Orthopaedic Management of Cerebral Palsy: Etiology & Classification
Key Takeaway
Cerebral palsy represents a heterogeneous group of nonprogressive neurodevelopmental disorders affecting movement and posture. While the initial neurological insult occurs in the developing brain, the musculoskeletal manifestations are highly dynamic. This guide provides an evidence-based overview of the etiology, pathophysiology, and classification of cerebral palsy, serving as a foundational resource for orthopaedic surgeons managing the complex, evolving musculoskeletal deformities associated with this condition.
Introduction to Cerebral Palsy in Orthopaedics
Cerebral palsy (CP) is a heterogeneous, overarching term used to describe a group of permanent, nonprogressive disorders of movement and posture caused by a static insult to the developing fetal or infant brain. The clinical presentation is highly variable, ranging from mildly affected individuals with subtle motor disturbances to severely involved patients with total body impairment, profound intellectual disability, and complex medical comorbidities.
Because of this vast phenotypic variability and the absence of a single definitive diagnostic biomarker, defining the exact parameters of cerebral palsy has historically been challenging. However, the international medical community generally agrees upon three distinctive, unifying features common to all patients with cerebral palsy:
- Motor Impairment: Some degree of motor impairment must be present. This distinguishes CP from primary cognitive or behavioral conditions, such as global developmental delay or autism spectrum disorder.
- Developing Brain Insult: An insult to the developing brain has occurred. This differentiates CP from neurodegenerative conditions or traumatic brain injuries that affect the mature brain in older children and adults. The critical window for this insult is generally accepted to be between conception and 2 years of age.
- Nonprogressive Neurological Deficit: The underlying neurological lesion is static and nonprogressive. This is a critical distinction from progressive motor diseases of childhood, such as spinal muscular atrophy or the muscular dystrophies.
Clinical Pearl: While the neurological deficit in cerebral palsy is permanent and nonprogressive, the musculoskeletal manifestations are highly dynamic. The orthopaedic surgeon must recognize that a static encephalopathy combined with somatic growth leads to progressive loss of motion, dynamic contractures, fixed deformities, and eventually joint subluxation or dislocation.
By 8 years of age, the majority of the immature brain's development is complete, and mature gait patterns are typically established. Insults to the brain after this developmental milestone result in a more adult-type clinical picture (e.g., traumatic brain injury or stroke) rather than classic cerebral palsy.
Epidemiology and Prevalence
Children with cerebral palsy constitute the largest single demographic of pediatric patients with neuromuscular disorders in the United States and globally. The prevalence of cerebral palsy varies internationally, heavily influenced by the availability and quality of prenatal care, maternal socioeconomic status, environmental factors, and the sophistication of obstetrical and neonatal intensive care.
Determining the true prevalence is complicated by delayed diagnoses; many children with mild involvement are not formally diagnosed until 2 to 3 years of age, particularly in socioeconomic groups with limited access to specialized pediatric care.
- United States Prevalence: The incidence is approximately 2 to 2.5 per 1,000 live births. This translates to roughly 25,000 new diagnoses annually, with an estimated 400,000 children living with CP at any given time.
- Historical Trends: In the 1950s and 1960s, the U.S. experienced a transient decrease in CP incidence due to the advent of Rho(D) immune globulin (improving the management of maternal-fetal Rh incompatibility) and advancements in obstetrical techniques.
- Modern Trends: It was previously hypothesized that the prevalence of CP was increasing due to the enhanced survival rates of extremely premature and low-birth-weight infants. However, large population-based epidemiological studies have demonstrated that while the survival of these fragile infants has improved, it has not led to a statistically significant increase in the overall prevalence of CP.
- Global Prevalence: Worldwide, the prevalence exhibits a wider range, from 0.6 to 7 cases per 1,000 live births, reflecting disparities in global healthcare infrastructure.
Etiology and Timing of Brain Injury
Injury to the developing brain can occur at any point from early gestation through early childhood. The etiology is typically categorized chronologically into prenatal, perinatal, and postnatal periods.
Surgical Warning: Contrary to historical dogma and popular medicolegal belief, fewer than 10% of injuries resulting in cerebral palsy occur during the actual birth process (intrapartum asphyxia). The vast majority of insults occur during the prenatal period.
Prenatal Factors
The prenatal period accounts for the largest percentage of CP cases. A wide variety of risk factors have been identified:
* Fetal Factors: Genetic disorders, congenital brain malformations, and chromosomal abnormalities.
* Maternal Factors: Maternal seizure disorders, cognitive impairment, thyroid disease, and a history of previous pregnancy loss.
* Pregnancy-Specific Factors: Rh incompatibility, polyhydramnios, placental abruption, placental insufficiency, and maternal exposure to teratogens (drugs or alcohol).
* Infectious Agents: The TORCH complex (Toxoplasmosis, Other agents [e.g., syphilis, varicella], Rubella, Cytomegalovirus, Herpes simplex) remains a significant cause of prenatal brain injury.
* Chorioamnionitis: Recent literature heavily implicates maternal intrauterine infection and subsequent fetal inflammatory response syndrome (FIRS) as a major catalyst for white matter injury in the developing fetus.
Perinatal Factors
The perinatal period encompasses the time from the onset of labor until the first few days of life. While birth asphyxia is a known cause, it is responsible for a minority of cases.
* Labor Complications: Oxytocin augmentation, umbilical cord prolapse, and breech presentation are associated with an increased risk.
* Apgar Scores: While CP is often associated with low Apgar scores, low scores are not exclusively indicative of asphyxia; they frequently reflect underlying prenatal genetic or congenital anomalies.
* Prematurity and Low Birth Weight: Infants weighing less than 1,500 grams are at a dramatically increased risk, with an incidence of 60 per 1,000 births (compared to 2 per 1,000 in normal-weight infants). This is the single most significant risk factor in modern neonatology.
Postnatal Factors
Postnatal causes account for a small but significant subset of CP cases, typically occurring before the age of 2.
* Hypoxic-Ischemic Encephalopathy (HIE): Often caused by meconium aspiration or persistent fetal circulation. It presents clinically with profound hypotonia, decreased spontaneous movement, and neonatal seizures.
* Infections: Bacterial meningitis (commonly Group B Streptococcus) and viral encephalitis (Herpes simplex).
* Trauma: Non-accidental trauma (child abuse/shaken baby syndrome) and severe accidental traumatic brain injuries.
* Kernicterus: Severe hyperbilirubinemia leading to basal ganglia damage, classically resulting in dyskinetic/athetoid CP (now rare in developed nations due to phototherapy).
Pathophysiology of Periventricular Leukomalacia (PVL)
The increased incidence of CP in premature infants is primarily driven by the unique vascular anatomy and fragility of the periventricular white matter during the late second and early third trimesters.
Between the 26th and 32nd weeks of gestation, the periventricular area—which contains the descending corticospinal tracts responsible for motor control—is a vascular watershed zone. The blood vessels in this region are highly fragile and lack autoregulatory capacity, making them exquisitely susceptible to physiological fluctuations.
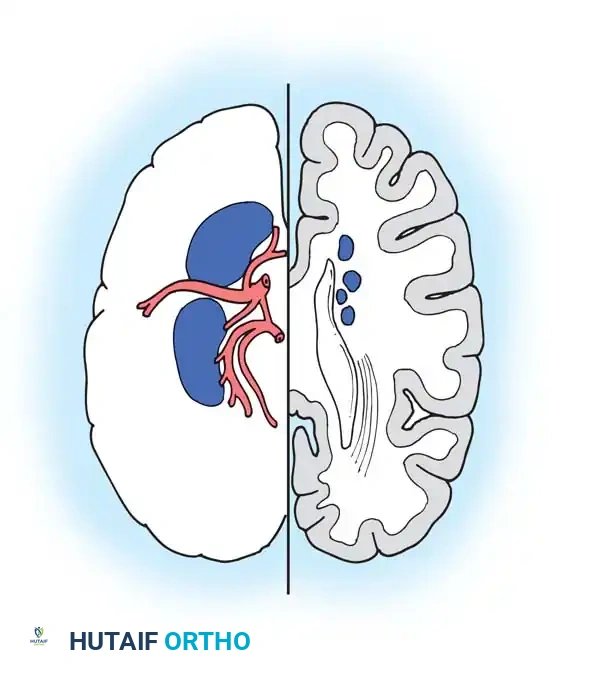
Hypoxic episodes, maternal diabetes, intrauterine infection, or rapid shifts in blood pressure can injure these delicate vessels. This leads to ischemia and subsequent necrosis of the white matter, a condition known as Periventricular Leukomalacia (PVL). Because the descending motor tracts to the lower extremities are located most medially in the periventricular space, they are the most vulnerable to this ischemic injury. This anatomical arrangement perfectly explains why premature infants with PVL classically present with Spastic Diplegia (lower extremities more involved than upper extremities).
Furthermore, these vascular fluctuations can lead to rupture of the germinal matrix, resulting in Intraventricular Hemorrhage (IVH). The severity of IVH is highly prognostic for future neurodevelopmental outcomes.
Grading of Periventricular Lesions (Intraventricular Hemorrhage)
The Papile classification is utilized to grade the severity of neonatal intraventricular hemorrhage via cranial ultrasound:
- Grade I: Bleeding is strictly confined to the germinal matrix.
- Grade II: Bleeding extends into the lateral ventricles, but without ventricular dilation.
- Grade III: Bleeding extends into the ventricles with subsequent ventricular dilation (hydrocephalus).
- Grade IV: Bleeding extends beyond the ventricles into the adjacent brain parenchyma (intraparenchymal hemorrhage).
Prognostic Pearl: Grades I and II IVH have a relatively low risk of progressing to severe cerebral palsy. Conversely, Grades III and IV carry a significantly higher incidence of severe neurological consequences, including spastic quadriplegia, profound intellectual disability, and the need for ventriculoperitoneal shunting due to post-hemorrhagic hydrocephalus.
Classification of Cerebral Palsy
Because cerebral palsy is a descriptive term rather than a specific disease entity, accurate classification is essential for communication among multidisciplinary teams, determining prognosis, and formulating orthopaedic treatment algorithms. CP is primarily classified by two distinct methods: Geographical (Topographical) and Physiological (Motor Type).
Geographical (Topographical) Classification
This system categorizes the patient based on the anatomical regions of the body affected by the movement disorder. While a patient's pattern of involvement can evolve subtly over time, this classification provides a rapid clinical picture of the patient's functional deficits.
Monoplegia
Involvement of a single limb. This is exceedingly rare in true cerebral palsy.
* Clinical Pitfall: If a patient presents with apparent monoplegia, the orthopaedic surgeon must maintain a high index of suspicion for alternative diagnoses, such as a spinal cord tumor, brachial plexus birth palsy, or an isolated peripheral nerve lesion.
Hemiplegia
Involvement of the upper and lower extremity on one side of the body.
* Pathophysiology: Typically results from a unilateral focal ischemic event, most commonly a middle cerebral artery (MCA) territory infarct.
* Clinical Presentation: The upper extremity is usually more severely affected than the lower extremity. Patients often present with a characteristic posture: shoulder internal rotation, elbow flexion, forearm pronation, wrist flexion, and thumb-in-palm deformity. In the lower extremity, a spastic equinovarus foot is the hallmark, often leading to a clinically significant limb length discrepancy (the hemiplegic side being shorter due to decreased growth). Independent ambulation is almost universally achieved.
Diplegia
Involvement of all four extremities, but the lower extremities are significantly more affected than the upper extremities.
* Pathophysiology: The classic manifestation of prematurity and periventricular leukomalacia (PVL).
* Clinical Presentation: Upper extremity involvement may be subtle, often manifesting only as mild fine motor clumsiness. The lower extremities exhibit significant spasticity, leading to the classic "crouch gait" or "scissoring gait" due to overactivity of the hip flexors, adductors, and hamstrings. These patients are the most frequent candidates for multi-level orthopaedic surgery (SEMLS - Single Event Multilevel Surgery) to optimize gait kinematics.
Quadriplegia (Tetraplegia)
Involvement of all four extremities, with the upper extremities equally or more affected than the lower extremities.
* Pathophysiology: Typically results from severe, global hypoxic-ischemic encephalopathy, often in full-term infants.
* Clinical Presentation: These patients have profound global motor impairment, often accompanied by bulbar dysfunction (swallowing difficulties, aspiration risk), seizure disorders, and severe cognitive impairment.
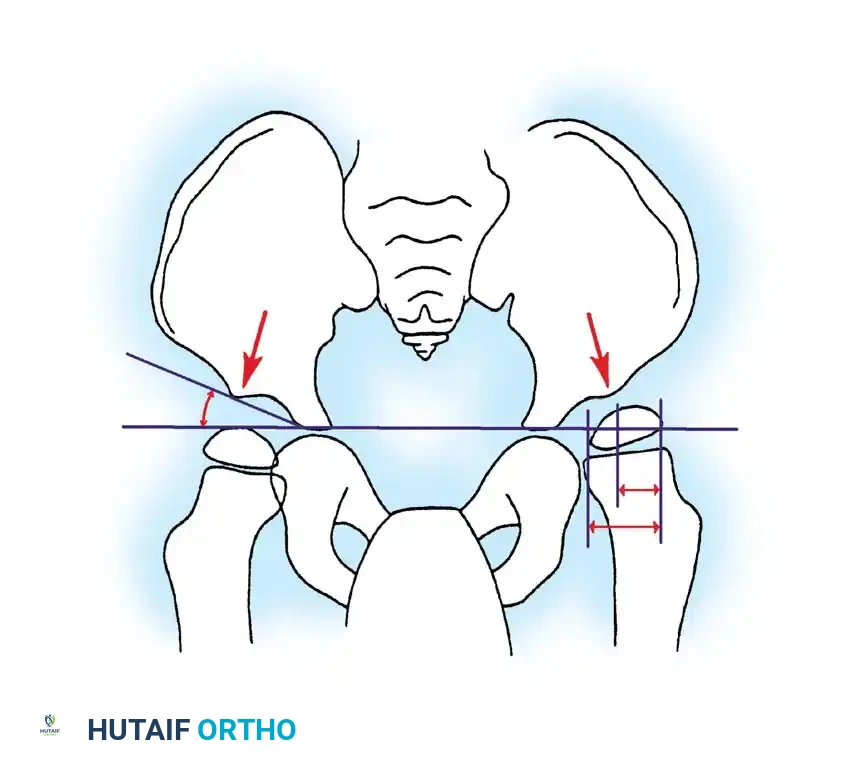
* Orthopaedic Implications: Quadriplegic patients are at the highest risk for severe, progressive musculoskeletal deformities, most notably spastic hip subluxation/dislocation and neuromuscular scoliosis. Orthopaedic management is usually focused on palliation, facilitating nursing care, maintaining perineal hygiene, and ensuring comfortable seating, rather than achieving independent ambulation.
Total Body Involvement
A term often used interchangeably with severe quadriplegia, but specifically highlighting the profound involvement of the head, neck, and trunk musculature, leading to complete lack of head control and truncal hypotonia despite appendicular spasticity.
Physiological (Motor Type) Classification
This classification is based on the predominant type of movement disorder and muscle tone abnormality. It directly correlates with the anatomical location of the brain lesion.
Spastic
The most common physiological type, accounting for 70-80% of all CP cases.
* Pathophysiology: Caused by injury to the pyramidal tracts (upper motor neurons) in the motor cortex or descending white matter pathways.
* Clinical Presentation: Characterized by a velocity-dependent increase in muscle tone (the "spastic catch"), hyperreflexia, clonus, and positive Babinski signs.
* Orthopaedic Relevance: Spasticity creates a chronic imbalance of muscle forces across joints. This is the type of CP most amenable to orthopaedic surgical intervention (e.g., tendon lengthenings, osteotomies) because the muscle overactivity is predictable and consistent.
Dyskinetic (Athetoid / Choreiform / Dystonic)
Accounts for 10-15% of cases.
* Pathophysiology: Caused by injury to the extrapyramidal system, specifically the basal ganglia. Historically associated with kernicterus, but now more commonly seen following severe term asphyxia.
* Clinical Presentation: Characterized by abnormal, involuntary, uncontrolled movements.
* Athetosis: Slow, writhing movements, particularly of the distal extremities.
* Chorea: Rapid, jerky, unpredictable movements.
* Dystonia: Sustained muscle contractions causing twisting and repetitive movements or abnormal postures.
* Orthopaedic Relevance: Surgical Warning: Orthopaedic procedures (particularly tendon transfers or lengthenings) in purely dyskinetic patients are fraught with complications. The unpredictable nature of the muscle tone often leads to severe reversal of deformity (e.g., lengthening an Achilles tendon may result in a devastating, progressive calcaneus gait). Surgery is generally avoided unless a fixed, rigid contracture is severely impeding care.
Ataxic
Accounts for less than 5% of cases.
* Pathophysiology: Caused by injury to the cerebellum or its pathways.
* Clinical Presentation: Characterized by a loss of balance, coordination, and depth perception. Patients exhibit a wide-based, unsteady gait and intention tremors. Pure ataxic CP is rare; it is often mixed with spasticity.
Hypotonic
Often a transient phase in infancy before the development of spasticity or dyskinesia. If it persists as the primary diagnosis, it is characterized by profound truncal and appendicular weakness. The orthopaedic surgeon must rule out underlying genetic syndromes or primary myopathies (e.g., spinal muscular atrophy) before accepting a diagnosis of purely hypotonic CP.
Mixed
Many patients do not fit neatly into a single physiological category. The most common mixed presentation is spasticity combined with dyskinesia. In these complex cases, the orthopaedic surgeon must carefully delineate which component of the deformity is driven by spasticity (potentially surgically correctable) and which is driven by dystonia (highly resistant to orthopaedic intervention).
The Orthopaedic Cascade: From Static Brain Lesion to Dynamic Deformity
Understanding the etiology and classification of cerebral palsy is paramount for the orthopaedic surgeon, as it dictates the natural history of the musculoskeletal pathology.
The fundamental orthopaedic problem in CP is that the skeleton grows at a normal rate, but the spastic, tethered musculature does not elongate proportionally. This creates a cascade of pathology:
1. Dynamic Contracture: Initially, the muscle is tight only when activated (spasticity). The joint has full passive range of motion under anesthesia.
2. Fixed Myostatic Contracture: Over time, the muscle undergoes structural changes (shortening of sarcomeres, increased collagen deposition), leading to a fixed contracture that does not resolve under anesthesia.
3. Bony Deformity: The abnormal, asymmetrical muscle forces acting on the growing, malleable pediatric skeleton alter normal bone modeling (Hueter-Volkmann principle). This leads to persistent fetal alignment, such as femoral anteversion, coxa valga, and tibial torsion.
4. Joint Instability: The combination of fixed contractures and bony deformity alters the joint reaction forces, inevitably leading to subluxation, dislocation, and premature degenerative joint disease (most critically in the hip).
The ultimate goal of orthopaedic intervention in cerebral palsy is to interrupt this cascade—optimizing function, preventing joint dislocation, and maximizing the patient's quality of life through a deep understanding of the underlying neurological etiology.
📚 Medical References
- cerebral palsy, J Hand Surg 13A:667, 1988.
- Houshian S, Schrøder HA: Wrist arthrodesis with the AO titanium wrist fusion plate: a consecutive series of 42 cases, J Hand Surg 26B:355, 2001.
- Howard AC, Stanley D, Getty CJ: Wrist arthrodesis in rheumatoid arthritis: a comparison of two methods of fusion, J Hand Surg 18B:377, 1993.
- Inoue G, Tamura Y: Radiolunate and radioscapholunate arthrodesis, Arch Orthop Trauma Surg 111:333, 1992.
- Jebson PJL, Adams BD: Wrist arthrodesis: review of current techniques, J Am Acad Orthop Surg 9:53, 2001.
- Kobus RJ, Turner RH: Wrist arthrodesis for treatment of rheumatoid arthritis, J Hand Surg 15A:541, 1990.
- Kulick RG, DeFiore JC, Straub LR, et al: Long-term results of dorsal stabilization in the rheumatoid wrist, J Hand Surg 6A:272, 1981.
- Lenoble E, Ovadia H, Goutallier D: Wrist arthrodesis using embedded iliac crest bone graft, J Hand Surg 18B:595, 1993.
- Louis DS, Hankin FM, Bowers WH: Capitate-radius arthrodesis: an alternative method of radiocarpal arthrodesis, J Hand Surg 9A:365, 1984.
- Luboshitz S, Burstein G, Engel J: Wrist arthrodesis: modified Gill’s technique, J Hand Surg 27B:568, 2002.
- Meads BM, Scougall PJ, Hargreaves IC: Wrist arthrodesis using a Synthes wrist fusion plate, J Hand Surg 28B:571, 2003.
- Mikkelsen OA: Arthritis of the wrist in rheumatoid arthritis, Hand 12:149, 1980.
- Mittal RL, Jain NC: Arthrodesis of the wrist by a new technique, Int Orthop 14:213, 1990.
- Moneim MS, Pribyl CR, Garst JR: Wrist arthrodesis: technique and functional evaluation, Clin Orthop Relat Res 341:23, 1997.
- Morelli M, Harris PG, Fowles JV, et al: A mechanical comparison of the immediate stability of three fixation devices used in wrist arthrodesis: a cadaver study, J Hand Surg 24A:828, 1999.
- Müller ME, Allgöwer M, Willenegger H, eds: Manual of internal fi xation, Heidelberg, 1970, Springer-Verlag. Murphy DM, Khoury JG, Imriglia JE, et al: Comparison of arthroplasty and arthrodesis for the rheumatoid wrist, J Hand Surg 28A:570, 2003.
- Nagy L, Büchler U: AO-wrist arthrodesis: with and without arthrodesis of the third carpometacarpal joint, J Hand Surg 27A:940, 2002.
- O’Bierne JO, Boyer MI, Axelrod TS: Wrist arthrodesis using a dynamic compression plate, J Bone Joint Surg 77B:700, 1995.
- Papaioannou T, Dickson RA: Arthrodesis of the wrist in rheumatoid arthritis, Hand 14:12, 1982.
- Rayan G: Wrist arthrodesis, J Hand Surg 11A:356, 1986.
- Rayan GM, Young BT: Arthrodesis of the spastic wrist, J Hand Surg 24A:994, 1999.
- Reeland AE, Sud V, Jemison DM: Early wrist arthrodesis for irreparable intraarticular
You Might Also Like