Knee Deformities in Cerebral Palsy: Evaluation & Surgery
Key Takeaway
Knee deformities in cerebral palsy rarely occur in isolation, heavily influenced by two-joint muscles crossing the hip and ankle. Flexion contractures are the most common presentation, often resulting in a jump or crouch gait. Successful management requires meticulous clinical evaluation to differentiate spasticity from fixed contracture, followed by targeted surgical interventions such as fractional hamstring lengthening to restore sagittal balance and optimize ambulatory function.
KNEE DEFORMITIES IN CEREBRAL PALSY
Deformities of the knee in patients with cerebral palsy (CP) present a complex biomechanical challenge. They are exceptionally difficult to evaluate and treat in isolation because pelvic, hip, knee, ankle, and foot deformities are inextricably interrelated. Cerebral palsy is an upper motor neuron disorder; the brain is geographically affected, causing the body to be regionally affected. This contrasts sharply with lower motor neuron injuries (such as peripheral nerve lacerations), where only a specific innervated muscle or group is compromised.
In CP, the hip and the knee are tightly coupled due to the complex network of "two-joint muscles" that cross both articulations. These crucial structures include the rectus femoris anteriorly, the gracilis medially, and the semimembranosus, semitendinosus, and biceps femoris posteriorly. Pathological conditions affecting these muscles—whether dynamic spasticity or fixed myostatic contracture—profoundly alter the kinematics of both joints. A similar interdependent relationship exists between the knee and the ankle via the gastrocnemius muscle.
Consequently, a patient with CP who ambulates with flexed knees may not necessarily have tight or spastic hamstrings. For instance, a patient with a primary hip flexion contracture will ambulate with compensatory knee flexion to maintain their center of gravity and sagittal balance. Therefore, a meticulous, systematic physical examination of the entire lower extremity is mandatory before formulating any surgical plan for the knee.
PATHOPHYSIOLOGY OF KNEE FLEXION DEFORMITY
Flexion is the most common knee deformity encountered in patients with cerebral palsy and is frequently observed in ambulatory children. Pathological knee flexion prevents the knee from fully extending at the terminal swing phase of gait. Consequently, the knee remains flexed during the stance phase, which drastically decreases stride length, increases the quadriceps' demand to prevent collapse, and exponentially increases the energy expenditure of walking.
Isolated knee flexion can be driven by spastic hamstrings, weak quadriceps, or a combination of both. However, it frequently results from adjacent joint pathology:
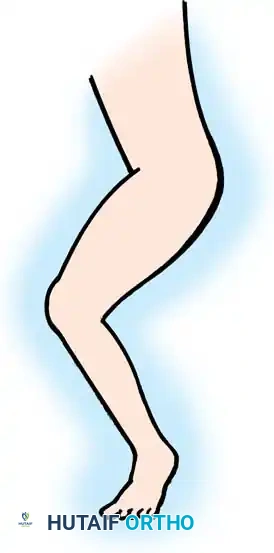
* Jump Gait: Patients with spastic hip flexors, weak hip extensors, or both will develop compensatory knee flexion, resulting in a "jump gait." In this pattern, the hips, knees, and ankles are all simultaneously flexed.
* Crouch Gait: Patients with weakened gastrocnemius-soleus complexes—either from the natural progression of CP or iatrogenically from over-lengthened Achilles tendons—ambulate with severe knee flexion to accommodate the relative overpull of the ankle dorsiflexors.
Fig. 30-19 Typical jump posture caused by plantar flexion deformities of ankles, which require flexion of knees, hip, and lumbar spine to place center of gravity over weight bearing surface.
Prolonged dynamic spasticity and chronic crouched knee gait inevitably lead to true, fixed capsular and musculotendinous contractures of the knee joint itself. To identify the true anatomical source of the knee flexion, the clinician must systematically assess the musculature to differentiate dynamic spasticity from fixed contracture.
💡 Clinical Pearl: The Spasticity vs. Contracture Paradigm
Dynamic spasticity is velocity-dependent resistance to stretch that may resolve under anesthesia. Fixed contracture is a structural shortening of the muscle-tendon unit and joint capsule that persists regardless of patient relaxation or anesthesia. Differentiating the two is the cornerstone of CP surgical decision-making.
COMPREHENSIVE CLINICAL EVALUATION
Strength testing and spasticity assessment can be notoriously difficult in patients with CP due to poor selective motor control. If the hamstrings are affected, the quadriceps are almost certainly affected to some degree. Quadriceps strength, spasticity, and firing patterns must be evaluated throughout the entire gait cycle, ideally supplemented by 3D Instrumented Gait Analysis (IGA) and dynamic electromyography (EMG).
Hamstring Assessment
Hamstring strength, spasticity, and knee contractures are assessed with the patient in both prone and supine positions.
Prone Assessment: The examiner extends the hips maximally and exerts gentle downward pressure on the calves. The angle formed between the femur and the tibia after dynamic spasticity has been overcome represents the true degree of fixed soft-tissue contracture behind the knee.
Supine Assessment (Popliteal Angle): The examiner stabilizes the contralateral knee in maximum extension. The ipsilateral hip is flexed to 90 degrees, and the knee is passively extended. If knee extension is limited, hamstring tightness is present.
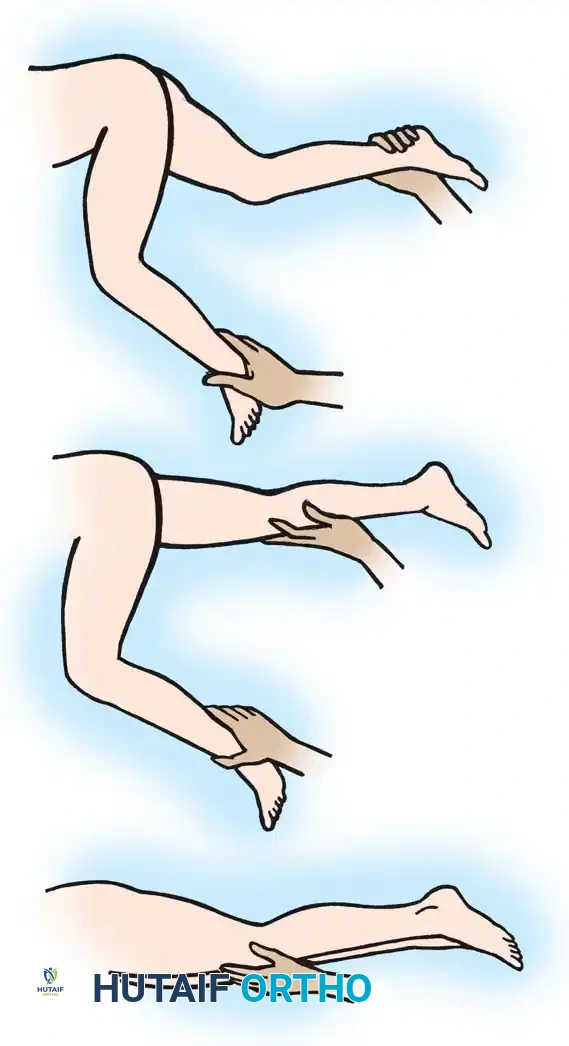
Fig. 30-20 Testing for hamstring spasticity and contracture. A, Patient is supine with hips extended. Pressure is exerted over knees, forcing them into extension. Flexion remaining in knees is absolute knee flexion contracture. B, Knee on side to be tested is flexed, while opposite knee is stabilized in extension. C, Attempted flexion of hip results in more flexion of knee.
Adductor and Medial Hamstring Assessment
To isolate medial hamstring spasticity, the patient is examined supine with the knees flexed over the edge of the table. This position relaxes the hamstrings proximally, allowing the hip to be abducted (provided there is no primary adductor contracture). If full knee extension is impossible unless the hip is adducted, tightness in the medial hamstrings and gracilis is confirmed.
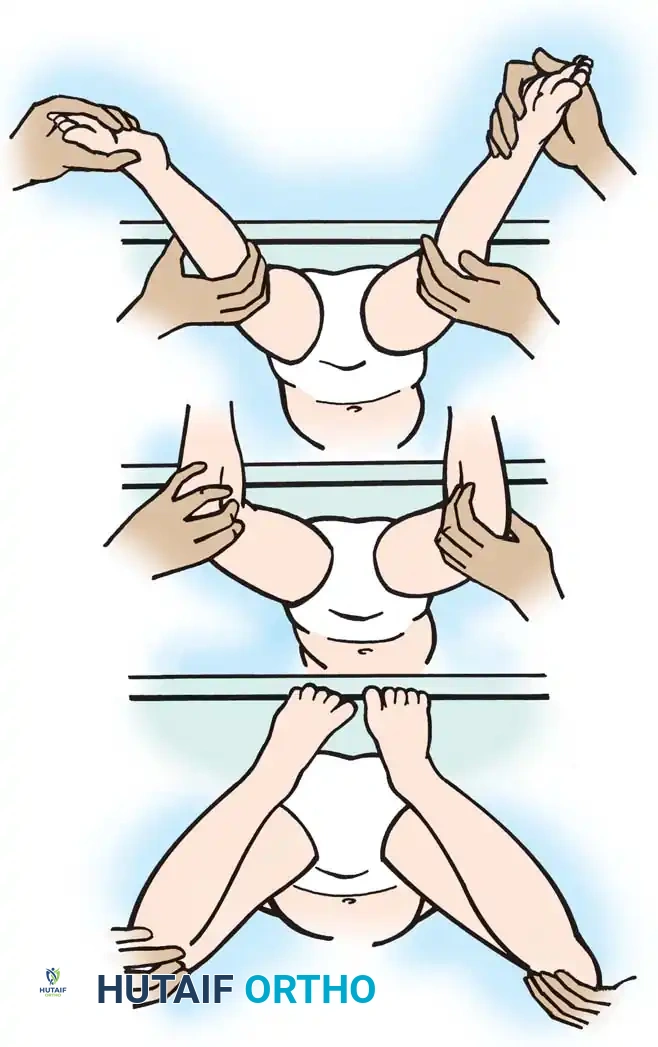
Fig. 30-21 Testing for adductor and medial hamstring tightness. A, Thighs abduct well with hips and knees flexed, indicating no adductor contracture. B, With hips extended and knees flexed, hips abduct well. C, With hips extended, bringing knees into extension causes thighs to adduct, indicating medial hamstring spasticity.
Gastrocnemius Assessment
The degree of ankle equinus must be measured with the knee both flexed and fully extended (the Silfverskiöld test principle). If ankle dorsiflexion significantly improves when the knee is flexed, the gastrocnemius (a two-joint muscle) is the primary source of spasticity or contracture.
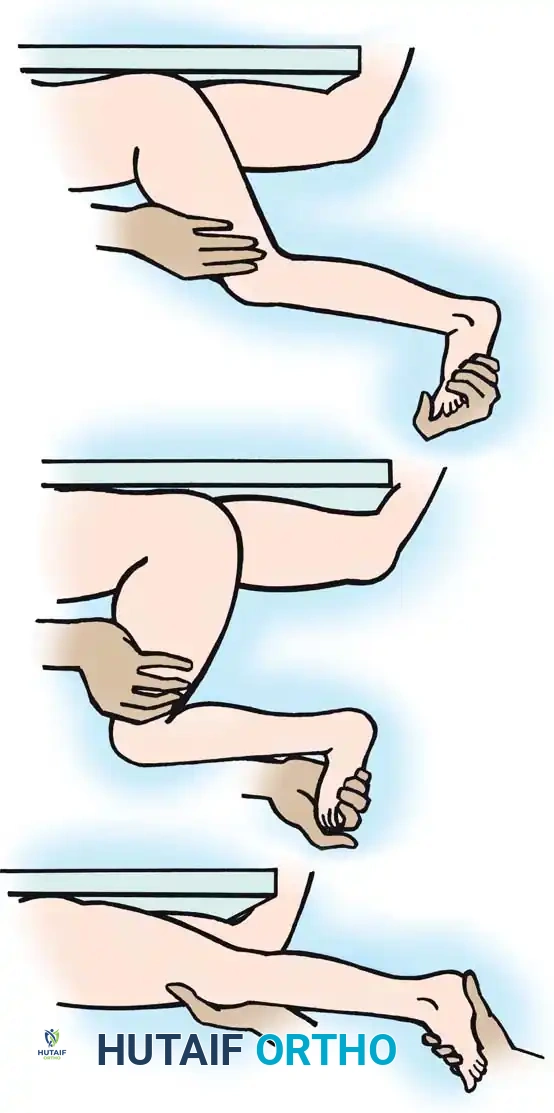
Fig. 30-22 Testing for gastrocnemius contracture and spasticity. A, With knee extended, equinus in ankle is noted. B, With knee flexed, ankle is easily dorsiflexed, indicating no soleus contracture. C, As knee is extended, ankle dorsiflexion is resisted by tight or spastic gastrocnemius muscles.
Quadriceps and Rectus Femoris Assessment
Quadriceps strength is best assessed with the patient supine and the lower legs dangling off the end of the examination table. The examiner extends the hips, allows the knees to flex passively, and then instructs the patient to voluntarily extend the knees against manual resistance.
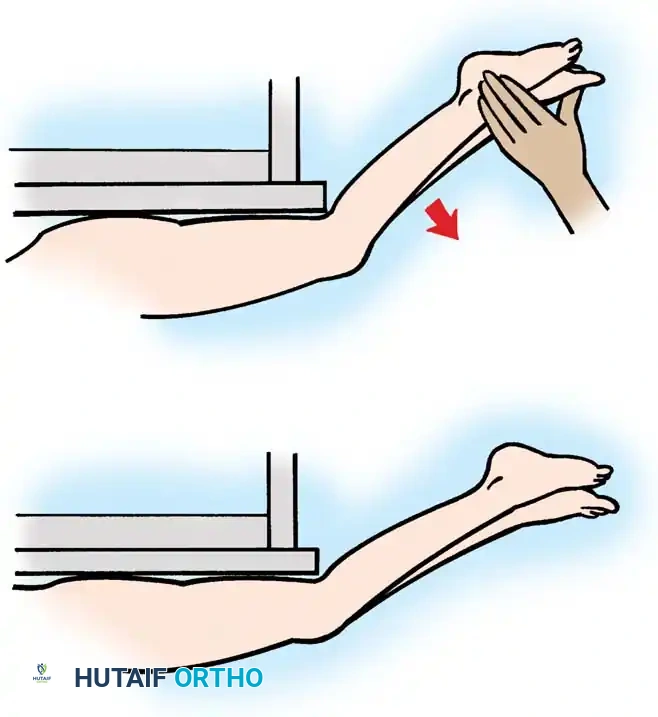
Fig. 30-23 Testing for quadriceps strength. A, With hips extended, knees are allowed to flex off end of table. B, Patient voluntarily extends knees from flexed position against resistance.
To isolate rectus femoris spasticity, the Prone Rectus (Ely) Test is utilized. With the patient prone and knees initially extended, the examiner rapidly flexes the knees. If the rectus femoris is spastic, the rapid stretch causes the hips to flex, and the patient's buttocks will rise off the table. This should be performed unilaterally to compare relative spasticity.
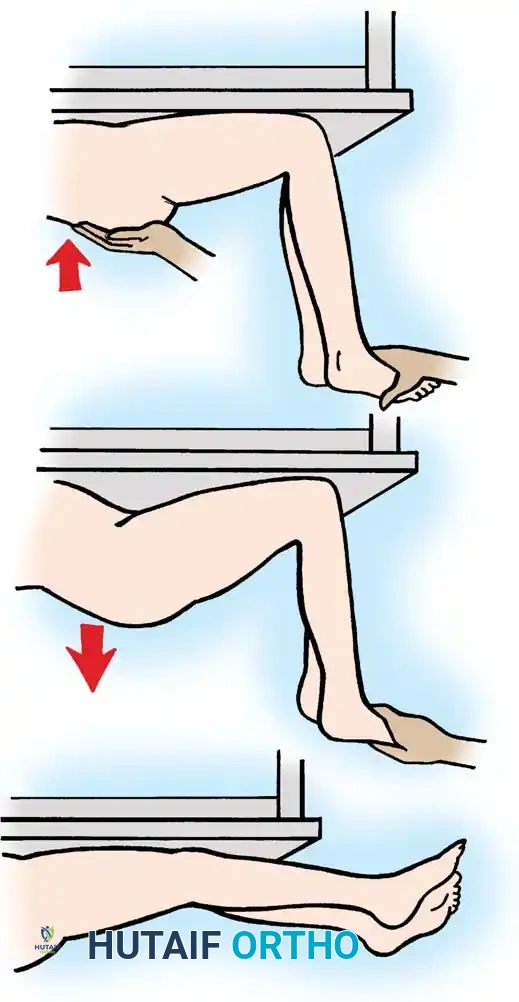
Fig. 30-24 Prone rectus test. A, Patient is prone, and knees are extended. B, Flexing knees causes buttocks to rise from table. C, Spasticity in rectus is overcome by downward pressure on buttocks.
SURGICAL INDICATIONS AND DECISION MAKING
The primary indications for hamstring lengthening in an ambulatory CP patient include:
1. A straight leg raise of less than 70 degrees.
2. A popliteal angle of less than 135 degrees (i.e., >45 degrees lacking from full extension).
3. A fixed knee flexion contracture of more than 10 degrees, which inevitably leads to excessive compensatory hip flexion and ankle dorsiflexion.
🚨 Surgical Warning: The Risk of Hyperextension Gait
Lengthening—and essentially weakening—the hamstrings in the presence of a spastic rectus femoris or weak quadriceps can precipitate a devastating iatrogenic genu recurvatum (hyperextension) gait. In this pattern, the femur translates anteriorly over a fixed tibia, which is locked by a spastic gastrocnemius or limited ankle dorsiflexion.
Because of this risk, most surgeons adopt a conservative, staged approach. The standard initial intervention is lengthening the medial hamstrings via a Z-plasty of the gracilis and semitendinosus tendons, combined with a fractional lengthening of the semimembranosus. If intraoperative testing reveals residual tightness, the lateral hamstrings (biceps femoris) can be addressed via fractional lengthening.
SURGICAL TECHNIQUES
Fractional Lengthening of Hamstring Tendons (Technique 30-8)
Fractional lengthening allows for controlled elongation of the muscle-tendon unit while preserving the continuity of the muscle belly, thereby minimizing the risk of catastrophic over-lengthening and subsequent weakness.
Positioning and Approach:
* Place the patient in the prone position. Pad all bony prominences carefully.
* Exsanguinate the limb and inflate a proximal thigh tourniquet.
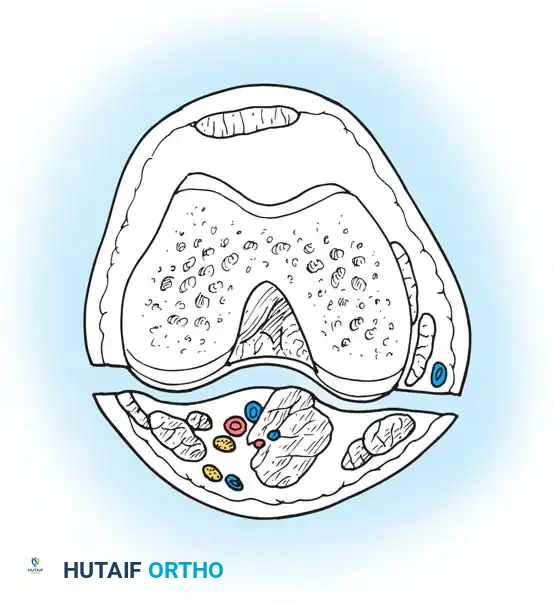
* Make medial and lateral posterior longitudinal incisions starting from the popliteal crease and extending 7 to 10 cm proximally. Alternatively, a single midline posterior incision can be utilized.

Incision mapping for posterior hamstring approach.
Medial Hamstring Lengthening:
* Divide the subcutaneous tissue and deep fascia strictly in line with the skin incision.
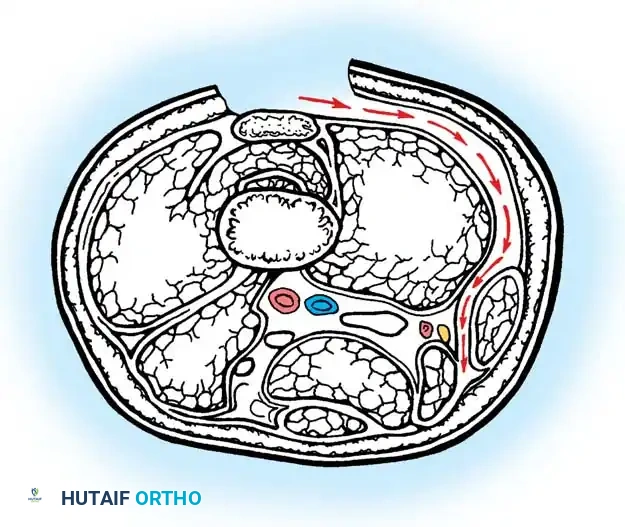
* Crucial Step: Identify and protect the posterior femoral cutaneous nerve in the proximal portion of the wound.
* Identify the hamstrings via blunt dissection. Isolate the semimembranosus muscle and incise its tendon sheath longitudinally.
* Divide the tendinous fibers of the semimembranosus on its deep (anterior) surface transversely at two distinct levels, leaving the underlying muscle fibers completely intact.
Forceps everting semimembranosus muscle to expose tendinous portion; division at two levels.
- Next, expose the semitendinosus tendon. Divide the distal portion of the tendon obliquely up to its muscle fibers. Depending on the severity of the contracture, incise the tendon transversely or perform a formal Z-plasty.
- Extend the knee and flex the hip simultaneously. The sectioned tendinous portion of the semimembranosus will slide smoothly over the intact muscle belly, achieving the desired lengthening.
Lateral Hamstring Lengthening (If Indicated):
* If further correction is required to achieve full extension, proceed to the lateral side.
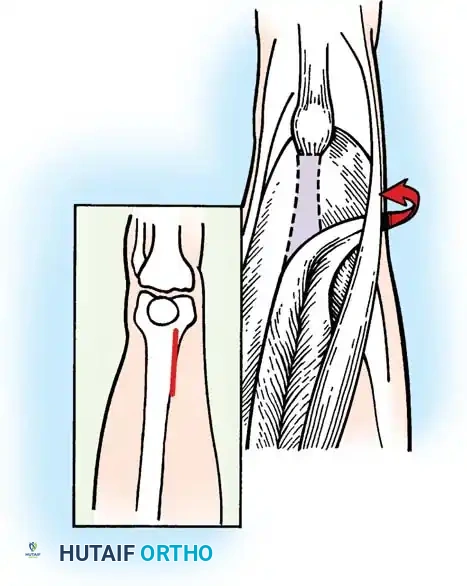
* Identify the biceps femoris tendon.
* Crucial Step: Meticulously isolate the biceps femoris from the common peroneal nerve, which lies immediately along its medial and posterior border.
* Pass a blunt right-angle instrument deep to the biceps femoris tendon to protect the nerve. Incise its tendinous portion transversely at two levels approximately 3 cm apart, leaving the muscle fibers intact.

Incisions in biceps femoris; note hemostat anterior to peroneal nerve protecting the neurovascular structures.
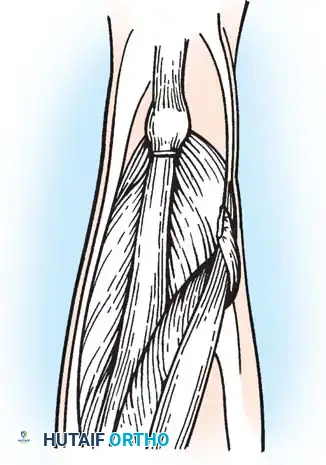
Closure:
* Perform a similar dynamic lengthening maneuver by flexing the hip and extending the knee to ensure the lateral structures slide appropriately.
* Close all individual tendon sheaths meticulously with absorbable suture.
* Do not close the deep fascia. Leaving the deep fascia open prevents postoperative compartment syndrome and allows for the expanded volume of the sliding muscle bellies.
Separate meticulous closure of each tendon sheath; deep fascia is not sutured.

Fig. 30-25 Fractional lengthening of hamstrings overview. A, Skin incision and incision in deep fascia over back of knee. B, Incisions in semimembranosus. C, Incisions in biceps femoris. D, Tendon sheaths of biceps femoris and semimembranosus are sutured before wound closure.
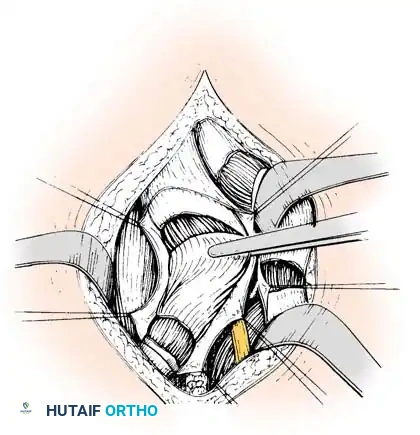
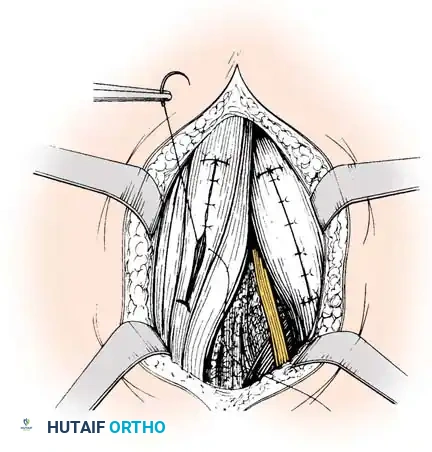
Intraoperative Photographic Series: Hamstring Lengthening
The following intraoperative images demonstrate the sequential isolation, fascial release, and controlled sliding of the hamstring musculotendinous units during a fractional lengthening procedure.
Intraoperative view: Initial isolation of the posterior hamstring structures.
Intraoperative view: Transverse fractional cuts made into the tendinous aponeurosis.
Intraoperative view: Demonstration of the muscle belly sliding beneath the sectioned tendon upon passive knee extension.
Intraoperative view: Assessment of the lateral compartment and biceps femoris tension.

Intraoperative view: Final verification of tendon sheath closure prior to dermal approximation.
Concurrent Management of Spastic Hip Dysplasia (Technique 30-7)
Because CP is a multi-level disorder, knee flexion deformities are frequently accompanied by spastic hip subluxation or dysplasia. Single Event Multilevel Surgery (SEMLS) is often required. If hip reconstruction is indicated concurrently:
- Place the patient supine with a soft pad under the gluteal region.
- Perform an adductor tenotomy to relieve medial deforming forces.
- Through a longitudinal lateral incision to the hip, split the gluteal muscles to access the joint capsule.
- Extend the exposure to allow for a fractional iliopsoas tenotomy, addressing the hip flexion contracture that drives the downstream knee crouch.
- If open reduction is required: Resect the pulvinar and ligamentum teres, clear the acetabulum, and deepen the dysplastic socket.
- Position the hip in 40 degrees of flexion, 15 degrees of abduction, and neutral rotation. Fixation (e.g., 4.5-mm AO-D cerebral palsy plate, AO-Cobra plate, or 6.5-mm cannulated screws) depends on bone quality and the required degree of correction.
POSTOPERATIVE PROTOCOL AND OUTCOMES
Rehabilitation
Following isolated hamstring lengthening, patients are typically immobilized in long-leg casts or knee immobilizers in maximum extension for 3 to 4 weeks. Upon cast removal, a rigorous, progressive range-of-motion and weight-bearing physical therapy program is initiated. Night splinting in extension is maintained for at least 6 to 12 months to prevent recurrence of the myostatic contracture.
For patients undergoing concurrent hip reconstruction (Technique 30-7), a hip spica cast is worn for 2 months postoperatively before transitioning to progressive mobilization.
Evidence-Based Outcomes
The literature demonstrates nuanced outcomes regarding hamstring lengthening in CP:
* Kinematic Improvements: Thometz, Simon, and Rosenthal utilized dynamic EMG and gait studies to evaluate 31 CP patients post-hamstring lengthening. While overall velocity, stride length, and cadence did not universally improve, knee extension in the stance phase improved dramatically. However, this was often accompanied by a slight decrease in knee flexion during the swing phase.
* Ambulatory Status: Mann's long-term review (3 to 14 years) of 126 patients undergoing distal hamstring lengthening revealed that 39% of previously nonambulatory patients became functional household ambulators. While popliteal angles improved universally at 1 year, 17% required reoperation due to recurrent contracture over time.
* Medial vs. Combined Lengthening: Kay et al. compared isolated medial hamstring lengthening against combined medial and lateral lengthenings. The combined group showed a trend toward greater improvement in popliteal angle and stance-phase knee extension, but carried a significantly higher risk of iatrogenic knee hyperextension and prolonged hamstring weakness up to 1.5 years postoperatively.
Careful patient selection, precise differentiation between spasticity and contracture, and conservative, staged surgical execution remain the hallmarks of successful knee deformity management in the cerebral palsy population.
You Might Also Like

