Correction of Thumb-in-Palm Deformity in Cerebral Palsy

Introduction and Epidemiology
The thumb-in-palm (TIP) deformity represents one of the most challenging and highly prevalent upper extremity manifestations of spastic cerebral palsy (CP). Characterized by a fixed or dynamic adduction and flexion posture of the first ray, this deformity severely compromises both the functional capacity and the hygiene of the affected hand. Cerebral palsy is fundamentally defined as a permanent, non-progressive disorder of movement and posture attributed to an anoxic, ischemic, or developmental insult to the fetal or infant brain. Although the primary central nervous system neurologic lesion is static, the secondary musculoskeletal manifestations in the upper extremity are relentlessly progressive.

In the typically developing infant, a supple thumb-in-palm posture, or "cortical thumb," is a physiologic finding during the first few months of life, reflecting the immaturity of the corticospinal tracts. However, persistence of a tightly clenched thumb beyond the first year of life is highly pathologic and warrants rigorous neurologic and orthopedic evaluation. The deformity initially presents as a dynamic imbalance driven by spasticity—a velocity-dependent increase in muscle tone resulting from disinhibition of the stretch reflex. Over time, chronic spasticity leads to structural shortening of the myotendinous units, a reduction in the number of in-series sarcomeres, and extracellular matrix fibrosis. This pathophysiologic cascade culminates in rigid myostatic contractures.
Epidemiologically, the thumb-in-palm deformity is most frequently observed in patients with spastic hemiplegia and spastic quadriplegia. The inability to extend and palmar-abduct the thumb effectively neutralizes the hand's ability to perform side-to-side (key) pinch, tip-to-tip pinch, and large object grasp. When the thumb is anatomically trapped within the palm, the ulnar digits are physically blocked from flexing fully into the palm, rendering the entire hand functionally deficient. Furthermore, in non-ambulatory, severely involved patients, fixed deformities lead to palmar maceration, recurrent paronychia, skin breakdown, and profound hygiene difficulties, necessitating surgical intervention even in patients without functional grasp potential.

Surgical Anatomy and Biomechanics
A profound understanding of the complex functional anatomy and kinematics of the thumb is prerequisite to executing a successful surgical correction. The thumb-in-palm deformity is rarely the result of a single pathologic muscle; rather, it represents a multi-level biomechanical collapse driven by a profound imbalance between spastic/contracted flexors and adductors, and paretic, overstretched extensors and abductors.

Intrinsic and Extrinsic Deforming Forces
The deforming forces driving the TIP posture are categorized into intrinsic and extrinsic muscle groups. The primary intrinsic deforming muscles include the adductor pollicis (AP), the flexor pollicis brevis (FPB), and the first dorsal interosseous (1st DI). The adductor pollicis, with its transverse head originating from the third metacarpal and its oblique head originating from the capitate and bases of the second and third metacarpals, exerts a massive adduction moment on the first metacarpal. The flexor pollicis brevis contributes to severe flexion at the metacarpophalangeal (MCP) joint. The first dorsal interosseous, while primarily an abductor of the index finger, acts as a secondary adductor of the first metacarpal when spastic, significantly narrowing the first web space.
The primary extrinsic deforming force is the flexor pollicis longus (FPL). Spasticity or structural contracture of the FPL leads to acute flexion at the interphalangeal (IP) joint. When the FPL is severely contracted, its moment arm crosses multiple joints, contributing to MCP and carpometacarpal (CMC) flexion as well.

Antagonist Muscle Weakness
Opposing these spastic forces are the thumb extensors and abductors, which are typically paretic and chronically overstretched. The extensor pollicis longus (EPL), extensor pollicis brevis (EPB), and abductor pollicis longus (APL) often lack the cross-sectional area and motor unit recruitment necessary to overcome the spastic flexors and adductors. This chronic imbalance leads to progressive attenuation of these extensor tendons, shifting the resting length-tension curve to a functionally disadvantageous position.
Joint Instability and Collapse Patterns
The skeletal architecture of the thumb frequently succumbs to these unbalanced forces, leading to predictable patterns of joint collapse. The most common secondary joint deformity is MCP joint hyperextension. As the patient attempts to actively extend the thumb against a tight FPL and AP, the extensor mechanism focuses its force entirely on the MCP joint rather than the IP joint. This chronic dorsal force leads to attenuation of the volar plate and subsequent hyperextension, creating a classic swan-neck deformity of the thumb (MCP hyperextension with IP flexion).

The CMC joint may also develop instability, subluxation, or even dislocation due to chronic adduction forces, although this is less common than MCP joint pathology. Recognizing the specific combination of muscle contracture and joint instability is the foundation of the House Classification system, which categorizes the deformity (Types I through IV) based on the primary site of contracture (adduction vs. flexion) and the presence of MCP hyperextension, directly guiding surgical decision-making.
Indications and Contraindications
Patient selection and precise timing of surgical intervention are critical for optimizing outcomes in the cerebral palsy population. The primary goal of surgery is to rebalance the hand to improve function (grasp, pinch, and release) or, in severely involved Global Motor Function Classification System (GMFCS) Level IV-V patients, to improve hygiene, nursing care, and cosmesis.
Clinical Evaluation and Decision Making
A meticulous physical examination must differentiate between dynamic spasticity and fixed myostatic contracture. Spasticity is evaluated using the Modified Ashworth Scale or the Tardieu Scale, specifically noting the catch phase (R1) during rapid passive stretch versus the absolute limits of passive motion (R2). Fixed contractures are identified by an inability to achieve full passive range of motion even with slow, sustained stretching (where R1 = R2).
The surgeon must also evaluate the patient's voluntary motor control, cognitive status, and sensibility. Patients with profound sensory deficits (e.g., lack of two-point discrimination or stereognosis) or a complete lack of voluntary motor control in the upper extremity are unlikely to achieve functional gains from tendon transfers, though they remain excellent candidates for hygiene-improving release procedures.
| Indication Category | Specific Clinical Findings | Recommended Interventions |
|---|---|---|
| Operative Functional | Dynamic or fixed TIP, good voluntary control, intact sensibility, grasp/release potential | Soft tissue releases, tendon transfers (EPL rerouting), MCP joint stabilization |
| Operative Hygiene | Severe fixed contracture, palmar maceration, absent voluntary control, painful spasticity | Radical intrinsic releases, FPL lengthening or tenotomy, formal arthrodesis |
| Non-Operative | Supple deformity, mild spasticity, responsive to therapy, age under 4 years | Splinting, occupational therapy, targeted Botulinum toxin A injections |
Contraindications to Surgery
Absolute contraindications include severe, uncontrolled movement disorders such as profound choreoathetosis or dystonia. These extrapyramidal disorders lead to unpredictable surgical outcomes, rapid recurrence, or even complete reversal of deformities (e.g., converting a thumb-in-palm to a rigid thumb-in-extension). Relative contraindications include severe cognitive impairment that precludes participation in postoperative neuromuscular rehabilitation, and a completely functionless, insensate hand where the deformity does not interfere with hygiene, dressing, or nursing care.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning requires a multidisciplinary approach involving the orthopedic/hand surgeon, pediatric neurologist, and occupational therapist.
Diagnostic Modalities and Botulinum Toxin Trials
Diagnostic injections of Botulinum toxin A (BoNT-A) into the adductor pollicis, flexor pollicis brevis, and flexor pollicis longus can serve as an invaluable preoperative tool. By temporarily paralyzing the spastic muscles via presynaptic blockade of acetylcholine release, the surgeon can unmask the underlying voluntary control of the extensor and abductor muscles. If thumb extension and palmar abduction improve significantly following the injection, the patient is likely an excellent candidate for surgical release without the absolute need for complex tendon transfers. Conversely, if no active extension is observed despite adequate temporary paralysis of the antagonists, augmentation of the extensors via tendon transfer must be incorporated into the surgical plan.

Patient Positioning and Setup
The patient is placed in the supine position on the operating table. A radiolucent hand table attachment is secured to the operative side to allow for intraoperative fluoroscopy if joint stabilization is planned. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is absolutely essential for identifying fine neurovascular structures in the pediatric hand. The upper extremity is prepped and draped in a standard sterile fashion, allowing access from the elbow to the fingertips. Loupe magnification (2.5x to 3.5x) is highly recommended for meticulous dissection of the intrinsic muscles and protection of the delicate digital nerves.

Detailed Surgical Approach and Technique
Correction of the thumb-in-palm deformity is rarely a single procedure; it is an "à la carte" reconstruction tailored to the patient's specific anatomic deficits. The surgical strategy generally follows a logical, sequential algorithm: release of contracted structures, augmentation of weak antagonists, and stabilization of hypermobile or collapsed joints.

Intrinsic Muscle Release Techniques
The release of the adductor pollicis and flexor pollicis brevis can be approached via a palmar or a dorsal incision, depending on the severity of the web space contracture.
For the palmar approach, a curved incision is made parallel to the thenar crease. The palmar fascia is incised, and the recurrent motor branch of the median nerve is carefully identified and protected. The flexor pollicis brevis is identified and its origin can be released or recessed. The neurovascular bundles to the thumb are gently retracted to expose the adductor pollicis. The transverse and oblique heads of the adductor pollicis are sharply released from their metacarpal origins. Extreme care must be taken to avoid injury to the deep palmar arch, which lies in intimate proximity to the oblique head of the adductor.
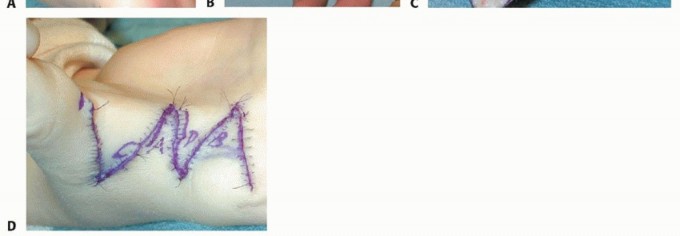
Alternatively, a dorsal approach through the first web space can be utilized. A Z-plasty, four-flap Z-plasty, or jumping-man flap is designed over the dorsal web space. This approach not only provides excellent access to the first dorsal interosseous and adductor pollicis insertions but also allows for simultaneous deepening of a contracted skin web. The first dorsal interosseous is released from the first metacarpal, and the adductor insertion is divided at the sesamoid level.
Extrinsic Tendon Lengthening
If the flexor pollicis longus is contracted, causing severe interphalangeal joint flexion (R2 < neutral), it must be lengthened. This is typically performed at the musculotendinous junction in the distal forearm to preserve tendon continuity and minimize adhesion formation at the wrist level.
A longitudinal incision is made over the volar radial forearm. The flexor carpi radialis is retracted ulnarly, and the flexor pollicis longus muscle belly is identified deep to the radial artery. A fractional lengthening is performed by making transverse step-cuts in the tendinous aponeurosis of the muscle while leaving the underlying muscle fibers intact. The wrist and thumb are then passively extended to achieve the desired lengthening, usually allowing the thumb to rest in neutral extension with the wrist at neutral. If the contracture is extremely severe or the muscle lacks sufficient aponeurosis, a formal Z-lengthening of the tendon may be required, though this carries a higher risk of postoperative weakness and over-lengthening.

Tendon Transfers for Extension and Abduction
When the extensor pollicis longus and abductor pollicis longus lack sufficient power to maintain the thumb out of the palm, tendon transfers are indicated.
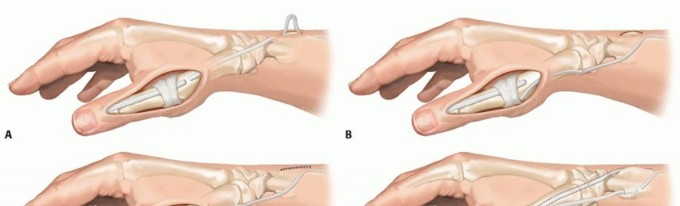
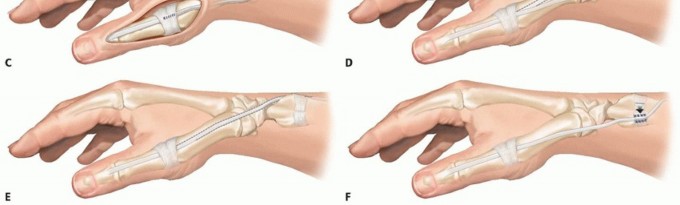
The rerouting of the extensor pollicis longus (Manske procedure) is a highly effective and widely utilized procedure. The EPL tendon is identified dorsally and released from the third extensor compartment (Lister's tubercle). It is then rerouted radially and volarly, often superficial to the abductor pollicis longus and extensor pollicis brevis in the first dorsal compartment, and sutured back onto itself or anchored to the first metacarpal base. This alters its biomechanical vector, changing it from a pure extensor/adductor into a powerful extensor and palmar abductor of the thumb.
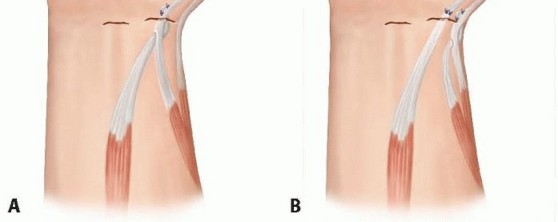
If additional power is needed due to profound weakness of the EPL, the brachioradialis (BR) or palmaris longus (PL) can be transferred. The brachioradialis is detached from its insertion on the radial styloid, mobilized proximally to free fascial attachments and ensure adequate excursion (typically 3 cm), and interwoven into the APL or EPB tendon using a Pulvertaft weave. Tensioning is critical; the transfer should be set with the thumb in full palmar abduction and extension while the wrist is in neutral.

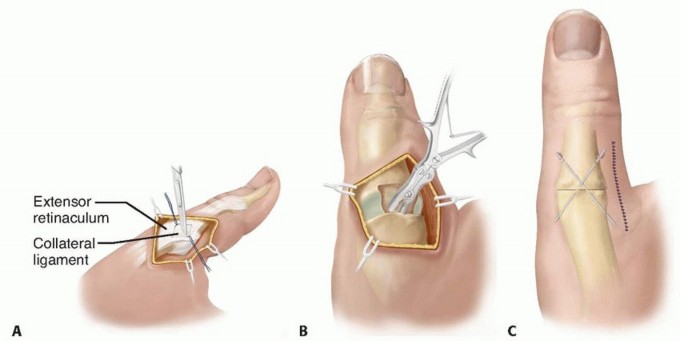
Joint Stabilization Procedures
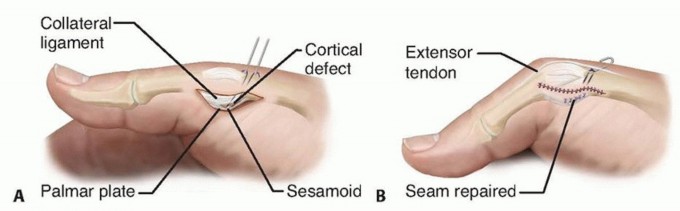
Addressing metacarpophalangeal joint hyperextension is absolutely mandatory to prevent functional failure of the reconstruction. If the joint is supple but hyperextends dynamically, a volar plate capsulodesis or sesamoidesis is performed. The volar plate is advanced and anchored into the metacarpal neck using suture anchors or transosseous sutures, effectively blocking hyperextension while preserving functional flexion.
In cases of fixed deformity, severe instability (collateral ligament attenuation), or in older adolescents, a formal MCP joint arthrodesis is the procedure of choice. The joint surfaces are prepared using a cup-and-cone reamer system to maximize cancellous bone contact and allow for precise multiaxial positioning. The joint is fused in approximately 15 to 20 degrees of flexion, 10 degrees of abduction, and slight pronation to optimize tip-to-tip and key pinch kinematics. Fixation is typically achieved with crossed Kirschner wires, a dorsal tension band construct, or a dedicated shape-memory compression staple.
Complications and Management
Surgical intervention for the spastic upper extremity is fraught with potential complications, primarily related to the unpredictable nature of spastic muscle, the delicate balance required for hand function, and the underlying static encephalopathy.

The most frequent complication is under-correction or recurrence of the deformity. This often results from inadequate initial release of the intrinsic muscles, failure to recognize an FPL contracture, or progressive spasticity during the patient's adolescent growth spurt (where bone growth outpaces spastic muscle-tendon unit elongation). Conversely, over-correction can lead to a fixed abduction-extension posture. This is equally detrimental to function, as the patient loses the ability to bring the thumb to the fingers for pinch, effectively creating an "apelike" hand.
| Complication | Incidence | Etiology | Salvage Strategy |
|---|---|---|---|
| Recurrent TIP Deformity | 10% - 20% | Inadequate release, adolescent growth spurt, poor splint compliance | Revision intrinsic release, formal Z-lengthening of FPL, CMC arthrodesis |
| Over-correction (Abduction Deformity) | 5% - 10% | Over-tensioned tendon transfer, excessive intrinsic release | Release/lengthening of transferred tendon, capsulorrhaphy |
| MCP Hyperextension Recurrence | 15% - 25% | Failure of capsulodesis, progressive intrinsic tightness | Revision to formal MCP arthrodesis |
| Web Space Contracture | 5% - 15% | Scar contracture, inadequate Z-plasty design | Revision Z-plasty, full-thickness skin grafting |
Meticulous surgical technique, precise tensioning of transfers, and rigid adherence to postoperative protocols are essential to minimize these risks. Complex regional pain syndrome (CRPS) is a rare but devastating complication in the CP population that requires immediate recognition and aggressive multimodal pain management, sympathetic blocks, and intensive desensitization therapy.

Post Operative Rehabilitation Protocols
The success of the surgical reconstruction is heavily dependent on the postoperative rehabilitation phase. Without dedicated therapy, the surgical gains are rapidly lost to scar contracture and recurrent spasticity. The initial postoperative management involves rigid immobilization. The patient is placed in a well-padded long-arm or short-arm thumb spica cast, depending on whether extrinsic forearm tendons were addressed. The thumb is immobilized in maximal palmar abduction and extension, with the interphalangeal joint left free if the flexor pollicis longus was not lengthened, or included in extension if it was.
Immobilization is maintained for 4 to 6 weeks to allow for tendon transfer healing and capsulodesis integration. Upon cast removal, a custom thermoplastic thumb spica splint is fabricated by the occupational therapist. The splinting regimen typically involves continuous wear (except for hygiene and supervised therapy) for an additional 4 weeks, followed by a transition to night-time only splinting for 6 to 12 months to prevent recurrence of myostatic contractures.
Occupational therapy is initiated immediately upon cast removal. The initial phase focuses on edema control, scar management (silicone elastomer, massage), and active range of motion. Neuromuscular re-education is critical, particularly if tendon transfers were performed. The patient must learn to activate the transferred muscle (e.g., BR) in its new biomechanical role through biofeedback and repetitive task practice. Therapy progresses to functional task training, emphasizing large object grasp, lateral key pinch, and fine motor manipulation.
Summary of Key Literature and Guidelines
The surgical management of the thumb-in-palm deformity is guided by several foundational academic works that have shaped modern orthopedic practice. The classification system proposed by House et al. remains the gold standard for categorizing the deformity based on the specific patterns of intrinsic and extrinsic involvement, as well as joint instability. This classification is vital for standardizing the surgical approach and allowing for reproducible research outcomes.
Manske's extensive work on the rerouting of the extensor pollicis longus has demonstrated that altering the vector of this tendon provides superior abduction and extension power compared to simple release alone, fundamentally changing the management of the weak CP thumb. Furthermore, long-term outcome studies by Smith and colleagues emphasize that while functional gains in grasp and pinch are achievable in patients with good voluntary control and proprioception, the most predictable outcome across all functional levels (including GMFCS V) is a significant improvement in hand hygiene and caregiver ease.
Current consensus guidelines from pediatric orthopedic and hand surgery societies strongly advocate for a single-stage, multi-level reconstruction (Single-Event Multilevel Surgery - SEMLS approach applied to the upper extremity). Staged procedures are generally discouraged due to the increased burden of multiple anesthetics, the
You Might Also Like

