Cerebral Palsy of the Hand: Comprehensive Surgical Management

Key Takeaway
Cerebral palsy of the hand presents complex spastic deformities, including forearm pronation, wrist flexion, and thumb-in-palm contractures. Successful management requires meticulous patient evaluation using the MACS and House classifications. Treatment ranges from nonoperative splinting and targeted nerve blocks to complex surgical interventions like tendon transfers and releases. The primary goal is to enhance functional capacity, improve hygiene, and correct biomechanical imbalances in the spastic upper extremity.
CEREBRAL PALSY OF THE HAND
Cerebral palsy (CP) encompasses a heterogeneous group of non-progressive, permanent disorders of movement and posture caused by a static insult to the developing fetal or infant brain. In the upper extremity, the spastic hemiplegic pattern is the most common presentation, characterized by a predictable cascade of deformities: shoulder internal rotation, elbow flexion, forearm pronation, wrist and finger flexion, and a thumb-in-palm posture.
The management of the spastic hand is one of the most challenging domains in orthopedic surgery. It requires a profound understanding of altered biomechanics, meticulous patient selection, and a tailored combination of nonoperative and operative strategies to optimize function and hygiene.
PATIENT EVALUATION
The cornerstone of successful intervention in the cerebral palsy hand is a rigorous, repeated clinical evaluation. Because the neurologic insult is static but the musculoskeletal manifestations are dynamic and progressive, the clinical picture evolves as the child grows.
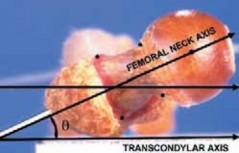
Evaluation must differentiate between dynamic spasticity (muscle overactivity that resolves under anesthesia or nerve block) and fixed myostatic contracture (structural shortening of the musculotendinous unit and joint capsule).
CLINICAL PEARL: Diagnostic nerve blocks using local anesthetics (e.g., lidocaine), or targeted motor point blocks using ethanol, phenol, or botulinum toxin, are invaluable. They temporarily eliminate the overbearing effect of spastic antagonist muscles, allowing the surgeon to assess the latent strength of weaker, underlying agonist muscle groups. This is critical for predicting surgical outcomes after tendon lengthening or tenotomy.
Functional Classification Systems
Standardized classification systems are essential for establishing baseline function, guiding surgical indications, and evaluating postoperative outcomes. The two most widely utilized systems are the House Classification and the Manual Ability Classification System (MACS).
Table 72-1: Upper Extremity Functional Use in Patients Before and After Surgery (According to the Classification of House et al.)
| Level | Category | Description | Before Surgery* | After Surgery* |
|---|---|---|---|---|
| 0 | Does not use | Does not use | 11 | 0 |
| 1 | Poor passive assist | Uses as stabilizing weight only | 44 | 0 |
| 2 | Fair passive assist | Can hold object placed in hand | 27 | 7 |
| 3 | Good passive assist | Can hold object and stabilize it for use by other hand | 4 | 30 |
| 4 | Poor active assist | Can actively grasp object and hold it weakly | 45 | 6 |
| 5 | Fair active use | Can actively grasp object and stabilize it well | 0 | 23 |
| 6 | Good active assist | Can actively grasp object and manipulate it | 0 | 48 |
| 7 | Spontaneous use, partial | Can perform bimanual activities and occasionally uses the hand spontaneously | 1 | 12 |
| 8 | Spontaneous use, complete | Uses hand completely independently without reference to the other hand | 0 | 4 |
(Data adapted from Van Heest AE, House JA, Cariello C: Upper extremity surgical treatment of cerebral palsy, J Hand Surg 24A:323, 1999. Numbers represent patient cohorts demonstrating functional shifts post-intervention).
Table 72-2: Summary of Manual Ability Classification System (MACS)
| MACS Level | Description |
|---|---|
| I | Handles most objects easily and successfully. |
| II | Handles most objects with somewhat reduced quality or speed of achievement. |
| III | Handles objects with difficulty; needs help to prepare or modify activities. |
| IV | Handles a limited selection of easily managed objects in adapted situations. |
| V | Does not handle objects and has severely limited ability to perform even simple actions. |
(From Arner M, Eliasson AC, Nicklasson S, et al: Hand function in cerebral palsy: report of 367 children in a population-based longitudinal health care program, J Hand Surg 33A:1337, 2008).
NONOPERATIVE MANAGEMENT
Nonoperative management is the first line of treatment and remains a critical adjunct even when surgery is indicated. The primary goals are to prevent fixed contractures, maintain joint suppleness, and maximize functional use during the child's early developmental years.
- Physical and Occupational Therapy: Focuses on passive stretching, active range of motion (ROM) exercises, and bimanual skills training.
- Orthotic Management: Splinting is utilized to maintain the hand and wrist in a functional position, counteracting the spastic flexor and pronator forces. Night splinting is particularly effective in preventing myostatic contractures.
FIGURE 72-2 Splint for spastic hand. A custom-molded volar resting splint designed to maintain the wrist in neutral to slight extension, fingers in functional flexion, and the thumb abducted out of the palm.
- Chemodenervation: Botulinum toxin type A (Botox) injections provide temporary relief of focal spasticity (lasting 3 to 6 months). This creates a "window of opportunity" for aggressive therapy, serial casting, and functional assessment prior to definitive surgical intervention.
OPERATIVE MANAGEMENT
GOALS
Surgical intervention in the spastic hand is generally considered when nonoperative measures fail to prevent contracture or when a plateau in functional improvement is reached. The overarching goals are:
1. Improvement of Function: Enhancing grasp, release, and bimanual dexterity.
2. Improvement of Hygiene and Care: Facilitating dressing, washing, and preventing skin maceration in severely contracted, non-functional hands.
3. Cosmesis: Normalizing the appearance of the limb, which has profound psychosocial benefits for the developing child.
PRINCIPLES
- Timing: Surgery is typically deferred until the child is at least 6 to 8 years old. By this age, neurologic maturation is complete, spontaneous improvement is unlikely, and the child is mature enough to cooperate with rigorous postoperative rehabilitation.
- Global Assessment: The upper extremity must be treated as a single kinetic chain. Proximal deformities (shoulder, elbow) can profoundly affect distal function and must be addressed either prior to or concurrently with hand surgery.
- Surgical Hierarchy: Address contractures first (via releases or lengthenings), followed by augmentation of weak antagonists (via tendon transfers), and finally, joint stabilization (via arthrodesis or tenodesis) if dynamic balancing is impossible.
SURGICAL WARNING: Over-lengthening of spastic flexors is a catastrophic error that can lead to a non-functional, flail hand. Fractional lengthening at the musculotendinous junction is strongly preferred over Z-lengthening of the tendon proper to preserve muscle power.
PRONATION CONTRACTURE OF THE FOREARM
Pronation deformity is driven primarily by spasticity of the pronator teres (PT) and, to a lesser extent, the pronator quadratus. This posture severely limits the patient's ability to accept objects into the palm (which requires supination).
Operative Technique: Pronator Teres Rerouting
Rerouting the pronator teres converts its deforming pronation force into a weak supination force, actively correcting the deformity while preserving the muscle's stabilizing effect on the radius.
- Incision: A longitudinal incision is made over the middle third of the radial aspect of the forearm.
- Dissection: The interval between the brachioradialis (BR) and the extensor carpi radialis longus (ECRL) is developed. The superficial radial nerve is identified and protected.
- Tendon Harvest: The broad, flat insertion of the PT on the middle third of the radius is identified. It is elevated with a strip of periosteum to maximize length.
- Rerouting: The interosseous membrane is identified. The PT tendon is passed posterior to the radius (through the interosseous space) from volar to dorsal.
- Reattachment: The tendon is passed laterally and reattached to its original insertion site on the radius using suture anchors or transosseous sutures, with the forearm held in maximal supination.
FLEXION DEFORMITIES OF THE WRIST AND FINGERS
Flexion deformities of the wrist and fingers are the hallmark of the spastic upper extremity. The flexor carpi ulnaris (FCU) is typically the most spastic muscle, pulling the wrist into severe flexion and ulnar deviation. The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) contribute to the clenched fist posture.
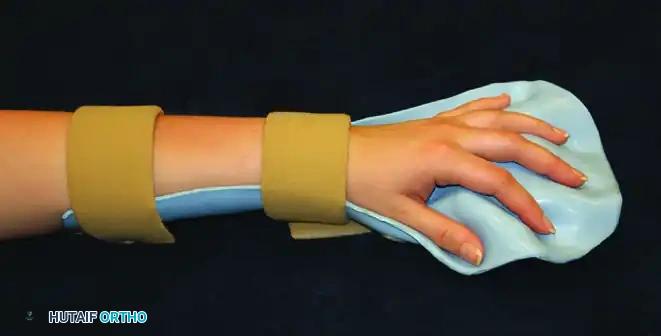
FIGURE 72-1 Typical upper extremity deformities in cerebral palsy: elbow flexion, forearm pronation, and wrist and finger flexion.
Operative Technique: Fractional Lengthening of Finger Flexors
Fractional lengthening allows for controlled elongation of the muscle while maintaining the continuity of the muscle fibers, thereby preserving grip strength.
- Incision: A volar longitudinal incision is made over the distal third of the forearm.
- Exposure: The antebrachial fascia is incised. The FDS and FDP musculotendinous junctions are systematically identified.
- Lengthening: Transverse incisions are made through the tendinous aponeurosis of the FDS and FDP, taking meticulous care to leave the underlying red muscle fibers intact.
- Stretching: The wrist and fingers are passively extended. The intact muscle fibers stretch, allowing the aponeurotic gaps to widen by 1 to 2 cm, effectively lengthening the unit.
Operative Technique: FCU to ECRB Tendon Transfer (Green's Transfer)
When wrist extension is weak or absent, transferring the spastic FCU to the extensor carpi radialis brevis (ECRB) provides active wrist extension and removes the primary deforming flexor force.
- Harvest: Through a volar-ulnar incision, the FCU is detached from its insertion on the pisiform. It is mobilized proximally to the mid-forearm, carefully preserving its proximal motor nerve branches from the ulnar nerve.
- Preparation of ECRB: A dorsal longitudinal incision is made over the wrist. The ECRB tendon is identified (central to the wrist, inserting on the base of the third metacarpal).
- Transfer: A wide subcutaneous tunnel is created around the ulnar border of the forearm. The FCU is passed through this tunnel to the dorsal wound.
- Weave and Fixation: The FCU is woven through the ECRB tendon using a Pulvertaft weave. Tension is set with the wrist in 30 to 45 degrees of extension and the forearm in neutral rotation.
THUMB-IN-PALM DEFORMITY
The thumb-in-palm deformity is a complex, multi-planar contracture that obliterates the first web space, preventing the patient from grasping large objects. It is caused by spasticity of the adductor pollicis, flexor pollicis brevis (FPB), first dorsal interosseous, and flexor pollicis longus (FPL), combined with weakness of the thumb extensors and abductors.
Treatment and Surgical Steps
Surgical correction requires a combination of intrinsic muscle release, web space deepening, and extrinsic tendon augmentation.
- First Web Space Release:
- A Z-plasty or four-flap Z-plasty is designed over the first web space to release the contracted skin.
- The fascia over the first dorsal interosseous is released.
- Adductor Pollicis Release:
- Through the web space incision, the transverse head of the adductor pollicis is identified and released from its origin on the third metacarpal shaft.
- If severe, the oblique head and the deep head of the FPB may also require release.
- FPL Lengthening: If the interphalangeal (IP) joint of the thumb is severely flexed, fractional lengthening of the FPL is performed at the musculotendinous junction in the distal forearm.
- Tendon Transfer for Thumb Extension: To augment weak thumb extension/abduction, the brachioradialis (BR) or palmaris longus (PL) can be transferred to the abductor pollicis longus (APL) or extensor pollicis brevis (EPB).
PITFALL: Failure to adequately release the adductor pollicis origin will result in rapid recurrence of the thumb-in-palm deformity, regardless of the strength of the tendon transfers performed.
SWAN-NECK DEFORMITY
Swan-neck deformity in cerebral palsy is characterized by proximal interphalangeal (PIP) joint hyperextension and distal interphalangeal (DIP) joint flexion. Unlike rheumatoid arthritis, where the deformity originates from terminal tendon rupture or PIP joint synovitis, the CP swan-neck is driven by intrinsic muscle spasticity pulling on the central slip, combined with secondary stretching of the PIP volar plate.
Operative Technique: Sublimis Tenodesis
When the PIP joint is supple but hyperextends dynamically, a sublimis (FDS) tenodesis is highly effective in creating a volar tether to prevent hyperextension.
- Incision: A mid-lateral or volar Brunner incision is made over the affected digit from the proximal phalanx to the middle phalanx.
- Exposure: The flexor tendon sheath is exposed. The A3 pulley is preserved.
- Tenodesis: One slip of the FDS tendon is divided proximally. The distal stump is left attached to the middle phalanx.
- Fixation: The proximal end of the divided FDS slip is routed volar to the PIP joint axis and anchored into the bone of the proximal phalanx (or sutured to the A2 pulley) with the PIP joint held in 20 to 30 degrees of flexion.
- Alternative (SORL): A Spiral Oblique Retinacular Ligament (SORL) reconstruction can be performed using a free tendon graft to simultaneously correct PIP hyperextension and DIP flexion.
POSTOPERATIVE PROTOCOLS
Meticulous postoperative care is as critical as the surgical execution.
* Immobilization: The upper extremity is immobilized in a bulky, long-arm cast for 4 to 6 weeks. The wrist is typically casted in slight extension, the forearm in supination, and the thumb abducted.
* Therapy: Upon cast removal, a custom thermoplastic splint is fabricated. Intensive occupational therapy commences immediately, focusing on active mobilization of tendon transfers and neuromuscular re-education.
* Long-term Splinting: Night splinting is often continued for 6 to 12 months postoperatively to protect tendon transfers from the relentless pull of underlying spasticity during sleep.
You Might Also Like