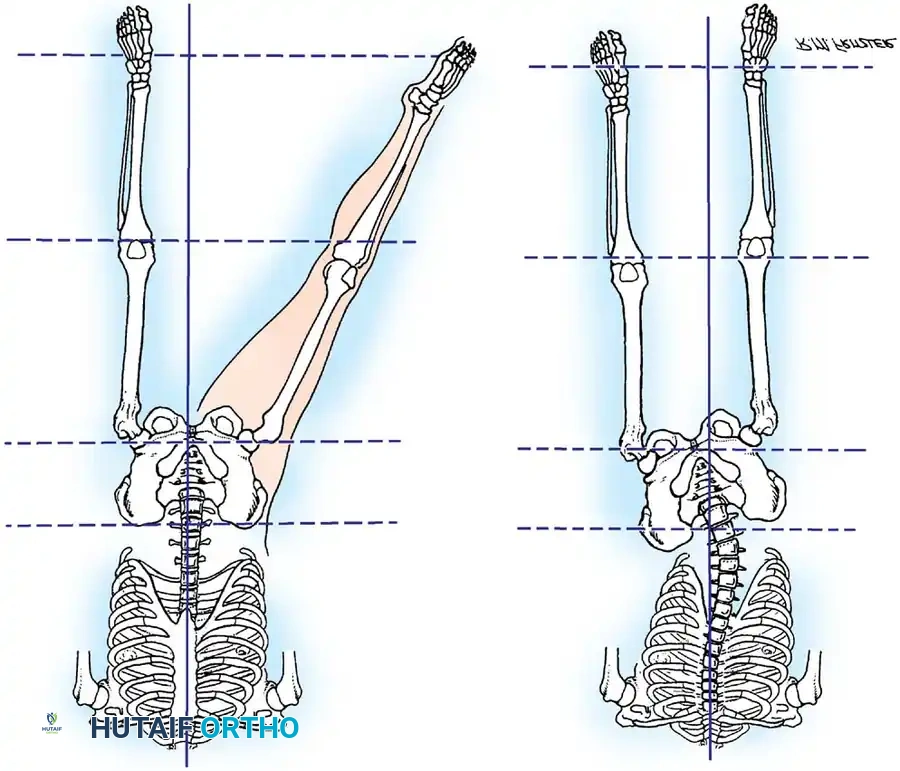
Paralytic deformities of the hip are driven by the unopposed action of the iliotibial band, hip flexors, and adductors in the setting of gluteal paralysis. This results in a classic flexion-abduction-external rotation contracture, pelvic obliquity, and eventual paralytic hip dislocation.
Management of Hip Contractures:
Early intervention is critical. A radical release of the iliotibial band (Yount's procedure) and fractional lengthening of the hip flexors are often required.
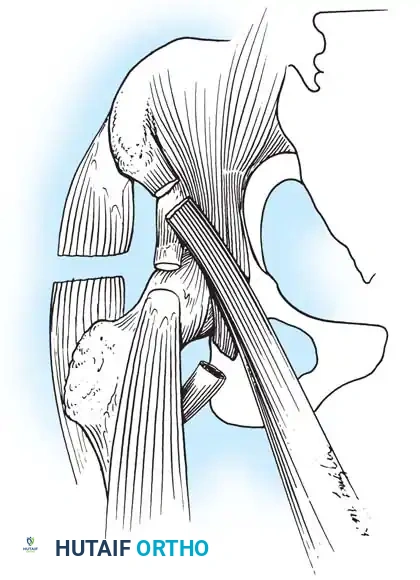
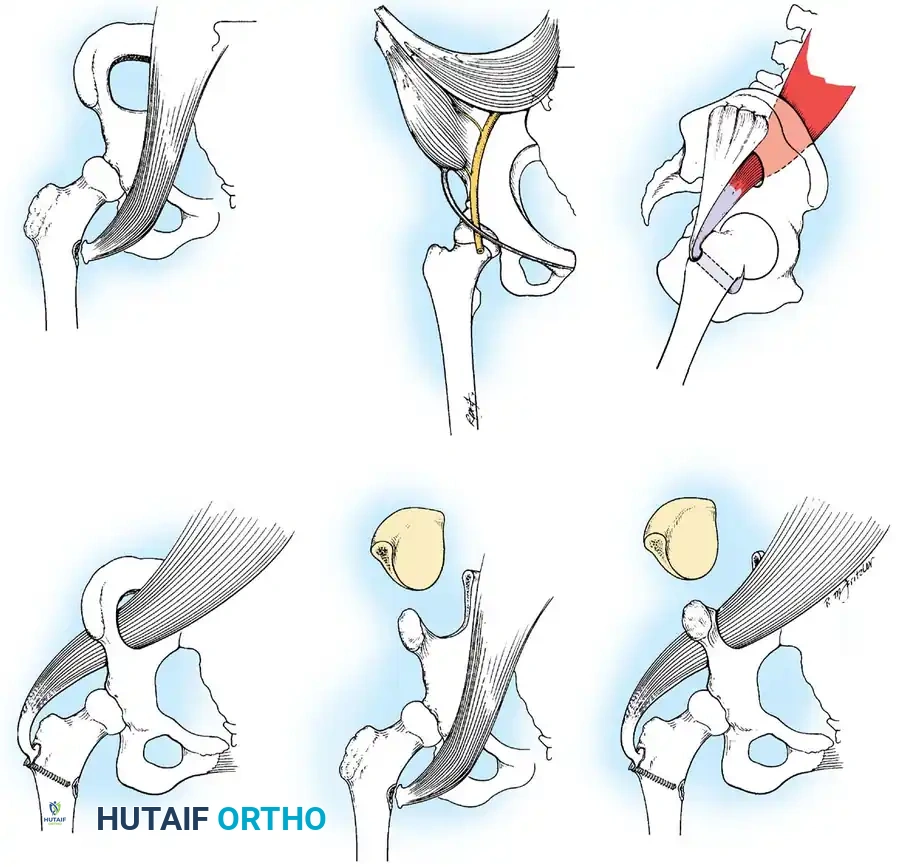
Gluteus Medius Paralysis:
Loss of hip abductors results in a severe Trendelenburg gait. The iliopsoas muscle can be transferred posterolaterally through a window in the ilium to the greater trochanter (Mustard or Sharrard transfer) to restore active abduction and stabilize the pelvis during the stance phase.
The Upper Extremity
While less frequently involved, upper extremity paralysis severely limits activities of daily living, particularly if the patient relies on crutches for ambulation.
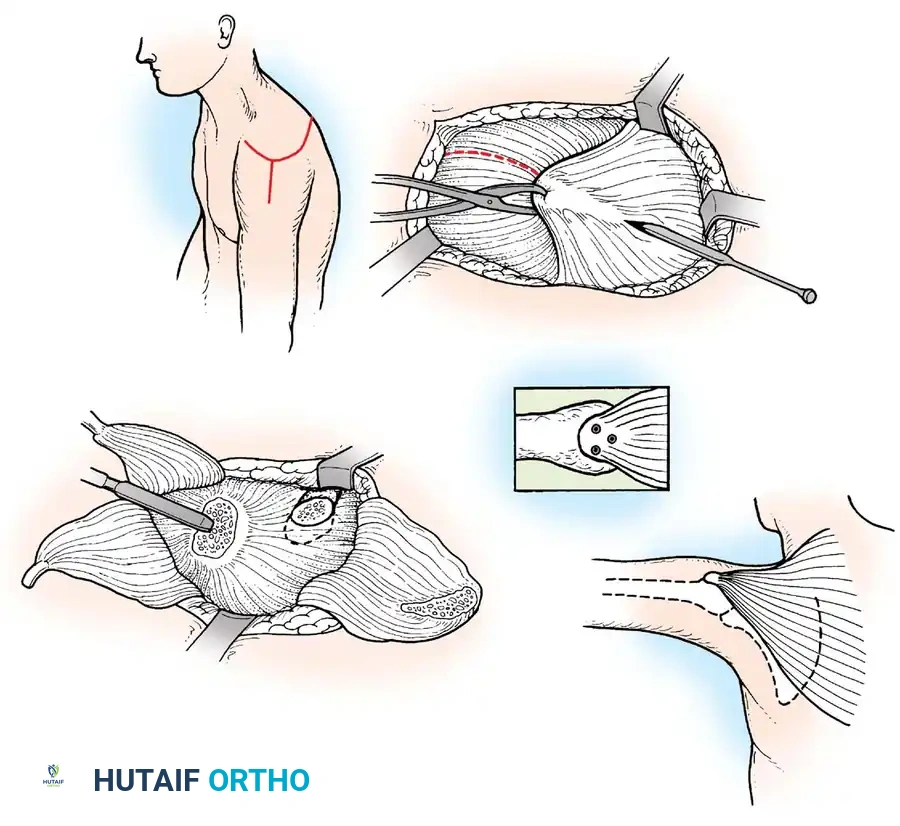
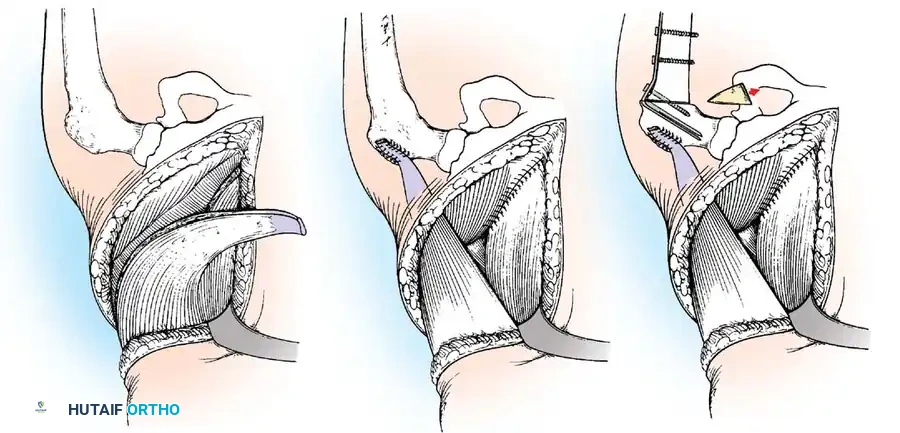
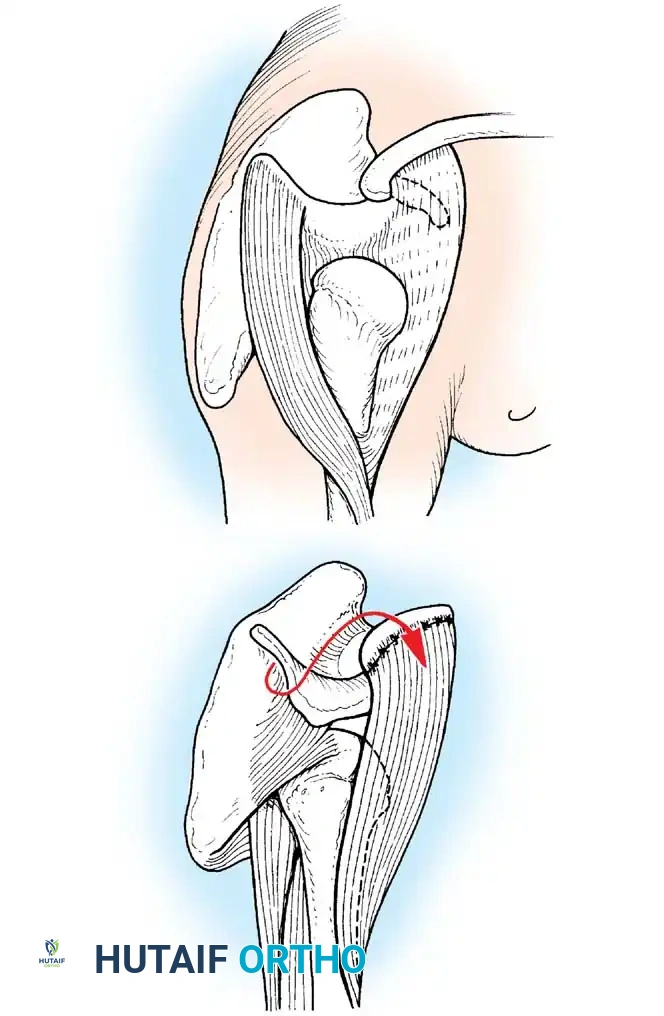
The Shoulder:
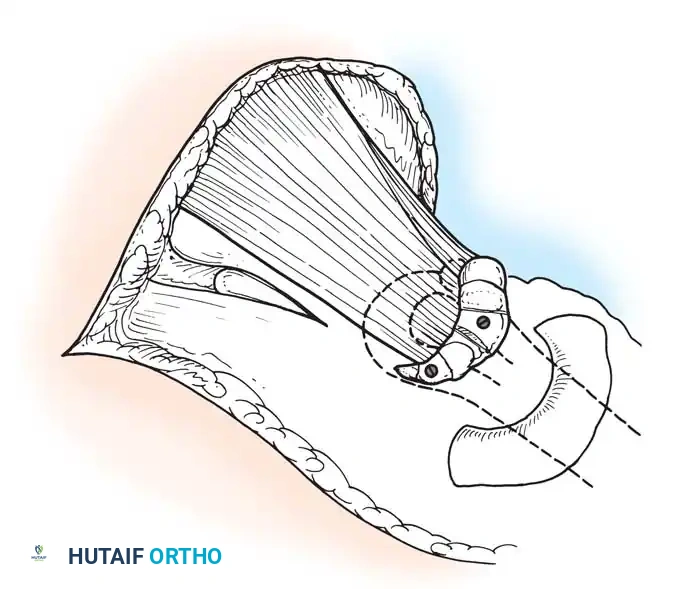
Paralysis of the deltoid and rotator cuff leads to a flail shoulder and inferior subluxation. If the periscapular muscles (trapezius, serratus anterior) are intact, a trapezius transfer (Bateman procedure) can be performed to restore active abduction.
If tendon transfer is not feasible due to widespread weakness, glenohumeral arthrodesis is the procedure of choice.
Clinical Pearl: The optimal position for shoulder arthrodesis in a polio patient is 30 degrees of abduction, 30 degrees of flexion, and 30 degrees of internal rotation. This allows the hand to reach the mouth for feeding while permitting the arm to rest comfortably at the side.
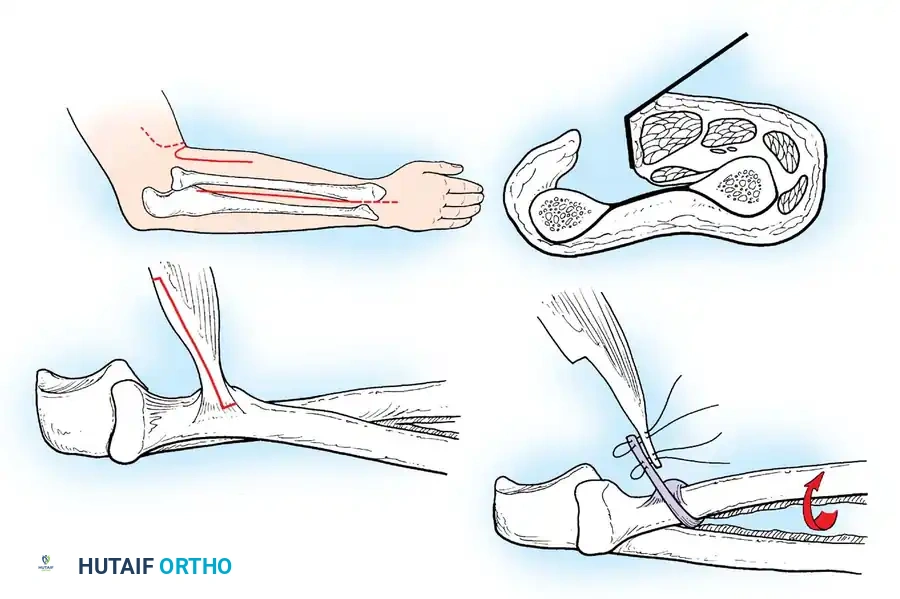
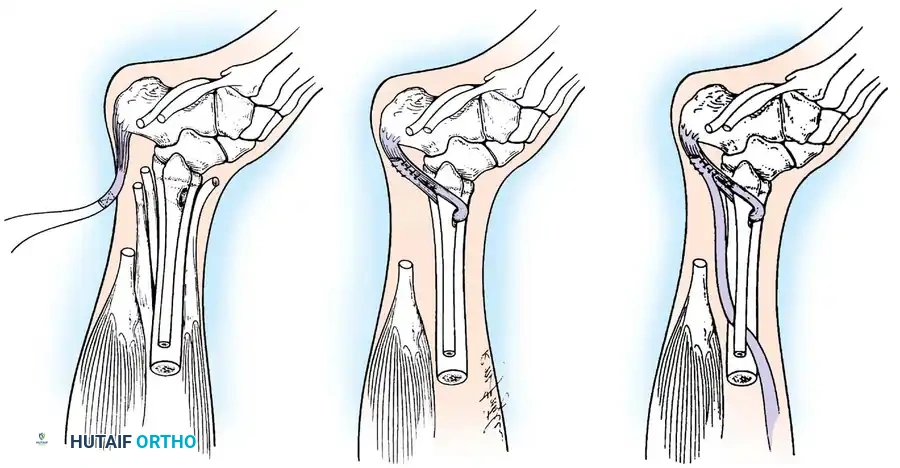
The Elbow:
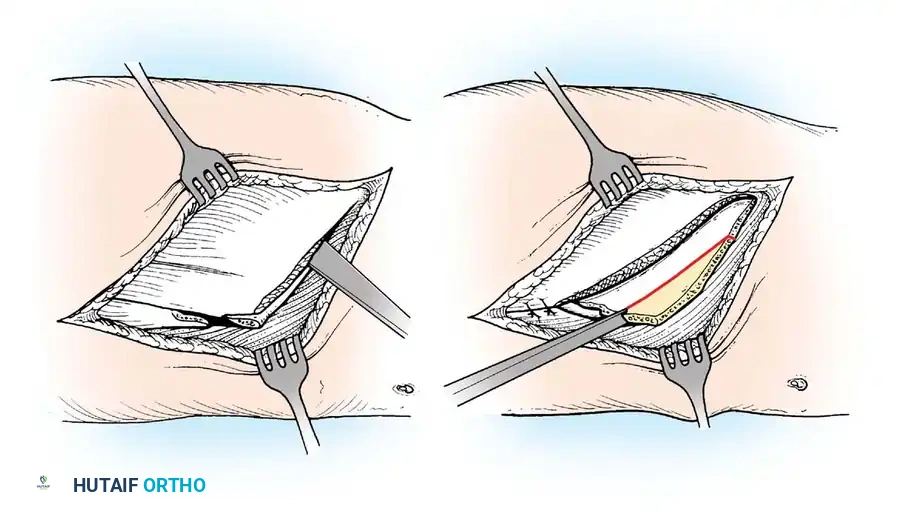
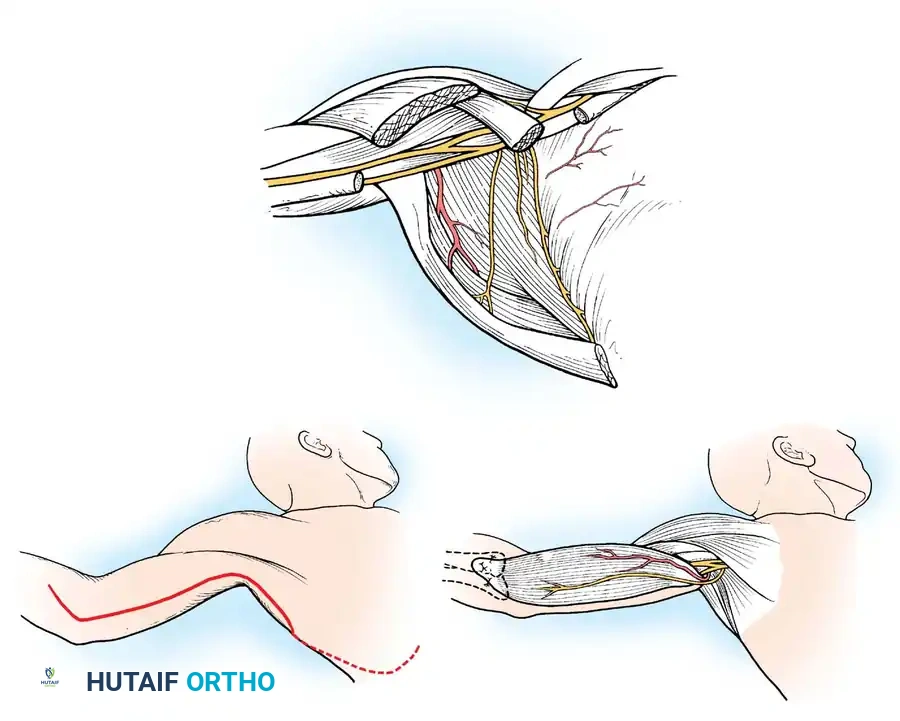
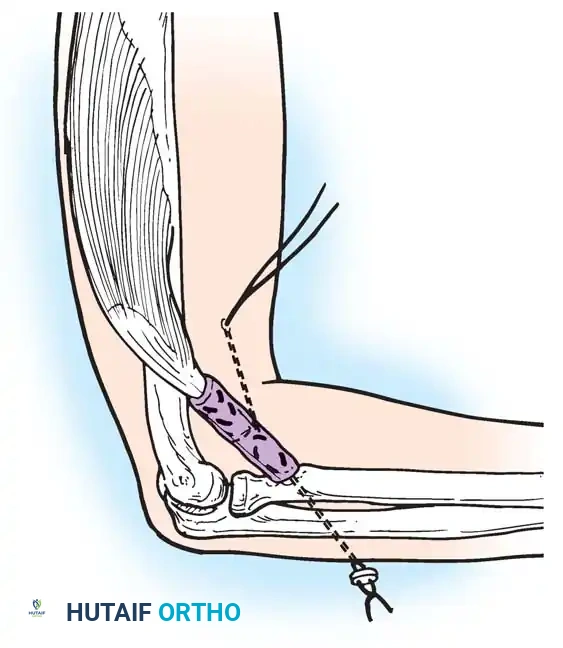
Loss of active elbow flexion prevents the patient from bringing the hand to the face. The Steindler flexorplasty is a classic and highly effective procedure.
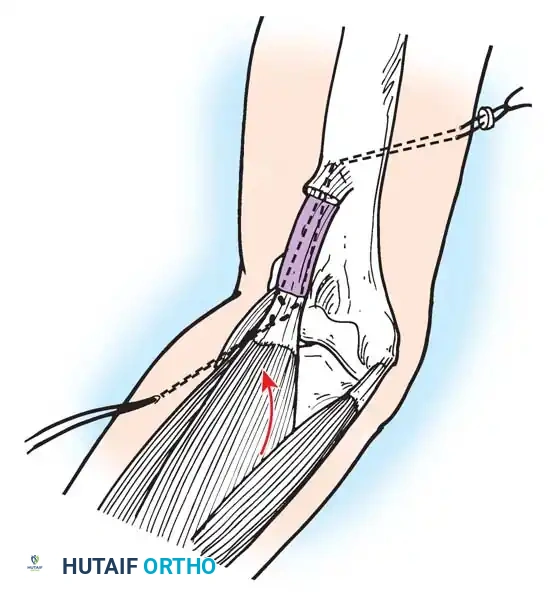
It involves proximal advancement of the flexor-pronator origin from the medial epicondyle to the anterior humerus. By increasing the moment arm of these muscles across the elbow joint, the patient can utilize wrist flexors to achieve active elbow flexion. Alternative options include transfer of the triceps, pectoralis major, or latissimus dorsi, depending on the availability of expendable donors.
Postoperative Protocols and Rehabilitation
The success of any paralytic reconstruction is inextricably linked to the postoperative rehabilitation protocol.
* Immobilization: Tendon transfers require rigid immobilization in a relaxed position for a minimum of 4 to 6 weeks to allow for secure biological healing at the tendon-bone interface.
* Muscle Re-education: Following cast removal, physical therapy focuses on isolated, gravity-eliminated activation of the transferred muscle. Biofeedback and electrical stimulation are highly beneficial adjuncts.
* Gradual Loading: Resistance and weight-bearing are introduced incrementally. Full functional integration of a transferred muscle, particularly a non-phasic transfer, may require 6 to 12 months of dedicated rehabilitation.
Conclusion
The orthopaedic management of poliomyelitis demands a profound understanding of neuromuscular biomechanics, meticulous surgical planning, and flawless execution. While the acute disease is increasingly rare, the principles of managing flaccid paralysis—meticulous contracture prevention, strategic tendon transfers, and definitive joint stabilization—remain foundational to the practice of reconstructive orthopaedic surgery. Through careful patient selection and adherence to established biomechanical tenets, the orthopaedic surgeon can dramatically improve the functional independence and quality of life for patients afflicted by paralytic conditions.
Associated Surgical & Radiographic Imaging




You Might Also Like


