Congenital Clubfoot (Talipes Equinovarus): Comprehensive Pathoanatomy and Surgical Management

Key Takeaway
Congenital clubfoot (talipes equinovarus) is a complex three-dimensional deformity characterized by cavus, adductus, varus, and equinus. Affecting approximately one in 1,000 live births, its management requires a profound understanding of subtalar biomechanics and soft-tissue contractures. While nonoperative serial casting remains the gold standard for initial treatment, rigid or recurrent deformities necessitate meticulous surgical intervention, ranging from posteromedial releases to corrective midfoot osteotomies, to achieve a plantigrade, functional foot.
CONGENITAL CLUBFOOT (TALIPES EQUINOVARUS)
Congenital clubfoot, or talipes equinovarus, represents one of the most complex and historically challenging pediatric foot deformities encountered by the orthopedic surgeon. The incidence of congenital clubfoot is approximately one in every 1,000 live births. Although the majority of cases manifest as sporadic occurrences, familial inheritance patterns have been documented, suggesting an autosomal dominant trait with incomplete penetrance. Bilateral deformities are observed in approximately 50% of patients.
To effectively manage this condition, the orthopedic surgeon must possess an exhaustive understanding of the three-dimensional pathoanatomy, the sequence of soft-tissue contractures, and the precise biomechanical alterations of the tarsal bones.
Fig. 1: Congenital clubfoot in a newborn. Posterior view demonstrating severe inversion, plantarflexion, and internal rotation of the calcaneus, alongside a cavus deformity with a deep transverse plantar crease.
Etiology and Pathogenesis
The precise etiology of congenital clubfoot remains multifactorial and heavily debated. Several prominent theories have been proposed:
1. Primary Germ Plasm Defect: This theory posits a primary osseous dysplasia within the talus, leading to continued plantarflexion and inversion. Secondary soft-tissue contractures subsequently develop in the surrounding capsuloligamentous and musculotendinous complexes.
2. Neuromuscular Theory: Proponents argue that primary soft-tissue abnormalities within the neuromuscular units (e.g., subtle imbalances or focal dysplasias) exert abnormal forces on the developing cartilaginous anlagen, causing secondary bony morphological changes.
3. Vascular Anomalies: Clinically, children with clubfoot frequently exhibit a hypotrophic or absent anterior tibial artery, relying heavily on the posterior tibial artery for pedal perfusion. This is accompanied by obvious atrophy of the calf musculature.
4. Histochemical Abnormalities: Histological analyses have documented an abnormal distribution and proportion of type I and type II muscle fibers in the posteromedial musculature of clubfeet.
Surgical Warning: The frequent presence of a hypotrophic anterior tibial artery makes the posterior tibial artery the dominant blood supply to the foot. Extreme caution must be exercised during posteromedial surgical releases to avoid catastrophic vascular compromise.
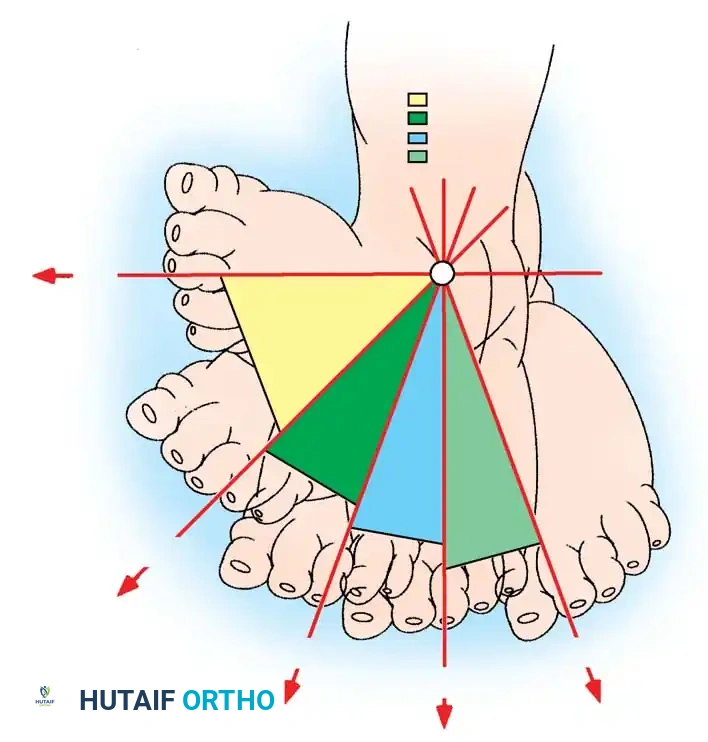
Fig. 2: Clinical presentation highlighting the profound medial deviation of the forefoot and the rigid equinus of the hindfoot.
Pathoanatomy and Biomechanics
The pathological changes inherent to congenital clubfoot must be conceptualized in three dimensions. The deformity is classically remembered by the acronym CAVE: Cavus (midfoot), Adductus (forefoot), Varus (hindfoot), and Equinus (hindfoot). The affected foot is typically one-half to one full size smaller in length and width compared to a normal foot, and the condition is universally accompanied by internal tibial torsion.
The Bony Deformity
The ankle, midtarsal, and subtalar joints are all intimately involved.
* Turco's Observations: In the 1970s, Turco revolutionized the surgical understanding of clubfoot by attributing the deformity to the medial displacement of the navicular and calcaneus around the talus. The talus is forced into equinus by the underlying calcaneus and navicular, while the talar head and neck deviate medially. The calcaneus is inverted under the talus; its posterior tuberosity is displaced upward and laterally, while its anterior process is displaced downward and medially.
* McKay's Kinematics: McKay expanded this into a three-dimensional model, emphasizing abnormal rotation in the sagittal, coronal, and horizontal planes. The calcaneus rotates horizontally, pivoting on the interosseous talocalcaneal ligament, slipping beneath the talar head anteriorly while the calcaneal tuberosity abuts the fibular malleolus posteriorly. This proximity to the fibula is driven by horizontal rotation, not merely equinus.
* Herzenberg's Computer Modeling: Utilizing 3D CT modeling, Herzenberg et al. demonstrated that the talar neck is internally rotated relative to the ankle mortise, but the talar body is externally rotated. The calcaneus is significantly internally rotated, and the sloped articular facet of the calcaneocuboid joint forces additional internal rotation of the midfoot.

Fig. 3: Severe bilateral talipes equinovarus demonstrating the classic CAVE deformity components.
Soft-Tissue Contractures
The bony malalignment is locked in place by severe soft-tissue contractures:
* Talocalcaneal Joint: Realignment is resisted by the calcaneofibular ligament, superior peroneal retinaculum, peroneal tendon sheaths, and the posterior talocalcaneal ligament.
* Talonavicular Joint: Medial reduction is opposed by the posterior tibial tendon, deltoid ligament (tibionavicular fibers), spring ligament (calcaneonavicular), dorsal talonavicular ligament, bifurcate ligament, inferior extensor retinaculum, and the master knot of Henry.
* Calcaneocuboid Joint: Internal rotation is tethered by the bifurcate ligament, long plantar ligament, plantar calcaneocuboid ligament, and the naviculocuboid ligament.

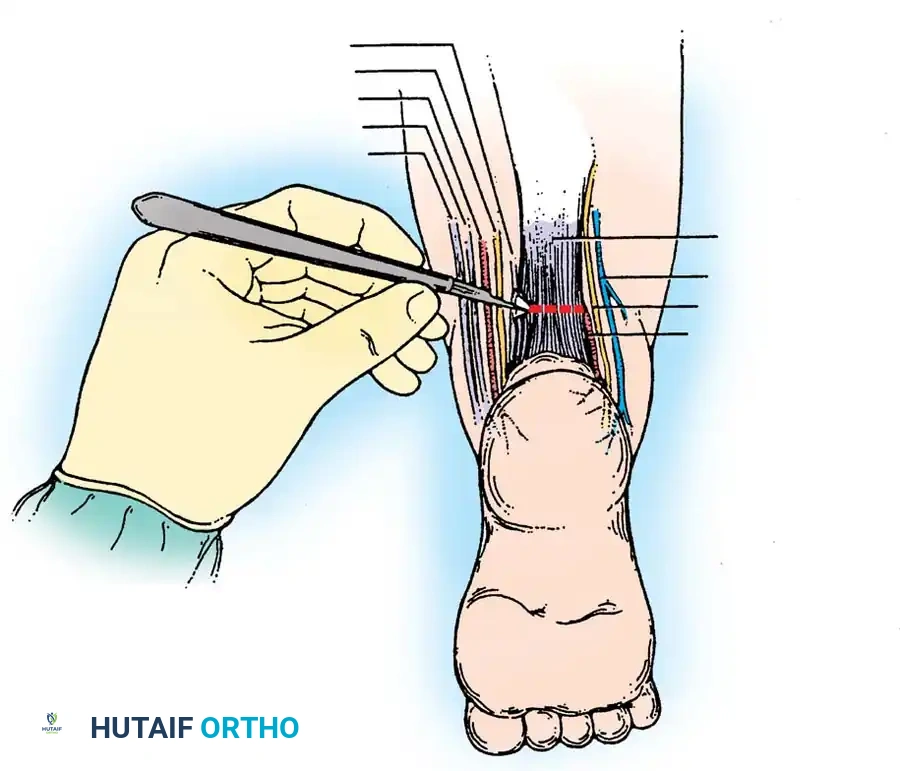
Fig. 4: Anatomical dissection diagram illustrating the contracted posteromedial structures that require meticulous release during surgical intervention.
CLINICAL EVALUATION AND CLASSIFICATION
Initial examination relies on clinical judgment to assess the rigidity of the deformity. Standardized classification systems are critical for predicting prognosis and comparing treatment outcomes.
Pirani and Diméglio Classification Systems
Two highly validated clinical classification schemes are widely utilized:
1. Pirani System: Comprises 10 physical examination findings, each scored 0 (normal), 0.5 (moderate), or 1 (severe). The maximum score is 10, with higher scores indicating greater severity and rigidity.
2. Diméglio System: Assesses four parameters based on their reducibility with gentle manipulation using a handheld goniometer:
* Equinus deviation in the sagittal plane.
* Varus deviation in the frontal plane.
* Derotation of the calcaneopedal block in the horizontal plane.
* Adduction of the forefoot relative to the hindfoot in the horizontal plane.
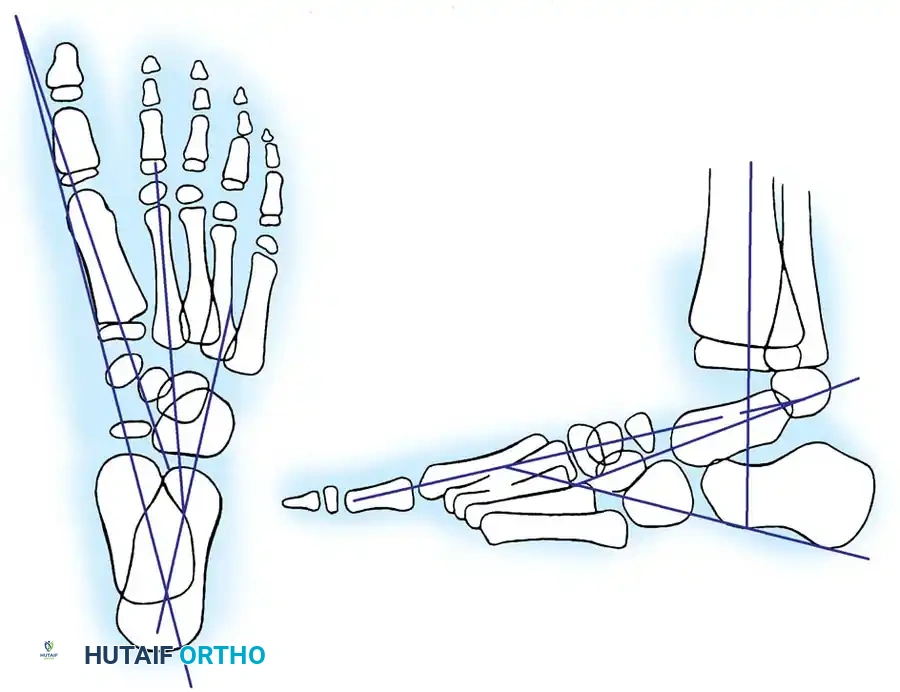
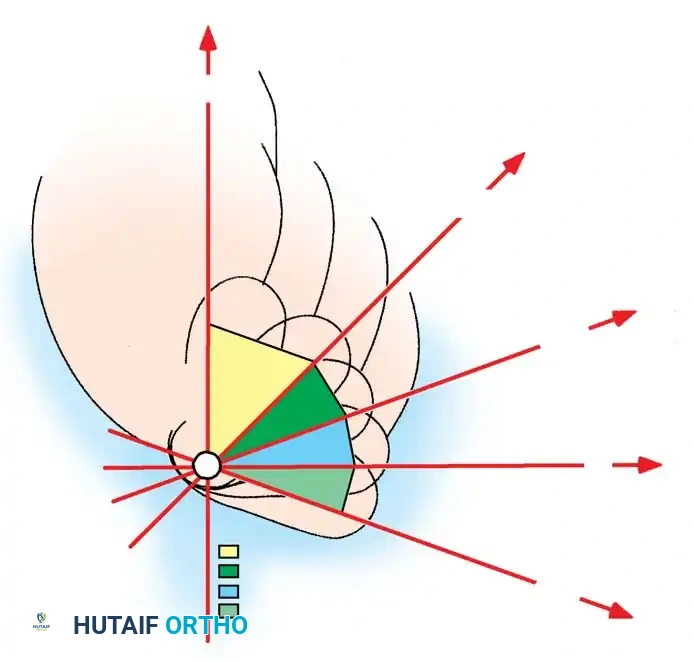
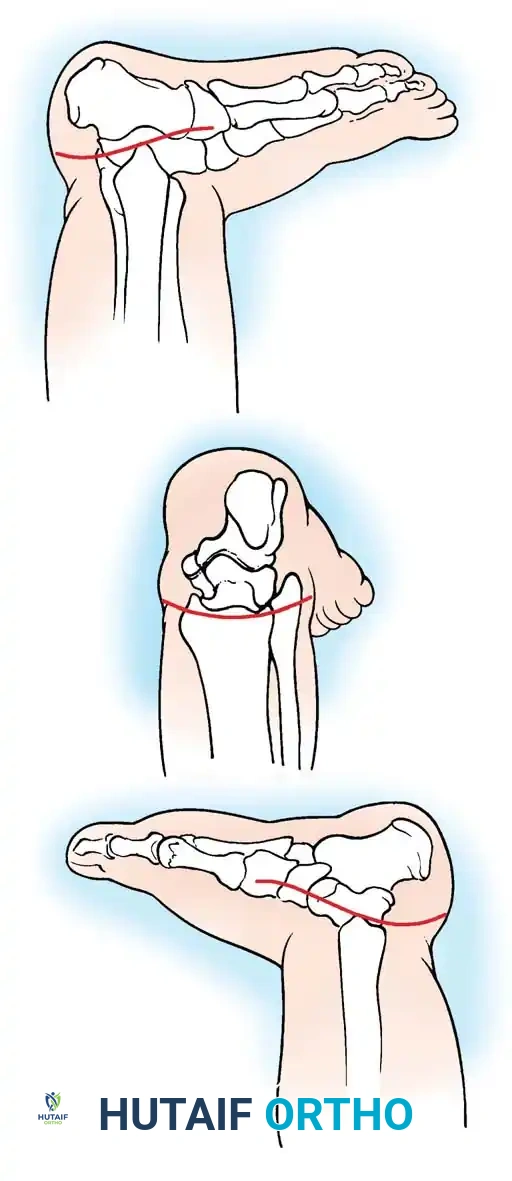
Fig. 5: The nine radiographic angles commonly used for the evaluation of clubfoot deformity, essential for preoperative planning and postoperative assessment.
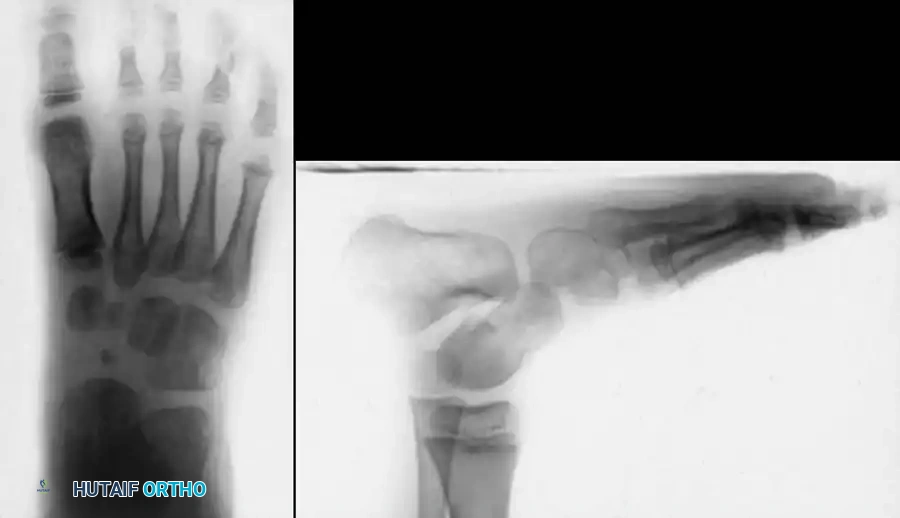
Fig. 6: Clinical assessment of hindfoot varus and forefoot adduction during the initial newborn examination.
RADIOGRAPHIC EVALUATION
Radiographs are an indispensable adjunct before, during, and after treatment to ensure that clinical correction correlates with true osseous realignment. In the non-ambulatory child, standard imaging includes anteroposterior (AP) and stress dorsiflexion lateral radiographs.
Key Radiographic Angles
- AP Talocalcaneal Angle (Kite's Angle): Normal is 30 to 55 degrees. In clubfoot, the talus and calcaneus are nearly parallel, progressively decreasing this angle toward 0 degrees as heel varus worsens.
- Lateral Talocalcaneal Angle: Normal is 25 to 50 degrees. In clubfoot, this angle decreases significantly.
- Stress Lateral Tibiocalcaneal Angle: Normal is 10 to 40 degrees. In clubfoot, this angle is often negative, indicating severe calcaneal equinus relative to the tibia.
- Talus–First Metatarsal Angle (AP View): Normal is 5 to 15 degrees. In clubfoot, it is usually negative, reflecting severe forefoot adduction.
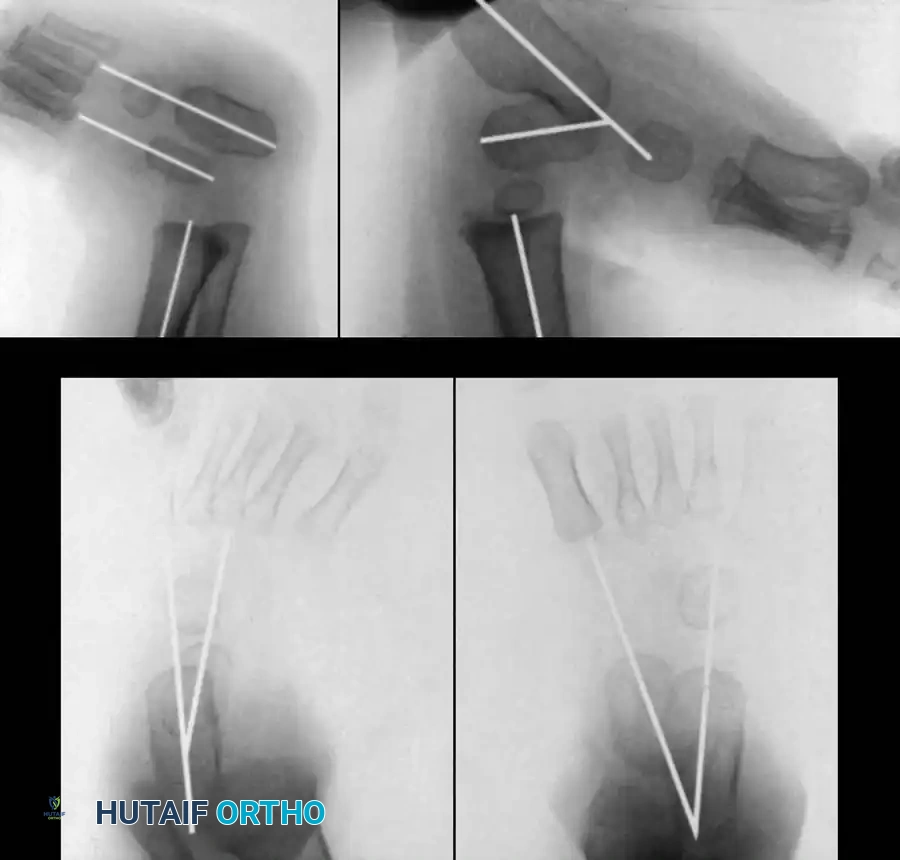
Fig. 7: Radiographic evaluation. (A) AP view of a right clubfoot showing a decreased talocalcaneal angle and negative talus-first metatarsal angle. (B) Normal AP view. (C) Dorsiflexion lateral view of a clubfoot showing parallel talus and calcaneus (0 degrees). (D) Normal lateral view.
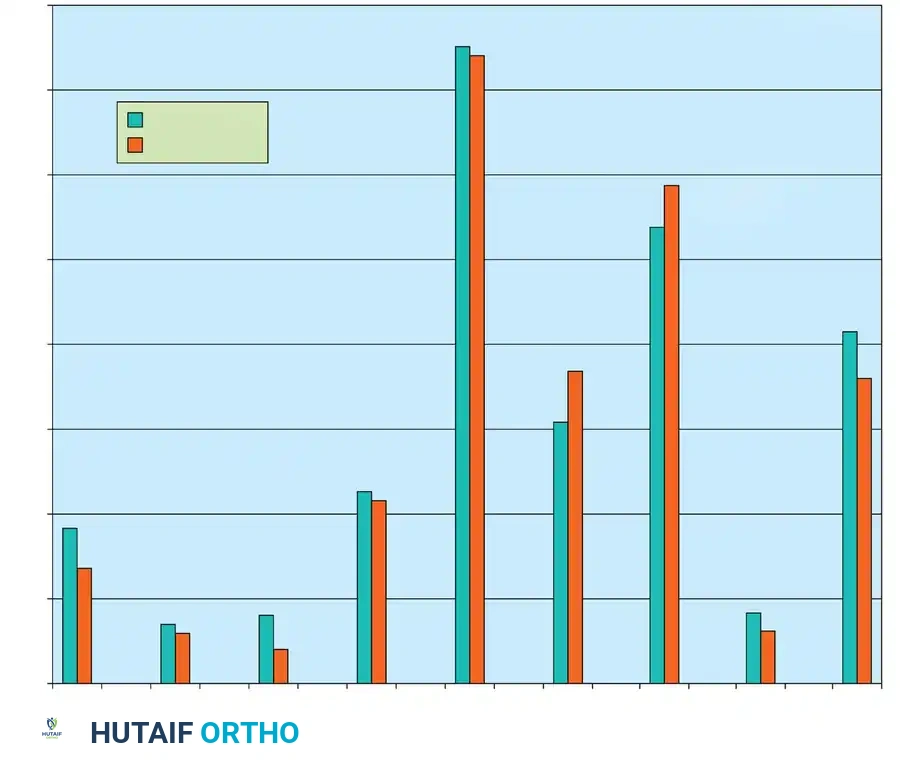
Fig. 8: Progression of foot angles in normal feet over an average 6-year follow-up, demonstrating the natural decrease in talocalcaneal angles with growth.
Clinical Pearl: Joseph et al. demonstrated that a difference of 20 degrees between the lateral talocalcaneal angles measured on stress dorsiflexion and plantarflexion views indicates a 93% probability that the hindfoot deformity has been adequately corrected.

Fig. 9: Preoperative AP and lateral radiographs demonstrating severe parallelism of the talus and calcaneus.
NONOPERATIVE MANAGEMENT
The initial treatment of congenital clubfoot is strictly nonoperative, ideally commencing within the first week of life. The Ponseti Method has become the international gold standard, relying on the principle of kinematic coupling of the subtalar joint.
Principles of Serial Casting
Treatment consists of weekly serial manipulation and long-leg casting. The order of correction is paramount and must strictly follow the CAVE sequence:
1. Cavus: Corrected first by elevating the first ray to align the forefoot with the hindfoot.
2. Adductus and Varus: Corrected simultaneously by abducting the supinated foot while applying counter-pressure over the lateral aspect of the talar head (NOT the calcaneocuboid joint).
3. Equinus: Corrected last. Once the foot is fully abducted (typically 60-70 degrees), dorsiflexion is attempted. If dorsiflexion to 15 degrees is not achievable, a percutaneous Achilles tenotomy is performed.
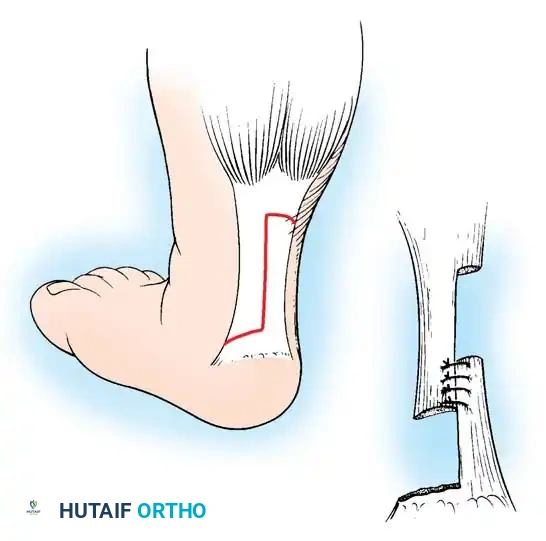
Fig. 10: Application of the long-leg plaster cast. The knee is flexed to 90 degrees to control tibial rotation and prevent the cast from slipping.

Fig. 11: Serial casting progression. Note the gradual improvement in forefoot adduction and hindfoot varus over successive weeks.

Fig. 12: Final cast applied post-percutaneous Achilles tenotomy, holding the foot in maximum abduction and dorsiflexion for 3 weeks.
SURGICAL MANAGEMENT
While the Ponseti method boasts success rates exceeding 90%, surgical intervention is indicated for rigid, syndromic (e.g., arthrogryposis, myelomeningocele), or neglected clubfeet that fail conservative management. The goal of surgery is to achieve a plantigrade, pliable, and pain-free foot.
Indications for Surgery
- Failure to achieve clinical and radiographic correction after exhaustive serial casting.
- Recurrence of deformity unresponsive to repeat casting.
- Late-presenting clubfoot in older children.
- Severe syndromic clubfoot with rigid teratologic contractures.
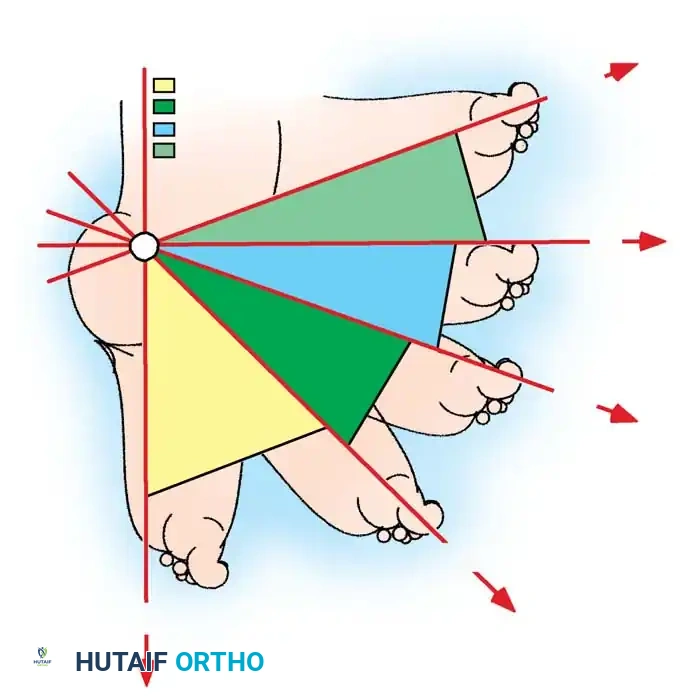
Fig. 13: A rigid, recurrent clubfoot deformity in an older child, representing a clear indication for comprehensive posteromedial release.
Comprehensive Posteromedial Release (PMR)
The surgical approach must allow extensive exposure of the medial, posterior, and lateral compartments of the subtalar complex. The Cincinnati incision (a transverse incision extending from the medial navicular, across the posterior heel crease, to the lateral fibula) or the Turco posteromedial incision are most commonly utilized.
Step-by-Step Surgical Technique
1. Positioning and Preparation:
The patient is placed prone or in a lateral decubitus position to allow access to the posterior and medial aspects of the foot. A pneumatic tourniquet is applied to the proximal thigh.
2. Incision and Superficial Dissection:
Using a Cincinnati incision, the skin and subcutaneous tissues are elevated as a full-thickness flap. The sural nerve and lesser saphenous vein are identified and protected laterally. Medially, the neurovascular bundle (posterior tibial artery and tibial nerve) is meticulously isolated and protected with vessel loops.

Fig. 14: Intraoperative view of the Cincinnati incision, providing circumferential access to the posterior and medial hindfoot structures.
3. Posterior Release:
* The Achilles tendon is identified and lengthened via a Z-plasty (usually leaving the medial half attached distally to aid in subsequent eversion).
* The deep fascia is incised, exposing the posterior ankle and subtalar joints.
* A posterior capsulotomy of the tibiotalar and talocalcaneal joints is performed. The posterior talofibular and calcaneofibular ligaments are sectioned to allow the calcaneus to translate anteriorly and laterally.

Fig. 15: Z-lengthening of the Achilles tendon and exposure of the posterior ankle capsule.
4. Medial Release:
* The sheaths of the tibialis posterior (PT), flexor digitorum longus (FDL), and flexor hallucis longus (FHL) are opened.
* The PT tendon is lengthened via Z-plasty.
* The master knot of Henry is released to allow independent excursion of the FDL and FHL.
* The talonavicular joint capsule is circumferentially released. The spring ligament (calcaneonavicular) and the superficial deltoid ligament (tibionavicular) are sectioned.
* Crucial Step: The navicular must be completely mobilized to allow it to be reduced laterally onto the head of the talus.
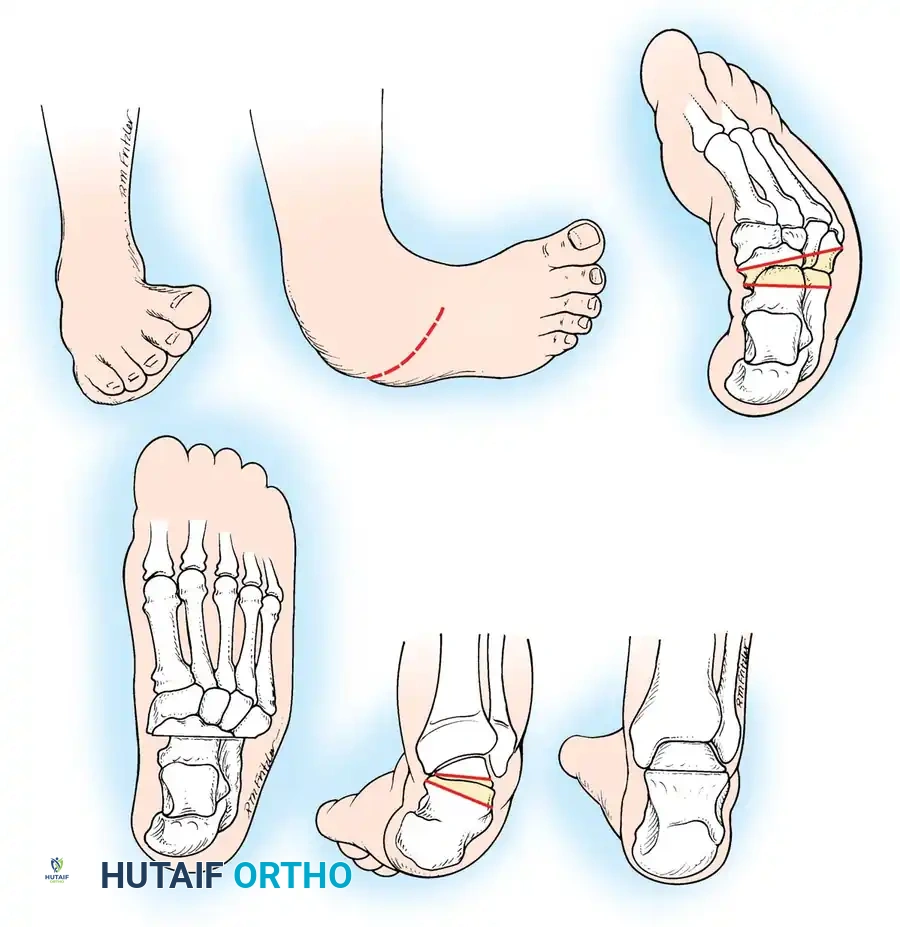
Fig. 16: Isolation of the medial neurovascular bundle and lengthening of the tibialis posterior tendon.
5. Lateral and Plantar Release (If necessary):
* If severe cavus persists, a plantar fasciotomy and release of the abductor hallucis origin are performed (Steindler stripping).
* The bifurcate ligament and calcaneocuboid joint capsule may be released if lateral column shortening is required to correct severe adductus.
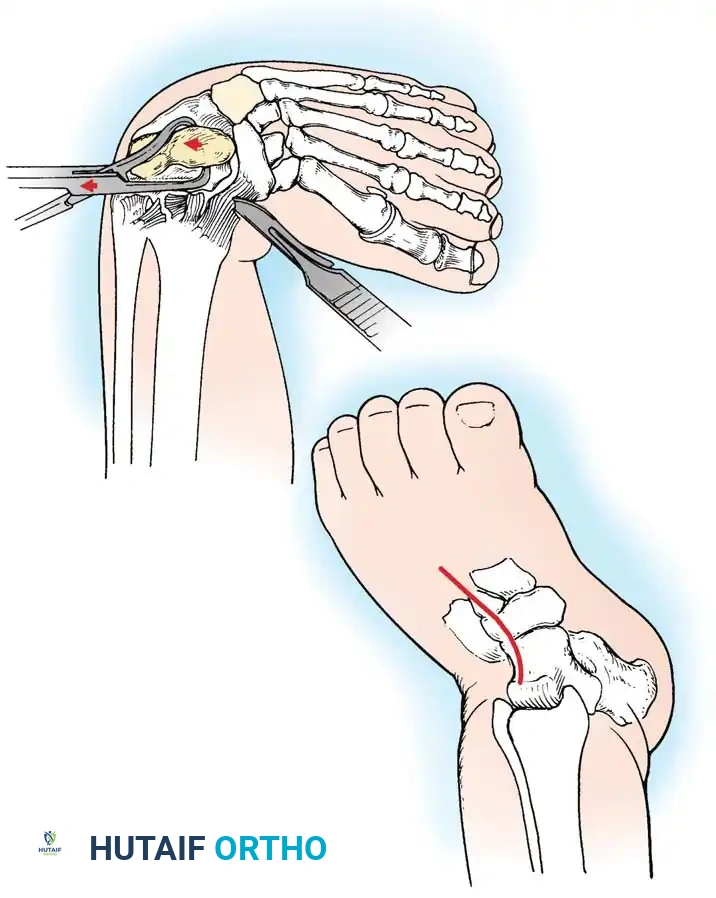
Fig. 17: Plantar release demonstrating the sectioning of the plantar fascia and intrinsic muscle origins to correct the cavus component.
6. Reduction and Fixation:
* The navicular is reduced onto the talar head and pinned with a smooth Kirschner wire (K-wire).
* The calcaneus is rotated externally and translated laterally beneath the talus, correcting the varus and equinus. A second K-wire is driven from the heel across the talocalcaneal joint.
* Intraoperative radiographs are obtained to confirm the restoration of the talocalcaneal and talus-first metatarsal angles.

Fig. 18: Intraoperative fluoroscopy confirming the reduction of the talonavicular joint and the placement of stabilizing K-wires.
7. Closure:
The tendons (Achilles, PT) are repaired in their lengthened positions. The tourniquet is deflated to ensure adequate perfusion before skin closure. If skin tension is excessive, the wound may be left partially open to heal by secondary intention, or a delayed primary closure is planned. A well-padded, long-leg cast is applied with the knee flexed and the foot in a plantigrade position.

Fig. 19: Postoperative long-leg cast application following comprehensive posteromedial release.
Bony Procedures for Residual or Late Deformity
In older children (typically >4 years) where adaptive bony changes have occurred, soft-tissue releases alone are insufficient. Bony osteotomies are required to correct the lateral column overgrowth and medial column shortening.
McHale Procedure (Medial Cuneiform Opening Wedge and Cuboid Closing Wedge)
For residual "bean-shaped" foot deformities characterized by severe midfoot adductus:
1. Lateral Incision: A closing wedge osteotomy of the cuboid is performed to shorten the lateral column.
2. Medial Incision: An opening wedge osteotomy of the medial cuneiform is performed.
3. Graft Transfer: The bony wedge excised from the cuboid is meticulously shaped and impacted into the medial cuneiform osteotomy to lengthen the medial column.
4. Fixation: Both osteotomies are stabilized with K-wires.
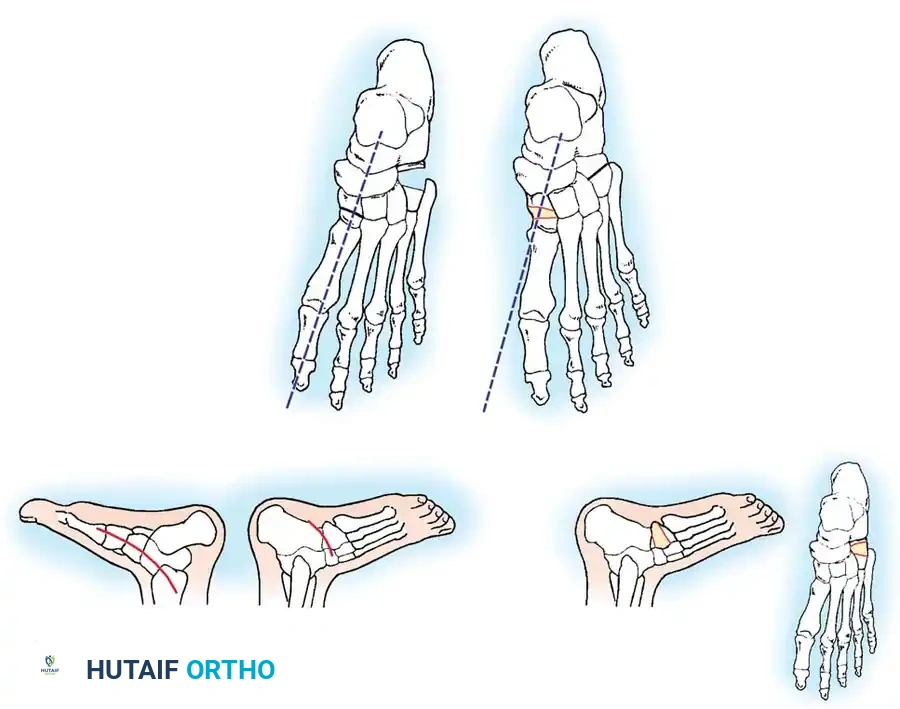
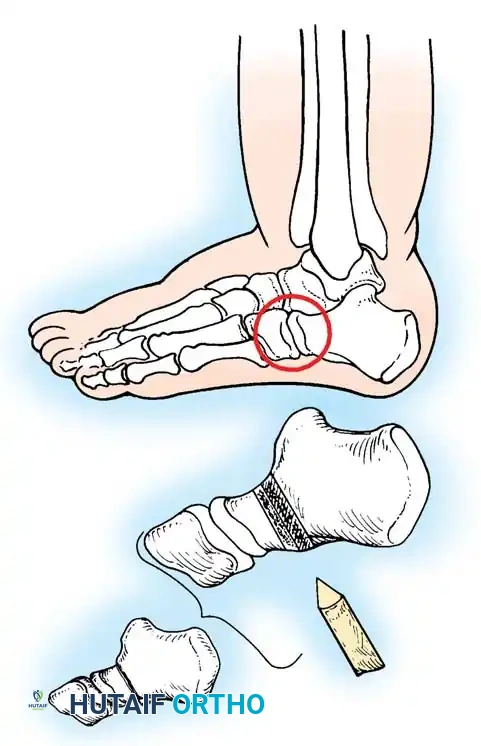
Fig. 20: Osteotomies of the medial cuneiform and cuboid for correction of residual deformity. (A) Lateral and medial incisions. (B) Removal of dorsolateral wedge from the cuboid. (C) Placement of the wedge into the opening osteotomy of the medial cuneiform.
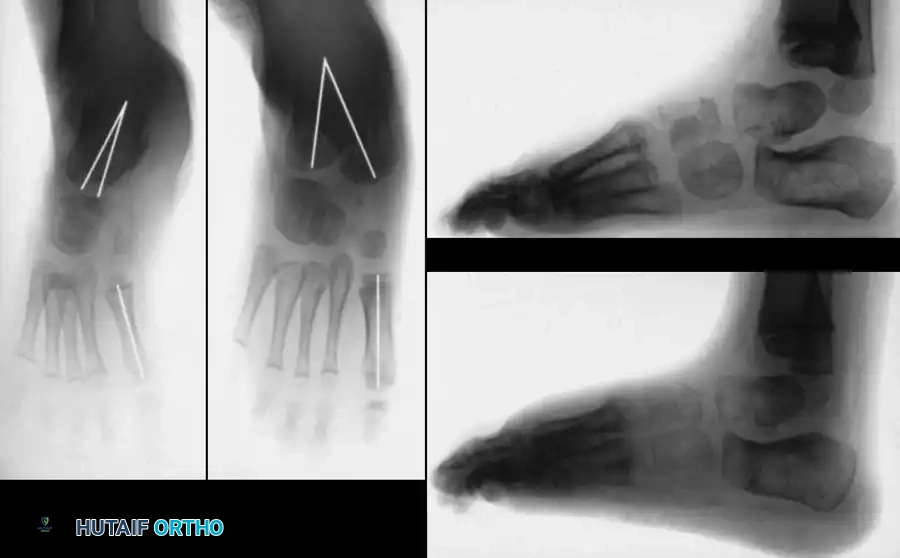
Fig. 21: Radiographic appearance post-midfoot osteotomies, demonstrating restoration of the straight lateral border of the foot.

Fig. 22: Clinical appearance of the foot following successful McHale procedure, showing excellent correction of the midfoot adductus.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Rehabilitation and Bracing
- 0-6 Weeks: The patient remains non-weight-bearing in a long-leg cast.
- 6 Weeks: The cast and K-wires are removed in the clinic or under light sedation. A short-leg walking cast may be applied for an additional 4 weeks.
- Long-term Maintenance: Following cast removal, the patient is transitioned to a foot abduction orthosis (e.g., Denis Browne splint or Mitchell brace) worn full-time for 3 months
Associated Surgical & Radiographic Imaging


📚 Medical References
- congenital clubfoot or congenital metatarsus varus, J Bone Joint Surg 40A:299, 1958.
- Katz K, David R, Soudry M: Below-knee plaster cast for the treatment of metatarsus adductus, J Pediatr Orthop 19:49, 1999.
- Kendrick RE, Sharma NK, Hassler WL, et al: Tarsometatarsal mobilization for resistant adduction of the fore part of the foot: a follow-up study, J Bone Joint Surg 52A:61, 1970.
- Lichtblau S: Section of the abductor hallucis tendon for correction of metatarsus varus deformity, Clin Orthop Relat Res 110:227, 1975.
- Ponseti IV, Becker JR: Congenital metatarsus adductus: the results of treatment, J Bone Joint Surg 48A:702, 1966.
- Stark JG, Johnson JE, Winter RB: The Heyman-Herndon tarsometatarsal capsulotomy for metatarsus adductus: results in 48 feet, J Pediatr Orthop 7:305, 1987.
- Theodorou DJ, Theodorou SJ, Boutin RD, et al: Stress fractures of the lateral metatarsal bones in metatarsus adductus foot deformity: a previously unrecognized association, Skeletal Radiol 28:679, 1999.
- Clubfoot Addison A, Fixen JA, Lloyd-Roberts GC: A review of the Dillwyn Evans type collateral operation in severe clubfoot, J Bone Joint Surg 65B:12, 1983.
- Allington NJ, Kumar SJ, Guille JT: Clubfeet associated with
You Might Also Like

